

Summary:
This article examines a specific technology, the germ-free "isolator," tracing its development across three sites: (1) the laboratory for the production of standard laboratory animals, (2) agriculture for the efficient production of farm animals, and (3) the hospital for the control and prevention of cross-infection and the protection of individuals from infection. Germ-free technology traveled across the laboratory sciences, clinical and veterinary medicine, and industry, yet failed to become institutionalized outside the laboratory. That germ-free technology worked was not at issue. Working, however, was not enough. Examining the history of a technology that failed to find widespread application reveals the labor involved in aligning cultural, societal, and material factors necessary for successful medical innovation.
Keywords: gnotobiotics; cross-infection; LOBUND; laboratoryanimal; bioethics; bubbleboy,
In 1963 at a symposium on the future of man, the biologist Julian Huxley forcefully declared a "germ-free world is an ecological absurdity, just as a perpetual motion machine is a mechanical absurdity . . . it is just nonsense to talk of eradication."1 Huxley was responding to a discussion between Hilary Koprowski, the renowned virologist and immunologist, and the Nobel Prize-winning molecular and exo-biologist Joshua Lederberg.2 Lederberg believed a "germ-free world" was hypothetically possible and a useful concept to think with.3 Koprowski in contrast warned that the relationship between man and microbe was a "battlefront" that had recently entered into "a sort of truce based upon the maintenance of ecological balance between man and the pathogenic bacteria." However, the "truce" was fragile because the "bacterial diseases of man are suppressed while at the same time the causative agents are allowed to propagate in nature." Attempts to eradicate germs were always hazardous, Koprowski explained, not least in medical interventions such as "surgical procedures which, when performed carelessly, have contributed to the increase of staphylococcal infection in hospital."4 Though Koprowski accepted Lederberg's notion that the "germ-free man" could "become less of an abstraction" in the future, he doubted a germ-free world was possible because the "the greatest danger of upsetting the equilibrium between man and his bacteria lies in anti-bacterial drug therapy . . . and in attempts to eradicate infections."5 A germ-free world would radically impair the immune system, making a single microbe deadly. A better strategy, Koprowski suggested, would be to "implant man with a known concoction of living infective agents under controlled conditions rather than let him go germ-free into the world."6 Whereas Lederberg thought a germ-free world to be an interesting possibility, Koprowski saw the idea as a threat to the future of man.
In post-Second World War medical, scientific, and popular discourses, germ-free life was a prominent topic of discussion, catalyzed in part by the advent of antibiotics. Antibiotics, in the words of Sir Macfarlane Burnet, promised the "virtual elimination of infectious disease as a significant factor in social life."7 Yet, as these words were written, many bacteriologists knew that the overuse of antibiotics risked the creation of new virulent and deadly bacteria resistant to these drugs.8 In any case, it was not through antibiotics that germ-free life was created. The modern concept of germ-free life emerged in the late nineteenth century concurrent with the development of bacteriology. By the 1960s germ-free life had long featured in the Anglo-American imagination and had begun to appear ever more regularly in the medical, scientific, and popular press, often represented futuristically entwining fact and fiction. There was only the slightest hint of playfulness when Dr. Charles Philips, of the Walter Reed Army Institute of Research, suggested that the space race may require "germfree men to explore space. . . . All we have to do is keep a man in a germfree cabinet for some 25 years following birth, meanwhile teaching him how to fly a spacecraft."9 Long before images of the earth taken from space reinforced the idea that the planet formed a closed environmental system, scientists such as Joshua Lederberg had recognized any extraterrestrial venture risked introducing terrestrial microbes to space and extraterrestrial microbes to earth with potentially devastating consequences in either case.10 As they were translated into the public imagination, potential risks became global threats. The Andromeda Strain, for example, narrated a fictional fight against a deadly and apparently unstoppable extraterrestrial pathogen introduced to earth as a consequence of man's exploration of space. Written by the medically qualified novelist Michael Crichton, the story was cast in a nonfictional style accurately incorporating many of the latest innovations in biomedical technology including those for creating microbially isolated environments necessary for the creation of germ-free life.11 By the close of the 1960s, these microbially secure worlds had began to appear in hospitals where members of the public might encounter them and, if unfortunate, find themselves living within. The development and subsequent adaptations of germ-free technologies for medical and veterinary uses forms the subject of this article.
Central to the historical development of post-Second World War health provision was the building of productive relationships across the laboratory-based sciences, clinical medicine, and corporate industry.12 The development and application of new technologies was a vector of closer integration across these diverse sites.13 Success, in this context, required technologies to operate as what Griesemer and Leigh Star have described as "boundary objects," which operate to allow different social worlds to communicate while simultaneously marking disciplinary territories. Boundary objects facilitate the building of material and social cultures by enabling the transmission and integration of practices across different sites of use. They achieve this by being robust enough to maintain a purposeful identity yet flexible enough to be adapted to local purposes.14 Boundary objects provide the basis for the construction of social alliances and interest groups, as Thomas Schlich has shown in his study of ostero-synthesis.15 The historical trajectory of germ-free technology, however, does not follow a narrative of successful innovation. On the contrary, these technologies failed as boundary objects. In order to explore why germfree technology could not establish itself at the majority of sites at which innovations were attempted, this article traces what could be termed a technological "biography." In recent years historians have embraced biographic narrative as a means to explore disease histories within historical and cultural contexts, though not without objections.16 Roger Cooter, for example, warns against the use of biography as an ordering device for the historical study of disease as it assumes an essentialist view, obfuscating the specific cultural and epistemological frames that made the construction of specific diseases possible.17 As technology is always already assumed to be artifice, this critique should not deter the pursuit of biographies of medical technologies.18 By tracing the life of germ-free isolators chronologically, across various sites of application, this article explores the wider cultural and epistemological frames that sustained and restrained their use. Placing germ-free technology at the center of analysis will show the difficulty of claiming it to have been definitively a success or a failure. Rather, the ideal of germ-free life enjoyed differing levels of support and application in accordance with contingent geographic, historical, and cultural factors within and without medicine.
The basic principles of germ-free technology were perfected in the 1940s by James Arthur Reyniers (1908-67) and Philip Charles Trexler (1911-) working at the University of Notre Dame, Indiana (USA). This article begins by locating the emergence of the concept of germ-free life in early-twentieth-century bacteriology and the popular imagination before addressing the perfection of germ-free isolators for use in the creation and maintenance of germ-free laboratory animals in the 1940s. It then examines how Reyniers and Trexler sought further applications for their technology at a variety of sites and across several professional and disciplinary boundaries. Germ-free techniques were applied, for example, to prevent cross-infection in the maternity ward and in general hospital wards as well as in the operating theatre. Germ-free technology was also applied within industrialized farming to create herds free of those pathogens thought to retard growth and as an aid to veterinary medicine. Notoriously, germ-free technology was utilized to protect immunocompromised babies at birth, thereby creating the first germ-free humans. Though germ-free technology traveled across the laboratory sciences, clinical medicine, veterinary practice, and industry, it failed to become widely embedded outside the laboratory. That germ-free technology worked was rarely questioned. Working, however, was not enough to ensure successful integration into existing practices. Reconstructing the historical development of this technology reveals the labor and difficulty involved in the work of aligning diverse and contingent cultural, societal, and material factors, necessary for successful medical innovation. Studying how, why, and to what consequence germ-free isolators, outside the laboratory, remained a peripheral technology always in search of application, contributes to understanding our increasingly technologically dependent contemporary health care.
Germ-Free Cultures
For its proponents, germ-free technologies had significant societal worth as they believed the eradication of germs would produce fitter, healthier, and longer living forms of life. Such technologies would find applications in areas from agricultural production to health care. This confidence, however, was far from universal. When Louis Pasteur discussed the question in 1885, he gently chastised the work of his friend Emile Duclaux, who sought to create a strain of beans completely isolated from all other forms of life. So-called "pure cultures," Pasteur felt, were impossible to realize because certain microbes were necessary for complex forms of life to exist. Whether microbes were entirely detrimental or in some ways necessary to the health and well-being of higher organisms became a question of heated debate among bacteriologists in the early decades of the twentieth century. Max Schottelius, for example, working at the University of Freiburg, undertook experimental investigations intended to demonstrate that microbes played an essential role in maintaining the health of chickens. At the University of Cambridge, in contrast, George Henry Falkiner Nuttall raised germ-free guinea pigs in order to substantiate the claim of Wilhelm Marceli Nencki that microbes were entirely detrimental to health. Conversely, at the Institut Pasteur Elie Metchnikoff and Michel Cohendy produced germ-free chickens and guinea pigs that appeared to thrive. Claims and counterclaims orbited about the reliability of the early technologies and material practices that had enabled the production and maintenance of germ-free animals in each case. Nevertheless the promise of germ-free living, particularly when the meaning of "purity" was detached from its restrictive scientific definition, quickly captured the public imagination. The work of Metchnikoff and Cohendy, for example, was extensively reported in the international press and interpreted to mean that germ-free life was not only possible but beneficial.19 When Cohendy reported that his germ-free animals grew quicker and larger than conventional animals, the New York Times quickly concluded that future "children may acquire stronger constitutions by similar treatment."20
By the 1920s, long before antibiotics, the ideal of germ-free living was well established as a characteristic of the imagined future. In her 1926 dystopian novel, Charlotte Haldane, for example, presented a future society dominated by male scientific rationalism which had perfected the ectogenetic creation of "aseptic cows . . . free from all harmful bacteria" and intended to apply the same techniques to human children.21 In a different vein, Francis Flagg's 1927 short story "The Machine Man of Ardathia" described a time-traveling historian from the future who existed within a crystalline cylinder without which "he would perish miserably" as it "protects him from the actions of a hostile environment."22 In this future, germs had been found to be the cause of all disease and aging; consequently, "man's bodily advancement lay on and through the machine."23
Historians have conventionally focused on how such narratives reflect interwar concerns over ectogenetic technologies of reproduction and eugenic manipulation of the "germ line" (as vividly described in Aldous Huxley's Brave New World). Thus Susan Merrill Squier has argued that the machine man's crystalline tube "anticipates the incubator used in in-vitro fertilization in the mid 1980s."24 Such focus, however, obscures both the prominence of the machine man's dependency on germ-free isolation and his possession of key characteristics associated with germ-free life (e.g., perfect health and extended life span).25
Of course there is no reason (beyond historiographical framing) to assume a strong distinction between the logics governing bacteriology and reproduction. Eugenic philosophies, for example, operated in large part through the metaphorical appropriation of language and logic drawn from bacteriology. This was facilitated by the word germ itself, carrying meanings for both biological hereditary (the germ plasm) and bacteriology (the germ as pathogen).26 Considerable interpretive flexibility existed in terms such as "purity," which consequently operated in a value-laden way across the discourses of bacteriology and eugenics. Practices of manipulating the heredity "germ line" as well as the eradication of potentially
Figure 1.
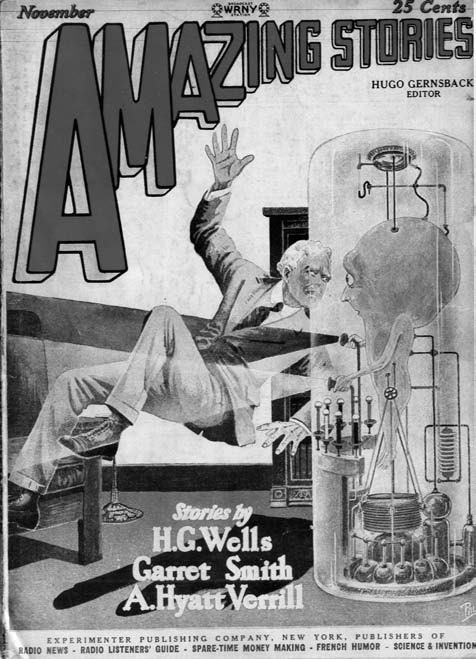
Francis Flagg's "germ-free" machine man of the future. Source: Amazing Stories, November 1927.
