

Abstract
Aim:
The aim of this in vitro study was to evaluate the flexural strength of a composite resin polymerized with three different modes of light exposure.
Materials and Methods:
The three different modes of light exposure were conventional, 600 mW/cm2/40s; soft start, 300 mW/cm2/10s + 600 mW/cm2/30s; pulse delay, 600 mW/cm2/1s + 60 s of waiting time + 600 mW/cm2/39s). Twenty samples were prepared for each polymerization method. Flexural strength (FS) tests were carried out with a 2 kN load at a speed of 0.5 mm/ min. All tested groups were submitted to analysis of variance (one-way-ANOVA) and Tukey's test (P < 0.05).
Results:
When stored in water, conventional and pulse delay groups presented higher FS values which were statistically different from the soft start group. When stored in 100% ethanol, conventional and soft start groups presented higher FS values which were statistically different from the pulse delay group.
Conclusion:
Different polymerization modes and immersion media can affect the physical properties (flexural strength) of composite resin.
Keywords: Composites resins, flexural strength, polymerization modes, storage media
INTRODUCTION
The appropriate polymerization of resin composites is a crucial factor in the clinical performance of restorations. Several problems can be associated with inadequate polymerization, such as: reduced physical properties, solubility in the oral environment, microleakage and pulp irritation.[1,2] The process of composite resin polymerization occurs through the conversion of the monomer molecules into a polymer network, accompanied by the narrowing of the space between the molecules which causes polymerization shrinkage in the composite.[3] When greater intensity of light energy is used for composite resin polymerization, larger amounts of photons reach the molecules of the photo-initiator within the resin, and more photoinitiator molecules are activated and raised to the excited state. In this excited state, the camphoroquinone collides with the amine, forming a free radical which then reacts with the double carbon bond (C = C), that are converted to single bonds (C-C) and begins polymerization.[4]
Some light polymerization techniques have been proposed in an attempt to decrease the stresses generated during the polymerization shrinkage of composite resins, such as the soft-start and pulse delay techniques.[5] Despite the fact that the degree of conversion of a monomer is the same with different polymerization modes, it is hypothesized that the formed polymer can have different structures, because of the slow pre-cure of some methods such as pulse delay.[6] In this sense, studies have shown some differences in some of the physical properties, like knoop hardness,[7] shear strength and diametral tensile strength, especially when the resin composite is immersed in ethanol.[6,8] Ethanol causes softening of the resin composite surface by removing the polymer structure as unreacted monomers, oligomers and linear polymers.[6] Thus, the aim of in this study was to investigate the effect of different modes of light exposure (conventional, soft start and pulse delay) and water or ethanol immersion on the flexural strength of a composite resin.
MATERIALS AND METHODS
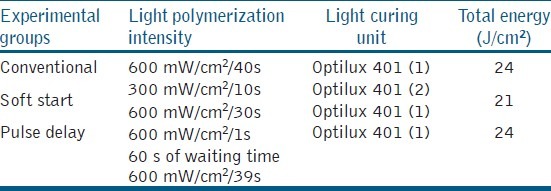
To conduct this study, a composite resin (Z350, 3M ESPE Dental Products, St Paul, MN, USA) was used. Sixty rectangular samples were prepared using steel moulds, with internal dimensions of 10 mm length, 2 mm width and 2 mm thickness,[9] totaling twenty samples for each light polymerization mode. The space in the mould was filled with composite resin in one increment. The surface of the restorative materials was covered with a polyester strip and a glass slide to flatten the surface. A 1 kg load was placed on the resin composite for 10 s. After the load and the glass slide were removed each test specimen was randomly polymerized using an Optilux 401 unit (Demetron/Kerr, Danbury, CT, USA), according to the three experimental light polymerization mode groups: conventional method (600 mW/cm2/40 sec.), pulse delay (600 mW/cm2/1 sec, 60s of waiting time + 600 mW/cm2/39 sec.) and soft start (300 mW/cm2/10 sec. 600 mW/cm2/30 sec.). Two units were used, Optilux 401 - one with 600mW/cm2 (1) and another with 300 mW/cm2 (2), as shown in Table 1.
Table 1.
Experimental polymerization modes in the study
Power density was periodically checked using a radiometer (Model 100 Optilux Radiometer, SDS Kerr, Danbury, CT, USA). Immediately after making each specimen test, the excess resin composite was removed with a scalpel blade No.12 and abrasive paper No.320 under water spray, and specimen thickness was gauged with a digital Pachymeter (Mitutoyo, Tokyo, Japan) accurate to two decimal places.
Following this, the values were recorded. All specimens were randomly assigned to one of the two media: distilled water for 24 h or 100% ethanol for 14 days.
The Flexural Strength (FS) tests were performed using the universal mechanical test equipment EMIC DL2000 (EMIC, São José dos Pinhais, PR - Brazil), with a 2 kN load and speed of 0.5 mm/min. The FS was calculated as follows:
![]()
- where FS is the flexural strength (in MPa); L, the failure load (in Newtons); D, the distance between the supports (in mm); w, the width; and h, the height of the specimen (both in mm). Data were submitted to analysis of variance (one-way ANOVA). Tukey's test was applied for multiple comparisons, with significance level set at 5%.
