

Summary
The removal of impacted mandibular third molar is a common surgical procedure entailing some risk of complications, especially when the tooth and the inferior alveolar nerve and/or lingual cortical plate are in close proximity. A technique that can reduce the possibility of damage is the Ultra Sonic Bone Surgery. The aim of this report is to present a paradigmatic case of an impacted mandibular third molar closely associated with a complex odontoma, which was treated with the Ultrasonic Bone Surgery (UBS) device. This technique appeared to be a valid alternative to manual or mechanical treatment, strongly minimizing trauma to the inferior alveolar nerve, vascular tissues, or surrounding dental tissues.
Keywords: lower third molar, odontoma, ultrasonic bone surgery
Introduction
The extraction of the lower third molar is one of the most frequent procedures in oral surgery (1). Common complications following third molar surgery include sensory nerve damage, alveolar osteitis, infection, or haemorrhage during or after surgery (2,3). Less common complications are severe trismus, iatrogenic damage to the adjacent second molar, and iatrogenic mandibular fracture (4–5). Rare complications are brain abscess, epidural abscess, benign paroxysmal positional vertigo, subcutaneous and tissue space emphysema, subdural emphysema, and herpes zoster syndrome (6). The incidence of inferior alveolar nerve (IAN) injuries ranges from 0.41% to 8.1% for temporary decreases of sensitivity and from 0.014 % to 3.6% for prolonged signs and symptoms (7). When the radiographic signs of proximity of the mandibular canal to the roots of the third molar are present, the incidence of damage can be as high as 35% (8).
Risk factors also include advanced age, surgeon’s experience, the use of burs during bone removal or tooth sectioning, and surgical difficulty associated with deeply impacted teeth, particularly if distal bone removal is required (9,10).
Thus, any technique that could reduce the possibility of these nerve damages is worthy of exploration: a good example is the Ultra Sonic Bone Surgery (UBS). This technique consists of inducing energetic micro-vibrations with a frequency in the 20–32 kHz range, above the audible spectrum. The vibrations are generated by a transducer, which is electrically, piezo-electrically or magnetically controlled. Piezo-electric materials vary in size when they are submitted to an intense electric field, typically in the 500–750 V/mm range. These deformations can further transmit energetic micronic mechanical forces to a tip vibrating up to amplitudes of 200μm. UBS uses piezo-electrical transducers, because the generated movements are more energetic. Ultrasonically moved knives have the ability to cut hard tissues, like teeth and bone. In contrast, soft tissues like gingiva, blood vessels, nerves and sinus membranes are preserved from injury because they vibrate with the tip. This makes UBS particularly suitable for a broad spectrum of surgical applications including apicectomy, bone block section, sinus lifting, split-crest, nerve lateralization, resective bone surgery, and biopsies (11). We present here a case of a deeply located odontoma encompassing an impacted left mandibular third molar in close proximity to the inferior alveolar nerve, which was treated by Ultrasonic Bone Surgery (UBS) device.