© Frank R. Paul Estate. Reprinted with permission.
pathogenic "germs" were both mobilized to serve the eugenic agenda of improving the quality of existing forms of life. Though eugenics is conventionally associated with the former, the latter might be equally as important in building a fuller understanding of what was at stake in such debates.27 Indeed, a sharp differentiation between hereditary and infection became extensively established only after 1945 with the routine use of antibiotics to combat epidemics.28 Be this as it may, the world did not have to wait until AD 16,000 for the first germ-free human as Flagg had imagined. Over the subsequent three decades all manner of nonhuman species were born into germ-free worlds, culminating in the birth of the first germ-free human.
Germ-Free Life in the Laboratory
The phenomenal proliferation of germ-free life was largely possible due to the development of robust technologies for germ-free isolation developed by James Arthur Reyniers and Philip C. Trexler.29 In 1930, during his final year of an undergraduate degree in microbiology at the University of Notre Dame, Reyniers, at twenty-two years of age, made a series of deductions that were to shape his career. Life was too varied to lend itself to experimental enquiry as it stood, and so it would have to be simplified through the use of new technologies capable of routinely isolating single cells. If the basic unit of biology were the cell, Reyniers reasoned, bacteriology would progress only if single cells could be isolated and maintained in isolation during experimental investigation.30 Reyniers's thinking derived from his formative experience of engineering workshops owned by his father, Leo A. Reyniers, the proprietor of a Chicago-based instrument and tool company. Reyniers pursued biological simplification through engineered mechanization and standardization, applying engineering principles to what he perceived to be the needs of bacteriology.31 Yet his early mechanical systems for establishing cells as pure cultures were frequently undermined by bacterial contaminants.32 Reyniers therefore built a second form of isolator system, designed to maintain isolated cells in secure microbial environments.33 This latter innovation was to make his name, providing the technology that facilitated the growth of germ-free science during and after the Second World War.
Philip C. Trexler, a recent microbiology graduate at Notre Dame, was appointed as Reyniers's "biological apprentice" in 1932. The first four years of this "apprenticeship" was spent in the machine shop of Reyniers's father's firm, Reyniers & Sons of Chicago, where Trexler learned engineering "on the job" while developing ever more robust versions of germ-free isolators. Reyniers was fiercely proud of his family background; his claims to expertise consistently drew on his experience in mechanical engineering as opposed to academic qualifications in microbiology or bacteriology.34 He wanted Trexler not only to share his engineering approach but also to understand its heritage. Reyniers understood his work to be the application of engineering expertise to produce innovative solutions to biological and biomedical problems, a field he called "biological engineering."35 The major product of this approach was the "Reyniers Steel Isolator System," perfected by the early 1940s and capable of maintaining an entirely germ-free environment. This isolator consisted of an airtight metal cylinder fitted with windows, inlet and outlet openings for ventilation, a supply inlet with integrated autoclave, various high-pressure steam mechanics to allow the internal environment to be sterilized, and integrated rubber gloves to allow users to work with the contents within.
The breeding of germ-free animals had began slightly earlier, in the mid-1930s, as a means to first test and then monitor the microbial security of the prototype isolators. By the mid-1940s, however, Reyniers had come to believe that germ-free animals were an end in themselves. By amalgamating the very different roles standardization played in engineering, the experimental sciences, and the bacteriological logic of "pure cultures," Reyniers developed a unique philosophy of science based about
[t]he need for isolating "pure units" from the natural complex in which they exist forms the basis of analysis . . . [w]hether these pure units are compounds, physical particles, bacteria, animals, or mathematical symbols does not alter the philosophy.36
Figure 2.
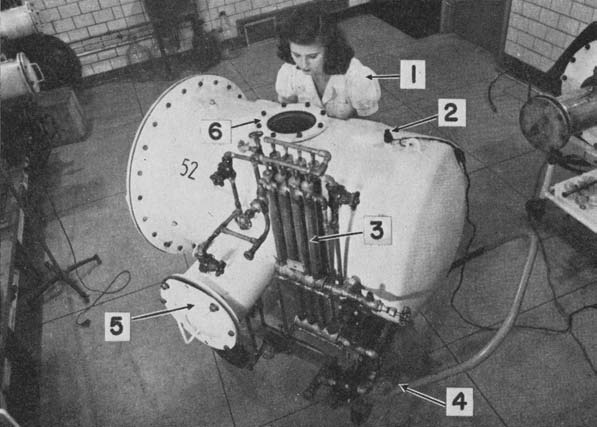
Reyniers's isolator; (1) technician, (2) electrical outlet, (3) air outlet, (4) mobile truck, (5) entrance/exit autoclave, (6) viewing port. Source: J. A. Reyniers, P. C. Trexler, and R. F. Ervin, "Rearing Germ-Free Albino Rats," LOBUND Rep. 1 (1946): 1-84, 5.
© University of Notre Dame. Reprinted with permission.
Unlike all other forms of life, whose microbial loads and histories could not be known, the germ-free animal was free of all microbes.37 Thus germ-free animals were "pure units," pathogenically standardized, and therefore—in Reyniers's view—ideal basic experimental tools. Reyniers consequently began to focus on the mass production of germ-free animals with the intent of supplying them for use as standardized experimental tools. Work began with the most commonly used small mammals, mice, rats and guinea pigs, before being extended to larger animals including cats, dogs, and monkeys.
Manufacturing germ-free animals combined the ability of the uterus to protect the young within a sterile environment and the capacity of germfree isolators to maintain them in that state. The process of engineering biology and machine began by removing intact uteruses from near- to full-term pregnant animals within a purpose-built germ-free "surgical isolator." The uterus was subsequently passed through various disinfection procedures, involving total immersion in germicide-filled "dunk tanks," before the progeny were surgically released and hand reared within a second microbially sterile isolator. Animals were born in this way within a sealed world in which they would never encounter a living organism other than their own species. Creating germ-free life was not, therefore, an ectogenetic procedure, yet was nevertheless a complex process requiring extensive trial, error, and innovation. Different species, moreover, presented different needs, posing subtly different challenges. Gestation periods, for example, had to be relearned for each species with any error proving fatal as progeny were more likely to survive the decontamination process when surgery was undertaken close to the time of "natural" birth. New husbandry techniques, particularly for hand rearing "preborn" animals, also had to be developed for each species. Nutrition proved particularly challenging, as sterilizing food without rendering it poisonous or destroying its nutritional content was difficult, as was assessing the nutritional requirements of species. Nevertheless, the creation and subsequent mass production of germ-free animals was achieved with remarkable speed.
By the early 1950s Notre Dame had become a must-visit location for biomedical scientists interested in germ-free techniques, while the promise of germ-free life had captured the American imagination. The uniqueness of Reyniers's technology led to government and private money flowing into Notre Dame culminating in the establishment of the Laboratories of Bacteriology, University of Notre Dame, or "LOBUND Institute," under Reyniers's directorship in 1946.38 Reyniers had greatly benefitted from the Second World War due to the utility of his germ-free isolators for biological warfare research. By reversing the isolators so that they protected those without from the dangerous pathogens within, Reyniers accessed substantial military investment.39 The use of isolator systems for biological warfare was obscured by a blaze of publicity after the close of war that served to reassociate his technology with germ-free life and the familiar future-orientated promise of health and longevity.40 Presenting germ-free life as an essential new tool for the fast-expanding biomedical sciences was a deliberate strategy adopted by Reyniers intended to integrate his work with the promise of future improvements in health and well-being. In the laboratory, germ-free life promised new understandings of aging as well as providing the vehicle by which new treatments would be discovered for diseases as diverse as tooth decay and cancer, promising healthier, happier, and longer futures for all.
Building Better Babies: Isolators in the Nursery
Reyniers did not limit his interests to the material cultures of the biomedical sciences. On the contrary, he believed isolator technologies could find application across "industry, hospitals, research laboratories and various specialists."41 In the late 1930s, the question of whether air could serve as a vector by which infections were spread resurfaced in medical discourse. So-called "air hygiene" subsequently became a prominent field of medical interest. The Medical Hygiene Unit of the British Medical Research Council (MRC), for example, undertook innovative investigations of the bacterial contents of air in part responding to Second World War fears of epidemics emanating from crowded air-raid shelters in cities whose infrastructure had buckled under aerial bombing.42 Similar moves occurred in America, where cross-infection within densely populated sites such as the nursery, school, and hospital increasingly came to be problematized through reference to air hygiene.43 The study of air hygiene, or "aerobiology," necessitated the mapping of microbial pathways across complex processes such as the physics of droplet atomization, the physiology of inhalation, and the biochemical and physiological activities of the body. To meet this challenge, multidisciplinary expertise was required from physics, engineering, bacteriology, chemistry, biochemistry, biology, physiology, and medicine. Such complexity well suited Reyniers's "biological engineering" approach, which cut across complexities through engineered standardization and mechanization.
Air hygiene could be considerably simplified, in Reyniers's view, as it was accepted that the "prevention of cross infection involves only one principle—physical isolation."44 This, of course, reflected Reyniers's work on mechanical isolators and germ-free life and enabled Reyniers's isolation techniques, such as food sterilization, filtering of air, the use of disinfection tanks and autoclaves, and the curtailing of direct contact between living organisms, to be translated to new uses and sites. However, adapting existing practices from animal to human, laboratory to hospital, was far from straightforward because it required a loosening of rigor.45 Nevertheless, even with this sacrifice, Reyniers believed cross-infection could be considerably reduced across a range of medical sites.
The maternity ward was an ideal location to begin such work as cross-infection was a recognized problem and the behavior of babies was easier to predict and control than that of adult patients. Nevertheless, the work of establishing the extent to which laboratory principles would have to be weakened was complex because it was "a clinical problem involving nursing skill." Recognizing this led Reyniers to work directly with intended users, beginning with The Cradle, an adoption agency with its own on-site nursery established in Evanston, Illinois. The result of this collaboration was the "Reyniers Baby Cubicle," consisting of a far section occupied by the baby and an immediate section used by nurses (and other visitors) who donned "flexible sheath barriers" consisting of sterile gowns, masks, and gloves before entry. The two sections were separated by a closed glass "delivery window" through which nurses' forearms could enter the baby section to care for the child.46
With temperature and humidity monitored, and each section of each cubicle having its own regularly cycled filtered air supply, the newborn's environment was meticulously controlled. Maintaining air pressure in the newborn section at a higher than normal rate ensured air could flow only outward, further preventing cross-infection. Food and other essentials were prepared in a sterile "work cubicle" that adapted principles and practices from the "Reyniers Germfree System" for hospital use. A prototype cubicle was rigorously trialed with guinea pigs, allowing for deliberate attempts to break the microbial barrier before being used with human newborns. In both cases, the cubicle was found to entirely eliminate cross-infection.47
Figure 3.
