

Abstract
Background:
The newest variation of i-gel is its pediatric version. This novel supraglottic airway device has the added advantage of a drain tube. In this study, we compared the effectiveness of size 2.5 i-gel with size 2.5 ProSeal LMA.
Aims:
This study was designed to investigate the usefulness of the size 2.5 i-gel compared with the ProSeal laryngeal mask airway (PLMA) of the same size in anesthetized, paralyzed children.
Materials and Methods:
Sixty ASA grade I – II patients undergoing elective surgery were included in this prospective study and were randomly assigned to the i-gel and PLMA groups (30 patients in each group). A size 2.5 supraglottic airway was inserted according to the assigned group. We assessed the ease of insertion, hemodynamic data, oropharyngeal sealing pressure, and postoperative complications.
Results:
There were no differences in the demographic and hemodynamic data, success rates for the first attempt of insertion, or postoperative airway morbidity among the two groups. The airway leak pressure of the i-gel group (27.12 ± 1.69 cm H2O) was significantly higher than that of the PLMA group (22.75 ± 1.46 cm H2O).
Conclusion:
Hemodynamic parameters, ease of insertion and postoperative complications were comparable between the i-gel and PLMA, but the nairway sealing pressure was significantly higher in the i-gel group.
Keywords: I-gel, Pediatric patients, ProSeal laryngeal mask airway
Introduction
The i-gel (Intersurgical Inc., Berkshire, Wokingham, UK)[1] is a novel, single–use, supraglottic airway device, without an inflatable cuff. It is composed of a soft, gel-like, transparent, thermoplastic elastomer. It is designed to achieve a mirrored impression of the pharyngeal and laryngeal structures and to provide a perilaryngeal seal without cuff inflation.
It has been used in adult practice and found comparable to the laryngeal mask airway (LMA).[2–4] The recent variations of i-gel are its pediatric versions. It is available in four different sizes: 1, 1.5, 2, and 2.5, depending on the body weight.[1] Pediatric ProSeal LMAs (Laryngeal Mask Company Ltd., Singapore.) are also relatively new supraglottic airway devices in anesthesia practice. Both these supraglottic devices incorporate a gastric channel,’ which can be used for gastric decompression.
In this study, we compared size 2.5 i-gel with ProSeal LMA of the same size in anesthetised, paralyzed children, undergoing elective surgery. The primary outcome measure was oropharyngeal seal pressure (OSP). We also compared the ease of insertion, hemodynamic effects, ease of insertion of gastric tube, and postoperative airway morbidity, including blood staining, sore throat, and hoarse cry.
Materials and Methods
After obtaining approval from the Hospital Ethics Committee, 60 patients were studied. A randomized prospective study was planned to compare size 2.5 i-gel with ProSeal LMA (PLMA) of the same size.
The children included in the study were 5-10 years of age, ASA physical status I-II, they weighed 20-30 kg, and were posted for elective surgeries of less than one hour duration in the supine position, including lower abdominal, inguinal, and orthopedic procedures. The following were excluded from the study: (i) Patients with upper respiratory tract symptoms, (ii) those with risk of gastroesophageal regurgitation, and (iii) those with airway related conditions such a trismus, limited mouth opening, trauma, or mass. Sixty patients were equally randomized to any of the two groups (i-gel and PLMA) of 30 each, for airway management, using a computer-generated randomization program.
Written informed consent was taken from the parents prior to intervention and a standardized protocol for anesthesia was maintained for all cases. All the children were kept nil per mouth, as per the standard guidelines. They were premedicated with 0.3 mg. kg-1 of midazolam syrup, one hour prior to induction of anesthesia. Induction of anesthesia included sevoflurane in oxygen with standard monitors placed. Anesthesia was maintained with 1-2 vol% sevoflurane and 60% nitrous oxide in oxygen.
Once an adequate depth of anesthesia was achieved, the supraglottic device was inserted by the standard technique recommended by the manufacturer. We considered easy up-and-down movements of the lower jaw, no reaction to pressure applied to both angles of the mandible, and end-tidal sevoflurane concentration (EtSev) of 2.5 vol%, to indicate the adequate depth of anesthesia, for insertion of the device. Each device was inserted by an experienced anesthesiologist who had performed at least 75, size 2.5 PLMA, and 20, size 2.5 i-gel placements.
