

Abstract
Introduction
The role of fusion of lumbar motion segments for the treatment of axial low back pain (LBP) from lumbar degenerative disc disease (DDD) without any true deformities or instabilities remains controversially debated. In an attempt to avoid previously published and fusion-related negative side effects, motion preserving technologies such as total lumbar disc replacement (TDR) have been introduced. The adequate extent of preoperative DDD for TDR remains unknown, the number of previously published studies is scarce and the limited data available reveal contradictory results. The goal of this current analysis was to perform a prospective histological, X-ray and MRI investigation of the index-segment’s degree of DDD and to correlate these data with each patient’s pre- and postoperative clinical outcome parameters from an ongoing prospective clinical trial with ProDisc II (Synthes, Paoli, USA).
Materials and methods
Nucleus pulposus (NP) and annulus fibrosus (AF) changes were evaluated according to a previously validated quantitative histological degeneration score (HDS). X-ray evaluation included assessment of the mean, anterior and posterior disc space height (DSH). MRI investigation of DDD was performed on a 5-scale grading system. The prospective clinical outcome assessment included Visual Analogue Scale (VAS), Oswestry Disability Index (ODI) scores as well as the patient’s subjective satisfaction rates.
Results
Data from 51 patients with an average follow-up of 50.5 months (range 6.1–91.9 months) were included in the study. Postoperative VAS and ODI scores improved significantly in comparison to preoperative levels (p < 0.002). A significant correlation and interdependence was established between various parameters of DDD preoperatively (p < 0.05). Degenerative changes of NP tissue samples were significantly more pronounced in comparison to those of AF material (p < 0.001) with no significant correlation between each other (p > 0.05). Preoperatively, the extent of DDD was not significantly correlated with the patient’s symptomatology (p > 0.05). No negative influence was associated with increasing stages of DDD on the postoperative clinical outcome parameters following TDR (p > 0.05). Increasing stages of DDD in terms of lower DSH scores were not associated with inferior clinical results as outlined by postoperative VAS or ODI scores or the patient’s subjective outcome evaluation at the last FU examination (p > 0.05). Conversely, some potential positive effects on the postoperative outcome were observed in patients with advanced stages of preoperative DDD. Patients with more severe preoperative HDS scores of NP samples demonstrated significantly lower VAS scores during the early postoperative course (p = 0.02).
Conclusion
Increasing stages of DDD did not negatively impact on the outcome following TDR in a highly selected patient population. In particular, no preoperative DDD threshold value was identified from which an inferior postoperative outcome could have been deduced. Conversely, some positive effects on the postoperative outcome were detected in patients with advanced stages of DDD. Combined advantageous effects of progressive morphological structural rigidity of the index segment and restabilizing effects from larger distraction in degenerated segments may compensate for increasing axial rotational instability, one of TDR’s perceived disadvantages. Our data reveal a “therapeutic window” for TDR in a cohort of patients with various stages of DDD as long as preoperative facet joint complaints or degenerative facet arthropathies can be excluded and stringent preoperative decision making criteria are adhered to. Previously published absolute DSH values as contraindication against TDR should be reconsidered.
Keywords: Total disc replacement, Disc arthroplasty, Disc degeneration, Degenerative disc disease, Histological degeneration
Introduction
Fusion of lumbar motion segments has previously been claimed to be the “gold standard” for the treatment of true deformities and instabilities of the lumbar spine that had proved unresponsive to conservative treatment. However, its role in the treatment of axial low back pain (LBP) from lumbar degenerative disc disease (DDD) remains controversially debated. A variety of early and late complications such as adjacent segment pathologies have been reported in a considerable number of patients following the surgical intervention [1–12].
In an attempt to avoid these fusion-related negative side effects, motion preserving technologies such as total lumbar disc replacement (TDR) procedures have been introduced. Their clinical efficacy has been demonstrated by a variety of class I to class IV studies worldwide [13–26].
However, the adequate extent of preoperative DDD for TDR remains controversially debated, the number of previously published studies is scarce and the limited data available reveal contradictory results. Moore et al. [27] were able to show delayed but significant changes of the facet joints at the index and adjacent levels during the progressive stages of DDD in a standardized animal model of disc degeneration. Significant preoperative facet joint degeneration remains to be one commonly agreed upon contraindication against TDR [28–31]. Thus, well-justified concern arises from possible degenerative changes in the facet joints with increasing stages of DDD with a potential detrimental effect on TDR outcome. Based on these concerns, different study groups have independently defined various contraindications against TDR. Zeh et al. and Lemaire et al. reported that a reduction in DSH of >50 % was considered a contraindication against TDR [20, 32] whilst other authors defined varying absolute DSH values as inclusion/exclusion criteria [30, 31, 33, 34]. Since their introduction, however, these previously defined contraindications have not been evaluated or confirmed with evidence based data.
The goal of this current analysis was to perform a prospective histological, X-ray and MRI investigation of the index-segment’s degree of DDD and to correlate these data with each patient’s pre- and postoperative clinical outcome parameters from an ongoing prospective clinical trial with ProDisc II (Synthes, Paoli, USA).
Materials and methods
Preoperative diagnosis and patient selection
All patients included in this study are part of an ongoing prospective clinical trial with ProDisc II (Synthes, Paoli, USA). Disc replacement was performed for the treatment of patients with predominant (≥80 %) axial low back pain originating from lumbar degenerative disc disease. Indications and contraindications for this procedure have been thoroughly outlined previously [13, 24, 26, 28–31]. A summary of exclusion criteria from this study is listed in Table 1.
Table 1.
Exclusion criteria/contraindications
| Central or lateral spinal stenosis |
| Predominant radiculopathy |
| Facet joint arthrosis/symptomatic facet joint complaints |
| Spondylolysis/spondylolisthesis |
| Spinal instability (iatrogenic/altered posterior elements, e.g. following laminectomy) |
| Major deformity/curvature deviations (e.g. scoliosis) |
| Metabolic bone disease (e.g. manifest osteoporosis/osteopenia) |
| Previous operation with severe scarring and radiculopathy |
| Compromised vertebral body (irregular endplate shape) |
| Previous/latent infection |
| Metal allergy |
| Spinal tumour |
| Post-traumatic segments |
All patients were non-responders to an intensive inpatient and outpatient conservative treatment program conducted over a minimum 6-month period.
The preoperative diagnosis was made on the basis of lumbar X-rays taken in ap and lateral view, functional flexion/extension images and preoperative MRI of the lumbar spine.
Preoperatively, all patients underwent fluoroscopically guided spine infiltrations to rule out non-discogenic pain sources. Patients who demonstrated a significant and reproducible pain relief (≥50 %) following infiltrations of the facet or the sacroiliac joints were not considered candidates for TDR.
The role of discography in identifying discogenic pain remains debatable. Previous studies showed a high rate of false positive and negative results equally [35], failure of the patient to distinguish between concordant and non-concordant pain [36], 100 % ‘memory pain’ in patients with abnormal psychometric testing [36] as well as 0.5 % infection rate [36, 37]. Furthermore, recent studies have shown that the degenerative process within a disc can be initiated with a mere needle puncture, i.e. performed during lumbar discography [27, 38–46]. Therefore, discography was not employed as a diagnostic tool in the present study.
Disc spaces were approached through a mini-open laparotomy and a retroperitoneal approach as described previously [47, 48]. Insertion of the ProDisc implant was performed according to the manufacturers guidelines [49].
