

Abstract
The paraspinal muscles have been implicated as a major causative factor in the progression of idiopathic scoliosis. Therefore, the objectives of this preliminary study were to measure the electromyographic activity (EMG) of the paraspinal muscles to determine its relationship to progression of the scoliotic curve. Idiopathic scoliotic patients were selected and identified afterwards on curve progression. The EMG activity on both sides of the spine was measured in a set of standardized postures using bipolar surface electrodes at the apex and two end vertebrae of the scoliotic curve. An EMG ratio involving measurements of the EMG activity on the convex and concave sides of the scoliotic curve was used to evaluate the paraspinal muscles. Enhanced EMG ratios at the apex of the scoliotic curve were found in both groups during sitting and standing. The most interesting finding was that children with progression of the curve also showed enhanced EMG ratios at the lower end vertebra of the curve. The EMG ratios between the groups were significantly different from each other at the apex and end vertebrae for several test conditions. Overlap in the EMG-ratio ranges made differentiation difficult for prediction of the progression of the individual scoliosis patient. However, the EMG ratio at the lower end vertebra of the scoliotic curve is significantly higher than 1 in all test conditions in the group of children with subsequent progression of the curve, whereas it is always normal in the non-progressive group. Therefore, EMG of the paraspinal muscles might be of value for prediction of progression in idiopathic scoliosis.
Keywords: Spine, Scoliosis, Progression, Electromyography, Asymmetry
Introduction
The high frequency with which scoliosis accompanies many different neurologic syndromes has led to repeated attempts to find a neuromuscular cause for idiopathic scoliosis [21, 22]. As a result, many studies have been published on electromyographic (EMG) activity of paraspinal muscles during the development and progression of idiopathic scoliosis [1, 2, 11, 12, 13, 18, 20, 23, 24]. The methods and interpretation of the EMG results have differed considerably, however. Some EMG tests were not performed systematically in well-defined body positions, or EMG recordings were qualitative readings only [2, 18, 24]. Some previous studies did not differentiate between well-defined groups [2, 18]. Although in most studies an increased EMG activity was found in the paraspinal muscles on the convex side of the scoliotic curve, it is still not clear whether the reported EMG findings reflect a primary neuromuscular factor causing scoliosis or whether they only indicate a secondary mechanism induced by the deformed spine. The results have been thought to be a sign of convex-side muscular weakness [24], while others explained it as an effect of the stretching of the erector spinae muscles on the convex side [2].
The object of this study was to examine the relation between the EMG activity of the paraspinal muscles measured in standardized tests and the progression of the scoliotic curve. Our idea was that the extent of paraspinal muscle activity would reveal differences in muscle involvement in idiopathic scoliosis that may correlate to the progression of the scoliotic curve. The hypothesis is that patients with non-progressive curves would show a higher EMG activity ratio, compared with patients with progressive curves in at least two levels of the scoliotic curve. A higher EMG activity ratio might be interpreted as a compensatory mechanism against progression of the idiopathic scoliotic curve. We now report the preliminary results.
Methods and materials
Patients with idiopathic scoliosis were measured two times with an interval of 4–5 months. EMG measurements of standardized postures as well as radiographs were made at T0 and T1. The EMG measurements at T0 were used for calculations in this study. At T1 the progression of the scoliotic curve could be assessed.
Progressiveness is defined as a documented Cobb angle change of less than 5° (non-progressive) or more than 5° (progressive) on a second radiograph after a period of 4–5 months, which results in a cutoff value of a rate of change of more than 12° per year. Based on the Cobb angle change, subjects with a progressive or non-progressive period could be identified and grouped accordingly. Then, the EMG measurements at T0 were coupled and analyzed for correlation with curve progression.