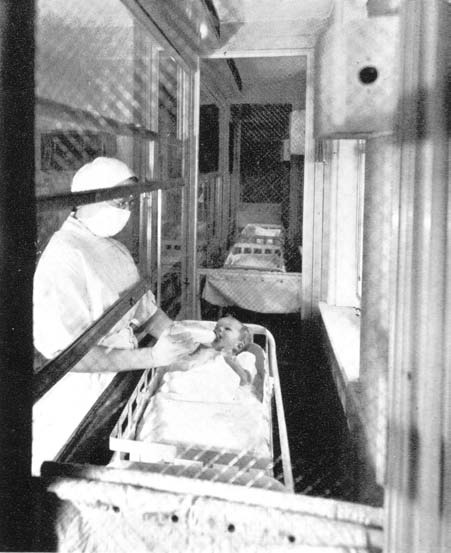
Reyniers's Baby Cubicle. Source: I. Rosenstern and E. Kammerling, "Air Conditioning, Ultra Violet Light, and Mechanical Barriers as Factors in the Prevention of Cross Infections in Nurseries," in Micrurgical and Germ-Free Techniques: Their Application to Experimental Biology and Medicine, ed. James A. Reyniers (Springfield, Ill.: Charles C Thomas, 1943), 233-59, 241. Reprinted with permission.
A significant difference between Reyniers's Germ-free System and the Baby Cubicle was the extent to which the quality of lived experience became an explicit consideration. Soundproofing was installed, for example, as the air filtration system was found to disturb occupants, which brought the extra benefit of isolating individual babies' cries. Initially, no consideration had been given to the impact of curtailing interaction. This oversight was in part a consequence of the fact that The Cradle housed only babies given up for adoption, thus there was no parent desiring to interact with his or her child. In a conventional hospital, long-term separation of parent and child would not have been practical, and so Reyniers designed an air filtration carry case to allow the transportation of babies. Reyniers, in any case, believed that the social isolation endured by this system was of no consequence as "that kind of neighboring has no social value during the first few days of a baby's life."48 Such reasoning would soon be questioned by those such as John Bowlby and later Harry Harlow, who placed new emphasis upon the importance of parent-child bonding.49 Perhaps for this reason, Reyniers's Baby Cubicle was not widely institutionalized. Moreover, it was expensive and required far more space, time, and effort than conventional practices. Nevertheless, as with other fantastical machines created by Reyniers, the concept achieved a public profile far beyond its actual usage. In March 1947, for example, Mechanix Illustrated, styled as a popular "how to do magazine," reported how one reader had adapted Reyniers's principles to build a "temperature and humidity controlled, dirt-free . . . glass house" with "built-in air filter." Within this "showcase," the baby "doesn't catch cold" and "visitors can't pass their germs through the class." Furthermore, sound proofing allowed the baby to "bellow without straining the family nerves."50 This do-it-yourself approach is indicative of how the public perceived the benefits of microbial isolation, as well as the technology's influence on the public imagination. Even the behaviorist B. F. Skinner was taken by the concept, building a similar device for his daughter that he called the "Baby Tender," which inspired a similar device known as the "Air Crib" to be commercially developed and marketed.51
Proliferation through Plastic: Isolators in the Hospital
By the late 1950s Reyniers and Trexler had arrived at fundamentally opposed views on the best way to promote germ-free technology. Their disagreement lay in the production of laboratory animals. Reyniers wished to retain full control over his steel isolator systems, envisioning a model of centralized animal production supported by the federal government "in much the same way as the large astronomic laboratories and centers for nuclear physics." Trexler, in contrast, believed the production of germfree animals should "be made simple and relatively inexpensive so that research could be carried on in any laboratory," and set out to provide a rival means of producing germ-free animals using plastic instead of steel.52 Intended to be simple, adaptable, and affordable, what came to be known as the "Trexler Plastic Isolator" was "designed with an eye to economy and mass-production." By 1957, Trexler was publically demonstrating his work, which could be manufactured at one-tenth of the cost of Reyniers's steel model.
The plastic film used by Trexler also offered vastly improved visibility, allowing more complex work to be attempted, while the prioritizing of economy, simplicity, and adaptability underlined the sharp contrast to Reyniers's steel design. These qualities suggested there was potential for adapting plastic isolators for use in the hospital at sites where the expensive, unwieldy, and inflexible steel isolator would have been impossible, most obviously in the control of cross-infection.
Well after the widespread adoption of antibiotics, airborne bacteria remained a prominent hospital concern.53 The British bacteriologist J. C. Gould, for example, believed that microbial contaminants in the air could explain the continued prevalence of cross-infection, postoperative infection, and the growing problem of antibiotic-resistant bacteria in hospitals.54 Prolonged ever deeper surgical innovations, such as hip replacement, also focused attention upon air hygiene. In 1966, John Charnley, the British pioneer of hip replacement, turned to industrial expertise to construct a clean air operating system.55 Charnley combined laminar air
Figure 4.
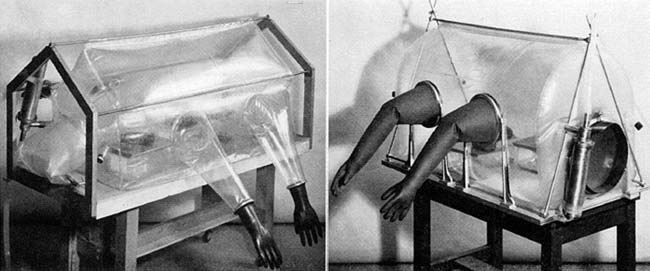
Early Trexler isolator. Source: P. C. Trexler and L. I. Reynolds, "Flexible Film Apparatus for the Rearing and Use of Germfree Animals," Appl. Microbiol.5 (1957): 406-12, 407.
© American Society for Microbiology. Reprinted with permission.
ventilation with a "body exhaust system" intended to prevent microbes carried by surgical staff from entering the patient.56 That postsurgical infection remained a major hospital problem is indicated by the variety of approaches employed to establish so-called "sterile" environments.57 Traditional cleansing and disinfection procedures were combined with innovations in clothing design, the use of ultraviolet light, the control of air flow, air filtration, and even the aerial release of antibiotics.58 All this operated through the Listerian logic of reducing the background bacterial load of the environment. Importantly, this logic left the barrier between normal and sterile environments undefined, making it "very difficult to evaluate . . . because of the dependence upon good barrier nursing techniques" and the voluntary cooperation of the human agents involved.59 Comparisons of the efficacy of different approaches were therefore highly contestable. The hospital environment, being made up of a multitude of local disparate routines, practices, and technologies, was too complex to consistently control and evaluate. This situation, however, made the hospital a perfect location to apply isolator technology, which had originally been developed to simplify and standardize laboratory practices across diverse localities.
In 1958 Trexler began working with Stanley M. Levenson, at the Albert Einstein College of Medicine (New York), exploring how germ-free isolators could be adapted for hospital use. It seemed "practical to transfer the technics of the germfree laboratory to the care of patients," Trexler wrote, "since we were operating in a sterile environment routinely in the laboratory to obtain germfree mammals, we ought to be able to operate on man in a sterile environment."60 Adopting the then voguish language of cybernetic systems theory, Trexler explained how isolators were superior to existing practices because they operated via "closed systems," isolating individuals within their own microbial environment. This was a "fundamental difference in concept" because the closed system relied upon a simple microbial impervious barrier and not a series of steps to reduce the environmental contamination to which patients were exposed.61 A plastic isolator established a microbial barrier which, being material, could be passed only via mechanized, rigorous, and unavoidable decontamination regimes. This contrasted with the Listerian "open system," which relied on adherence to decontamination routines that were difficult to enforce and easily ignored. Reyniers's steel isolators, of course, could never have been utilized in the hospital setting. The expense of a man-sized steel isolator was prohibitive, and, in any case, they were impractical for human surgery. The porthole design restricted the vision of the operating team, while the unwieldy gauntlets inhibited movement. Trexler's plastic isolator, however, was comparatively cheap, entirely transparent, easily adaptable, and flexible enough not to hamper the actions of the surgical team and, in an emergency, could be removed in seconds.
In 1962 Trexler moved from Notre Dame to Albert Einstein College in order to investigate "the possibility of translating the technique of the germfree laboratory to the hospital operating room."62 The main innovation in the prototype human isolator was the substitution of gauntlets for a bodysuit encapsulating the surgeon's upper body.63 This was intended to replicate the "feel" of being entirely within the surgical environment, allowing the operating team to work "naturally" while never crossing the secure barrier.
Presterilized surgical equipment placed within sealed plastic bags could be glued to the outside of the plastic isolator and accessed internally by slicing through the isolator, allowing the bag to maintain the microbial barrier. With the exception of scale, most other features mirrored that of laboratory isolators. Thus filtered air was maintained at pressure slightly higher within than without, ensuring accidental air transmission would be outward. The prototype, developed at the Bronx Municipal Hospital using large laboratory animals (dogs), was demonstrated to successfully exclude "[a]ll exogenous microorganisms" from the surgical environment.64 Furthermore, as the plastic barrier of the isolator was disposed of after each procedure, there was no build up of microbial contamination over time. By 1964 the isolator was in regular use and postoperative infections had fallen from 14.6 percent to 3.8 percent.65
Trexler was keen to apply his isolation technology more generally, for example in hospital wards to protect "those patients highly susceptible to infections" and prevent "cross-contamination when infections already exists."66 Against the background of mounting concerns regarding the indiscriminate use of antibiotics and the incremental rise in antibiotic resistant infections within hospitals, Trexler and his collaborators believed isolators could serve as alternatives to prophylactic antibiotics.67 Initially, enthusiasm for the isolator appeared to bear out this hope. A number of commercial producers began developing and marketing versions of
Figure 5.
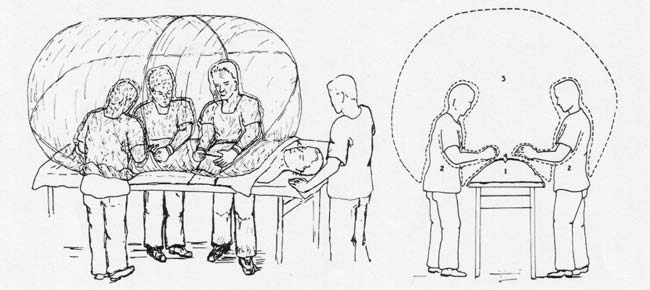
Sketch of a plastic surgical isolator. Left: Operating on a man in a plastic isolator. Right: Head-on view of surgical isolator illustrating basic principles; (1) patient's body, (2) surgical team, (3) sterile environment, (4) wound. Source: S. M. Levenson, P. C. Trexler, O. J. Malm, M. L. LaConte, R. E. Horowitz, and W. H. Moncrief, "A Plastic Isolator for Operating in a Sterile Environment," Amer. J. Surg.104, no. 6 (1962): 891-99, 894.
© Elsevier Limited. Reprinted with permission.
Trexler's technology, which was possible because the development of medical isolators at the Albert Einstein College had in part been funded by the National Institutes of Health, which insisted patents deriving from its support be placed in the public domain.68 Reyniers, in contrast, had ensured, regardless of fact, that patentable technologies were attributed to funding received from the Department of Defense, as it allowed patents to be retained by the grantee. Consequently, Reyniers had complete control over his "steel" isolators (exclusively manufactured by his father's Chicago company). In part, the absence of protection served Trexler's aim to promote the use of isolator technology. However, the gradual expansion of users led to the proliferation of approaches to the design and use of plastic isolators, making consolidation about agreed standards difficult to negotiate. Moreover, the simplicity of design destabilized Trexler's claim to expertise. Lacking the means of control that patents would have allowed, Trexler instead turned to history in order to bolster his claim to expertise and to distinguish his work from that of others. Increasingly, Trexler rhetorically located himself within the seventy-five-year history of germ-free science, stretching from the late nineteenth century to its perfection at Notre Dame.69 In doing so, he emphasized (and thereby established) his credibility on the basis of three decades of personal hard-won experience. This narrative also relocated the technology as the basis of a newly emerging science of "gnotobiotics." The perfection of isolators, Trexler believed, had enabled organisms or all kinds, up to and including the human, to be defined in terms of their microbial loads. This promised a new approach to biomedicine, where known (gnoto) life (bios) could be studied in controlled isolation.