The ease of insertion was graded as very easy, easy, or difficult by the attending anesthesiologist. The device was inserted in the ‘sniffing’ position. The following maneuvres were included, (i) chin lift, (ii) jaw thrust, (iii) head extension, and (iv) neck flexion. If the device could be inserted without any manipulation, it was graded as ‘very easy’. If there was only one manipulation required, it was called ‘easy,’ and any difficulty more than that was graded as ‘difficult’. The number of attempts was noted, and it was considered a failure if the insertion was not successful in three attempts. The patient was then excluded from the study, and either a different size of the same device was inserted or the child was intubated with an endotracheal tube.
The device was fixed from maxilla to maxilla, and the cuff was inflated in the PLMA group using a cuff pressure monitor (Mallinckrodt Medical Gmbh, Hennef, Germany) to achieve a pressure of 60 cm H2O. This pressure was maintained throughout the surgery by continuous cuff pressure monitoring. A lubricated gastric tube was passed through the gastric channel. The device was connected to a closed circle breathing system (Fabius® plus anesthesia work station, Draeger, Germany) and an effective airway was defined by a square wave capnograph trace, normal chest movements, stable oxygen saturation (SpO2), not less than 95%, and bilateral auscultation of the chest.
Any coughing, breath holding, or laryngospasm were noted. Non-invasive systolic blood pressure (SBP), heart rate (HR), and oxygen saturation (SpO2) were recorded just before and one and five minutes after insertion. A 20% increase or decrease in SBP and HR between, before, and after insertion was considered clinically significant. The ease of insertion was graded by the attending anesthesiologist, but the rest of the data were recorded by an independent observer who was blinded to the study.
The oropharyngeal sealing pressure (OSP) was measured by closing the expiratory valve of the circle system at a fixed gas flow of 3 L. min-1, observing the airway pressure at which equilibrium was reached. At this point, gas leakage was heard at the mouth, at the epigastrium (epigastric auscultation), or coming out of the drainage tube. The Manometric stability test was supposed to be the most reliable test.
Statistical analysis
Statistical analysis was done using the SPSS software version 17.0;(SPSS Inc. Chicago, USA). Sample size was based on a crossover pilot study of 10 patients, and was selected to detect a projected difference of 30% between the groups for airway sealing pressure, for a type 1 error 0.05 and a power of 0.8. The demographic data (age, weight, and height) and complications were analyzed using the Chi-square test. The OSP and hemodynamic data were compared using the unpaired t-test. The Fisher's exact test was used to analyze the insertion characteristics and insertion attempts of the gastric tube. Unless otherwise stated, data are presented as mean (SD). A ‘P value’ of <0.05 was considered statistically significant.
Results
There was no significant difference in demographic data in the two groups [Table 1]. There were no failures in insertion of the airway in any group. The number of attempts of insertion was comparable, as shown in Table 2. Ease of insertion was more in the i-gel group (no ‘difficult’ insertion) compared to the PLMA group (three ‘difficult’ insertions) [Table 2]. The OSP was 27.12 ± 1.69 and 22.75 ± 1.46 cm H2O for the i-gel and PLMA groups, respectively, which was statistically significant (P < 0.0001).
Table 1.
Patient characteristics; data are mean (range) for age, weight, and height
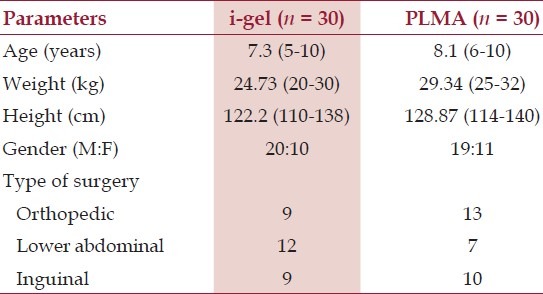
Table 2.