Subjects
Patients were included from our orthopaedic outpatients’ department. All patients suffered from adolescent idiopathic scoliosis with right-sided lateral spinal curves. Besides scoliosis, the patients had no history of other physical disorders. Spinal curves (according to Cobb [4]) ranged from 10° to 60° at T0. All patients had Risser sign 1 to 4. In Table 1 the results of Cobb angle changes are presented. The Cobb angle at the start of the observation period is not statistically different between the groups. Identified at T1, the progressive group consisted of one male and seven female patients with a mean age of 13.6 years (range 12–16 years). The non-progressive group consisted of two male and 13 female patients, with a mean age of 14.3 years (range 11–16 years). All subjects were examined by the same physician, using the same measuring equipment, and in the same testing conditions. Informed consent was given by each subject, or by his or her parents.
Table 1.
Cobb angle changes in the two groups of patients in this study (SD standard deviation)
| Group | |||
|---|---|---|---|
| Non-progressive | Progressive | Difference | |
| Mean (SD) | Mean (SD) | p value | |
| Cobb angle (°) | |||
| Start interval | 29.8 (11.1) | 39.2 (18.3) | 0.141 |
| Change (range) | −8.4–3.7 | 5.3–23.9 | - |
Cobb angle measurements
Cobb angles were measured from digitized radiographs by recording the angles between the upper and lower most-tilted end vertebra, by drawing lines through the endplates of the scoliotic curve on the monitor with the cursor according to the Cobb method [4]. This digital radiographic measurement technique was described in detail earlier [3].
EMG recordings
To measure whether muscle activity was present, disposable bipolar surface EMG electrodes (NEOTRODE 10 mm diameter, Utica, NY, USA) with a 25 mm interelectrode center distance were used and placed on the erector spinae. The electrodes were connected to a multichannel physiologic recording device (Porti system, TMS International, Enschede, The Netherlands). The EMG signal picked up by each electrode was amplified, AD-converted and stored in a computer for analysis. The EMG signals were low-pass filtered and full-wave rectified. The sampling rate was 800 Hz. During each test condition, a technician continuously monitored the EMG recordings. The recordings were made at T0 and T1.
Measuring procedure and protocol
Six pairs of EMG electrodes were placed symmetrically at the superficial erector spinae muscles (longissimus) at three levels, 30 mm from the midline and parallel to the spinous processes (Fig. 1). The electrode levels corresponded to the apex vertebra and both end vertebrae of the curve. Two pairs of EMG electrodes were placed symmetrically at the latissimus dorsi muscles at level T12. A set of ECG electrodes was placed at the ictus cordis. The patients were carefully instructed before recording in three test conditions: (1) lying supine, relaxed with head straight and arms along the body; (2) sitting relaxed with hands on lap and feet together flat on the ground; and (3) standing relaxed with arms along body and feet together. These postures were used because they correspond to easy natural physiological human statures. The execution of each test was demonstrated by the investigator.
Fig. 1.

Positioning of the eight bipolar electrodes at the upper end vertebra (U), the apex (A) vertebra and lower end vertebra (L) of the scoliotic curve. An extra pair of electrodes was placed at the latissimus dorsi muscles (D). a Radiographical determination of the apex and end vertebrae of the scoliotic curve. b After radiographical confirmation the electrodes are placed on the back of the patient. c A schematic view of the position of the eight pairs of electrodes
Data and statistical analysis
Data consisted of raw EMG (Fig. 2a) and Cobb angles (Fig. 1a). It was necessary to compensate for the contamination of the EMG activity by the ECG. Therefore, ECG activity was removed by zero offsetting during an interval of 125 around the QRS-complex (Fig. 2b). The variables used in this study are defined as follows:
Fig. 2.

Example of the raw EMG and ECG data of one of the exercises (standing). a EMG and ECG signals over the eight pairs of electrodes (elec1 stands for the signal of the concave electrode at the upper end vertebra; elec2 is the signal of contralateral convex electrode at the upper end vertebra; elec3 and elec4 are the signals of the concave and convex electrodes at the apex vertebra; elec5 and elec6 are identical to elec1 and elec2, but at the lower end vertebra; elec7 and elec8 represent the EMG signals on the concave and convex side on the latissimus dorsi muscle). b The raw EMG data after digital filtering of the ECG signals
Paraspinal activity (EMG) ratio
This is defined as the absolute summated EMG amplitudes of the total EMG recording time (corrected for cardiac contamination) of a convex electrode pair divided by a contralateral concave electrode pair of the erector spinae muscles. In this way an activity EMG ratio of 1 (unity) means that the EMG activities on the convex and concave sides of the scoliotic curve are the same. An EMG activity ratio higher than 1 means that the EMG activity on the convex side is greater than that on the concave side. Finally, an EMG activity ratio lower than 1 stands for less EMG activity on the convex side than on the concave side. The EMG recordings of the apex vertebra and the two end vertebrae were compared between the progressive and non-progressive groups.