In 1962 Trexler established the "Association for Applied Gnotobiotics" to provide a professional identity for those who worked with isolators and, importantly, institute standards for the fast multiplying technologies located at a variety of sites.70 In 1964 Trexler became "Director of Research" in two companies: Charles River Breeding Laboratories (Boston, Mass.) and Snyder Laboratories (Dover, Ohio), leading specialists in the production of laboratory animals and clinical technologies, respectively.71 At Charles River, Trexler established methods of producing and supplying pathogenically standardized laboratory animals; at Snyder, he oversaw the development of isolators for hospital use.72 Charles River applied isolator technology to eradicate known pathogens in animal stock and thereby produced high-quality animals of reliable health. Here, Trexler was essentially working with the intended user of his plastic isolators. The collaboration helped establish Charles River as a leading global supplier of laboratory animals.73 Establishing hospital isolators, however, was not so straightforward.
In part this was because Trexler was now working with a technology supplier, not the end user; the latter remained critically undefined due to the plurality of demands and disparate regimes of practice found in hospitals across the United States. He was further hampered by the myriad of different companies developing what appeared to be essentially the same technology. Some firms, such as Plastifab (Columbus, Ohio), embraced the flexibility of plastic isolators to such an extent that rather than offer models for specific purposes, they manufactured and supplied a variety of parts providing for "the ever changing needs" of users who wished to deploy their own "gadgeteering skill" to answer highly localized problems.74 The main rival to Trexler's isolator, however, was a similar product produced by Mathews Research Inc. (Alexandria, Va.). Marketed as the imaginatively named "Life Island," it was the first hospital isolator to capture the public imagination.75 The Life Island was often applied to protect patients whose immune systems were severely compromised, such as in cases of childhood leukemia or as a general consequence of chemotherapy, where antibiotics alone were insufficient. It also found use in cases where a body was severely burned and thus open to infection. However, the simplicity and adaptability of the plastic isolator, which facilitated its widespread adoption in laboratories, worked against the establishment of standards in the hospital environment. Lacking a unified market, or a standardized product, it proved difficult to establish hospital isolators particularly in the face of its major competitor: prophylactic antibiotics. Consequently, there were no assessments of isolators on a scale that could rival clinical trials of antibiotics, for example, which were highly standardized, superficially simpler to administer, and vigorously commercialized.76
Perfecting the Pig: Gnotobiotics on the Farm
Obstacles to the institutionalization of hospital isolators in the United States informed Trexler's willingness to move to Britain when invited by the veterinarian Alan Betts to establish gnotobiotic facilities at the Royal Veterinary College (RVC) in 1966. In Britain there was only one customer for hospital isolators that mattered—the National Health Service (NHS)—which promised a much easier route to standardization and institutionalization. Trexler's immediate work, however, was to apply isolators to veterinary practice. Betts, professor of veterinary microbiology at the RVC, was anxious to develop gnotobiotic technology in Britain as
Figure 6.
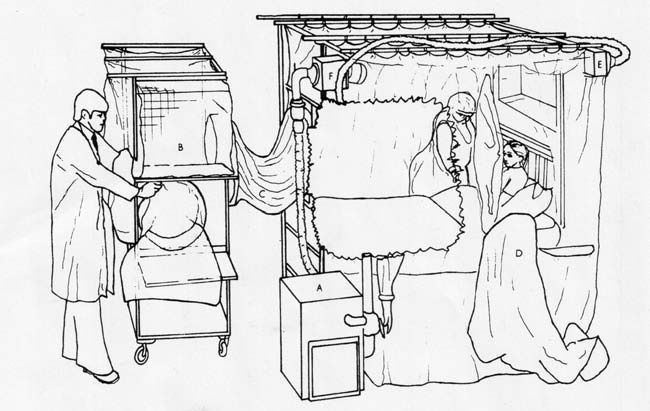
Containment bed isolator showing a patient in bed, a nurse in a half-suit, and the entry port on the supply trolley in use; (A) air supply unit, (B) supply trolley, (C) attachment sleeve, (D) half-suit, (E) supply air filter, (F) exhaust air filter. Source: P. C. Trexler, R. T. D. Emond, and B. Evans, "Negative-Pressure Plastic Isolator for Patients with Dangerous Infections," Brit. Med. J. 2 (1977): 559-61, 560.
© BMJ Publishing Group Ltd. Reprinted with permission.
part of a wider attempt to modernize the college as a research-orientated institution.77 One of the many atypical features of germ-free life was that it exhibited similar patterns of increased growth to that of animals dosed with antibiotics. This suggested that the so-called antibiotic "growth effect" had less to do with antibiotics per se than the removal of growth-inhibiting intestinal flora.78 By the late 1960s agricultural usages of antibiotics was highly controversial, again presenting an opportunity for gnotobiotic technology to offer a credible alternative.79 Trexler's plastic isolators were first applied to farming by George Young at the University of Minnesota (later University of Nebraska), who adapted gnotobiotic principles to create pig stocks free of growth-retarding pathogens.80 Working with volunteer farmers, Young refounded pig stocks as "specific pathogen free" (SPF).81 A farm site was evacuated of animals, rigorously disinfected, and left empty for at least six weeks, after which new isolator-derived stocks were transported to the now "sterile" farm.82 Though not without its problems, Young's "swine repopulation program" improved efficiencies of production and eradicated common diseases and parasites.83 When Young died unexpectedly in 1964, the "National SPF Swine Accrediting Agency" was established to continue his work (which continues to campaign for the wider adoption of SPF animals as an alternative to routine use of antibiotics).84 Betts was much impressed by Young's work, which he encountered when traveling on a Commonwealth Fellowship in 1960. He was convinced a similar system would be successful in Britain, where intensive pig farming was more organized.85 In a reversal of the "brain drain," Trexler was enticed to Britain by the promise of new sources of state/industrial funding supporting the development of his isolators for use in veterinary and human medicine.
Despite the complete absence of the necessary technical expertise to build, maintain, and develop plastic isolators at the RVC, Trexler had established facilities to produce SPF piglets within months of his arrival.86 Attempts to replicate the American swine repopulation program met with mixed results, however, with some farms reporting improved production efficiencies while others encountered problems with infection and difficulties in meeting the nutritional requirements of the faster-growing SPF pigs.87 To investigate these problems, Trexler installed enormous isolators at the RVC capable of maintaining farm animals in a permanent germ-or specific-pathogen-free environment so as to allow for their prolonged study.88 Betts and Trexler subsequently examined the role of various gut microbes in growth and general health, as well as the relationship between human and swine respiratory infections among other questions of comparative medicine.89 This work is indicative of Betts's broad interest in comparative medicine, which, in later decades, led him to call for a rapprochement of veterinary and human medicine under the banner of "one medicine." Consequently, Trexler's desire to develop isolators for use in human clinical medicine was perfectly compatible with Betts's understanding of the relationship between human and veterinary medicine.
Hemorrhagic Diseases: From Prevention to Protection
Any hope that antibiotics had made infectious disease a problem of the past had evaporated by the early 1970s with the arrival of new and deadly hemorrhagic diseases. One of the earliest was Marburg or "green monkey" virus, first encountered when imported experimental monkeys infected their researchers in a German laboratory. This was swiftly followed by Lassa fever and Ebola.90 In early 1970s Britain Lassa fever acquired a reputation for virulence and fatality that gave it an importance far beyond the danger it was later found to pose (so much so that investigations were halted for a time due to safety concerns).91 The novelty of these diseases, all thought to emerge from foreign, largely African localities, inspired new fears that in a world connected by air transport the prevention of global pandemics had become impossible. Containment, therefore, became a central question for which gnotobiotic technology was perfectly positioned to answer. Since the 1940s isolators had been adapted to serve the purpose of containment within biological warfare research. In the early 1970s, against the background of growing fears over antibiotic resistant bacteria as well as the emergence of new and apparently highly infectious diseases from Africa, Trexler successfully obtained substantial state and industrial funding to adapt isolators for the purpose of microbial containment in hospitals, the former from the National Research and Development Corporation (NRDC), a state body established to promote and protect British innovation, and the Department of Health, and the latter from Vickers Medical Engineering Ltd.92
Trexler developed a prototype "containment isolator" from a design originally intended to protect patients with impaired immune systems. His experience derived from building the above sized farm animal isolators at the RVC was brought to bear as the containment isolator had to be large enough to provide comfortable living space given the potentially lengthy confinement periods.93
The new design was trialed at Coppetts Wood Hospital, London, with volunteer patients suffering from minor infectious diseases (usually chicken pox and hepatitis). Isolators had to be integrated within existing medical regimes, which were particularly complex as rather than their being an individual user there were multiple users: encompassing specialists, nursing staff, and the patient.94 The expectation of prolonged confinement placed new emphasis on the danger of isolation causing physical and psychological harm. The experience of volunteer patients was carefully assessed, with alterations made wherever possible to meet their needs. Substantial effort had to made to reduce noise caused by the air ventilator mechanism, for example, necessitating engineering innovations that later translated back to laboratory and farm isolators so as to reduce the stresses placed on animals housed within environments increasingly recognized to be "unnatural."95 In moves that reflected ethological efforts to enrich the environments of captive animals, everyday items such as newspapers, books, television, and radio were introduced to "normalize" the living environment. In 1976 the Trexler containment isolator at Coppetts Wood was successfully used for the treatment of a scientist accidentally exposed to the Ebola virus at the Ministry of Defence's research establishment (Porton Down).96 Subsequent publicity cast the isolator as the cutting edge of infectious disease control. Its capacity to provide robust microbiological security while facilitating close to normal clinical treatment saw it recommended to the NHS for the treatment of patients suspected to be suffering from hemorrhagic infections.97 The containment isolator, in sharp contrast to Trexler's other hospital applications, was uniquely successful.
Figure 7.

Patient's perspective. Source: National Archives of the UK, Kew, MH148/362.
© National Archives of the UK. Reprinted with permission.
Having learned how hard it was to alter entrenched hospital practices, Trexler worked to collaborate with British medical professionals. Users of the containment isolator were encouraged to report negative experiences, yet no difficulties emerged. Even the upper body suit design, which in all other contexts had been a focus of sustained complaint, in this case was universally reported to be "comfortable to wear."98 Indeed, British surgeons had so critiqued this feature that Trexler had removed the suit in his latest surgical isolator, returning to the gauntlet style originally developed for animal isolators. This, Trexler claimed, answered surgeons' criticism, while further enhancing economy and time-efficiency.99 Several studies confirmed the plastic isolator to be a cheap, simple, and efficient means to guarantee a surgical environment free of microbial contaminants.100 Nonetheless, the surgical isolator failed to attract widespread support, whereas the containment isolator was universally popular.101
Why was the Trexler containment isolator alone judged an efficient and practical addition to the British hospital receiving widespread endorsement? Though all plastic isolators deployed comparable technologies, one significant difference was in perceptions of risk. Where the patient was at risk, and despite every effort to simplify the isolator, it could not compete with antibiotic treatments that required little to no new expertise or alteration of established practices. Even though antibiotic treatment was known to be problematic, both for individual patient and in terms of antibiotic resistant bacteria, their ease of use, alongside significant corporate reinforcement, ensured they remained the treatment of choice. Only when the health of the medical professional was at risk, that is, when the patient's microbial load posed the threat, was the isolator successful in establishing itself as a necessary technology within the hospital.
