

Abstract
This report describes an unusual case of bilaterally symmetrically occurring hyperpigmented itchy popular lesions on both forearms of a 50-year-old woman. The woman had antecedent hyperkeratotic eczema of the feet and she had a similar eruption in the past which had cleared with topical steroid application. Biopsy of the lesion showed syringomas. We present this case to highlight an unusual case of bilaterally symmetrical papular pruritic eruption against a background of hyperkeratotic eczema. Some syringomas are supposed to be a response to an inflammatory trigger and we wonder if in this case the eczema acted as an inflammatory trigger.
Keywords: Eruptive syringomas, forearms, itching, upper extremities
INTRODUCTION
A 50-year-old patient, who was under treatment for eczema of the feet, presented with itchy papular eruptions of both forearms. She had two such episodes, one of which resolved once with topical steroids and once spontaneously. The biopsy showed syringomas. The diagnosis of eruptive, pruritic syringomas localized to only both forearms is rare. We do not know if the hyperkeratotic eczema distant to the lesions was a coincidental finding in the light of some workers suggesting that some eruptive syringomas may be reactive to an inflammatory trigger.
CASE REPORT
A 50-year-old woman under treatment for hyperkeratotic eczema of the feet presented in this clinic with mildly itchy lesions on both forearms for the past few weeks. She said that they had appeared twice in the past 4 years over the same areas during summer and were once treated with topical steroids and once resolved spontaneously; however, the authenticity of these observations cannot be ascertained as the patient was new to this clinic. On examination, there were multiple 2–4 mm, non-scaly, skin-colored, flattened, light brown papules on both her forearms with relative sparing of the medial aspect [Figures 1 and 2]. No other body areas were affected and the previous two appearances were in the same area according to the patient. She had no other problems except her hyperkeratotic eczema of long standing. She was mildly obese, but euglycemic, euthyroid, normotensive and was on no drugs. A biopsy of one lesion from the forearm showed several ductal structures lined by a double epithelium with cells containing abundant cytoplasm and elongated tadpole-like epithelial cells in the upper reticular dermis [Figures 3 and 4]. The collagen was sclerotic. There was no inflammatory infiltrate surrounding the ductal structures. The epidermis was unremarkable except mild acanthosis. A few short cords of eccrine ductal epithelium were seen. A diagnosis of bilaterally symmetrical eruptive syringomas on forearms with itching was made. The condition was explained to the patient and she decided not to take any treatment after being told the benign nature of the disease. The case is being reported for its rarity owing to the very unusual features of bilateral symmetrical eruptive syringomas localized only to both forearms with mild itching and two long remissions.
Figure 1.

Bilaterally symmetrical syringomas on the forearms in a patient of hyperkeratotic foot eczema
Figure 2.