Extraspinal activity (EMG) ratio
This ratio is identical to the paraspinal activity (EMG) ratio, except that it is measured for the latissimus dorsi muscles. These muscles were measured to determine whether muscles groups in another anatomical region than the vertebral column were affected by the scoliosis.
Statistical considerations
In Table 1, means and standard deviation (SD) and in Table 2 means and their 95% confidence interval (CI) and range are presented. For the EMG ratios these parameters were constructed assuming they had a log-normal distribution. Statistical significance of differences was assessed by Student’s t-test, accounting for variance inhomogeneity when necessary. A two-sided p value of less than 0.05 was considered significant.
Table 2.
The mean EMG ratio (with its 95% CI and range) at the three levels of the curve in the three test conditions (CI confidence interval; M. latis.dorsi musculus latissimus dorsi)
| Group | |||||
|---|---|---|---|---|---|
| Non-progressive | Progressive | Difference | |||
| (n=15) | (n=8) | p value | |||
| Electrode level | Mean (95%CI : range) | Mean (95%CI : range) | |||
| Upper end vertebra | 0.69 (0.47–1.02:0.11–1.69) | 0.97 (0.64–1.47:0.54–3.13) | 0.294 | ||
| 1 | Supine | Apex | 1.83 (1.29–2.58:0.75–4.00)* | 0.90 (0.62–1.33:0.35–2.20) | 0.021 |
| Lower end vertebra | 0.91 (0.74–1.13:0.33–1.71) | 1.74 (1.10–2.76:0.97–5.41)* | 0.009 | ||
| M. latis.dorsi | 1.20 (0.99–1.45:0.93–1.86) | 0.96 (0.79–1,17 : 0.27–3.45) | 0.718 | ||
| Upper end vertebra | 0.87 (0.56–1.36:0.18–5.13) | 2.00 (0.98–4.06:0.58–7.87) | 0.055 | ||
| 2 | Sitting | Apex | 2.51 (1.52–4.14:0.34–14.4)* | 2.13 (1.33–3.43:0.61–5.20)* | 0.685 |
| Lower end vertebra | 1.09 (0.77–1.55:0.33–3.01) | 3.37 (1.84–6.15:1.24–13.4)* | 0.003 | ||
| M. latis.dorsi | 1.20 (0.78–1.85:0.38–2.11) | 1.08 (0.70–1.66:0.41–2.77) | 0.858 | ||
| Upper end vertebra | 0.74 (0.55–1.00:0.21–1.61)* | 1.88 (1.00–3.55:0.50–8.37)* | 0.007 | ||
| 3 | Standing | Apex | 2.10 (1.47–3.00:0.58–6.26)* | 1.65 (1.15–2.36:0.86–3.93)* | 0.400 |
| Lower end vertebra | 0.96 (0.80–1.15 : 0.43–1.64) | 2.55 (1.50–4.34:0.80–7.86)* | 0.000 | ||
| M. latis.dorsi | 1.04 (0.64–1.67:0.29–2.18) | 0.92 (0.57–1.47:0.21–1.81) | 0.456 | ||
*A p value <0.05, which means that the ratio difference of the convex and concave side is significantly different from 1
Results
Paraspinal activity (EMG) ratio
The EMG ratios, measured from the erector spinae muscles, were consistently higher than 1 at the apex in the non-progressive group, in all test conditions. The results are summarized in Table 2. The EMG ratios at the lower end vertebra of the curve in the non-progressive group do not significantly differ from unity in all three test conditions. The EMG ratios at the upper end vertebra in the non-progressive group were not significantly different from 1 in the supine and sitting test conditions. However the EMG ratio at the upper end vertebra was significantly lower than 1 in this group in the standing test condition.