In 1950, only 1,400 passengers a day passed through Heathrow and diseases such as Lassa and Ebola were unknown. By 1976, 100,000 people passed daily through Heathrow alone, with 2,000 of these arriving from Africa.102 With speculation abounding regarding what new foreign disease might follow Ebola, and on the back of a government enquiry having reported a dangerous absence of microbiological security in British laboratories, Trexler's containment isolator found a niche.103 Yet the widespread institutionalization of Trexler containment isolators within the NHS never materialized. In the early 1980s it became apparent that the virulence of Lassa and Ebola had been greatly exaggerated. Traditional methods of infection control were found more than adequate.104 Willingness to explore new uses for gnotobiotic technology in the hospital subsequently faded, this despite cross-infection remaining an entrenched problem. The final use for which Trexler adapted his technology was for postmortem. Here, isolators could protect the living from potentially hazardous pathogens of the corpse (with the additional benefit of curtailing nauseating odors). Yet, again, pathologists found little reason to change their established ways of working. Trexler's hope that it would "be commercially developed and made available to pathologists in the near future" never occurred.105 In 1986, Trexler published his last professional work on gnotobiotics, a lengthy survey of its use and future potential that reads as though he recognized that isolator technology would remain peripheral across the various sites he had traveled, at least until a microbial threat occurred to necessitate its adoption.106
The Boy in the Bubble
Isolator technologies found one further hospital application that, notoriously, established germ-free science in the public imagination of the 1970s: the creation of germ-free humans. This process literally translated laboratory practices to the hospital setting, simultaneously, albeit unintentionally, instigating a host of new bioethical problems. One of the earliest germ-free humans was produced by a team led by Ron D. Barnes, a clinical scientist based at the Institute of Child Health (London). Barnes was seeking a treatment for a recently identified inheritable condition that caused children to be born with dysfunctional immune systems.107 By combining the techniques and technologies of germ-free animal production with those of surgical and infection control isolators, Barnes worked to develop a means by which children suspected to have dysfunctional immune systems could be born into safe germ-free environments.108
Figure 8.
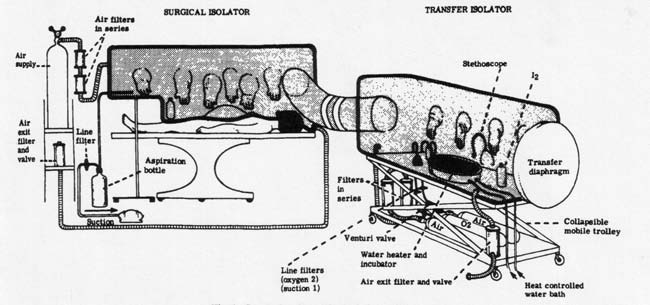
Surgical and transfer isolators. Source: R. D. Barnes, D. V. I. Fairweather, J. Holliday, C. Keane, A. Piesowicz, J. F. Soothill, and M. Tuffrey, "A Germfree Infant," Lancet 293 (January 25, 1969): 168-71, 169.
© Elsevier Limited. Reprinted with permission.
Trexler was consulted on the design of the isolator and advised on technicalities such as how to safely sterilize milk.109 Barnes and his team were aware that living in isolation was potentially damaging. In order to meet the child's presumed emotional needs, Barnes insisted that the father hold the child (via plastic gloves) within an hour of birth. Because interaction was possible without the use of face-obscuring masks, Barnes hoped the isolator might be less damaging to the formation of parent-child bonds than conventional barrier nursing.110 When the practice was trialed in 1968, the first child so born was found not to have the immune deficiency condition and was subsequently habilitated into a "normal" environment after a week of germ-free life. Nonetheless, the procedure was considered a success, and the birth of a germ-free human was widely reported in the medical and popular presses.111 Isolator birthing, Barnes claimed, represented the "ultimate in human environmental control" and promised that the "kitchen table could once again become the surgeons' workplace."112 Such hopes, however, were short-lived.
In 1971, at the Texas Children's Hospital (Houston, USA), Raphael Wilson, one of the earliest qualified "gnotobiologists" trained at LOBUND, used a similar technique with a child who was found to possess severe combined immune deficiency.113 The child, David Vetter, was to be confined within a germ-free environment his entire life. His story captured the public imagination, inspiring a movie starring John Travolta as The Boy in the Plastic Bubble (1976). Whereas Travolta's character was saved by a spontaneous recovery of immune function, Vetter, in stark contrast, died in 1984. His death, according to Time magazine, was "felt across the country."114 Though fiction was compelled to offer a happier ending than fact, it is notable that in neither case was success attributed to medical science. In reality, the original plan to obtain a bone marrow transplant and "kick-start" David's immune system proved impossible when his sister unexpectedly proved not to be a match. What had been envisioned as a temporary life isolated within a bubble quickly became permanent, leaving David, in the words of one article, "alive, well and waiting."115
In his short life David possessed many identities from medical marvel to laboratory animal to irresolvable bioethical problem. According to Reverend Raymond J. Lawrence, then chaplain of Texas Children's hospital, the
great scandal of the Bubble Boy was that he was conceived for the bubble. . . . The team . . . didn't consider what would happen if they didn't find an immediate cure. They operated on the assumption that you could live to be 80 years old in a bubble, and that would be unfortunate but okay.116
As the first human to develop in a germ-free environment, David became a unique and important research object.117 His experience was used to investigate how isolation produced cognitive abnormalities that hitherto had been inaccessible to researchers working with nonhuman animals. David was consequently found to possess greatly reduced spatial awareness that improved little when NASA provided him with a custom-built "space suit" intended to allow him to travel outside for the first time. The idea of limitless space confused and scared him. Uniquely, as time determined all activities that happened about him, David had developed a highly acute sense of time. It was time, not space, by which David had learned to orientate his world.118
Despite, indeed because of, his scientific utility, David posed an acute ethical problem. Without any means of treating David, the only viable option was to do nothing and hope his immune system would begin to work of its own accord.119 Within his isolator David was perfectly healthy, but he was dependent upon it to remain so. In an echo of fictional imaginings of germ-free humans, David was regularly reported as being physically and psychologically highly advanced for his age. The Association for Gnotobiotics Newsletter, for example, described him as "thriving . . . developing an intelligence far above the average and a maturity far beyond his years."120 Yet, for others, David was a new form of life in which the fictional dream of germ-free living had become a factual nightmare. For these, isolated as he was, David existed at the very limit of the human, a living exemplar of the threat posed by a medico-scientific "technocratic imperialism" in its pursuit of the "technical capacity to get the job done."121 Significantly, for those of this opinion, David himself complained that he "had been put into a cage and treated like a wild animal." Perhaps, had he been worldlier, he would have recognized, as many others did, that the animal he resembled was not wild but domesticated. The technology that had given David life carried with it its own history, a history that helped determine David's role as an object of scientific interest, comparable, if not directly akin, to the laboratory animal.
By the time David was twelve, new medical techniques had made the use of unmatched bone marrow possible, allowing him to receive a transplant from his sister. Within a few months David fell ill for the first time in his life. Quite undetected, the bone marrow transplant had contained the Epstein-Barr virus. After developing Burkitt's lymphoma, David died on February 11, 1984. In the same year LOBUND hosted the Eighth International Symposium on Germfree Research focused on "the life-prolonging germfree techniques used by doctors and researchers to care for David, Houston's 'bubble boy.'"122 Trexler was guest of honor, the University of Notre Dame choosing this occasion to award him an honorary doctorate in recognition of him being
principally responsible for the development of the plastic isolator systems which have had very important contributions to experimental and clinical problems in hospital practice and aseptic surgery, and safe autopsy procedures. All of the procedures currently being practised in germfree laboratories, including the germfree "bubble" used in Houston . . . were derived from work done at Notre Dame by Trexler.123
When accepting this honor Trexler was ambivalent about the future of gnotobiotic technology. In a prepublished abstract Trexler cautiously suggested that the science had "reached a stage in its development comparable to that of genetics a few years after Mendel." On delivery, he retracted his excessive doubts, having become convinced "we are now considerably farther along the road."124 Such hesitancy no doubt derived from the fact that while application of gnotobiotic technology had occurred in locations as diverse as the laboratory, the farm, and the hospital, this had not led to widespread interest or investment in the technology. He concluded with the downbeat warning that "further development may continue to be difficult to obtain unless a sufficient market develops to attract industrial interests."125
Conclusion
Germ-free technology did not emerge from a defined medical problem; rather, it was a novel laboratory technique that was later transitioned to a variety of new sites and uses. Despite its promoters working closely with potential new users to adapt germ-free techniques to localized settings, the technology remained in a state of transition, always at the periphery. This was not because the technology failed to work. There is no evidence that the ability of germ-free isolators to create and maintain secure microbial environments was ever questioned. Rather, germ-free techniques remained at the periphery because the case for their widespread adoption was never conclusively made.
In part, this was because the multiple sites and uses for which germ-free techniques were adapted did not foster the creation of a coherent shared agenda about which a communal identity could form. Trexler's attempts to create a productive relationship across science, medicine, and industry, synergizing medical and veterinary concerns, via the proposed science of gnotobiotics and the related Association for Applied Gnotobiotics, could not overcome the sheer diversity of agendas, professional interests, and disciplinary practices of those he courted. Germ-free technology was not powerful enough to act as a boundary object through which the interests of a veterinarian on the farm, a surgeon in the hospital, and a nurse on the ward could coalesce. Health care systems in particular are notoriously fragmented and physicians generally conservative. To overcome these and other forms of embedded resistance, technological innovators must construct communal social spaces about common interests and shared goals, a process that Thomas Schlich has called the building of a "fraternity."126 In the case of germ-free technology, such a shared community was absent. A technology without a defined user was not a safe investment for industry. The U.K. situation differed to that of the United States, in that the NHS could be portrayed as such a user, and this enabled Trexler to succeed in obtaining industrial investment from Vickers, although not, in the end, to establish his technology within the health service in the way that he had hoped due to the absence of perceived need.