Case report
A 40-year-old man was referred to the Oral Surgery Unit - Department of Oral and Maxillofacial Sciences (Sapienza University of Rome, Italy) for recurrent episodes of infection and pain in the mandibular left third molar region. Clinical examination revealed the presence of a partially impacted left mandibular third molar showing mild signs of gingival inflammation (plaque retention and bleeding on probing), without deformations or swelling of the region (Fig.1). The panoramic x-ray (Fig.2) revealed the presence of two large dense radiopaque masses in close association mesially and distally to the roots of the impacted tooth, consistent with the provisional diagnosis of complex odontoma. A computed tomography (CT) with the Dentascan program (Siemens Rs Somaton Volume Zoom Kv 120 mA 140; Siemens, Erlangen, Germany) (Figs. 3, 4), obtained in order to define the extension of the lesion and the anatomical topography, showed an intimate relationship between the inferior alveolar nerve and the odontoma-tooth unit. Surgical removal of the impacted third molar and the associated odontoma was planned. The patient received a single dose of 2 g of amoxicillin and clavulanic acid (Augmentin 1 g, GlaxoSmithKline, Verona, Italy) 1 h before surgery, together with a single dose (100 mg) of non-steroidal anti-inflammatory drug (Nimesulide, Aulin, Hoffmann-La Roche, Basel, Switzerland). Surgery was performed under local anesthesia. Local anaesthesia was performed (2% mepivacaine with 1:100,000 epinephrine) by IAN block injection and tissue infiltration. A mucoperiosteal buccal flap was reflected and bone was removed on the mesial, buccal and distal aspect of the third molar area with the Ultra-Sonic Bone Surgery UBS® device (Italia Medica, Milan, Italy) (Fig.5). The same device was used to separate the odontoma from the tooth. After sectioning, both the third molar and the associated lesion were gently removed using root elevators (Figs. 6, 7). The wound was carefully irrigated and the flap was repositioned and sutured with 4.0 suture (Vicryl®, ETHICON GmbH, Germany) (Figs. 8, 9). On macroscopic examination, the masses appeared to be a complex odontoma (Fig. 10), and the histopathological examination confirmed this diagnosis (12). After surgery, amoxicillin and clavulanic acid (1 g twice a day for 1 week) and nimesulide (100 mg twice a day for 2 days, and then as needed) were prescribed to the patient. Immediate postoperative wound healing was satisfactory, and the post-operative panoramic radiograph showed the integrity of the mandibular canal (Fig. 11). No symptoms or signs of neurosensory impairment of the innervated area, the inferior alveolar nerve, or the lingual nerve could be detected.
Figure 1.

Clinical examination of the impacted left mandibular third molar showing mild signs of gingival inflammation.
Figure 2.

Appearance of two large dense radiopaque masses closely associated to the roots of the impacted lower third molar at the orthopanoramic examination.
Figure 3.

Panorex CT scan obtained in order to define the extension of the lesion and regional anatomical topography.
Figure 4.

Sagittal CT scan examination showing an intimate relationship between the inferior alveolar nerve and the odontoma-tooth unit.
Figure 5.
Mucoperiosteal buccal flap reflection and bone removal with the Ultrasonic Bone Surgery.
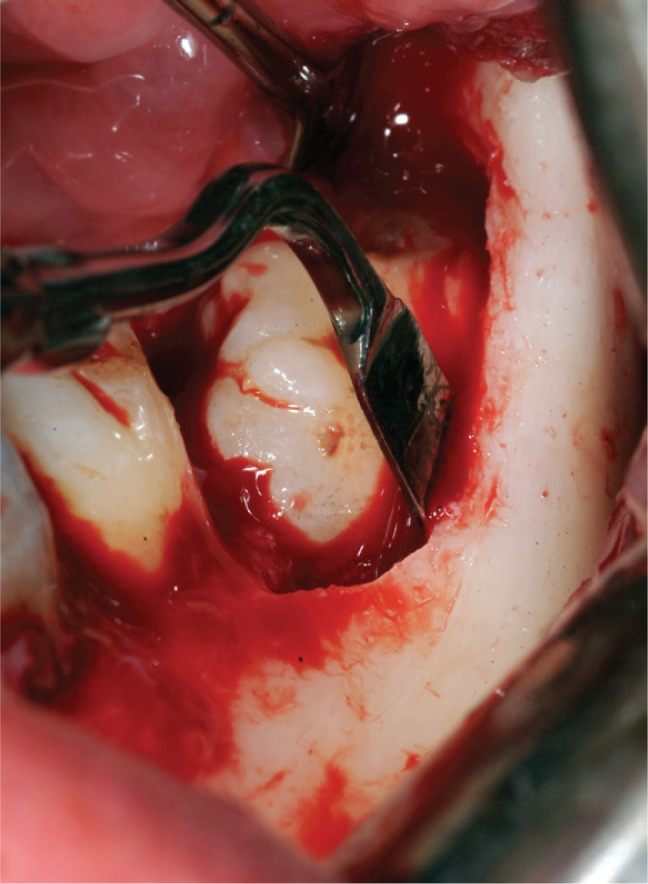
Figure 6.