The EMG ratio was found to be significantly higher than 1 at the lower end vertebra of the curve in the progressive group in all three test conditions (Table 2). The EMG ratio was not significantly different from 1 at the apex in the progressive group in the supine test condition. However, EMG ratios were significantly higher than 1 at the apex in the progressive group when sitting and standing. The EMG ratios at the upper end vertebra in the progressive group did not significantly differ from 1 in the supine and sitting test conditions. For standing, the EMG ratio was significantly higher than 1 at the upper vertebra.
Comparing both groups, the EMG ratio patterns are different. In the progressive group, higher EMG ratios were found at the lower end vertebra in all three test conditions (p=0.009, p=0.003 and p=0.000 for supine, sitting and standing respectively, Table 2). The group’s individual Cobb angle changes vs EMG ratios to show the predictive nature of the EMG are depicted in Fig. 3.
Fig. 3.
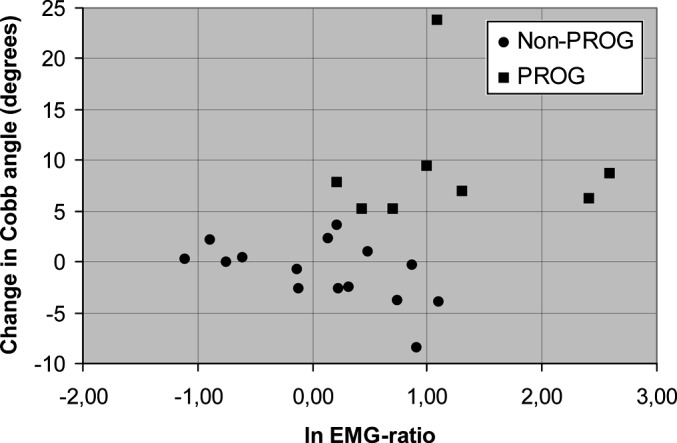
The individual Cobb angle changes vs EMG ratios at the lower end vertebra in the sitting posture to show the predictive nature of the EMG
At the upper end vertebra a statistically significant difference between the two groups was only found in the standing test condition (p=0.007). In this condition the EMG ratio was lower for the non-progressive group than for the progressive group. Comparing both groups at the apex vertebra, a statistically significant difference was only found in the supine test condition (p=0.021). There was a higher apical EMG ratio in the non-progressive group when compared with the progressive group.
Extraspinal activity (EMG) ratio
The EMG ratio (as summated for both groups in Table 2) between the right and left muscle groups of the latissimus dorsi muscles was never different from unity in both groups for all three test conditions.
Discussion
In this study, we measured the electromyographic (EMG) activity of the paraspinal muscles to assess whether there is a relationship between EMG activity and progressiveness of the curve in idiopathic scoliosis. In our study the patients were divided into two groups, based on clinical evaluation criteria and progressiveness. Geometrically, the scoliotic deformity involves the whole vertebral column. It is for this reason that we performed our measurements on the entire course of the scoliotic curve. Therefore, both the apex and the upper and lower end vertebrae of the scoliotic curve were taken into account. In addition, to study asymmetry in spinal EMG activity, a ratio was introduced. The EMG activity ratio is defined as spinal muscle activity on the convex side divided by activity on the concave side of the scoliotic curve. All patients in this study had spinal growth potential, since maximum skeletal maturity (Risser sign 5) was never observed. Our hypothesis was that patients with non-progressive curves would show a higher EMG activity ratio compared with patients with progressive curves in at least two levels of the scoliotic curve.