Unlike other techniques, technologies, and tools that successfully made the transition from laboratory to clinic, germ-free technology did not promise to reduce or refine the labor involved in hospital material cultures. As several scholars have argued, medical culture was radically refashioned in the twentieth century not because of science but through an economic logic of ever greater efficacy that science could be mobilized to attain.127 Germ-free technology did not sit well with this underlying administrative logic that transformed medical practice in the twentieth century, which largely displaced individualized and personalized medical practice in favor of generalized, standardized, and routinized approaches compatible with medicine in the age of mass health care.128 Germ-free isolation, in contrast, was highly personalized. It assumed every patient possessed a unique microbial load that should be secured within its own individual environment. Furthermore, the introduction of a patient to an isolator required careful coordination of the technology, personnel (including several nursing and medical staff), and the patient. When the "Life Island" was used for the care of a badly burned child, for example, staff reported that the work of establishing the isolator
was accomplished with delay and mass-confusion . . . only two of the personnel donned sterile gowns, gloves and masks. Two others wore masks . . . the stretcher was too far away from the unit, thus there was over exposure of the child as she was carried to the Island. Upon insertion, the head of the nurse carrying the patient became inserted within the unit and the bare hand of one of the observers moved within the unit to hold the stethoscope out of the way.129
The experience of working with the isolator was "not the easiest." Routine nursing was reported to be possible but "difficult"; nursing staff suffered many "bumps and bruises" and became "drenched in perspiration after just a few minutes enveloped in the plastic."130
Moreover, total isolation prevented a medical practice that, however ephemeral, was widely considered crucial to proper care: that of touch. Medical technology has long been accused of distancing the physician (or nurse) from the patient.131 Technologies of blood pressure measurement, for example, were highly controversial when first introduced because they replaced the traditional method of measuring the pulse by touch.132 By forbidding any form of touch not mediated by plastic, germ-free technology removed a practice that, though lacking objectively established therapeutic value, nonetheless was widely known to be an important, albeit tacit, aspect of care.133 The unnaturalness of human relations within isolation was consequently a recognized though difficult to articulate problem. Guidance for the use of the "Life Island," for example, emphasized how "personnel should be adept, well informed, and confident" in order to ensure "a "calm, confident attitude" that would "lessen the apprehension and fear of the patient."134 Conventionally, fear would have been overcome by a momentary touch. Despite every effort to make the isolator simple, efficient, and comfortable, germ-free technology continued to demand higher levels of labor and remained experientially different in ways that could not be easily effaced.
Constituting a willingness of use was made all the more difficult because it was never clear that the technology was necessary. In the clinical ward and the operating theatre, germ-free technology was preventative, not curative, and thus governed by a logic that denied a choice in its use. Antibiotics, in contrast, could be deployed to combat specific infections as and when their use was necessary. Their necessity and efficacy was tangible and confirmable through bacteriological tests. The credibility and necessity of germ-free isolators as a preventative tool, however, was more difficult to establish because of the inherent difficulty of proving one had prevented something that had not occurred. Only when the microbial threat shifted from the patient to the medical professional, as in the early encounters with Lassa and Ebola, was the new technology deemed necessary. The redistribution of risk perception promised to move the germ-free isolator from a peripheral to a central medical technology.135 Under these circumstances, the isolator also offered a comfort it could not match at any other time, with one report claiming that the "half-suits are comfortable to wear and the rubber gloves do not impair touch for standard medical and nursing procedures."136 The threat posed to the patient by the bacterial loads of medical professionals could not compare to the fear engendered in those same professionals by the new hemorrhagic diseases harbored by patients. When hemorrhagic diseases were found not to be as infectious as first feared, the Trexler isolator quickly fell into disuse. Within the NHS, at the time of writing, isolators are a peripheral technology maintained at two designated High-Security Infectious Diseases Units (the Royal Free Hospital, Hampstead, which was previously Coppetts Wood Hospital, and Newcastle upon Tyne Hospital). Yet, germ-free life and medical isolators, continue to wield a strong presence in the cultural imagination. Within fiction, germ-free isolation technologies have become an instantly recognizable backdrop of imagined future worlds, where deadly and highly infectious diseases necessitate their existence.
In the absence of highly infectious diseases, and whilst antibiotics continue to be a viable treatment of choice, it would seem that, outside the laboratory, germ-free technology will remain more prominent in science fiction than medical fact. At least, that is, for now.137
Figure 9.
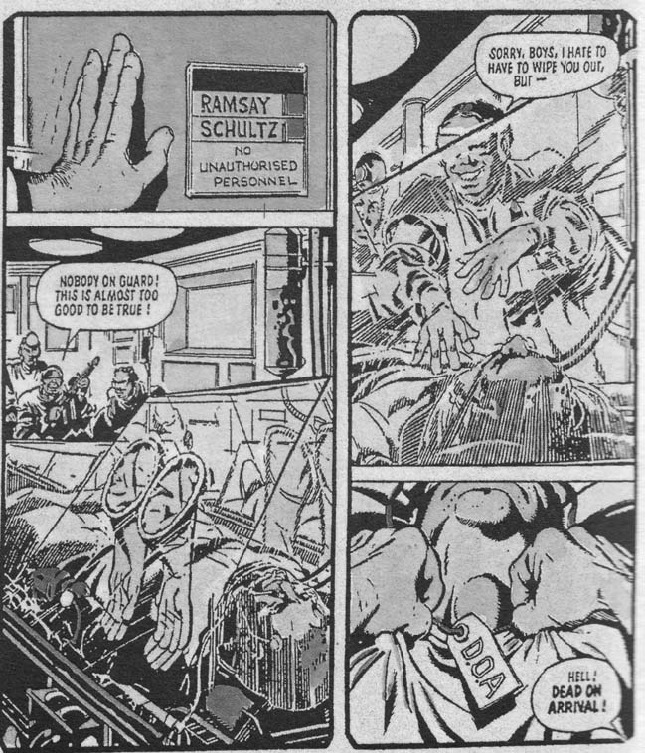
The Trexler isolator has frequently featured in the imagined medical future of Judge Dredd, a fictional lawman combining the roles of judge, jury, and executioner to keep order in the violent and overpopulated twenty-second-century "Mega City One" (1977 to date). Dredd is among the best known of British comic characters whose chief writers in the 1980s, Wagner and Grant, drew inspiration for their work by extrapolating from contemporary scientific and medical journals. Source: John Wagner and Alan Grant, "Otto Sump's Ugly Clinic," 2000 AD 187 (1980): 7.
© 2012 Rebellion A/S. All rights reserved. Used with permission. www.2000ADonline.com
Acknowledgments
I began working on wider uses of gnotobiotic technology in response to an invitation to participate in the Veterinary Knowledge: Between Human Medicine and Agriculture, 1870-1970 workshop held at the Ecole des Hautes Etudes en Sciences Sociales, Paris, in 2008. My thanks to Delphine Berdah and Jean-Paul Gaudillière for providing this unique opportunity to think across human and veterinary medicine. Several archivists were more than helpful in tracking down and making materials available, I would to thank in particular Janice Goldblum (National Academy of Sciences Archives) and Sharon Sumpter (University of Notre Dame) as well as the staff at the U.K. National Archives (Kew). Finally, I would like to thank the anonymous reviewers and editors for their incisive and helpful comments. This research was generously supported by the Wellcome Trust (grant number 084988/Z/08/Z), to which I remain indebted.
Biography
Robert G. W. Kirk is a Wellcome Research Fellow at the Centre for the History of Science, Technology and Medicine (CHSTM), University of Manchester. His research addresses nonhuman animal roles in science and medicine, as well as the place of nonhuman animals in history and historical writing, a subject he has explored through the history of the medicinal leech. He is currently working on the history of twentieth-century animal experimentation, focusing on the growing importance of laboratory animal welfare and the emergence of the "3Rs" (being the reduction, refinement, and replacement of animals in biomedical research).
Footnotes
Health and Disease Discussion in Man and His Future ed. Wolstenholme Gordon. London: Churchill; 1963. 230–246. quotation on 236.
Koprowski Hilary. Future of Infectious and Malignant Diseases in Wolstenholme ed., Man and His Future n. 1 196–216.
Koprowski Hilary. Future of Infectious and Malignant Diseases in Wolstenholme ed., Man and His Future n. 1 234–235.
Koprowski Hilary. Future of Infectious and Malignant Diseases in Wolstenholme ed., Man and His Future n. 1 197 198
Health and Disease Discussion (n. 1 236 Koprowski Future of Infections. :198. n. 2.
Health and Disease Discussion. p. 236. n. 1.
Burnet Macfarlane. Natural History of Infectious Disease. 2nd ed. Cambridge: Cambridge University Press; 1953. p. ix.
Bud Robert. Penicillin: Triumph and Tragedy. Oxford: Oxford University Press; 2007.
Gannon Robert. Life in a Germfree World. Popular Sci. 1962 Aug;181:90–93. quotation on 93. Germ-free monkeys were bred at the Walter Reed Institute for use in the space program.
Wolfe A. J. Germs in Space: Joshua Lederberg, Exobiology, and the Public Imagination, 1958-1964. Isis. 2002;93:183–205. doi: 10.1086/344962.
Crichton Michael. The Andromeda Strain. New York: Knopf; 1969. Such was its popularity that the novel was faithfully adapted to film in 1971 and more imaginatively translated into a TV miniseries in 2008.
Löwy Ilana. Between Bench and Bedside: Science, Healing and Interleukin-2 in a Cancer Ward. Cambridge, Mass.: Harvard University Press; 1996. Gaudillière Jean-Paul, Löwy Ilana. eds., The Invisible Industrialist: Manufacturers and the Production of Scientific Knowledge Houndmills: Macmillan; 1998.
Blume Stuart S. Insight and Industry: On the Dynamics of Technological Change in Medicine. Cambridge, Mass.: MIT Press; 1992. Pickstone John V. ed., Medical Innovations in Historical Perspective Houndmills: Macmillan; 1992. Timmermann Carsten, Anderson Julie. eds., Devices and Designs: Medical Technologies in Historical Perspective Basingstoke: Palgrave Macmillan; 2006.
Star Susan Leigh, Griesemer James R. Institutional Ecology, 'Translations' and Boundary Objects: Amateurs and Professionals in Berkeley's Museum of Vertebrate Zoology, 1907-39. Soc. Stud. Sci. 1989;19:387–420.
Schlich Thomas. Surgery, Science and Industry: A Revolution in Fracture Care 1950s-1990s. Houndmills: Palgrave Macmillan; 2002.
See the Johns Hopkins Biographies of Disease series (edited by Rosenberg Charles. and the Oxford University Press Biographies of Disease series (edited by William, Bynum Helen.
Cooter Roger. The Life of a Disease? Lancet. 2010;375:111–112.
Historians of science have profitably applied biography to the objects and technologies of science as a means to explore and not avoid the question of cultural and epistemological construction; e.g., Daston Lorraine. ed., Biographies of Scientific Objects Chicago: University of Chicago Press; 2000
Finds Life without Microbes Possible. Chickens Raised amid Microbe-Proof Conditions Just as Big and Healthy as Others in Farmyard. New York Times. 1912 Feb 16;:4. col. 5.
Thrive without Microbes: Sterilized Guinea-Pigs Grow 30 Per Cent Faster Than Others. New York Times. 1914 May 10;:3.
Haldane Charlotte. Man's World. London: Chatto & Windus; 1926. pp. 56–57.
Flagg Francis. The Machine Man of Ardathia. Amazing Stories. 1927 Nov;:62–63.
Flagg Francis. The Machine Man of Ardathia. Amazing Stories. 1927 Nov;:61.
Squier Susan Merrill. Babies in Bottles: Twentieth-Century Visions of Reproductive Technology. New Brunswick, N.J.: Rutgers University Press; 1994. pp. 43–44.
The creation of an aseptic environment was critically important to the early tissue culture work, such as that of Alexis Carrel, which also informed Flagg's story; see Witkowski J. A. Alexis Carrel and the Mysticism of Tissue Culture. Med. Hist. 1979;23:279–296. doi: 10.1017/s0025727300051760. For popular understandings of germs in this period, see Tomes Nancy. The Gospel of Germs: Men, Women, and the Microbe in American Life. Cambridge, Mass.: Harvard University Press; 1998.
Racial hygiene being an obvious example; see Proctor Robert N. Racial Hygiene: Medicine and the Nazis. Cambridge, Mass.: Harvard University Press; 1988.