Study documentation
All data were recorded within the framework of an ongoing prospective clinical trial. Patients were examined preoperatively, followed by routine clinical and radiological examinations at 3, 6 and 12 months postoperatively, annually from then onwards. Study documentation was standardized and included the Visual Analogue Scale (VAS), Oswestry Disability Index [50], as well as numerous clinical and radiological parameters. The patient’s subjective outcome evaluation was based on a 3-scale grading system, namely ‘highly satisfied’, ‘satisfied’ and ‘not satisfied’.
At all pre- and postoperative FU examinations, radiological images were obtained which included standard ap, lateral and functional images taken between maximum flexion and extension movements.
Study cohort definition and inclusion criteria
In order to create a homogenous study population, the following additional inclusion and exclusion criteria were defined:
Only monosegmental TDRs were included.
Histological sample of nucleus pulposus (NP) and/or annulus fibrosus (AF) available in all patients, preoperative MRI and X-rays where available.
Exclusion of patients with combined fusion and disc replacement procedures or TDR for the treatment of adjacent segment instability.
No history of postoperative revision surgery.
Exclusion of spondylophyte formations at the index segment
Radiological evaluation
The hard copies of the patient’s preoperative radiographic X-ray films were scanned using a high-resolution scanner and a standard image-capture software program. The images were then transferred to a computer station for further analysis. All measurements were performed with the aid of a custom-made medical image analysis software (Medimage V 5.0, VEPRO AG, Pfungstadt, Germany). With the aid of computer guidance, all images were corrected for radiographic magnification error. Standard implant reference points and implant dimensions (Fig. 1) were used to determine the percentage of magnification error [51]. Well-defined vertebral body geometries were measured on largely magnified postoperative digital X-ray images and were calibrated for length according to precisely defined implant geometries such as the top fin of the upper implant endplate which remains constant at 17.1 mm for various implant sizes (Fig. 1). These distances were used to calibrate distances on preoperative images. All following distance measurements were automatically corrected accordingly.
Fig. 1.

Endplate geometries of the Prodisc-L implant, superior endplate size medium (M), with 6° of lordosis. The length of the fin remains constant with 17.1 mm for various ProDisc-L endplate geometries
The anterior and posterior disc space height (DSH) was determined preoperatively from standard lateral standing radiographs. DSH was measured by using the shortest distance between the anterior and posterior edges of the vertebral endplates as reference points. As described previously, the mean distance between the anterior and posterior DSH was considered to represent the mean disc height [39, 45, 52–55].
The measurements were performed by two independent observers (F.H., E.H.). The observers were blinded to the clinical results. The means of all measurements were calculated and incorporated into the final statistical analysis.
MRI investigation
All MRI images were evaluated by two skeletal radiologists who are specialized in the evaluation of spinal pathologies (US, A.S.). Both radiologists were blinded to the clinical results and were not included in the process of pre- or postoperative decision making.
The condition of the intervertebral disc at the index level was evaluated on all MRI images. The degree of disc degeneration was classified on a 5-scale grading system as described by previously Pfirrmann et al. [56].
Histological evaluation
All tissue samples from this current study were obtained intraoperatively from the index-segment’s disc space. The tissue samples were immediately fixed in 4–6 % buffered formaldehyde, pH 7.4, for a duration of approx. 12–16 h. In cases with residual bone material or calcifications, the samples were carefully decalcified in 0.1 M EDTA, pH 7.4. The paraffin-embedded specimens were cut into slices (2–4 μm) and routine stainings were performed (Haematoxylin and Eosin (H&E), Masson-Goldner or Elastica van Gieson’s connective tissue stain, Alcian blue-PAS). The histomorphological distinction between annular and nuclear disc tissue was performed by light microscopic criteria, particularly under polarized light, allowing the evaluation of the organization of the collagen network (Fig. 2a–d) [57].
Fig. 2.
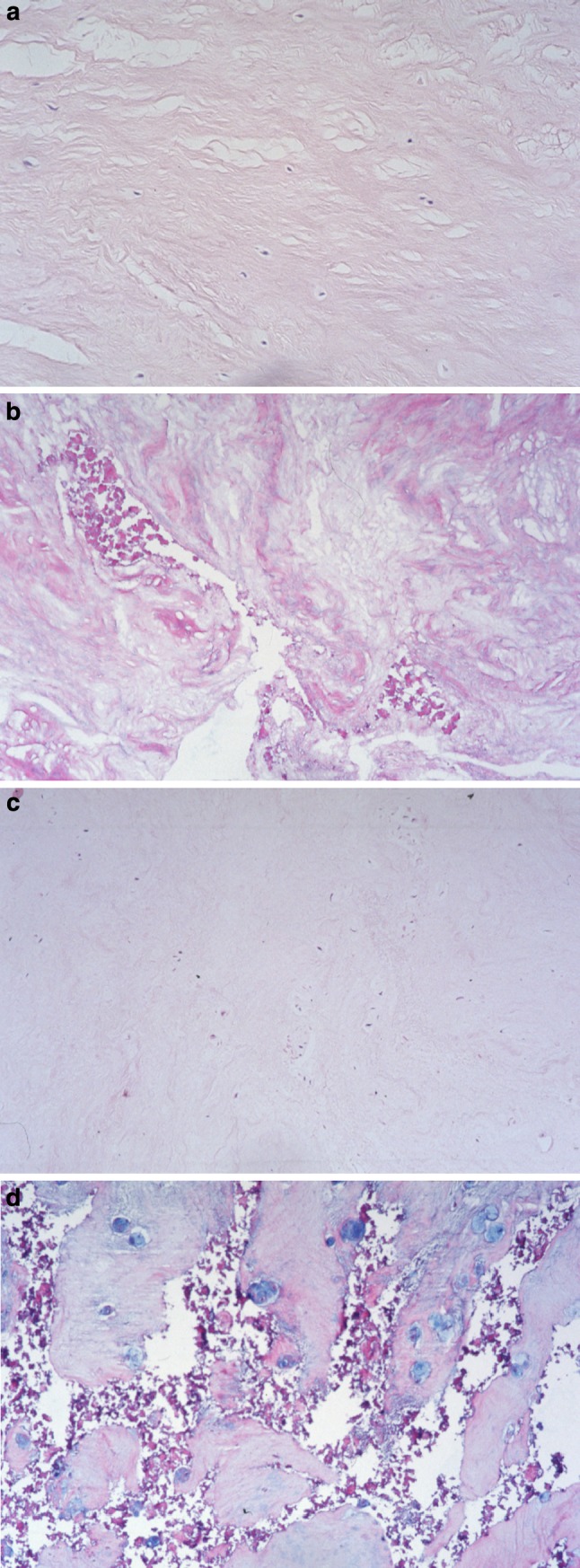
Histomorphological features of normal and pathological disc tissue specimens [Haematoxylin and Eosin (H&E), ×300]. a Sample from the (inner) annulus fibrosus with fairly parallel arranged collagen fibres and few unremarkable cells (HDS score 0). b Annulus fibrosus tissue area with clefting and extensive granular matrix alteration (HDS score 6). c Nucleus pulposus section with fibrocartilaginous matrix and very slightly enhanced, single layered nuclear chondrocytes (HDS score 1). d Nucleus pulposus section with extensive clefting, granular matrix changes and focal clonal chondrocyte proliferation (HDS score 10)
The following histological parameters were taken into account: extent of cellularity, structural changes of granular and/or mucoid alteration and the formation of clefts and tears. All data were obtained as a summary score from 0 to 15 which was recorded for each patient for both annulus and nucleus structures, with 0 delineating none and 15 the most advanced degenerative changes (Table 2).
Table 2.