The results of this study show that EMG activity ratios higher than 1 were generally found at the apex vertebra in both groups. These results are in agreement with the asymmetrical EMG activation of the paraspinal muscles, as found previously by other authors [11, 13, 23, 24]. However, in contrast, the higher muscle activity on the convex side of the deformed spine was interpreted as being a problem of convex-side muscular strength or weakness [1, 13, 24]. Zetterberg et al. described asymmetrical EMG changes in a quantitative way [23]. They found higher convex-side EMG activities in the erector muscle groups in curves greater than 30° when raising the head and trunk from a prone position. In the study of Reuber et al., the authors found significant EMG differences between controls and idiopathic scoliosis patients with curves exceeding 25° [12]. In contrast to our study, they found no EMG activity differences between patients with progressive and non-progressive curves. Guth and co-workers, on the other hand, found a distinct asymmetric activity in non-progressive scoliosis [5, 7]. Other investigators see the asymmetry as a symptom for possible progression [5, 11, 16, 18]. Finally a number of researchers suggested that EMG findings on the convex side are a biomechanical necessity to balance the deviated spine [7, 12].
Our results do not support this hypothesis, because EMG activity ratios higher than 1 were also present in the progressive group. Further, the groups show different EMG ratio patterns of EMG activity ratios during the three test conditions. The higher EMG ratios at the apex in both groups in most test conditions might indeed be a biomechanical necessity to keep balance. But the pronounced asymmetric EMG activity in the progressive group at the lower end vertebra is a striking difference between the groups. An explanation could be that asymmetric EMG activity at the apex in the non-progressive group is not only sufficient to maintain balance but also to keep the Cobb angle unchanged by bone remodeling, as long as growth velocity is relatively low. In the progressive group, the similar asymmetric activity at the apex may not be sufficient to prevent progression of the Cobb angle, because bone remodeling can not keep up with a relatively high growth velocity. Indeed, the mean Cobb angle in the progressive group is larger than in the non-progressive group at first visit. However, due to the large variance and the limited number of patients, the difference did not reach statistical significance. As a result, the further deviation of the spine would lead to such an imbalance that a higher EMG ratio at the lower end of the curve is also necessary to maintain balance by pulling the whole vertebral column to the convex side. This sort of traction on the spine might even aggravate its malformation instead of stabilizing it. The progression of the scoliosis may even be such that a higher EMG ratio at the upper end of the curve is needed to keep head and neck upright, as found in the standing position. In the supine position, where stimuli to keep balance are lacking, only the result of the main process of adaptation is seen: asymmetric activity at the apex in the non-progressive group and asymmetric activity at the lower end of the curve in the progressive group.
In this study, the latissimus dorsi muscle groups showed no evidence of asymmetric EMG activity. We therefore concluded that the muscle activity changes in scoliosis are localized to the anatomic region of the deformed spine. Other investigators have examined extraspinal muscles and found muscle changes. However, their results were based on histometric and morphologic findings and not on electromyographic findings [7, 14, 15, 21, 22].
If abnormal muscle activity were the cause of the deformity, one would expect that the unilaterally increased activity of the paraspinal muscle group would result in a concavity on the active side. However, we found that the most active muscles were located on the right convex side of the scoliotic curve.
A number of important methodological points should be kept in mind in this study. First, the erector spinae muscle groups were investigated, since they are the most important muscle group in maintaining spinal balance in the human body [8]. Second, the EMG activity was measured only in the superficially located muscle groups by surface electrodes. In a pilot study we found that surface and needle EMG recordings of the scoliotic curve show qualitatively the same EMG-activity asymmetry [19]. For that reason and for practical reasons, surface electrodes were used in this study. Third, only three levels of the scoliotic spine (apex and both end vertebrae) and the latissimus dorsi muscles were measured. In order to take more anatomical regions at the back into consideration, other muscles are currently being examined. Fourth, it should be noted that this study was restricted to right-sided single curves. Further studies are needed to evaluate other types of curves (such as double curves). Finally, the EMG-activity ratios differed considerably between individuals within a group. This may be due to variability in muscle tension, body posture and electrode position [9, 17]. As a consequence, this large variation prohibited the use of the EMG activity ratio for individual scoliotic prognosis.
The present study is part of an extended project, in which parameters are being developed in order to predict the progression of a scoliotic curve based on EMG measurements. At the moment, a prospective longitudinal study of the spinal growth determined from more than two consecutive radiographs correlated to the concomitant EMG activity ratios is in progress. This may enable us to clarify the associations between muscle asymmetry, growth velocity and changes in the progression of scoliosis. We expect that children will only show asymmetric EMG activity during growth, which disappears after final height is reached. For the moment, we are inclined to postulate that growth is, apart from EMG-activity asymmetry, an important issue in the progression of idiopathic scoliosis. It is not our intention to examine its etiology.