As already noted, the vocal interwar eugenicist Alexis Carrel devoted much of his scientific work to developing aseptic methods for the study of tissues and organs outside the body. See Reggiani Andrés Horacio. God's Eugenicist: Alexis Carrel and the Sociobiology of Decline. New York: Berghahn Books; 2007.
Gaudillière Jean-Paul, Löwy Ilana. Heredity and Infection: The History of Disease Transmission. London: Routledge; 2001.
Enclosure "Staff in Bacteriology, University of Notre Dame, Indiana," ca. October 1942, in Committees on Biological Warfare, Series 6: Name Files ("Academy Files"), box 8, Reyniers, Dr. James A.: 1942-1943, p. 2, National Academies Archives, Washington, D.C., USA (hereafter NAA).
LOBUND Institute for Research in the Life Sciences. pp. 2–3. PNDP40-Lo-1 Folder: LOBUND (Laboratories of Bacteriology U.N.D.) 1940s-1980s, Archives of the University of Notre Dame, Notre Dame, Ind., USA (hereafter UND)
"Standardization through mechanization" became Reyniers's mantra; see Thone Frank. New Safety for Babies. Sci. News-Letter. 1940 Aug 17;38:102–103.
Reyniers J. A. A New and Simplified Micrurgical Apparatus Especially Adapted to Single Cell Isolation. J. Bacteriol. 1932;23:183–192. doi: 10.1128/jb.23.2.183-192.1932.
Reyniers's difficulties paralleled those faced by early attempts to work with tissue culture; see Witkowski Alexis Carrel. n. 25.
In 1942 Reyniers wrote, "Undoubtedly at first glance, my age and formal education does not seem to warrant rank or consideration. However, when my record is examined it will be found that my age and lack of the conventional 'moulding' that invariable accompanies the doctorate have aided rather than hindered my progress." Letter James A. Reyniers to Dr. E. B. Fred (National Academy of Sciences) 23rd October 1942 p. 2 NAA
Reflecting what Pauly describes as the "engineering standpoint in biology"; see Pauly Philip J. Controlling Life: Jacques Loeb and the Engineering Ideal in Biology. Oxford: Oxford University Press; 1987. pp. 28–54. esp.
Reyniers J. A. The Production and Use of Germ-Free Animals in Experimental Biology and Medicine. Amer. J. Vet. Res. 1957;18:678–687. quotation on 678.
Literature on the importance of standards in the provision of experimental organisms is too vast to cite fully; key contributions include Clause B. The Wistar Rat as a Right Choice: Establishing Mammalian Standards and the Ideal of a Standardized Mammal. J. Hist. Biol. 1993;26:329–349. doi: 10.1007/BF01061973. Kohler Robert E. Lords of the Fly: Drosophila Genetics and the Experimental Life. Chicago: University of Chicago Press; 1994. Creagar Angela N. H. The Life of a Virus: Tobacco Mosaic Virus as an Experimental Model, 1930-1965. Chicago: University of Chicago Press; 2002. Rader Karen. Making Mice: Standardizing Animals for American Biomedical Research, 1900-1955. Princeton, N.J.: Princeton University Press; 2004.
Appleton B. LOBUND Comes of Age. Sci. Monthly. 1955;80:57–58.
For the LOBUND Institute's role in American biological warfare research, see Fitzgerald Gerard James. From Prevention to Infection: Intramural Aerobiology, Biomedical Technology, and the Origins of Biological Warfare Research in the United States, 1910-1955. Carnegie Mellon University; 2003. Ph.D. diss.
Life Without Germs. Life Magazine. 1949 Sep 26;:107–113. 107.
Enclosure Staff in Bacteriology, University of Notre Dame, Indiana ca. October 1942. p. 3 NAA (n. 29)
Bourdillon R. B., Lidwell O. M., Lovelock J. E. Studies in Air Hygiene: Medical Research Council Special Report Series no. 262. London: HMSO; 1948.
Wells W. F., Wells M. W., Wilder T. S. The Environmental Control of Epidemic Contagion: I. An Epidemiologic Study of Radiant Disinfection of Air in Day Schools. Amer. J. Hygiene. 1942;35:97–121. Moulton Forest Ray. ed., Aerobiology Washington, D.C. American Association for the Advancement of Science; 1942.
Reyniers J. A. The Control of Cross Infection among Limited Populations: The Use of Mechanical Barriers in Preventing Cross Infection among Hospitalized Infant Populations in Micrurgical and Germ-Free Techniques: Their Application to Experimental Biology and Medicine ed. Reyniers J. A. Springfield, Ill. Charles C Thomas; 1943. 205–232. 206
Reyniers J. A. The Control of Cross Infection among Limited Populations: The Use of Mechanical Barriers in Preventing Cross Infection among Hospitalized Infant Populations in Micrurgical and Germ-Free Techniques: Their Application to Experimental Biology and Medicine ed. Reyniers J. A. Springfield, Ill. Charles C Thomas; 1943. 207
Reyniers J. A. Design Characteristics of Double Cubicle System for Protecting Babies in Nurseries. Amer. J. Dis. Child. 1942;63:934–944.
Reyniers J. A. Design Characteristics of Double Cubicle System for Protecting Babies in Nurseries. Amer. J. Dis. Child. 1942;63:243.
Thone New Safety for Babies. p. 103. n. 31.
Indeed, Harlow's work was in part inspired by his observation that the introduction of isolation to prevent the spread of infection among his experimental monkeys detrimentally affected their learning capacity.
Showcase Baby. Mechanix Illustrated. 1947 Mar;:74.
Skinner B. F. Baby in a Box: Introducing the Mechanical Baby Tender. Ladies Home Journal. 1945 Oct;:62, 30–31. Subsequent letters (135-36, 138) attest to the popularity of the concept. Retrospectively, however, due to Skinner's association with operant conditioning, the "Baby Tender" has been confused with the "Skinner Box," leading some to erroneously relate it to the management of child psychology rather than their physical and microbial environment.
Trexler P. C. The Evolution of Gnotobiotic Technology 4 ca. June 1984. in folder UDIS100/02, "LOBUND Laboratory Conference: Bubble Boy (6/84); International Symposium on Germfree Research 1972-1984," UND.
See Hillier K. Babies and Bacteria: Phage Typing, Bacteriologists, and the Birth of Infection Control. Bull. Hist. Med. 2006;80:733–761. doi: 10.1353/bhm.2006.0130.
Gould undertook extensive investigations of the antibiotic content of air in the hospital, pharmaceutical factory, and farm, in order to prove (a) bacteria traveling from patient to patient via the air was exposed to antibiotics for longer periods than conventional treatment allowed, thus explaining the inexplicably fast rise of resistant bacteria; (b) antibiotics themselves could travel by air, thus persons who worked in antibiotic heavy environments would be carriers of resistant bacteria. See Gould J. C. Environmental Penicillin and Penicillin-Resistant Staphylococcus Aureus. Lancet. 1958;271:489–493. doi: 10.1016/s0140-6736(58)90807-9.
Anderson J. Greenhouses and Bodysuits: The Challenge to Knowledge in Early Hip Replacement Surgery 1960-1982 in Timmermann, Anderson Devices and Designs n. 13 175–191. Anderson J., Neary F., Pickstone John V. Surgeons, Manufacturers and Patients: A Transatlantic History of Total Hip Replacement. Basingstoke: Palgrave Macmillan; 2007. pp. 96–103. esp.
Charnley J. Clean Air Operating Room Enclosures. Brit. Med. J. 1974;5938:224–225. doi: 10.1136/bmj.4.5938.224.
Howe C. W. Prevention and Control of Postoperative Wound Infections Owing to Staphylococcus Aureus. New Engl. J. Med. 1956;255:787–794. doi: 10.1056/NEJM195610252551701. Walter C. W., Kundsin R. B. The Floor as a Reservoir of Hospital Infections. Surg. Gyn. Obstet. 1960;111:412.
Gibson R. Myles. Application of Antibiotics (Polybactrin) in Surgical Practice, Using the Aerosol Technique. Brit. Med. J. 1958;5083:1326–1327. doi: 10.1136/bmj.1.5083.1326. Hart D. Bactericidal Ultraviolet Radiation in the Operating Room: Twenty-Nine Year Study for Control of Infections. J. Amer. Med. Assoc. 1960;172:1019–1028. doi: 10.1001/jama.1960.03020100027006.
Letter, Philip C. Trexler to Mathew Maley (Shriners Hospital for Crippled Children, Cincinnati, Ohio) November 18 1969. p. 1 Shriners Hospital Patient Isolation Unit Records, Archives Center, National Museum of American History, Smithsonian Institution, box 1, folder 4 (hereafter SHPI).
Levenson S. M., Trexler P. C., Laconte M., Pulaski E. J. Application of the Technology of the Germfree Laboratory to Special Problems of Patient Care. Amer. J. Surg. 1964;107:710–722. doi: 10.1016/0002-9610(64)90298-3. quotation on 710.
Levenson S. M., Trexler P. C., Malm O. J., Horowitz R. E., Moncrief W. H. A Disposable Plastic Isolator for Operating in a Sterile Environment. Surg. Forum. 1960;11:306–308. 307.
Levenson S. M., Trexler P. C., Malm O. J., LaConte M. L., Horowitz R. E., Moncrief W. H. A Plastic Isolator for Operating in a Sterile Environment Amer. J. Surg. 104 no. 6 1962. 891–899. quotation on 891.
U.S. Patent Office, number 3051164, filed August 17, 1959.
Levenson, et al. Plastic Isolator for Operating. p. 897. n. 62.
Alpert S., Salzman T., Dinerman M., Clark J., Levenson S. M. A Study of Patients Operated on Using a Surgical Isolator Technique or in a Conventional Operating Room Environment. Surg. Forum. 1968;19:68–69.
Levenson, et al. Application of the Technology. p. 721. n. 60.
'Giant Bubble' Unit Serves to Limit Cross Infections. Antib. News. 1964 Nov 11;:8. Levenson, et al. Application of the Technology. p. 721. n. 60.
Trexler Philip C. Development of Gnotobiotics and Contamination Control in Laboratory Animal Science in American Association for Laboratory Animal Science 50 Years of Laboratory Animal Science Memphis: AALAS; 1999. 121–128. 123
Trexler P. C. An Isolator for the Maintenance of Aseptic Environments. Lancet. 1973 Jan 13;7794:91–93. 92. doi: 10.1016/s0140-6736(73)90481-9.
Trexler P. C. Report of the Gnotobiotic Workshop for Laboratory Animal Breeders. Proc. Animal Care Panel. 1961;11:249–253. 253.
"Information for a Non-faculty Research Appointment Graduate School University of Notre Dame, Trexler, Philip Charles, 12th July 1983," in folder UDIS100/02, "LOBUND Laboratory Conference: Bubble Boy (6/84); International Symposium on Germfree Research 1972-1984," UND.
Charles River remains a global leader in the production and supply of laboratory animals. Snyder Laboratories was acquired by Zimmer (Warsaw, Ind.) in 1978.
A key innovation was Trexler's design of robust microbial-secure containers for the shipment of animals; see U.S. Patent Office, no. 3238922, filed November 13, 1964; U.S. Patent Office, no. 3396701, filed August 15, 1966.
"Plastifab—Specialists in Germ-Free Enclosures," 2, box 1, folder 8, "Materials Samples and Plastics Used in the Snyder Unit, Undated," SHPI.
U.S. Patent Office, no. 3265059, filed February 21, 1962. Details on the "Life Island" isolator can be found in box 1, folder 2, "Life Island (Mark V) Advertisements and Correspondence," SHPI. For its popular representation, see Life in a Life Island. Time. 1964 May 29;:52.