RESULTS
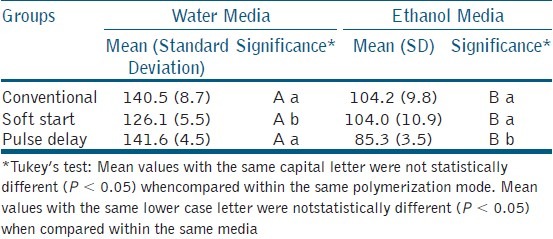
The mean flexural strength values (MPa), standard deviations (SD) and statistical results of the restorative materials are presented in Table 2. The ANOVA showed a statistically significant difference among experimental groups (P < 0.001). The Tukey's test showed statistical differences between the two immersion media. Independent of the experimental polymerization mode, all samples immersed in ethanol presented lower flexural strength values than those immersed in water. With regards to the polymerization modes it was observed that for the samples immersed in water, the pulse delay and the conventional polymerization modes showed the highest FS means, and were statistically different from the soft start. For the samples immersed in ethanol, the conventional and soft start polymerization modes showed the highest FS means, and were statistically different from pulse delay.
Table 2.
Results of flexural strength means for the experimental groups (MPa), standard deviation (SD) and significance
DISCUSSION
Different polymerization techniques such as those tested in this study (soft start and pulse delay) have been proposed in an attempt to reduce the stress caused by polymerization shrinkage generated at the time of photoactivation. There is a general consensus about the reduction of polymerization shrinkage stress,[7] but apparently structures of polymer chains with fewer cross-links are generated.[10] An alternative method, as used in this study, is the immersion of samples in organic solvents such as ethanol and subsequent mechanical test. Considering that polymers with higher degrees of cross-links are more resistant to degradation caused by organic solvents, it becomes interesting to investigate the polymerization method associated to ethanol immersion.
Clinically, composite restorations can be subjected to considerable flexural stresses in both anterior and posterior teeth. At present, biomaterial performance is frequently evaluated using laboratory tests.[11] The physical properties of a restorative material is indicative of how the material will function under stress in the oral environment, indirectly determining the resistance to fracture in the areas of great masticatory effort.[12,13] The parameters for performing the flexural strength test are supplied by the ISO specification 4049 - (International Organization for Standardization – ISO, 2000).[14] However, in resin composite evaluations, the difficulty of polymerizing large specimens (25 mm), as recommended, with a light source of reduced diameter (± 11 mm) can influence the results. For this reason, the option was to use specimens with dimensions of 10 mm × 2 mm × 2 mm in this study.[9] The use of smaller test specimens has no influence on the flexural strength results and decreases the amount of time and material used to perform the test, as well as being closer to clinical reality.[9,15]
The light activation methods tested in the present study affected the FS. For specimens stored in water, the conventional and pulse delay groups presented higher FS values which were statistically different (P < 0.05) from the soft start group. The clinical performance of BisGMA-based materials depends, to a great extent, on their mechanical properties. These characteristics are determined by the degree of conversion of the material.[16,17] The degree of conversion in light-activated materials is related to the energy density delivered by the light unit (expressed in J/cm2),[18] considering energy density as a product of power density (expressed in mW/cm2) through time of exposure (in seconds).[19] In this study the soft start group presented the lowest energy density (21 J/cm2) when compared with the conventional and pulse delay groups (24 J/cm2). The lowest conversion of material in the soft star group might explain the worse flexural strength. This is in accordance with the findings of the study of Asmussen and Peutzfeldt (2001),[6] suggesting that different polymerization methods induce the formation of structurally different polymers.
In this study, all the groups immersed in ethanol presented lower flexural strength than those immersed in water. Ethanol causes softening of the resin composite surface by removing the unreacted monomers, oligomers and linear polymers from the structure of the polymer.[6] When ethanol penetrates the polymeric network it causes an expansion of the structure, allowing the release of unreacted monomers and causing the breakup of the linear chains of the polymer.[15] This expansion is facilitated when the cross-link density is low, since the solvent can break the secondary links of the structure, but not the cross-links.[20] The pulse mode obtained the lowest results when specimens were stored in ethanol, when compared with conventional and gradual modes. Different irradiation procedures will lead to different structures in the resulting polymer, even though the degree of conversion of double bonds is the same.[20] At a pre-cure stage many more growth centers are formed, resulting in the fact that a larger part of the polymer structure will be linear before final polymerization.[6] The longer the time of delay before the final polymerization, the greater the trend to form a more linear polymer will be, diminishing the cross-link density, which could explain the results of polymerization with the pulse mode when specimens were stored in 100% ethanol.
Physical properties of resin composite are dependent on the polymer structures that are formed. In this light, different polymerization modes and immersion media can affect the physical properties (flexural strength) of a composite resin. Ethanol immersion resulted in the lowest flexural strength values for the composite resin evaluated. The conventional and pulse delay methods achieved the highest flexural strength for samples immersed in water while the conventional and soft start methods resulted in the highest FS for those immersed in ethanol.