Parameters collected for the histologic assessment of disc degeneration and scoring
| Criteria | Grading |
|---|---|
| Cell density (chondrocyte proliferation): multiple chondrocytes growing in small rounded groups or clusters sharply demarcated by a rim of territorial matrix | 0 = no proliferation 1 = increased cell density 2 = connection of two chondrocytes 3 = small size clones (several chondrocytes grouped together, 3–7 cells) 4 = moderate size clones (8–15 cells) 5 = huge clones (>15 cells) |
| Structural alterations (tears and clefts): concentric tears following the collagen fibre bundles orientation in the annulus fibrosus or radiating defects extending from the nucleus pulposus to the outer annulus lamellae parallel or oblique to the end-plate (clefts) | 0 = absent 1 = rarely present 2 = present in intermediate amounts between 1 and 3 3 = abundantly present 4 = scar tissue |
| Granular changes: eosinophilic-staining amorphous granules within the fibrocartilage matrix | 0 = absent 1 = rarely present 2 = present in intermediate amounts between 1 and 3 3 = abundantly present |
| Mucous degeneration: cystic, oval or irregular areas with an intense deposition of acid mucopolysaccharides (i.e. sulfated glycosaminoglycans) staining dark blue with Alc-PAS | 0 = absent 1 = rarely present 2 = present in intermediate amounts between 1 and 3, 3 = abundantly present |
| Histologic Degeneration Score (HDS) | 0–15 points |
In a previously conducted histological investigation, one of the senior authors of this study (A.N.) was involved in the development and evaluation of this quantitative classification system for both histological annulus fibrosus (AF) and nucleus pulposus (NP) changes of intervertebral discs (Histological Degeneration Score, HDS) [57]. All tissue samples from this study were quantitatively rated and evaluated accordingly as outlined in Table 2.
The classification system has been thoroughly evaluated with regard to validity, practicability and reliability. The interrater reliability, as demonstrated by means of Kappa statistics, has previously been reported to range between moderate to excellent (κ values 0.49–0.98) [57–59].
In the first part of this study, all parameters representative of lumbar DDD were evaluated separately and correlated with each other in a horizontal analysis to establish any possible interaction. In the second part of this study, a longitudinal analysis was performed to establish the influence of preoperative DDD on the patient’s symptomatology preoperatively as well as on the postoperative clinical outcome parameters.
Statistical analysis
All data were statistically evaluated by an external, independent statistician not involved in the process of pre- or postoperative decision making (W.H.). Pearson’s and Spearman’s correlation coefficients with corresponding statistical tests were computed. One factorial ANOVAs with unpaired and two-sided Student’s t tests as post hoc tests were applied to test for significant differences among means. Two-sided and paired Student t tests were used to compare dependent samples. Statistical significance was established with p < 5 %. All computations and illustrations were done with Statistica 6.1 (StatSoft, Tulsa, OK, USA) [60].
Results
Fifty-one patients were included in the final statistical analysis. A description of the preoperative histological and radiological parameters of DDD is delineated in Table 3; the overall pre- and postoperative clinical results are outlined in Table 4.
Table 3.
Overall results of preoperative parameters of disc degeneration
| Histological evaluation (Histological Degeneration Score, HDS) [57, 58] | |
| Nucleus pulposus (n = 44) | 11.4 Range 7–14 SD ± 2.0 |
| Annulus fibrosus (n = 45) | 7.6 Range 4–12 SD ± 2.2 |
| X-ray investigation (n = 35) | |
| Disc space heightanterior | 8.6 mm Range 5.9–13.1 mm SD ± 2.1 |
| Disc space heightposterior | 5.0 mm Range 2.3–7.4 mm SD ± 1.2 |
| Disc space heightmean | 6.8 mm Range 4.1–9.7 mm SD ± 1.5 |
| MRI investigation (n = 30) | |
| Disc degeneration (Pfirrmann classification) [56] | 0 to <3rd degree DDD n = 0/30 (0 %) 3rd degree DDD n = 2/30 (6.7 %) 4th degree DDD n = 9/30 (30.0 %) 4th–5th degree n = 3/30 (10.0 %) 5th degree DDD n = 16/30 (53.3 %) |
Table 4.
Overall clinical results for the entire study cohort of 51 patients with an average follow-up of 4 years (mean 50.5 months) following total lumbar disc replacement
| Preoperative data | 3 months | 6 months | 12 months | 24 months | 36 months | 48 months | Overall improvement (difference preoperative vs. last FU) | Overall results at last FU | |
|---|---|---|---|---|---|---|---|---|---|
| Number of patients | n = 51 | n = 34 | n = 33 | n = 30 | n = 34 | n = 24 | n = 15 | n = 51 | n = 51 |
| Oswestry Disability Index (ODI) | 39.3 ± 12.7 % | 18.5 ± 15.9 % | 17.3 ± 17.5 % | 20.2 ± 19.0 % | 15.9 ± 17.5 % | 15.0 ± 18.5 % | 11.5 ± 12.6 % | −24.1 ± 16.8 % | 15.2 ± 16.7 % |
| Visual Analogue Scale Scores (VAS) | 6.9 ± 1.6 | 2.6 ± 2.1 | 2.5 ± 2.4 | 2.7 ± 2.8 | 2.5 ± 2.5 | 2.6 ± 2.9 | 1.9 ± 1.8 | −4.1 ± 2.8 | 2.7 ± 2.6 |
| Subjective satisfaction rates | |||||||||
| Highly satisfied | – | 54.8 % (n = 17/31) | 62.1 % (n = 18/29) | 69.2 % (n = 18/26) | 70.0 % (n = 21/30) | 63.6 % (n = 14/22) | 65.5 % (n = 9/12) | n.a. | 75.6 % (n = 34/45) |
| Satisfied | – | 29.0 % (n = 9/31) | 31.0 % (n = 9/29) | 23.1 % (n = 6/26) | 16.7 % (n = 5/30) | 27.3 % (n = 6/22) | 25.5 % (n = 3/12) | 17.8 % (n = 8/45) | |
| Not satisfied | – | 16.1 % (n = 5/31) | 6.9 % (n = 2/29) | 7.7 % (n = 2/26) | 13.3 % (n = 4/30) | 9.1 % (n = 2/22) | 0 % (n = 0) | 6.7 % (n = 3/45) | |
| Satisfied + highly satisfied | – | 83.9 % (n = 26/31) | 93.1 % (n = 27/29) | 92.3 % (n = 24/26) | 86.7 % (n = 26/30) | 90.1 % (n = 20/22) | 100 % (n = 12/12) | n.a. | 93.3 % (n = 42/45) |
Mean values ± standard deviation (SD) are provided
ODI Oswestry Disability Index, VAS Visual Analogue Scale, FU follow-up
The average follow-up was 50.5 months (range 6.1–91.9 months), with 92.2 % of all patients (n = 47/51) completing a min. 12-month FU. A FU of >2 years was available in n = 40 patients (78.4 %), >4 years in n = 26 patients (51.0 %), and >6 years in n = 16 patients (31.4 %), respectively.
Study population
n = 32 patients were male (62.7 %), n = 19 were female (37.3 %) with an average age of 42.4 years (range 29.8–62.1 years). All TDR’s were performed monosegmentally at the levels L5/S1 (n = 38, 74.5 %), L4/5 (n = 9, 17.6 %), L3/4 (n = 2, 3.9 %), L4/S1 (n = 1, 2.0 %) or L5/6 (n = 1, 2.0 %), respectively.
TDR was performed for the treatment of DDD with (n = 21; 41.2 %) and without Modic changes (n = 9, 17.6 %). In n = 14 patients (27.5 %), TDR was performed following a previous discectomy. In n = 7 patients (13.7 %), TDR was performed for the treatment of DDD with an accompanying central disc bulge and clinically predominant axial LBP (≥80 %).
