

Abstract
Background:
In this study, we aimed to assess the association between air pollution and cerebrovascular complications in Tehran, one of the most air-polluted cities in the world, among different subgroups of patients with stroke in 2004.
Methods:
In this ecologic study, we calculated the daily average levels of different air pollutants including CO, NOX, SO2, O3, and PM10 and also humidity and temperature on the day of stroke and 48 hours prior to stroke in 1 491 patients admitted with the diagnosis of stroke in eight referral hospitals in different areas of Tehran. Then, we evaluated the association between the rate of stroke admissions and the level of the selected pollutants, humidity, and temperature on the day of stroke and 48 hours prior to stroke among different subgroups of patients.
Results:
There was no significant association between the same-day level of the pollutants and the rate of stroke admissions, but an association was seen for their level 48 hours before stroke. These associations differed among different subgroups of age, sex, history of underlying diseases, and type of stroke. Same-day temperature had a reverse association in patients with hemorrhagic stroke and in patients without a history of heart disease or previous stroke. A direct significant association was seen for humidity level 48 hours before stroke in patients with a history of heart disease.
Conclusions:
It is inferred that air pollution has a direct association with the incidence of stroke and these association differs among different subgroups of patients. The results of this study are not time-dependant and can be generalized to different times and regions. Moreover, these results may be useful for environmental health policy makers.
Keywords: Air pollution, cerebrovascular complications, CO, humidity, NOx, O3, PM10, SO2, temperature, Tehran
INTRODUCTION
Air pollution is a health problem which results in several medical conditions in human beings. Many of these disorders, especially respiratory diseases, are fully recognized.[1,2] Currently, the potential hazards of air pollution dramatically influence the human population. Old persons, children, patients with cardiovascular problems, pregnant women, and fetuses are more susceptible to these pollutants.[3] These side effects include respiratory diseases and exacerbations of cardiopulmonary diseases.[4]
Tehran is the capital of Iran, a metropolitan area with more than 12 million inhabitants, more than 3 million cars and many factories, which all lead the city to be one of the most air-polluted cities in the world.[5] In a study conducted in 2004 in Tehran, the air quality over 262 days was worse than the standard levels specified by the U.S. Environment Protection Agency (i.e., AQI = 100). Comparing with past years, the quality of Tehran's air in 2004 was still threatening to people, especially vulnerable populations.[6] Previous studies have indicated that there is a significant association between air pollution and a high rate of cardiovascular disease, including deep vein thrombosis and other atherosclerotic disorders such as myocardial infarction.[7–9] A study conducted in Seoul, South Korea, between 1995 and 1998 investigated the delayed effect of air pollution on mortality due to stroke, and the results showed that O3 and PM10 had the highest relationship with mortality due to stroke on the same day. Meanwhile, CO, SO2, and NO2 densities at 48 hours before indicated a higher risk for mortality due to stroke.[10] A study conducted in Isfahan, the second most air-polluted city in Iran, showed that there is an association between air pollution and the development of atherosclerosis in its first stages in the early life and emphasized the importance of considering the harmful effects of air pollution on children.[11] Another study conducted in Isfahan suggested an independent association between air pollution and systemic inflammatory and coagulation responses by studying a genetic polymorphism in a tissue factor in atherosclerotic lesions.[12]
Although many studies have discussed the side effects of air pollution on human health, there is not yet a consensus on the vascular side effects of air pollution.[13,14] In order to provide more comprehensive data on the effects of air pollution on the health, we investigated the association between air pollution in Tehran and the number of stroke admissions in the main referral hospitals of Tehran. We hypothesized that the rate of stroke would be higher on more polluted days.
METHODS
This was a cross-sectional analytical study on the ecological level. The sample size was 1 491 patients primarily diagnosed as stroke in 2004. We assessed all patient files which satisfied inclusion criteria. The patients were admitted in eight referral hospitals, located in different areas of Tehran. These are the main referral hospitals in Tehran which figured out that more than 90% of patients with stroke would be admitted by them. Complementary data including age, sex, risk, and modifying factors on stroke including hyperlipidemia, hypertension, cardiovascular disease, diabetes, smoking status, and type of stroke were obtained from the patient's file. In order to cover stroke in the younger group during analysis, the age cut-off point was defined as 40 years.