Cf. Timmermann C., Valier H. Clinical Trials and the Reorganization of Medical Research in Post-Second World War Britain. Med. Hist. 2008;52:493–510. doi: 10.1017/s0025727300002994.
For Betts, see Boden Edward. Professor Alan Betts. The Independent. 2005 Dec 27;:47.
Gordon H. A., Wagner M., Wostmann B. S. Studies on Conventional and Germ-Free Chickens Treated Orally with Antibiotics. Antib. Annu. 1957;48:248–255. Jukes T. H. The History of the 'Antibiotic Growth Effect,'. Federation Proc. 1977;36:2514–2518.
Bud Penicillin. pp. 163–191. n. 8.
Young G. A., Underdahl N. R. An Isolation Brooder for Raising Disease-Free Pigs. J. Amer. Vet. Med. Assoc. 1957;131:279–283.
Young G. A., Underdahl N. R., Sumpton L. J., Peo E. R., Olsen L. S., Kelley G. W., Hudman D. B., Caldwell J. D. Swine Repopulation. I. Performance within a Disease-Free Experiment Station Herd. J. Amer. Vet. Med. Assoc. 1959;134:491–496.
Young G. A., Underdahl N. R., Hinz R. W. Procurement of Baby Pigs by Hysterectomy. Amer. J. Vet. Res. 1955;58:123–131.
Caldwell J. D., Young G. A., Underdahl N. R. Swine Repopulation. III. Performance of Primary Specific Pathogen Free Pigs on Farms. J. Amer. Vet. Med. Assoc. 1961;138:141–145.
As in the hospital, isolators on the farm were rivaled by pharmaceutical companies and feed manufacturers; see Finlay Mark R. Hogs, Antibiotics and the Industrial Environments of Postwar Agriculture in Industrializing Organisms: Introducing Evolutionary History ed. Schrepfer Susan R., Scranton Philip. London: Routledge; 2004. 237–260.
Betts A. O., Luke D. The Specific Pathogen-Free Pig Programme in the USA. Vet. Rec. 1961;73:283–286.
Trexler P. C. Microbiological Isolation of Large Animals. Vet. Rec. 1971;88:15–20. doi: 10.1136/vr.88.1.15. Betts A. O. SPF Animals in Intensive Livestock Farming ed. Blount W. London: Heinemann; 1968. 508–513.
Heard T. W., Jollins J. L. Observations on Closed Hysterectomy Founded Pig Heard. Vet. Rec. 1967;81:481–487. doi: 10.1136/vr.81.19.481.
Drummond A. J., Trexler P. C., Edwards G. B., Hillidge C., Cox J. E. A Technique for the Production of Gnotobiotic Foals. Vet. Rec. 1973;92:555–557. doi: 10.1136/vr.92.21.555.
Betts A. O., Trexler P. C. Development and Possible Uses for Gnotobiotic Farm Animals. Vet. Rec. 1969;84:630–632. doi: 10.1136/vr.84.25.630.
Virus from Monkeys. Brit. Med. J. 1968;5605:575–576.
Work Stopped on Deadly Virus. The Times. 1970 Feb 11;:7. col. C.
Trexler Development of Gnotobiotics. p. 123. n. 68. "Application to the Department of Health and Social Security for Support to Finance Continuation of a Programme for Development of Hospital Isolators for Patients Suffering from Dangerous Infection," March 10, 1975, Medical Research Council Archive, National Archives, Kew, UK (hereafter NA), NA MH148/361. For the NRDC, see Keith S. T. Inventions, Patents and Commercial Development from Governmentally Financed Research in Great Britain: The Origins of the National Research Development Corporation. Minerva. 1981;19:92–122.
Spiers A. S., Trexler P. C. The Use of a Plastic Isolator for the Prevention of Infection in Patients with Acute Leukaemia. J. Physiol. 1973;231:66P–67P.
Stanton Jennifer. ed., Innovations in Health and Medicine: Diffusion and Resistance in the Twentieth Century London: Routledge; 2002. esp. 3
A Patient's Eye View of Life in an Isolator. Jun, 1977. NA MH148/362.
Emond R. T. D., Evans B., Bowen E. T. W., Lloyd G. A Case of Ebola Virus Infection. Brit. Med. J. 1977;2:541–544. doi: 10.1136/bmj.2.6086.541.
Hutchinson J. G. P., Gray J., Flewett T. H., Emond R. T. D., Evans B., Trexler P. C. The Safety of the Trexler Isolator as Judged by Some Physical and Biological Criteria: A Report of Experimental Work at Two Centres. J. Hygiene (Cambridge) 1978;81:311–319. doi: 10.1017/s0022172400025158. Trexler P. C. Patient Isolators. Brit. J. Clin. Equipment. 1979;4:126. Department of Health and Social Security. Memorandum on Lassa Fever. London: HMSO; 1976.
Evaluation of the Trexler Containment Isolator: Report of the Central Steering Committee Appendix C June 1977. p. 2 NA MH148/362
McLauchlan J., Pilcher M. F., Trexler P. C., Whalley R. C. The Surgical Isolator. Brit. Med. J. 1974 Feb 23;5903:322–324. 324. doi: 10.1136/bmj.1.5903.322.
Trexler P. C. An Isolator for the Maintenance of Aseptic Environments. Lancet. 1973 Jan 13;301:91–93. doi: 10.1016/s0140-6736(73)90481-9.
See files NA MH148/362 and NA MH148/362.
Emond R. T. D. Hospitalisation of Patients Suspected of Highly Infectious Disease in Ebola Virus Haemorrhagic Fever ed. Pattyn S. R. Amsterdam: Elsevier; 1978. 251–254. 251
Godber George. Report of the Working Party on the Laboratory Use of Dangerous Pathogens, Cmnd 6054. London: HMSO; 1975.
Helmick C. G., et al. No Evidence for Increased Risk of Lassa Fever Infection in Hospital Staff. Lancet. 1986 Nov 22;8517:1202–1205. doi: 10.1016/s0140-6736(86)92206-3.
Trexler P. C., Gilmour A. M. Use of Flexible Plastic Film Isolators in Performing Potentially Hazardous Necropsies. J. Clin. Path. 1983;36:527–529. 529. doi: 10.1136/jcp.36.5.527.
Levenson S. M., Trexler P. C., van der Waaij D. Nosocomial Infection: Prevention by Special Clean-Air, Ultraviolet Light, and Barrier (Isolator) Techniques. Curr. Problems Surg. 1986;23:458–558. doi: 10.1016/0011-3840(86)90033-x.
Thompson E. N. Thymic Lymphocytophthisis with Terminal Aplastic Anaemia. Proc. Roy. Soc. Med. 1967;60:895–897.
Barnes R. D., Tuffrey M., Cook R. A 'Germfree' Human Isolator. Lancet. 1968 Mar 23;7543:622–623. doi: 10.1016/s0140-6736(68)91241-5.
Barnes R. D., Fairweather D. V. I., Holliday J., Keane C., Piesowicz A., Soothill J. F., Tuffrey M. A Germfree Infant. Lancet. 1969 Jan 25;293:168–171. 169. doi: 10.1016/s0140-6736(69)91187-8.
Barnes R. D., Bentovim A., Hensman S., Piesowicz Alina T. Care and Observation of a Germ-Free Neonate. Arch. Dis. Childh. 1969;44:211–217. doi: 10.1136/adc.44.234.211.
In addition to articles cited, see Barnes R. D., Fairweather D. V. I., Reynolds E. O. R., Tuffrey M., Holliday J. A Technique for the Delivery of a Germfree Child. J. Obstet. Gyn. Brit. Commonwealth. 1968;75:689–697. doi: 10.1111/j.1471-0528.1968.tb01544.x. "ORaising a Germ-Free Baby The Times January 28 1969. 6 Germ-Free Baby. Chemist and Druggist. 1968 Aug 10;:127.
Germfree Baby (thirty-five-minute film, Boehringer Ingelheim Ltd.), Wellcome Library for the History of Medicine, London, item BMA299.
See Wilson, Raphael—Biology. folder UDIS119/104. and Rev Raphael Wilson (formerly Br) re 'Bubble Boy' Case 1984. folder UDIS214/32. UND.
The Bubble Boy's Lost Battle. Time. 1984 Mar 05;:51.
Baby David: Alive, Well and Waiting. Sci. News. 1974 May 25;105:335.
McVicker Steve. Bursting the Bubble. Houston News. 1997 Apr 10;
See Paediatr. Res. 1977;11(pt. 1)
Murphy M. A., Vogel J. B. Looking Out from the Isolator: David's Perception of the World. Dev. Behav. Pediatr. 1985;6:118–121.
For an account of David's life by his mother, see Demaret Kent. David's Story: Victim of an Immune Deficiency That Condemned Him to Exist in a Sterile World, the Bubble Boy Lived a Full Life. People Weekly. 1984;22:120–132. and The Bubble Boy. People Weekly. 1984;22:107–116.
David, the Boy in the Bubble. Assoc. Gnotobiotics Newsl. 1984 May;:1–2.
Lawrence R. J. David the 'Bubble Boy' and the Boundaries of the Human. JAMA. 1985;253:74–75.
"University of Notre Dame News, 8th June 1984," folder UDIS100/02, "LOBUND Laboratory Conference: Bubble Boy (6/84); International Symposium on Germfree Research 1972-1984," UND.
Letter Morris Pollard (director, LOBUND Institute) to Francis Castellino, 16th March 1984. folder UDIS100/02, UND.
Trexler Evolution of Gnotobiotic Technology. p. 5. n. 52.
Trexler Evolution of Gnotobiotic Technology. p. 4. n. 52.
Schlich Surgery, Science and Industry. pp. 35–41. n. 15.
Berg M. Rationalizing Medical Work Decision Support Techniques and Medical Practices. Cambridge, Mass.: MIT Press; 1997. Sturdy S., Cooter R. Science, Scientific Management, and the Transformation of Medicine in Britain, 1870-1950. Hist. Sci. 1998;36:421–466. doi: 10.1177/007327539803600402.
Sturdy, Cooter Science, Scientific Management. n. 127.
Life Island Isolation ca. March 1967. 1 box 1, folder 2, SHPI
Life Island Isolation ca. March 1967. 7
Reiser Stanley Joel. Medicine and the Reign of Technology. Cambridge: Cambridge University Press; 1978.
Evans Hughes. Losing Touch: The Controversy over the Introduction of Blood Pressure Instruments into Medicine. Technol. Cult. 1993;34:784–807.
Gadow Sally. Touch and Technology: Two Paradigms of Patient Care. J. Religion Health. 1984;23:63–69. doi: 10.1007/BF00999900. Sandelowski Margarete. Devices and Desires: Gender, Technology and American Nursing. Chapel Hill: University of North Carolina Press; 2000.
I. Purpose: To Provide a Contamination Free Environment for a Patient with Low Resistance to Infection Life Island Instructions p. 14 SHPI
For the role of risk perception in medical innovation, see Schlich Thomas, Tröhler Ulrich. eds., The Risks of Medical Innovation Risk Perception and Assessment in Historical Context London: Routledge; 2006
Evaluation of the Trexler Containment Isolator, Report of the Central Steering Group, June 1977. NA MH148/362.
Concerns regarding a return of infectious diseases, catalyzed by the fear of bioterrorism and potential flu pandemics, have refocused attention on microbial isolation as a means of containment; see Clin. Microbiol. Infect. 2009;15:8.