Clinical outcome
The clinical results for the entire study cohort are outlined in Table 4. For both parameters VAS and ODI we observed a highly significant postoperative improvement in comparison to preoperative levels (p < 0.002). At the last FU examination, 75.6 % of all patients (n = 34/45) were ‘highly satisfied’, 17.8 % (n = 8/45) reported a ‘satisfactory’ outcome, whilst 6.7 % (n = 3/45) were ‘not satisfied’ with their subjective outcome of the operation.
Parameters of disc degeneration
The overall results for all parameters of disc degeneration which were assessed in the current study are outlined in Table 3.
X-ray evaluation
Disc space height
The mean preoperative disc space height (DSH) was 6.8 mm (range 4.1–9.7 mm) as established from the measurement of both independent observers. It was 8.6 mm for the anterior DSH (range 5.9–13.1 mm) and 5.0 mm (range 2.3–7.4 mm) for the posterior DSH, respectively.
MRI investigation
The degree of preoperative disc degeneration is outlined in Table 3. The majority of all patients showed advanced stages of disc degeneration on preoperative MRI images, classified as 4th degree (n = 9/30; 30.0 %), 4–5th degree (n = 3/30; 10.0 %) or 5th degree (n = 16/30; 53.3 %). Only n = 2 patients (6.7 %) were classified as 3rd degree DDD according to the Pfirrmann classification system [56].
Histological evaluation
Histo Degeneration Score (HDS) of annulus and nucleus tissue samples
HDS scores of either NP or AF tissue material were available in all patients. AF material was available in n = 45 patients, NP tissue samples were available from n = 44 patients, respectively.
The data showed that the histological degeneration as classified by the HDS was more advanced in the nucleus pulposus material (mean 11.4, range 7–14) in comparison to the degeneration of the annulus fibrosus (mean 7.6, range 4–12; Table 3). The difference between the degenerative changes in NP and AF material was highly significant (p < 0.001).
Correlation between preoperative parameters of disc degeneration
A horizontal analysis between different parameters of lumbar DDD at the index segment revealed a highly significant correlation between the degeneration on MRI images as outlined by the Pfirrmann classification system with the disc space heights that were measured preoperatively (p < 0.001). A strong negative correlation was observed between both parameters (r = −0.74), indicating an increasing loss of DSH with advanced stages of disc degeneration on MRI images.
The parameters of DSHanterior and DSHposterior were highly significantly correlated with each other (p < 0.001, r = 0.79). Conversely, it was interesting to observe that this same strong interdependence was not observed between histological NP and AF samples (p > 0.05; r = 0.3).
Preoperative DDD versus preoperative clinical symptomatology
The correlation between the MRI grading of DDD and the patient’s preoperative symptomatology in terms of VAS or ODI scores was not statistically significant (p = 0.06).
Although patients with higher DSH values revealed lower preoperative VAS and ODI scores in comparison to the results from patients with more collapsed segments, statistical analysis similarly did not reveal any significant correlation between both parameters (p > 0.05).
Finally, there was no significant correlation between the preoperative histological changes of either nucleus or annulus material on the one hand with preoperative VAS or ODI scores, respectively (p > 0.05).
Influence of preoperative DDD on postoperative outcome
Increasing stages of DDD in terms of lower DSH scores were not associated with inferior clinical results as outlined by postoperative VAS or ODI scores (p > 0.05). Furthermore, there was no significant correlation between the patient’s satisfaction rates observed at the last FU examination and the degree of preoperative DSH (p > 0.05).
Conversely, patients with more severe preoperative histological NP scores demonstrated significantly lower VAS scores during the early postoperative course (p = 0.02, r = −0.43; Fig. 3).
Fig. 3.

Patients with more severe preoperative histological nucleus pulposus degeneration scores demonstrated significantly lower VAS scores during the early postoperative course (3-month FU evaluation; p = 0.02, r = −0.43). HDS histological degeneration score, AF annulus fibrosus, NP nucleus pulposus
Whilst patients with preoperative NP scores between 7 and 9 revealed an overall ODI improvement of only 16.8 %, an ODI improvement of 29.2 % was observed for patients with preoperative HDSnucleus scores ranging between 12 and 14 points. However, statistical testing did not reveal any significance (p > 0.05).
Although it was observed that increasing stages of DDD on preoperative MRI images were associated with lower VAS levels during the early postoperative course, statistical analysis similarly did not reveal any significance (p = 0.057).
Discussion
Lumbar degenerative disc disease
Clinically symptomatic low back pain (LBP) is multifactorially influenced. Degenerative changes resulting from lumbar degenerative disc disease (DDD) have been associated with a negative impact on the clinical manifestation of LBP. Hereditary as well as mechanical factors have been discussed in the pathogenesis of DDD, and experimental studies demonstrated that the degenerative cascade can be initiated with a mere needle puncture into the disc [27, 38, 40, 43–46, 61–63]. Once initiated, the degenerative process is progressive, irreversible and closely associated with a mechanical dysfunction of the affected segment. A quantitative assessment of the degree of DDD has been performed via invasive and non-invasive means, including X-ray, MRI as well as histological evaluations.
Sequelae of lumbar disc degeneration
The first degenerative structural changes in human lumbar intervertebral discs can be observed histologically. As a consequence of diminished blood supply, clefts and tears within the disc become evident from the age of 15 years, the cell density decreases, accompanied by a steady increase in structural defects which extend into the annulus [38, 57, 58, 64]. The initial stages of the degenerative cascade can first be observed in the endplates, followed by nucleus and finally annulus tissue [38, 57–59].
Secondary stages of DDD are characterized by a loss of fluid content which can be detected on MRI images [39, 53, 56, 65]. Thereafter, the degenerative cascade will result in a loss of intervertebral disc space height (DSH) which from then on can be observed on X-ray images. Depending on the degree of DDD, these degenerative changes have been shown to have a significant influence on the biomechanics and kinematics of a lumbar motion segment [38, 39, 41, 45, 65–71].
The goal of this current study was therefore to analyze the above mentioned parameters of DDD and to establish their influence on motion preserving technologies with total lumbar disc replacement.
Interdependence between parameters of DDD
In accordance with these above mentioned studies and as a consequence of the degenerative cascade of disc degeneration, our results demonstrated a significant correlation and interdependence between the various parameters of DDD.
The degenerative changes in NP tissue samples were significantly more pronounced in comparison to those of AF material (p < 0.001) [38, 57–59].
X-ray evaluation of anterior and posterior DSH revealed a significant and strong correlation between each other (p < 0.001, r = 0.79). Interestingly, this homogenous progression of disc degeneration was not confirmed in our histological analysis between NP and AF tissue samples (p > 0.05). These results indicate that the degenerative cascade in the AF follows NP degenerative changes at delayed time intervals and to a varying extent, and that different underlying pathomechanisms may initiate and sustain the degenerative cascade within the AF and NP material.
DDD versus preoperative clinical symptomatology
The question as to whether the degree of DSH and disc degeneration corresponds with the patient’s symptomatology has been the subject of previous studies [52, 69, 72–75]. None of these studies were able to find a significant correlation between the DSH and the patient’s complaints. Our study similarly confirms that the preoperative DSH was not correlated with the patient’s pain severity in terms of VAS or ODI scores (p > 0.05).
Furthermore, we investigated whether MRI and histological parameters of DDD were correlated with preoperative VAS and ODI scores in order to establish whether morphological degenerative changes have an impact on the patient’s pain severity. Since histological and cellular investigations have previously demonstrated neural innervations in NP and AF tissue samples, it was one of the aims of this study to assess whether progressive histological degenerative changes, in particular those of AF tissue samples, are associated with increasing pain levels preoperatively [38, 76]. This hypothesis was not confirmed, and the current data did not provide a significant correlation between the clinical data and the histological results (p > 0.05).