The separation of the odontoma from the third molar and its removal with the ultrasonic device.
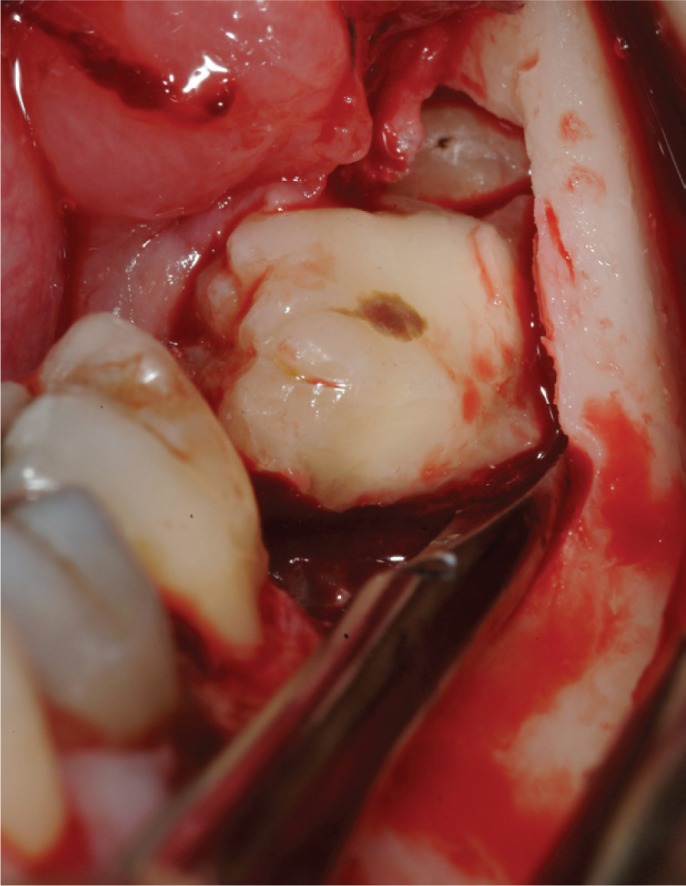
Figure 7.

The third molar sectioned and then removed using root elevators.
Figure 8.
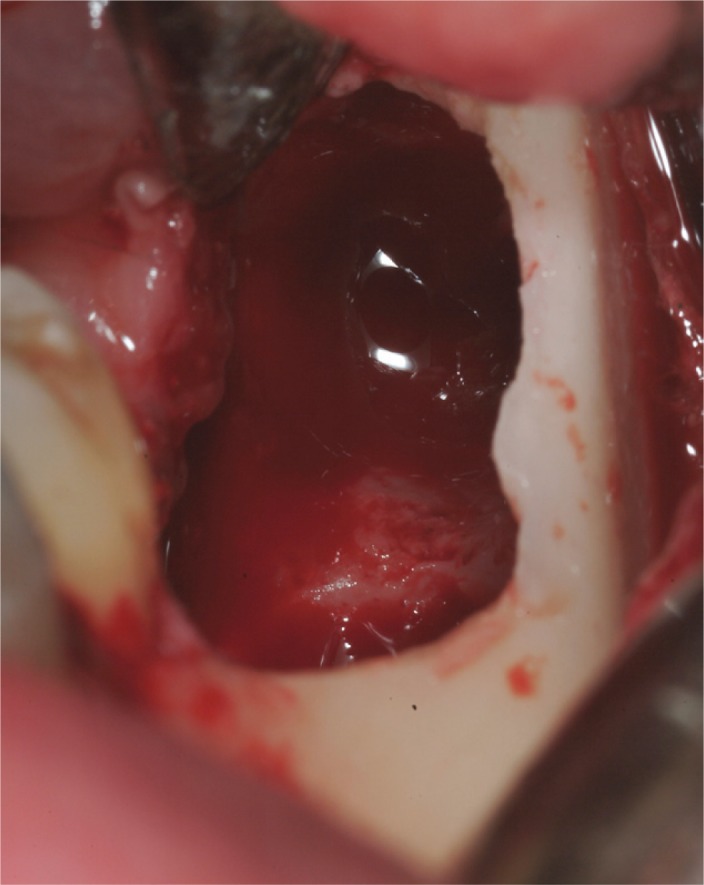
The wound after third molar removal.