Comparison between i-gel and ProSeal LMA; data are mean (SD)
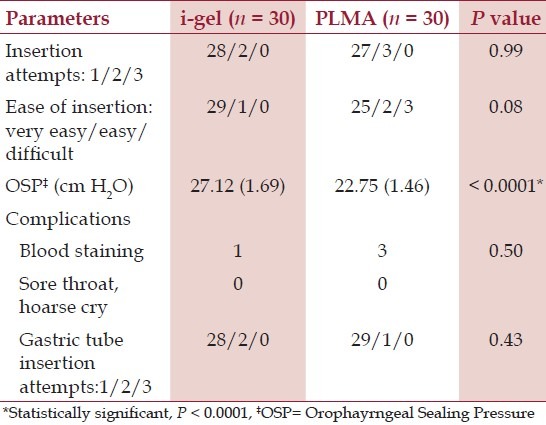
Blood staining was observed in three cases in the PLMA groups and in one case in the i-gel group. There was no incidence of sore throat or hoarse cry in either of the groups.
A gastric tube was easily passed through all PLMAs (14 Fr) and i-gel (12 Fr), [Table 2].
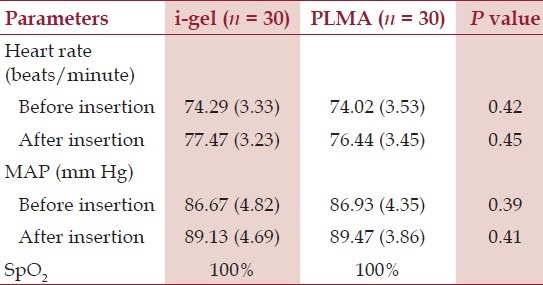
The mean arterial pressure (MAP), heart rate (HR), and SpO2 were comparable in all patients. There was neither desaturation nor any significant change in MAP or HR before and after insertion of the airway in any case, as shown in Table 3. There was no laryngospasm in any patient.
Table 3.
Hemodynamic parameters, data are mean (SD)
Discussion
The i-gel is a new single-use, noninflatable supraglottic airway for use in anesthesia during spontaneous or intermittent positive pressure ventilation.[5] The i-gel airway is an anatomically designed mask made of a gel-like thermoplastic elastomer, with a soft durometer and a gel-like feel.[6] The pediatric i-gel is a new, smaller model of the well-known i-gel used in adult patients. It has a channel for gastric catheter placement, except for size 1.[1] The soft, noninflatable cuff fits snugly into the perilaryngeal framework, mirroring the shape of the epiglottis, aryepiglottic folds, piriform fossae, perithyroid, peri-cricoid, posterior cartilages, and spaces. Therefore, each structure receives an impression fit, thus supporting the seal by enveloping the laryngeal inlet.[7] The seal created is sufficient for both spontaneous breathing as well as for paralyzed patients. Studies in adults have been promising, showing an easy insertion, high airway leak pressures, and low complication rates, with few postoperative complaints.[8–11]
In this study, we found that insertion of the i-gel was successful on the first attempt in 29 of the 30 patients and was comparable to 27 of 30 in the PLMA group. A global study, involving 50 children undergoing ventilation using the i-gel pediatric device, was carried out over two months. In that study the success rate for inserting the device was 80% on the first attempt and 100% after two attempts.[12,13] Other studies of using the pediatric i-gel[14] and LMAs[15,16] have shown similar results. The ease of insertion was graded as ‘easy’ or ‘very easy’ in all cases in the i-gel group and 90% (27 of 30) in the PLMA groups. This higher number of difficult insertions in the PLMA group may be explained by the relative anatomy of the pediatric oro-hypopharynx and the bowl of the PLMA. The larger bowl of the PLMA is more difficult to insert in the mouth and is more likely to fold over. For the most part, a relatively large tongue, a floppy epiglottis, a cephalad and more anterior larynx, and a frequent presence of tonsillar hypertrophy may disturb PLMA insertion in pediatric patients.[17] However, the i-gel is easier to insert because of a non-inflatable cuff and smaller bowl.[1]
We found that the oropharyngeal sealing pressure of the i-gel was significantly higher than that of PLMA. A similar result in OSP was observed by Goyal et al.[18] They found that the OSP in size 2 i-gel (26 ± 2.6 cm H2O) was significantly higher than that in size 2 PLMA (23 ± 1.2 cm H2O). Shin et al.[19] found no difference in OSP between i-gel and PLMA, in adult patients. On the contrary, Singh et al.[4] found that the OSP of PLMA was higher than that of i-gel (29.60 vs. 25.27 cm H2O). Schmidbauer et al.[20] also found that the OSP of PLMA was higher than that of i-gel. Higher OSP in PLMA could be explained by the presence of a dorsal cuff, which was found in PLMA size 3 and above.[21] In our study, higher sealing pressure in i-gel might be due to the lack of a dorsal cuff in size 2.5 PLMA. On the other hand, the sealing pressure quality was the same in all sizes of i-gel, because of its non-inflatable cuff. This observation was further substantiated by Beylacq et al.[14] (25 cm H2O) and Bopp et al. (25.1 ± 4.7 cm H2O).[11]
The incidence of complications (airway trauma and sore throat) has been very low in all cases, except for blood staining in a few children in the PLMA group, which is neither clinically important nor statistically significant. Other studies have also reported a similar incidence. [14,15] Although i-gel inserts less pressure on the perilaryngeal tissue because of its non-inflatable cuff, the incidence of sore throat is comparable in the two groups. This observation in our study is supported by the study of Seet et al.[22] where they stated that a sore throat could be minimal even with supraglottic devices with an inflatable cuff, if the intracuff pressure remained less than 60 cm H2O.