Close-up of syringomas of forearms
Figure 3.
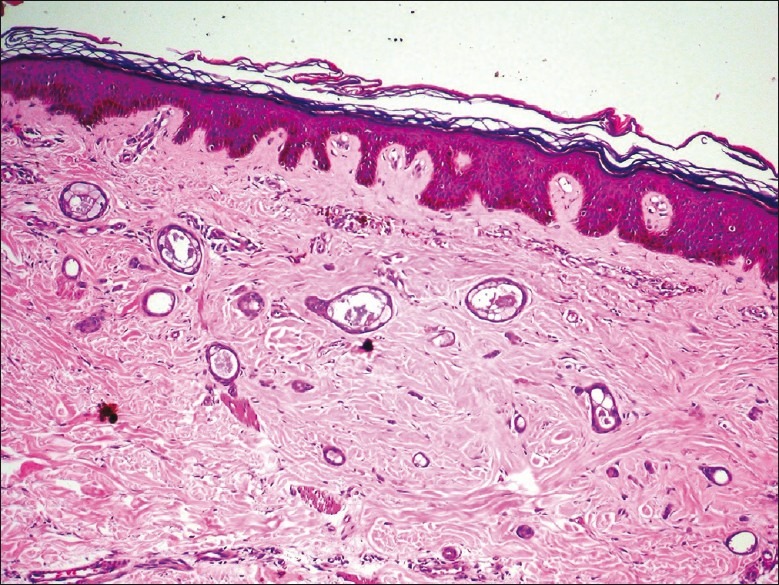
Elongated, tadpole like ductal structures (H and E, ×10)
Figure 4.
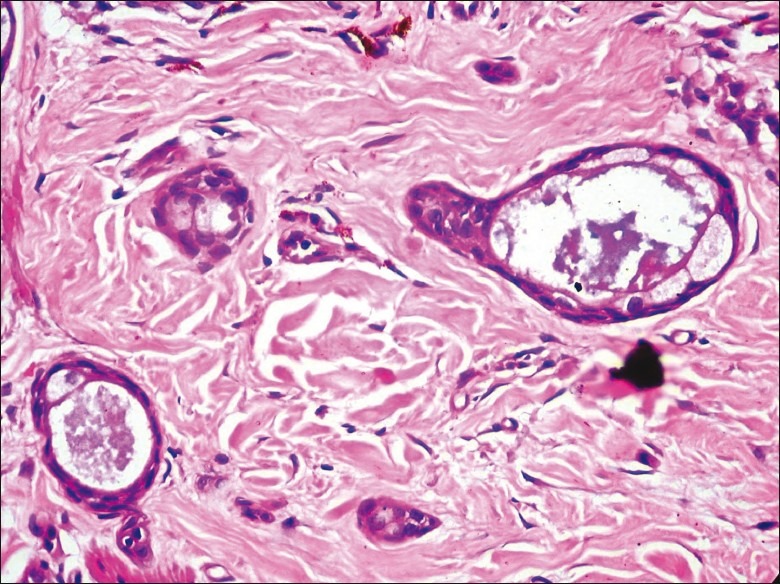
Elongated, tadpole like ductal structures (H and E, ×40)
DISCUSSION
Syringomas are benign eccrine sweat gland tumors of the acrosyringium. Eruptive syringomas were first described by Jacquet and Darier in 1887. The commonest ones are found around the eyelids of women. There is a marked female predominance even in the rare eruptive form.[1] The largest series of eruptive syringomas published in this decade and the second largest in world literature describes a rate of 1/2500 biopsies, which shows its rarity.[1] There are less than 100 cases of eruptive syringomas reported in the world literature.[1,2] In 33–50% of cases, they appear before the age of 15 years.[1] A classification of syringomas categorizing them into localized, familial, associated with Down's syndrome and generalized eruptive variants has been suggested.[3]
Eruptive syringomas are asymptomatic, yellowish to brown, non-scaly, flat-topped papules. They occur on face, neck, anterior trunk, axillae, and genitalia and can come in successive crops as was seen in this patient.[1,4,5] There are just six reports of involvement localized to upper extremities and even less for bilateral symmetrical localized as seen in this case.[4,6–9] General experience and two of the largest series indicate that they are asymptomatic and pruritus occurs very rarely as seen in our case.[4,10]
Other unusual features of eruptive syringomas include unilateral nevoid, linear, bathing trunk, milia like, in association with neoplasms and familial.[1–5,9] They are more common in patients with Down's syndrome.[1,3] Syringomatous changes have been reported in cases of diffuse alopecia, alopecia areata, prurigo nodularis and melanocytic nevi.[1–3,5,9] There is also a proposal that some of these eruptive syringomas may occur as a reactive hyperplasia of the eccrine duct to an inflammatory trigger rather than be truly neoplastic in origin.[11] We cannot comment on whether our patient's hyperkertatotic eczema of the feet is coincidental or otherwise.
This case is being reported for its clearly rare features. It is most unusual to see late onset, itchy, eruptive syringomas localized to the forearms. The coexistence of hyperkeratotic eczema of the feet may be a red herring, but needs to be studied further.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Soler-Carrillo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242–6. doi: 10.1046/j.1468-3083.2001.00235.x. [DOI] [PubMed] [Google Scholar]
- 2.Seirafi HH, Akhyani M, Naraghi ZS, Mansoori P, Dehkordi HS, Taheri A, et al. Eruptive syringomas. Dermatol Online J. 2005;11:13. [PubMed] [Google Scholar]
- 3.Friedman SJ, Butler DF. Syringoma presenting as milia. J Am Acad Dermatol. 1987;16:310–4. doi: 10.1016/s0190-9622(87)70041-3. [DOI] [PubMed] [Google Scholar]
- 4.Patrizi A, Neri I, Marzaduri S, Varotti E, Passarini B. Syringoma: a review of twenty-nine cases. Acta Derm Venereol. 1998;78:460–2. doi: 10.1080/000155598442791. [DOI] [PubMed] [Google Scholar]
- 5.Calonje E, MackKie RM. Tumors of the Skin Appendages. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 5th ed. Vol. 2. Oxford: Blackwell Science; 2004. pp. 20–1. [Google Scholar]
- 6.van den Broek H, Lundquist CD. Syringomas of the upper extremities with onset in the sixth decade. J Am Acad Dermatol. 1982;6:534–6. doi: 10.1016/s0190-9622(82)80368-x. [DOI] [PubMed] [Google Scholar]
- 7.Metze D, Jurecka W, Gebhart W. Disseminated syringomas of the upper extremities.Case history and immunohistochemical and ultrastructural study. Dermatologica. 1990;180:228–35. [PubMed] [Google Scholar]
- 8.Hughes PS, Apisarnthanarax P. Acral syringoma. Arch Dermatol. 1977;113:1435–6. [PubMed] [Google Scholar]
- 9.Berbis P, Fabre JF, Jancovici E, Privat Y, Benderitter T. Late-onset syringomas of the upper extremities associated with a carcinoid tumor. Arch Dermatol. 1989;125:848–9. [PubMed] [Google Scholar]
- 10.Kuttner BJ, Kaplan DL, Rothstein MS. Eruptive pruritic papules. Arch Dermatol. 1989;125:985–90. doi: 10.1001/archderm.1989.01670190119017. [DOI] [PubMed] [Google Scholar]
- 11.Guitart J, Rosenbaum MM, Requena L ,Eruptive syringoma‘: a misnomer for a reactive eccrine gland ductal proliferation? J Cutan Pathol. 2003;30:202–5. doi: 10.1034/j.1600-0560.2003.00023.x. [DOI] [PubMed] [Google Scholar]