Figure 9.
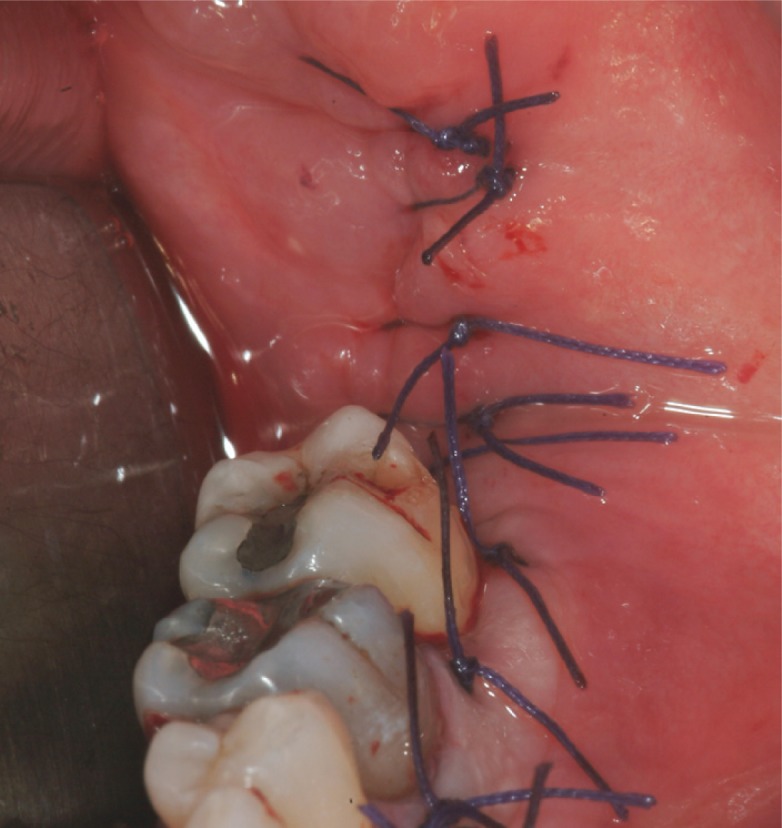
The flap repositioned and sutured.
Figure 10.

The complex odontoma.
Figure 11.

The post-operative orthopanoramic radiographs showing the integrity of the mandibular canal.
We confirm that we have read the Helsinki Declaration and have followed the guidelines concerning this report.
Discussion
The present case showed an impacted lower third molar associated with a relatively large complex odontoma in an intimate relationship with the inferior alveolar nerve canal. Surgical technique seems to play a major role in causing complications related to third molar extraction (13). Thus, a careful operating technique and adequate instruments may limit the occurrence of complications. Here, the removal of the odontoma-tooth unit was carried out by using an ultrasonic surgery device in order to reduce risk for inferior alveolar nerve damage. Ultra-sonic surgery is a tissue-selective technique that allows a micrometric, precise and smooth cut into mineralized tissue, while adjacent soft tissue such as nerves, vessels, periosteum or Schneiderian membrane (in case of maxillary sinus surgery) remain uninjured, because surgical action ceases when the device tips come in contact with non-mineralized tissue (14,15). An in vitro study concerning inferior alveolar nerve transposition by piezoelectric surgery showed that after surgery the epineurium became roughened without any damage to the deeper structures (16). Compared to traditional surgery by conventional burs or chisels, ultrasonic cutting precision and selectivity constitute important advantages, particularly in those cases where the surgery target is in close relationship with noble soft tissue structures (17). As a result, even less experienced surgeons (though properly trained) can perform such procedure, since the learning curve with ultrasonic surgery technique is strongly reduced compared to traditional surgery with rotating instruments (15). Nevertheless, a careful surgical approach remains critical considering that soft tissue can be damaged by excessive mechanical force while using the device. In addition, when compared with traditional surgery, bone healing following piezoelectric surgery seems similar (18) or even improved because piezoelectric bone surgery seems to induce an earlier increase in neo-osteogenesis, resulting in a more positive osseous response (19, 20). The latter may depend on the cavitation effect induced by ultrasonic cutting that allows an effective cooling avoiding significant hyperthermia and coagulation damages to the surrounding area (21). The same effect is responsible for a higher visibility during surgery compared to conventional instruments due to the evacuation of detritus with the aerosol formation (14). In the present case, the piezoelectric device used is the Ultra Sonic Bone Surgery UBS® (UBS). The vibration frequency of UBS is in the 20–32 kHz range and the maximum ultrasound power is 90 W. Increased power of the ultrasonic vibration and a higher vibrating frequency may result in a higher cutting efficiency in hard bone. Therefore, less pressure on the working tip is required further reducing the risk of thermal damage to the bone. High power also allows for good cutting in case there is soft bone, since the softer the bone the higher the ultrasound power required (21). Finally, the decrease of post-surgical complications with the use of ultrasound bone surgery after lower third molar removal must be considered, as reported by different authors (22,23).