In summary, none of the statistical tests performed in this study demonstrated any significant correlation between the morphological degenerative changes and the patient’s clinical symptomatology (p > 0.05).
Total lumbar disc replacement
Fusion of lumbar motion segments has been associated with a variety of early and late complications in a considerable number of patients [1–12]. In an attempt to avoid these fusion-related negative side effects, motion preserving technologies such as total lumbar disc replacement (TDR) procedures have been introduced. Their clinical efficacy has been demonstrated by a variety of class I to class IV studies worldwide [13–26].
Despite the widespread clinical application of TDR, the adequate extent of preoperative DDD remains controversially debated, the number of previously published studies is scarce and the limited data available reveal contradictory results. The fact that access to in vivo human histological tissue samples is challenging explains the paucity of currently available studies that have investigated the influence of DDD on the patient’s symptomatology in a clinical setting. To date, no study has specifically investigated the influence of different parameters of DDD and their possible role as a predictor of outcome in a prospective clinical trial setting for a cohort of TDR candidates.
Contraindications against TDR
Moore et al. [27] were able to show delayed but significant changes of the facet joints at the index and adjacent levels during the progressive stages of DDD in a standardized animal model of disc degeneration. Significant preoperative facet joint degeneration remains a commonly agreed upon contraindication against TDR [28–31]. Thus, well-justified concern arises from possible degenerative changes in the facet joints with increasing stages of disc degeneration. Furthermore, advanced stages of disc space collapse may also require more excessive intraoperative release, which similarly bears the potential to impair the postoperative outcome. Freeman et al. [77] therefore concluded that TDR may be limited to the treatment of DDD at the early stages.
Based on these concerns, different study groups have independently defined various contraindications against TDR. Zeh et al. and Lemaire et al. reported that a reduction in DSH of >50 % was considered a contraindication against TDR [20, 32]. Other authors defined an absolute DSH value of 4 mm as inclusion/exclusion criteria [30, 31, 33]. A disc space height of more or less than 4 mm was considered one of the criteria for prime, good, borderline or poor indication for TDR by Bertagnoli et al. [34].
Influence of preoperative DDD on the outcome of TDR
Since their introduction, these previously defined contraindications have not been evaluated or confirmed with evidence based data. Yaszai et al. [78] recently reported that optimal pre or postoperative disc height did not translate into an improved clinical outcome in a 2-year FU study. Other studies did not report a significant influence of preoperative DSH on postoperative VAS and ODI scores, and patients with more collapsed DSH even revealed higher patient satisfaction rates [55].
Similarly, the data compiled from this study did not reveal a negative impact of increasing stages of preoperative disc degeneration on postoperative outcome. In particular, there was no preoperative DDD threshold value for any one of the parameters investigated from which an inferior postoperative outcome could have been deduced.
Conversely, patients with more severe preoperative HDS scores of NP samples demonstrated significantly lower VAS scores during the early postoperative course (p = 0.02, r = −0.43; Fig. 3).
Although not statistically significant, patients with advanced HDS-NP scores also showed signs of greater overall improvement from preoperative ODI levels (p = 0.056), whilst patients with advanced stages of disc degeneration (MRI grading) revealed lower VAS-levels during the early postoperative course (p = 0.057).
Clinical implications
In a previous study it has been hypothesized that more rigid and collapsed segments could potentially compensate for increased axial rotational instability, one of TDR’s perceived negative side effects [55, 79–81].
Biomechanical studies have furthermore demonstrated that destabilizing effects following PLL resection can be reversed using a higher implant [82, 83]. According to the authors, the increased laxity is taken up by disc space restoration [83], and the prosthesis height seemed to be more crucial than PLL preservation to maintain the primary stability after TDR [82]. Since the vast majority of all patients (n = 47/51; 92.2 %) were treated with the same implant heights (10 mm), stabilizing effects in this particular cohort can furthermore be explained by means of increasing distraction in patients with smaller preoperative disc space heights.
Thus, the clinical data obtained from this study did not confirm a negative effect of increasing stages of DDD on the postoperative outcome following TDR, and, contrary to our primary working hypothesis, revealed some advantageous effects postoperatively. These positive effects can possibly be referred to increasing segmental rigidity resulting from morphological changes with increasing stages of DDD on the one hand as well as restabilizing effects from slightly more distraction in degenerated segments on the other hand.
In accordance with the results published by Moore et al. who demonstrated delayed degenerative changes of the facet joints during progressive stages of DDD, our data reveal a therapeutic window for TDR in a cohort of patients with various stages of DDD as long as preoperative facet joint complaints or degenerative facet arthropathies can be excluded and stringent preoperative decision making criteria are adhered to. This implies that previously published absolute disc space heights which have been defined as threshold values and contraindications against TDR should be reconsidered.
Conclusion
Histological, X-ray and MRI parameters of disc degeneration demonstrated a significant interdependence amongst each other preoperatively but showed no correlation with the patient’s clinical symptomatology.
Increasing stages of disc degeneration did not negatively impact the outcome following TDR in a highly selected patient population. No preoperative DDD threshold value was identified from which an inferior postoperative outcome could have been deduced. Conversely, potential advantageous effects on the postoperative outcome were detected in patients with advanced stages of DDD. The combined effects of increasing morphological structural rigidity of the index segment and restabilizing effects from larger distraction in degenerated segments may compensate for increasing axial rotational instability, one perceived disadvantage of TDR procedures.
Our data reveal a “therapeutic window” for TDR in a cohort of patients with various stages of DDD as long as preoperative facet joint complaints or degenerative facet arthropathies can be excluded and stringent preoperative decision making criteria are adhered to. Previously published absolute DSH values as a contraindication against TDR should be reconsidered.
Acknowledgment
The authors of this study would like to thank Pauline Jansen van Rensburg of “The Language Laboratory”, Munich, for the proof reading and editing of this article.
Conflict of interest
None.