Conclusion
From our study we conclude that size 2.5 i-gel is comparable to PLMA of the same size, in terms of hemodynamic parameters, ease of insertion, and postoperative complications. The oropharyngeal sealing pressure is the only parameter that is significantly higher in the i-gel group. Size 2.5 i-gel is equally safe, efficient, and cost-effective in children, compared to other prototypical pediatric supraglottic airway devices. Therefore, i-gel must be more frequently used in children in both elective surgeries and in procedures requiring anesthesia outside the Operating Room.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Userguides/i-gel_users Guide_English.pdf. 2010. [Accessed January 10, 2012]. at http://www.i-gel.com/
- 2.Uppal V, Fletcher G, Kinsella J. Comparison of the i-gel with the cuffed tracheal tube during pressure-controlled ventilation. Br J Anaesth. 2009;102:264–8. doi: 10.1093/bja/aen366. [DOI] [PubMed] [Google Scholar]
- 3.Francksen H, Renner J, Hanss R, Scholz J, Doerges V, Bein B. A comparison of the i-gel with the LMA Unique in non-paralysed anaesthetised adult patients. Anaesthesia. 2009;64:1118–24. doi: 10.1111/j.1365-2044.2009.06017.x. [DOI] [PubMed] [Google Scholar]
- 4.Singh I, Gupta M, Tandon M. Comparison of clinical performance of i-gel with LMA Proseal in Elective surgeries. Indian J Anesth. 2009;53:302–5. [PMC free article] [PubMed] [Google Scholar]
- 5.Gabbot DA, Beringer R. The iGEL supraglottic airway: A potential role for resuscitation? Resuscitation. 2007;73:161–2. doi: 10.1016/j.resuscitation.2006.10.026. [DOI] [PubMed] [Google Scholar]
- 6.Sharma S, Scott S, Rogers R, Popat M. The I-gel™ airway for ventilation and rescue intubation. Anaesthesia. 2007;62:419–20. doi: 10.1111/j.1365-2044.2007.05045.x. [DOI] [PubMed] [Google Scholar]
- 7.Levitan RM, Kinkle WC. Initial anatomic investigations of the i-gel airway: A novel supraglottic airway without inflatable cuff. Anaesthesia. 2005;60:1022–6. doi: 10.1111/j.1365-2044.2005.04258.x. [DOI] [PubMed] [Google Scholar]
- 8.Jackson KM, Cook TM. Evaluation of four airway training manikins as patient simulators for the insertion of eight types of supraglottic airway devices. Anaesthesia. 2007;62:388–93. doi: 10.1111/j.1365-2044.2007.04983.x. [DOI] [PubMed] [Google Scholar]
- 9.Keijzer C, Buitelaar DR, Efthymiou KM, Srámek M, ten Cate J, Ronday M, et al. A comparison of postoperative throat and neck complaints after the use of the i-gel and the La Premiere disposable laryngeal mask: A double-blinded, randomized, controlled trial. Anesth Analg. 2009;109:1092–5. doi: 10.1213/ANE.0b013e3181b6496a. [DOI] [PubMed] [Google Scholar]
- 10.Richez B, Saltel L, Banchereau F, Torrielli R, Cros AM. A new single use supraglottic airway device with a noninflatable cuff and an esophageal vent: An observational study of the i-gel. Anesth Analg. 2008;106:1137–9. doi: 10.1213/ane.0b013e318164f062. [DOI] [PubMed] [Google Scholar]