Conclusion
The use of Ultrasound Bone Surgery in surgical cases, where risk for noble soft tissue damage is high, appears to be a valid alternative technique confirming other literature reports.
References
- 1.Marciani RD. Third molar removal: an overview of indications, imaging, evaluation, and assessment of risk. Oral Maxillofac Surg Clin North Am. 2007 Feb;19(1):1–13. doi: 10.1016/j.coms.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 2.Bui CH, Seldin EB, Dodson TB. Types, frequencies, and risk factors for complications after third molar extraction. J Oral Maxillofac Surg. 2003 Dec;61(12):1379–89. doi: 10.1016/j.joms.2003.04.001. [DOI] [PubMed] [Google Scholar]
- 3.Malkawi Z, Al-Omiri MK, Khraisat A. Risk indicators of postoperative complications following surgical extraction of lower third molars. Med Princ Pract. 2011;20(4):321–5. doi: 10.1159/000324550. [DOI] [PubMed] [Google Scholar]
- 4.Chrcanovic BR, Custódio AL. Considerations of mandibular angle fractures during and after surgery for removal of third molars: a review of the literature. Oral Maxillofac Surg. 2010 Jun;14(2):71–80. doi: 10.1007/s10006-009-0201-5. [DOI] [PubMed] [Google Scholar]
- 5.Woldenberg Y, Gatot I, Bodner L. Iatrogenic mandibular fracture associated with third molar removal. Can it be prevented? Med Oral Patol Oral Cir Bucal. 2007 Jan 1;12(1):E70–2. [PubMed] [Google Scholar]
- 6.Brauer HU. Unusual complications associated with third molar surgery: a systematic review. Quintessence Int. 2009 Jul-Aug;40(7):565–72. [PubMed] [Google Scholar]
- 7.Renton T, McGurk M. Evaluation of factors predictive of lingual nerve injury in third molar surgery. Br J Oral Maxillofac Surg. 2001 Dec;39(6):423–8. doi: 10.1054/bjom.2001.0682. [DOI] [PubMed] [Google Scholar]
- 8.Tay AB, Go WS. Effect of exposed inferior alveolar neuro-vascular bundle during surgical removal of impacted lower third molars. J Oral Maxillofac Surg. 2004 May;62(5):592–600. doi: 10.1016/j.joms.2003.08.033. [DOI] [PubMed] [Google Scholar]
- 9.Tolstunov L. Lingual nerve vulnerability: risk analysis and case report. Compend Contin Educ Dent. 2007 Jan;28(1):28–31. [PubMed] [Google Scholar]
- 10.Ziccardi VB, Zuniga JR. Nerve injuries after third molar removal. Oral Maxillofac Surg Clin North Am. 2007 Feb;19(1):105–15. doi: 10.1016/j.coms.2006.11.005. [DOI] [PubMed] [Google Scholar]
- 11.Blus C, Szmukler-Moncler S, Vozza I, Rispoli L, Polastri C. Split-crest and immediate implant placement with ultrasonic bone surgery (piezosurgery): 3-year follow-up of 180 treated implant sites. Quintessence Int. 2010 Jun;41(6):463–9. [PubMed] [Google Scholar]
- 12.Philipsen HP, Reichart PA. Classification of odontogenic tumours. A historical review. J Oral Pathol Med. 2006 Oct;35(9):525–9. doi: 10.1111/j.1600-0714.2006.00470.x. [DOI] [PubMed] [Google Scholar]