References
- 1.Gillet P. The fate of the adjacent motion segments after lumbar fusion. J Spinal Disord Tech. 2003;16:338–345. doi: 10.1097/00024720-200308000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Goulet JA, Senunas LE, DeSilva GL, Greenfield ML (1997) Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop Relat Res 76–81 [DOI] [PubMed]
- 3.Kumar MN, Jacquot F, Hall H. Long-term follow-up of functional outcomes and radiographic changes at adjacent levels following lumbar spine fusion for degenerative disc disease. Eur Spine J. 2001;10:309–313. doi: 10.1007/s005860000207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee CK. Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine. 1988;13:375–377. doi: 10.1097/00007632-198803000-00029. [DOI] [PubMed] [Google Scholar]
- 5.Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine. 2004;29:1938–1944. doi: 10.1097/01.brs.0000137069.88904.03. [DOI] [PubMed] [Google Scholar]
- 6.Umehara S, Zindrick MR, Patwardhan AG, Havey RM, Vrbos LA, Knight GW, Miyano S, Kirincic M, Kaneda K, Lorenz MA. The biomechanical effect of postoperative hypolordosis in instrumented lumbar fusion on instrumented and adjacent spinal segments. Spine. 2000;25:1617–1624. doi: 10.1097/00007632-200007010-00004. [DOI] [PubMed] [Google Scholar]
- 7.Katz V, Schofferman J, Reynolds J. The sacroiliac joint: a potential cause of pain after lumbar fusion to the sacrum. J Spinal Disord Tech. 2003;16:96–99. doi: 10.1097/00024720-200302000-00015. [DOI] [PubMed] [Google Scholar]
- 8.Maigne JY, Planchon CA. Sacroiliac joint pain after lumbar fusion. A study with anesthetic blocks. Eur Spine J. 2005;14:654–658. doi: 10.1007/s00586-004-0692-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ha KY, Lee JS, Kim KW. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up. Spine. 2008;33:1192–1198. doi: 10.1097/BRS.0b013e318170fd35. [DOI] [PubMed] [Google Scholar]
- 10.Moshirfar A, Jenis LG, Spector LR, Burke PJ, Losina E, Katz JN, Rand FF, Tromanhauser SG, Banco RJ. Computed tomography evaluation of superior-segment facet-joint violation after pedicle instrumentation of the lumbar spine with a midline surgical approach. Spine. 2006;31:2624–2629. doi: 10.1097/01.brs.0000240691.35707.e8. [DOI] [PubMed] [Google Scholar]
- 11.Shah RR, Mohammed S, Saifuddin A, Taylor BA. Radiologic evaluation of adjacent superior segment facet joint violation following transpedicular instrumentation of the lumbar spine. Spine. 2003;28:272–275. doi: 10.1097/01.BRS.0000042361.93572.74. [DOI] [PubMed] [Google Scholar]
- 12.Cardoso MJ, Dmitriev AE, Helgeson M, Lehman RA, Kuklo TR, Rosner MK. Does superior-segment facet violation or laminectomy destabilize the adjacent level in lumbar transpedicular fixation? An in vitro human cadaveric assessment. Spine. 2008;33:2868–2873. doi: 10.1097/BRS.0b013e31818c63d3. [DOI] [PubMed] [Google Scholar]
- 13.Blumenthal S, McAfee PC, Guyer RD, Hochschuler SH, Geisler FH, Holt RT, Garcia R, Jr, Regan JJ, Ohnmeiss DD. A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine. 2005;30:1565–1575. doi: 10.1097/01.brs.0000170587.32676.0e. [DOI] [PubMed] [Google Scholar]
- 14.Cinotti G, David T, Postacchini F. Results of disc prosthesis after a minimum follow-up period of 2 years. Spine. 1996;21:995–1000. doi: 10.1097/00007632-199604150-00015. [DOI] [PubMed] [Google Scholar]
- 15.David T. Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITE artificial disc in 106 patients. Spine. 2007;32:661–666. doi: 10.1097/01.brs.0000257554.67505.45. [DOI] [PubMed] [Google Scholar]
- 16.Delamarter RB, Fribourg DM, Kanim LE, Bae H. ProDisc artificial total lumbar disc replacement: introduction and early results from the United States clinical trial. Spine. 2003;28:S167–175. doi: 10.1097/01.BRS.0000092220.66650.2B. [DOI] [PubMed] [Google Scholar]
- 17.Guyer RD, McAfee PC, Banco RJ, Bitan FD, Cappuccino A, Geisler FH, Hochschuler SH, Holt RT, Jenis LG, Majd ME, Regan JJ, Tromanhauser SG, Wong DC, Blumenthal SL (2009) Prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: five-year follow-up. Spine J 9:374–386 [DOI] [PubMed]
- 18.Hochschuler SH, Ohnmeiss DD, Guyer RD, Blumenthal SL. Artificial disc: preliminary results of a prospective study in the United States. Eur Spine J. 2002;11(Suppl 2):S106–110. doi: 10.1007/s00586-002-0439-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Huec JC, Basso Y, Aunoble S, Friesem T, Bruno MB. Influence of facet and posterior muscle degeneration on clinical results of lumbar total disc replacement: two-year follow-up. J Spinal Disord Tech. 2005;18:219–223. [PubMed] [Google Scholar]
- 20.Lemaire JP, Carrier H, Ali HS, Skalli W, Lavaste F. Clinical and radiological outcomes with the Charite artificial disc: a 10-year minimum follow-up. J Spinal Disord Tech. 2005;18:353–359. doi: 10.1097/01.bsd.0000172361.07479.6b. [DOI] [PubMed] [Google Scholar]
- 21.McAfee PC, Cunningham B, Holsapple G, Adams K, Blumenthal S, Guyer RD, Dmietriev A, Maxwell JH, Regan JJ, Isaza J. A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes. Spine. 2005;30:1576–1583. doi: 10.1097/01.brs.0000170561.25636.1c. [DOI] [PubMed] [Google Scholar]
- 22.Sasso RC, Foulk DM, Hahn M. Prospective, randomized trial of metal-on-metal artificial lumbar disc replacement: initial results for treatment of discogenic pain. Spine. 2008;33:123–131. doi: 10.1097/BRS.0b013e31816043af. [DOI] [PubMed] [Google Scholar]
- 23.Tropiano P, Huang RC, Girardi FP, Cammisa FP, Jr, Marnay T. Lumbar total disc replacement. Seven to eleven-year follow-up. J Bone Joint Surg Am. 2005;87-A:490–496. doi: 10.2106/JBJS.C.01345. [DOI] [PubMed] [Google Scholar]
- 24.Zigler J, Delamarter R, Spivak JM, Linovitz RJ, Danielson GO, 3rd, Haider TT, Cammisa F, Zuchermann J, Balderston R, Kitchel S, Foley K, Watkins R, Bradford D, Yue J, Yuan H, Herkowitz H, Geiger D, Bendo J, Peppers T, Sachs B, Girardi F, Kropf M, Goldstein J. Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine. 2007;32:1155–1162. doi: 10.1097/BRS.0b013e318054e377. [DOI] [PubMed] [Google Scholar]
- 25.Siepe CJ, Mayer HM, Heinz-Leisenheimer M, Korge A. Total lumbar disc replacement: different results for different levels. Spine. 2007;32:782–790. doi: 10.1097/01.brs.0000259071.64027.04. [DOI] [PubMed] [Google Scholar]
- 26.Siepe CJ, Mayer HM, Wiechert K, Korge A. Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine. 2006;31:1923–1932. doi: 10.1097/01.brs.0000228780.06569.e8. [DOI] [PubMed] [Google Scholar]
- 27.Moore RJ, Crotti TN, Osti OL, Fraser RD, Vernon-Roberts B. Osteoarthrosis of the facet joints resulting from anular rim lesions in sheep lumbar discs. Spine. 1999;24:519–525. doi: 10.1097/00007632-199903150-00003. [DOI] [PubMed] [Google Scholar]