Footnotes
Source of Support: This in vitro study was partially supported by Foundation of Support to Research of the State of Minas Gerais (FAPEMIG).
Conflict of Interest: NIL
REFERENCES
- 1.Smicrohardness and polymerization. Oper Dent. 2007;32:571–8. doi: 10.2341/06-163. [DOI] [PubMed] [Google Scholar]
- 2.Calheiros FC, Kawano Y, Stansbury JW, Braga RR. Influence of radiant exposure on contraction stress, degree of conversion and mechanical properties of resin composites. Dent Mater. 2006;22:799–803. doi: 10.1016/j.dental.2005.11.008. [DOI] [PubMed] [Google Scholar]
- 3.Friedl KH, Schmalz G, Hiller KA, Märkl A. Marginal adaption of Class V restorations with and without “softstart-polymerization”. Oper Dent. 2000;25:26–32. [PubMed] [Google Scholar]
- 4.Price RB, Dérand T, Loney RW, Andreou P. Effect of light source and specimen thickness on the surface hardness of resin composite. Am J Dent. 2002;15:47–53. [PubMed] [Google Scholar]
- 5.Yap AU, Soh MS, Siow KS. Post-gel shrinkage with pulse activation and soft-start polymerization. Oper Dent. 2002;27:81–7. [PubMed] [Google Scholar]
- 6.Asmussen E, Peutzfeldt A. Influence of pulse-delay curing on softening of polymer structures. J Dent Res. 2001;80:1570–3. doi: 10.1177/00220345010800061801. [DOI] [PubMed] [Google Scholar]
- 7.Aguiar FH, Braceiro AT, Ambrosano GM, Lovadino JR. Hardness and diametral tensile strength of a hybrid composite resin polymerized with different modes and immersed in ethanol or distilled water media. Dent Mater. 2005;21:1098–103. doi: 10.1016/j.dental.2004.11.010. [DOI] [PubMed] [Google Scholar]
- 8.Hegde MN, Hegde P, Malhan B. Evaluation of depth of cure and knoop hardness in a dental composite, photo-activated using different methods. J Conserv Dent. 2008;11:76–81. doi: 10.4103/0972-0707.44055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yap AU, Teoh SH. Comparison of flexural properties of composite restoratives using the ISO and mini-flexural tests. J Oral Rehabil. 2003;30:171–7. doi: 10.1046/j.1365-2842.2003.01004.x. [DOI] [PubMed] [Google Scholar]
- 10.Benetti AR, Asmussen E, Munksgaard EC, Dewaele M, Peutzfeldt A, Leloup G, et al. Softening and elution of monomers in ethanol. Dent Mater. 2009;25:1007–13. doi: 10.1016/j.dental.2009.01.104. [DOI] [PubMed] [Google Scholar]
- 11.Krithikadatta J. Research methodology in Dentistry: Part I - The essentials and relevance of research. J Conserv Dent. 2012;15:5–11. doi: 10.4103/0972-0707.92598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Peumans M, Kanumilli P, De Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dent Mater. 2005;21:864–81. doi: 10.1016/j.dental.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 13.Reza F, Lim SP. Effects of curing mode of resin cements on the bond strength of a titanium post: An intraradicular study. J Conserv Dent. 2012;15:123–6. doi: 10.4103/0972-0707.94576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.ISO 4049 dentistry-polymer-based filling restorative and luting materials. 3rd ed. Geneva: International Organization for Geneve/International Organization for Standardization; 2000. ISO-Standards; pp. 7–27. [Google Scholar]
- 15.Ribeiro JC, Gomes PN, Moysés MR, Dias SC, Pereira LJ, Ribeiro JG. Shear strength evaluation of composite-composite resin associations. J Dent. 2008;36:326–30. doi: 10.1016/j.jdent.2008.01.015. [DOI] [PubMed] [Google Scholar]
- 16.Sharma S, Padda BK, Choudhary V. Comparative evaluation of residual monomer content and polymerization shrinkage of a packable composite and an ormocer. J Conserv Dent. 2012;15:161–5. doi: 10.4103/0972-0707.94592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lovell LG, Newman SM, Donaldson MM, Bowman CN. The effect of light intensity on double bond conversion and flexural strength of a model, unfilled dental resin. Dent Mater. 2003;19:458–65. doi: 10.1016/s0109-5641(02)00090-8. [DOI] [PubMed] [Google Scholar]
- 18.Sakaguchi RL, Berge HX. Reduced light energy density decreases post-gel contraction while maintaining degree of conversion in composites. J Dent. 1998;26:695–700. doi: 10.1016/s0300-5712(97)00048-1. [DOI] [PubMed] [Google Scholar]
- 19.Halvorson RH, Erickson RL, Davidson CL. Energy dependent polymerization of resin-based composite. Dent Mater. 2002;18:463–9. doi: 10.1016/s0109-5641(01)00069-0. [DOI] [PubMed] [Google Scholar]
- 20.Soh MS, Yap AU. Influence of curing modes on crosslink density in polymer structures. J Dent. 2004;32:321–6. doi: 10.1016/j.jdent.2004.01.012. [DOI] [PubMed] [Google Scholar]