- 11.Theiler LG, Kleine-Brueggeney M, Kaiser D, Urwyler N, Luyet C, Vogt A, et al. Crossover comparison of the laryngeal mask supreme and the i-gel in simulated difficult airway scenario in anesthetized patients. Anesthesiology. 2009;111:55–62. doi: 10.1097/ALN.0b013e3181a4c6b9. [DOI] [PubMed] [Google Scholar]
- 12.Bopp C, Chauvin C, Schwaab C, Mayer J, Marcoux L, Diemunsch P. L’I-gel en chirurgie pediatrique: serie initiale. 51eme Congres National d’anesthesie et de Reanimation (SFAR) Paris, 23-26 september 2009. Ann Fr Anesth Reanim. 2009:28. [Google Scholar]
- 13.Bopp C, Carrenard G, Chauvin C, Schwaab C, Diemunsch P. The I-gel in paediatric surgery: Initial series. New Orleans, USA: American Society of Anesthesiologists (ASA) Annual Meeting; 2009. Oct 17–21, p. A147. [Google Scholar]
- 14.Beylacq L, Bordes M, Semjen F, Cros AM. The i-gel, a single use supraglottic airway device with a non-inflatable cuff and an esophageal vent: An observational study in children. Acta Anaesthesiol Scand. 2009;53:376–9. doi: 10.1111/j.1399-6576.2008.01869.x. [DOI] [PubMed] [Google Scholar]
- 15.Karippacheril JG, Varghese E. Crossover comparison of airway sealing pressures of 1.5 and 2 size LMA-ProSeal™ and LMAClassic™ in children, measured with the manometric stability test. Paediatr Anaesth. 2011;21:668–72. doi: 10.1111/j.1460-9592.2011.03554.x. [DOI] [PubMed] [Google Scholar]
- 16.Shimbori H, Ono K, Miwa T, Morimura N, Noguchi M, Hiroki K. Comparison of the LMA-ProSeal and LMA-Classic in children. Br J Anaesth. 2004;93:528–31. doi: 10.1093/bja/aeh238. [DOI] [PubMed] [Google Scholar]
- 17.Comparison of Two Insertion Techniques of Proseal Laryngeal Mask airway by unskilled personnel in children. [Accessed 2010 January 10, 2012]. at http: //www.clinicaltrials.gov/ct2/show/NCT01191619 .
- 18.Goyal R, Shukla RN, Kumar G. Comparison of size 2 i-gel supraglottic airway with LMAProSeal™ and LMA-Classic™ in spontaneously breathing children undergoing elective surgery. [Accesed 2012 January 10, 2012]. at http://www.onlinelibrary.wiley.com/doi/10.1111/j.1460-9592.2011.03757.x . [DOI] [PubMed]
- 19.Shin WJ, Cheong YS, Yang HS, Nishiyama T. The supraglottic airway I-gel in comparison with ProSeal laryngeal mask airway and classic laryngeal mask airway in anaesthetized patients. Eur J Anaesthesiol. 2010;27:598–601. doi: 10.1097/EJA.0b013e3283340a81. [DOI] [PubMed] [Google Scholar]
- 20.Schmidbauer W, Bercker S, Volk T, Bogusch G, Mager G, Kerner T. Oesophageal seal of the novel supralaryngeal airway device I-Gel™ in comparison with the laryngeal mask airway Classic™ and ProSeal™ using a cadaver model. Br J Anaesth. 2009;102:135–9. doi: 10.1093/bja/aen319. [DOI] [PubMed] [Google Scholar]
- 21.LMA PRO-SEAL® Instruction Manual/lma_pro-seal_book_issue_3_aug_2009.pdf. 2009. [Accessed 2011 January 22, 2011]. at http://www.intaventdirect.co.uk .
- 22.Seet E, Yousaf F, Gupta S, Subramanyam R, Wong DT, Chung F. Use of manometry for laryngeal mask airway reduces postoperative pharyngolaryngeal adverse events : A prospective, randomized trial. Anesthesiology. 2010;112:652–7. doi: 10.1097/ALN.0b013e3181cf4346. [DOI] [PubMed] [Google Scholar]