- 28.Huang RC, Lim MR, Girardi FP, Cammisa FP., Jr The prevalence of contraindications to total disc replacement in a cohort of lumbar surgical patients. Spine. 2004;29:2538–2541. doi: 10.1097/01.brs.0000144829.57885.20. [DOI] [PubMed] [Google Scholar]
- 29.McAfee PC. The indications for lumbar and cervical disc replacement. Spine J. 2004;4:177S–181S. doi: 10.1016/j.spinee.2004.07.003. [DOI] [PubMed] [Google Scholar]
- 30.Wong DA, Annesser B, Birney T, Lamond R, Kumar A, Johnson S, Jatana S, Ghiselli G. Incidence of contraindications to total disc arthroplasty: a retrospective review of 100 consecutive fusion patients with a specific analysis of facet arthrosis. Spine J. 2007;7:5–11. doi: 10.1016/j.spinee.2006.04.012. [DOI] [PubMed] [Google Scholar]
- 31.Chin KR. Epidemiology of indications and contraindications to total disc replacement in an academic practice. Spine J. 2007;7:392–398. doi: 10.1016/j.spinee.2006.08.009. [DOI] [PubMed] [Google Scholar]
- 32.Zeh A, Planert M, Siegert G, Lattke P, Held A, Hein W. Release of cobalt and chromium ions into the serum following implantation of the metal-on-metal Maverick-type artificial lumbar disc (Medtronic Sofamor Danek) Spine. 2007;32:348–352. doi: 10.1097/01.brs.0000253599.89694.c0. [DOI] [PubMed] [Google Scholar]
- 33.Chung SS, Lee CS, Kang CS. Lumbar total disc replacement using ProDisc II: a prospective study with a 2-year minimum follow-up. J Spinal Disord Tech. 2006;19:411–415. doi: 10.1097/00024720-200608000-00007. [DOI] [PubMed] [Google Scholar]
- 34.Bertagnoli R, Kumar S. Indications for full prosthetic disc arthroplasty: a correlation of clinical outcome against a variety of indications. Eur Spine J. 2002;11(Suppl 2):S131–136. doi: 10.1007/s00586-002-0428-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Carragee EJ, Tanner CM, Yang B, Brito JL, Truong T. False-positive findings on lumbar discography. Reliability of subjective concordance assessment during provocative disc injection. Spine. 1999;24:2542–2547. doi: 10.1097/00007632-199912010-00017. [DOI] [PubMed] [Google Scholar]
- 36.Carragee EJ, Chen Y, Tanner CM, Hayward C, Rossi M, Hagle C. Can discography cause long-term back symptoms in previously asymptomatic subjects? Spine. 2000;25:1803–1808. doi: 10.1097/00007632-200007150-00011. [DOI] [PubMed] [Google Scholar]
- 37.Block AR, Vanharanta H, Ohnmeiss DD, Guyer RD. Discographic pain report. Influence of psychological factors. Spine. 1996;21:334–338. doi: 10.1097/00007632-199602010-00017. [DOI] [PubMed] [Google Scholar]
- 38.Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31:2151–2161. doi: 10.1097/01.brs.0000231761.73859.2c. [DOI] [PubMed] [Google Scholar]
- 39.Berlemann U, Gries NC, Moore RJ. The relationship between height, shape and histological changes in early degeneration of the lower lumbar discs. Eur Spine J. 1998;7:212–217. doi: 10.1007/s005860050058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Carragee EJ, Don AS, Hurwitz EL, Cuellar JM, Carrino J, Herzog R. 2009 ISSLS Prize Winner: does discography cause accelerated progression of degeneration changes in the lumbar disc: a ten-year matched cohort study. Spine (Phila Pa 1976) 2009;34:2338–2345. doi: 10.1097/BRS.0b013e3181ab5432. [DOI] [PubMed] [Google Scholar]
- 41.Fujiwara A, Lim TH, An HS, Tanaka N, Jeon CH, Andersson GB, Haughton VM. The effect of disc degeneration and facet joint osteoarthritis on the segmental flexibility of the lumbar spine. Spine. 2000;25:3036–3044. doi: 10.1097/00007632-200012010-00011. [DOI] [PubMed] [Google Scholar]
- 42.Fujiwara A, Tamai K, Yamato M, An HS, Yoshida H, Saotome K, Kurihashi A. The relationship between facet joint osteoarthritis and disc degeneration of the lumbar spine: an MRI study. Eur Spine J. 1999;8:396–401. doi: 10.1007/s005860050193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hsieh AH, Hwang D, Ryan DA, Freeman AK, Kim H. Degenerative anular changes induced by puncture are associated with insufficiency of disc biomechanical function. Spine. 2009;34:998–1005. doi: 10.1097/BRS.0b013e31819c09c4. [DOI] [PubMed] [Google Scholar]
- 44.Korecki CL, Costi JJ, Iatridis JC. Needle puncture injury affects intervertebral disc mechanics and biology in an organ culture model. Spine. 2008;33:235–241. doi: 10.1097/BRS.0b013e3181624504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Masuda K, Aota Y, Muehleman C, Imai Y, Okuma M, Thonar EJ, Andersson GB, An HS. A novel rabbit model of mild, reproducible disc degeneration by an anulus needle puncture: correlation between the degree of disc injury and radiological and histological appearances of disc degeneration. Spine. 2005;30:5–14. doi: 10.1097/01.brs.0000148152.04401.20. [DOI] [PubMed] [Google Scholar]
- 46.Nassr A, Lee JY, Bashir RS, Rihn JA, Eck JC, Kang JD, Lim MR. Does incorrect level needle localization during anterior cervical discectomy and fusion lead to accelerated disc degeneration? Spine. 2009;34:189–192. doi: 10.1097/BRS.0b013e3181913872. [DOI] [PubMed] [Google Scholar]
- 47.Mayer HM, Wiechert K. Microsurgical anterior approaches to the lumbar spine for interbody fusion and total disc replacement. Neurosurgery. 2002;51:S159–165. doi: 10.1097/00006123-200211002-00022. [DOI] [PubMed] [Google Scholar]
- 48.Mayer HM, Wiechert K, Korge A, Qose I. Minimally invasive total disc replacement: surgical technique and preliminary clinical results. Eur Spine J. 2002;11(Suppl 2):S124–130. doi: 10.1007/s00586-002-0446-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Bertagnoli R, Marnay T, Mayer HM. The ProDisc book spine solutions GmbH. Germany: Tuttlingen; 2003. [Google Scholar]
- 50.Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;66:271–273. [PubMed] [Google Scholar]
- 51.Ravi B, Rampersaud R. Clinical magnification error in lateral spinal digital radiographs. Spine (Phila Pa 1976) 2008;33:E311–316. doi: 10.1097/BRS.0b013e31816f6c3f. [DOI] [PubMed] [Google Scholar]
- 52.Dabbs VM, Dabbs LG. Correlation between disc height narrowing and low-back pain. Spine. 1990;15:1366–1369. doi: 10.1097/00007632-199012000-00026. [DOI] [PubMed] [Google Scholar]
- 53.Luoma K, Vehmas T, Riihimaki H, Raininko R. Disc height and signal intensity of the nucleus pulposus on magnetic resonance imaging as indicators of lumbar disc degeneration. Spine. 2001;26:680–686. doi: 10.1097/00007632-200103150-00026. [DOI] [PubMed] [Google Scholar]
- 54.Andersson GB, Schultz A, Nathan A, Irstam L. Roentgenographic measurement of lumbar intervertebral disc height. Spine. 1981;6:154–158. doi: 10.1097/00007632-198103000-00008. [DOI] [PubMed] [Google Scholar]
- 55.Siepe CJ, Hitzl W, Meschede P, Sharma AK, Khattab MF, Mayer MH. Interdependence between disc space height, range of motion and clinical outcome in total lumbar disc replacement. Spine. 2009;34:904–916. doi: 10.1097/BRS.0b013e31819966b0. [DOI] [PubMed] [Google Scholar]