Conclusions
Our findings did not support the hypothesis that EMG activity ratios higher than 1 would only be observed in patients with non-progressive scoliotic curves as a compensatory mechanism. The current results show that there is a relationship between initial EMG activity at the lower end vertebra of the curve and subsequent progressiveness of the curve in idiopathic scoliosis. Whether the EMG asymmetry was a consequence of a decreased activity on the concave side or an increased activity on the convex side could not be determined from this study. However, it was clear that the pattern of asymmetry in paraspinal EMG activity at the lower end vertebra of the curve is associated with progressiveness of the scoliosis. Therefore, we will correlate both spinal growth speed and muscle activity asymmetry to the progression of idiopathic scoliosis in a larger future study, using several consecutive radiographs and surface EMG measurements in a cohort of patients.
Acknowledgments
The authors thank Dr. Tom W. van Weerden for his contribution to the discussion and Ronald Davidsz for his technical support. This work was supported by STW (Netherlands Technology Foundation)
References
- 1.Alexander Arch Phys Med Rehabil. 1978;59:314. [PubMed] [Google Scholar]
- 2.Butterworth South Med. 1969;J:1. [Google Scholar]
- 3.Cheung Eur Spine J. 2002;11:535. doi: 10.1007/s00586-001-0381-7. [DOI] [PubMed] [Google Scholar]
- 4.Cobb Am Acad Orthop. 1948;5:261. [Google Scholar]
- 5.G Z Orthop Ihre Grenzgeb. 1976;114:480. [PubMed] [Google Scholar]
- 6.Henssge Z Orthop Ihre Grenzgeb. 1980;99:167. [PubMed] [Google Scholar]
- 7.Hopf Eur Spine J. 1998;7:6. doi: 10.1007/s005860050019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hoppenfeld S (1974) Histochemical findings in paraspinal muscles of patients with idiopathic scoliosis. In: Zorab PA (ed) Scoliosis and muscle. Heinman, London, pp 113–114
- 9.Lindstr Proc IEEE. 1977;65:653. [Google Scholar]
- 10.LonsteinJ Bone Joint Surg Am 19846616690430 [Google Scholar]
- 11.Redford Arch Phys Med Rehabil. 1969;50:434. [PubMed] [Google Scholar]
- 12.Reuber Spine. 1983;8:447. doi: 10.1097/00007632-198307000-00002. [DOI] [PubMed] [Google Scholar]
- 13.Riddle Lancet. 1955;1:1. doi: 10.1016/s0140-6736(55)91020-5. [DOI] [PubMed] [Google Scholar]
- 14.Spencer J Neurol Sci. 1976;30:137. doi: 10.1016/0022-510X(76)90261-6. [DOI] [PubMed] [Google Scholar]
- 15.Spencer J Neurol Sci. 1976;30:143. doi: 10.1016/0022-510X(76)90262-8. [DOI] [PubMed] [Google Scholar]
- 16.Tanchev Spine. 2000;11:1. [Google Scholar]
- 17.Türker KS (1993) Electromyography: some methodological problems and issues. Phys Ther 698–710 [DOI] [PubMed]
- 18.Valentino Anat Clin. 1985;7:55. doi: 10.1007/BF01654630. [DOI] [PubMed] [Google Scholar]
- 19.Weerden v TW (2000) EMG recordings of the scoliotic spine. A pilot study. Personal communication
- 20.WynarskySpine 19891412783630 [Google Scholar]
- 21.Yarom Israel J Med Sci. 1979;15:917. [PubMed] [Google Scholar]
- 22.YaromSpine 1979412432711 [Google Scholar]
- 23.Zetterberg Acta Orthop Scand. 1984;55:304. doi: 10.3109/17453678408992362. [DOI] [PubMed] [Google Scholar]
- 24.Zuk J Bone Joint Surg Br. 1962;44:102. [Google Scholar]