- 13.Brann CR, Brickley MR, Shepherd JP. Factors influencing nerve damage during lower third molar surgery. Br Dent J. 1999 May 22;186(10):514–6. doi: 10.1038/sj.bdj.4800155. [DOI] [PubMed] [Google Scholar]
- 14.Barone A, Santini S, Marconcini S, Giacomelli L, Gherlone E, Covani U. Osteotomy and membrane elevation during the maxillary sinus augmentation procedure. A comparative study: piezoelectric device vs. conventional rotative instruments. Clin Oral Implants Res. 2008 May;19(5):511–5. doi: 10.1111/j.1600-0501.2007.01498.x. [DOI] [PubMed] [Google Scholar]
- 15.Schlee M, Steigmann M, Bratu E, Garg AK. Piezosurgery: Basics and Possibilities. Implant Dent. 2006 Dec;15(4):334–40. doi: 10.1097/01.id.0000247859.86693.ef. [DOI] [PubMed] [Google Scholar]
- 16.Degerliyurt K, Akar V, Denizci S, Yucel E. Bone lid technique with piezosurgery to preserve inferior alveolar nerve. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Dec;108(6):e1–5. doi: 10.1016/j.tripleo.2009.08.006. [DOI] [PubMed] [Google Scholar]
- 17.Chiriac G, Herten M, Schwarz F, Rothamel D, Becker J. Autogenous bone chips: influence of a new piezoelectric device (Piezosurgery) on chip morphology, cell viability and differentiation. J Clin Periodontol. 2005 Sep;32(9):994–9. doi: 10.1111/j.1600-051X.2005.00809.x. [DOI] [PubMed] [Google Scholar]
- 18.Preti G, Martinasso G, Peirone B, et al. Cytokines and growth factors involved in the osseointegration of oral titanium implants positioned using piezoelectric bone surgery versus a drill technique: a pilot study in minipigs. J Periodontol. 2007 Apr;78(4):716–22. doi: 10.1902/jop.2007.060285. [DOI] [PubMed] [Google Scholar]
- 19.Vercellotti T, Kim DM, Wada K, Fiorellini JP. Osseous response following respective therapy with piezosurgery. Int J Periodontics Restorative Dent. 2005 Dec;25(6):543–9. [PubMed] [Google Scholar]
- 20.Emam TA, Cuschieri A. How safe is high-power ultrasonic dissection? Ann Surg. 2003 Feb;237(2):186–91. doi: 10.1097/01.SLA.0000048454.11276.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Blus C, Szmukler-Moncler S. Split-crest and immediate implant placement with ultra-sonic bone surgery: a 3-year life-table analysis with 230 treated sites. Clin Oral Implants Res. 2006 Dec;17(6):700–7. doi: 10.1111/j.1600-0501.2006.01206.x. [DOI] [PubMed] [Google Scholar]
- 22.Goyal M, Marya K, Jhamb A, Chawla S, Sonoo PR, Singh V, Aggarwal A. Comparative evaluation of surgical outcome after removal of impacted mandibular third molars using a Piezotome or a conventional handpiece: a prospective study. Br J Oral Maxillofac Surg. 2011 Nov 14; doi: 10.1016/j.bjoms.2011.10.010. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 23.Barone A, Marconcini S, Giacomelli L, Rispoli L, Calvo JL, Covani U. A randomized clinical evaluation of ultrasound bone surgery versus traditional rotary instruments in lower third molar extraction. J Oral Maxillofac Surg. 2010 Feb;68(2):330–6. doi: 10.1016/j.joms.2009.03.053. [DOI] [PubMed] [Google Scholar]