- 56.Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001;26:1873–1878. doi: 10.1097/00007632-200109010-00011. [DOI] [PubMed] [Google Scholar]
- 57.Boos N, Weissbach S, Rohrbach H, Weiler C, Spratt KF, Nerlich AG. Classification of age-related changes in lumbar intervertebral discs: 2002 Volvo Award in basic science. Spine (Phila Pa 1976) 2002;27:2631–2644. doi: 10.1097/00007632-200212010-00002. [DOI] [PubMed] [Google Scholar]
- 58.Weiler C, Lopez-Ramos M, Mayer HM, Korge A, Siepe CJ, Wuertz K, Weiler V, Boos N, Nerlich AG (2011) Histological evidence for intervertebral disc degeneration in lumbar surgical disc tissue samples suggests statistical association to increased body mass index. BMC Res Notes 4:497. doi:10.1186/1756-0500-4-497 [DOI] [PMC free article] [PubMed]
- 59.Liebscher T, Haefeli M, Wuertz K, Nerlich AG, Boos N. Age-related variation in cell density of human lumbar intervertebral disc. Spine (Phila Pa 1976) 2011;36:153–159. doi: 10.1097/BRS.0b013e3181cd588c. [DOI] [PubMed] [Google Scholar]
- 60.Hill T, Lewicki P. Statistiks: methods and applications. Tulsa: StatSoft Inc.; 2007. [Google Scholar]
- 61.Veres SP, Robertson PA, Broom ND. ISSLS prize winner: How loading rate influences disc failure mechanics: a microstructural assessment of internal disruption. Spine (Phila Pa 1976) 2010;35:1897–1908. doi: 10.1097/BRS.0b013e3181d9b69e. [DOI] [PubMed] [Google Scholar]
- 62.Battie MC, Videman T, Parent E. Lumbar disc degeneration: epidemiology and genetic influences. Spine. 2004;29:2679–2690. doi: 10.1097/01.brs.0000146457.83240.eb. [DOI] [PubMed] [Google Scholar]
- 63.Videman T, Battie MC, Ripatti S, Gill K, Manninen H, Kaprio J. Determinants of the progression in lumbar degeneration: a 5-year follow-up study of adult male monozygotic twins. Spine. 2006;31:671–678. doi: 10.1097/01.brs.0000202558.86309.ea. [DOI] [PubMed] [Google Scholar]
- 64.Nerlich AG, Schleicher ED, Boos N. 1997 Volvo Award winner in basic science studies. Immunohistologic markers for age-related changes of human lumbar intervertebral discs. Spine (Phila Pa 1976) 1997;22:2781–2795. doi: 10.1097/00007632-199712150-00001. [DOI] [PubMed] [Google Scholar]
- 65.Frobin W, Brinckmann P, Kramer M, Hartwig E. Height of lumbar discs measured from radiographs compared with degeneration and height classified from MR images. Eur Radiol. 2001;11:263–269. doi: 10.1007/s003300000556. [DOI] [PubMed] [Google Scholar]
- 66.Kirkaldy-Willis WH, Farfan HF (1982) Instability of the lumbar spine. Clin Orthop Relat Res 110–123 [PubMed]
- 67.Rohlmann A, Zander T, Schmidt H, Wilke HJ, Bergmann G (2006) Analysis of the influence of disc degeneration on the mechanical behaviour of a lumbar motion segment using the finite element method. J Biomech 39:2484–2490 [DOI] [PubMed]
- 68.Rousseau MA, Bradford DS, Hadi TM, Pedersen KL, Lotz JC (2006) The instant axis of rotation influences facet forces at L5/S1 during flexion/extension and lateral bending. Eur Spine J 15:299–307 [DOI] [PMC free article] [PubMed]
- 69.Schulte TL, Leistra F, Bullmann V, Osada N, Vieth V, Marquardt B, Lerner T, Liljenqvist U, Hackenberg L. Disc height reduction in adjacent segments and clinical outcome 10 years after lumbar 360 degrees fusion. Eur Spine J. 2007;16:2152–2158. doi: 10.1007/s00586-007-0515-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE. Intervertebral disc degeneration reduces vertebral motion responses. Spine. 2007;32:E544–E550. doi: 10.1097/BRS.0b013e318145ac39. [DOI] [PubMed] [Google Scholar]
- 71.Acaroglu ER, Iatridis JC, Setton LA, Foster RJ, Mow VC, Weidenbaum M. Degeneration and aging affect the tensile behavior of human lumbar anulus fibrosus. Spine (Phila Pa 1976) 1995;20:2690–2701. doi: 10.1097/00007632-199512150-00010. [DOI] [PubMed] [Google Scholar]
- 72.Pope MH, Hanley EN, Matteri RE, Wilder DG, Frymoyer JW. Measurement of intervertebral disc space height. Spine. 1977;2:282–286. doi: 10.1097/00007632-197712000-00007. [DOI] [Google Scholar]
- 73.Lidar Z, Beaumont A, Lifshutz J, Maiman DJ. Clinical and radiological relationship between posterior lumbar interbody fusion and posterolateral lumbar fusion. Surg Neurol. 2005;64:303–308. doi: 10.1016/j.surneu.2005.03.025. [DOI] [PubMed] [Google Scholar]
- 74.Schepper EI, Damen J, Meurs JB, Ginai AZ, Popham M, Hofman A, Koes BW, Bierma-Zeinstra SM. The association between lumbar disc degeneration and low back pain: the influence of age, gender, and individual radiographic features. Spine (Phila Pa 1976) 2010;35:531–536. doi: 10.1097/BRS.0b013e3181aa5b33. [DOI] [PubMed] [Google Scholar]
- 75.Bendix T, Kjaer P, Korsholm L. Burned-out discs stop hurting: fact or fiction? Spine (Phila Pa 1976) 2008;33:E962–E967. doi: 10.1097/BRS.0b013e31818804b3. [DOI] [PubMed] [Google Scholar]
- 76.Coppes MH, Marani E, Thomeer RT, Groen GJ. Innervation of “painful” lumbar discs. Spine. 1997;22:2342–2349. doi: 10.1097/00007632-199710150-00005. [DOI] [PubMed] [Google Scholar]
- 77.Freeman BJ, Davenport J. Total disc replacement in the lumbar spine: a systematic review of the literature. Eur Spine J. 2006;15:439–447. doi: 10.1007/s00586-006-0186-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Yaszay B, Bendo JA, Goldstein JA, Quirno M, Spivak JM, Errico TJ. Effect of intervertebral disc height on postoperative motion and outcomes after ProDisc-L lumbar disc replacement. Spine. 2008;33:508–512. doi: 10.1097/BRS.0b013e318165b998. [DOI] [PubMed] [Google Scholar]
- 79.McAfee PC, Cunningham BW, Hayes V, Sidiqi F, Dabbah M, Sefter JC, Hu N, Beatson H. Biomechanical analysis of rotational motions after disc arthroplasty: implications for patients with adult deformities. Spine. 2006;31:S152–160. doi: 10.1097/01.brs.0000234782.89031.03. [DOI] [PubMed] [Google Scholar]
- 80.Sariali H, Lemaire JP, Pascal-Mousselard H, Carrier H, Skalli W. In vivo study of the kinematics in axial rotation of the lumbar spine after total intervertebral disc replacement: long-term results: a 10–14 years follow-up evaluation. Eur Spine J. 2006;15:1501–1510. doi: 10.1007/s00586-005-0016-5. [DOI] [PubMed] [Google Scholar]
- 81.Ching AC, Birkenmaier C, Hart RA. Short segment coronal plane deformity after two-level lumbar total disc replacement. Spine (Phila Pa 1976) 2010;35:44–50. doi: 10.1097/BRS.0b013e3181b9d556. [DOI] [PubMed] [Google Scholar]
- 82.Cakir B, Richter M, Schmoelz W, Schmidt R, Reichel H, Wilke HJ (2009) Resect or not to resect: the role of posterior longitudinal ligament in lumbar total disc replacement. Eur Spine J. doi:10.1007/s00586-009-1193-4 [DOI] [PMC free article] [PubMed]
- 83.Demetropoulos CK, Sengupta DK, Knaub MA, Wiater BP, Abjornson C, Truumees E, Herkowitz HN. Biomechanical evaluation of the kinematics of the cadaver lumbar spine following disc replacement with the ProDisc-L prosthesis. Spine (Phila Pa 1976) 2010;35:26–31. doi: 10.1097/BRS.0b013e3181c4eb9a. [DOI] [PubMed] [Google Scholar]