Daily information on Tehran's air pollution in 2004 was supplied from the Centre for Control of Traffic, transportation and air pollution of Tehran. The data included daily levels of CO, SO2, NOx, PM10, ozone (O3), and meteorological variables (temperature and humidity). We used the information from seven air-check stations of the eleven stations in Tehran. Then, daily average levels of pollutants were separately calculated. We used the Air Quality Index (AQI) to describe air quality which consists of six levels, which are shown in Table 1.[7] Categories of pollutant density, necessary for calculating the air quality control index, are also shown in Table 1. In this table, the average 8-hour density was used for CO and O3 and the average 24-hour density was used for SO2 and PM10. The density of PM10 was assessed by radiating beta ray, the density of CO was assessed by using a non-dispersive infrared analyzer, the densities of O3 and SO2 were assessed by using light spectrometry, and temperature and humidity were assessed by the Vaisala model mp 113y and were analyzed continuously.[15,16] Due to the lack of information on NO2, NOX was used in some stations. According to the standard table of clean air, offered by the U.S. Environmental Protection Agency, the density of NO2 and NOX was not mentioned in this classification. We analyzed the data by STATA software version 8. To evaluate the association between each pollutant and the rate of hospitalization separately, we used univariate analysis. We also used multi-variable Poisson regression in which the number of hospitalizations for each day was the dependent variable and the previously mentioned air pollutants with a P value lower than 0.2 in the univariate analysis were independent variables.[17] Type one error in all analysis including regression was considered 0.05. Poisson regression was also performed separately for each stratum of the variables of age (cut-off point: 40 years), sex, and underlying diseases (diabetes, hypertension, hypercholesterolemia, cardiovascular diseases, and smoking status). In this analysis, the adjusted relative risk (RR) was defined as the increase in the rate of hospitalization by the increased level of pollutants. The confidence interval was set at 95%. The level of significance in this study was considered to be 0.05.
Table 1.
Classes for density of pollutants in order to calculate Air Quality Control Index[8]

RESULTS
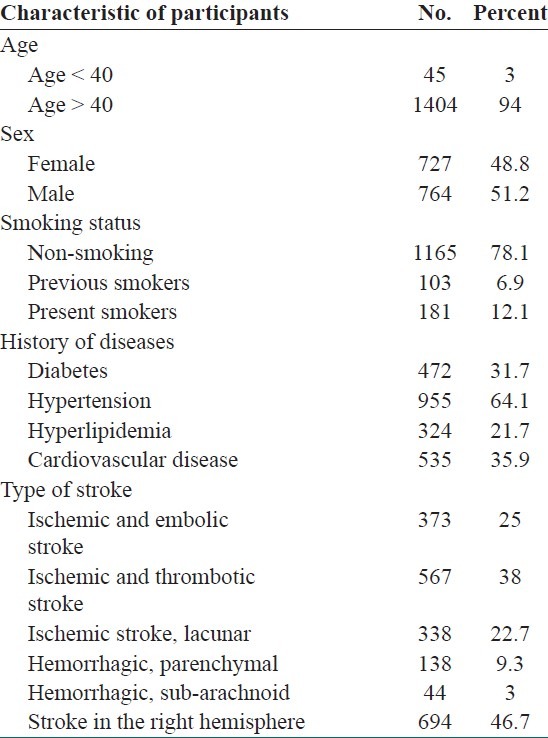
Characteristics of studied subjects and their general information are shown in Table 2.
Table 2.
Characteristics of studied subjects (n = 1491)
The statistical significance of association between the 24 hour average of air pollutants with the number of stroke admissions on the same day and 48 hours before in univariate analysis based on analysis of variance and univariate Poisson regression is shown in Table 3.
Table 3.
Statistical significance level of association of average air pollutants with number of hospital admission for stroke
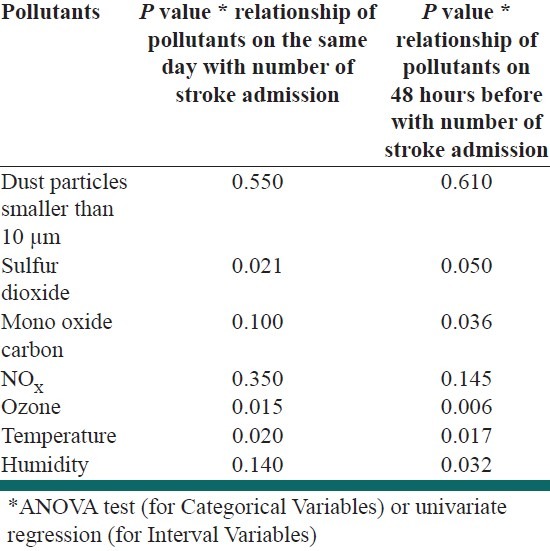
As shown in Table 3, the variables O3, CO, SO2, temperature, and humidity on the day of stroke and the variables NOX, CO, SO2, temperature, and humidity 48 hours before stroke had P values lower than 0.2 and were therefore entered into multivariate Poisson regression. In the multivariate Poisson regression, as shown in Table 4, the same-day level of the pollutants had no significant effect on the number of admitted stroke patients. As shown in Table 5, the level of NOX at 48 hours before had a significant effect on the number of hospitalizations (P = 0.02).
Table 4.
Association between the same-day level of the pollutants and stroke admission in the different variables strata through multivariate poisson regression
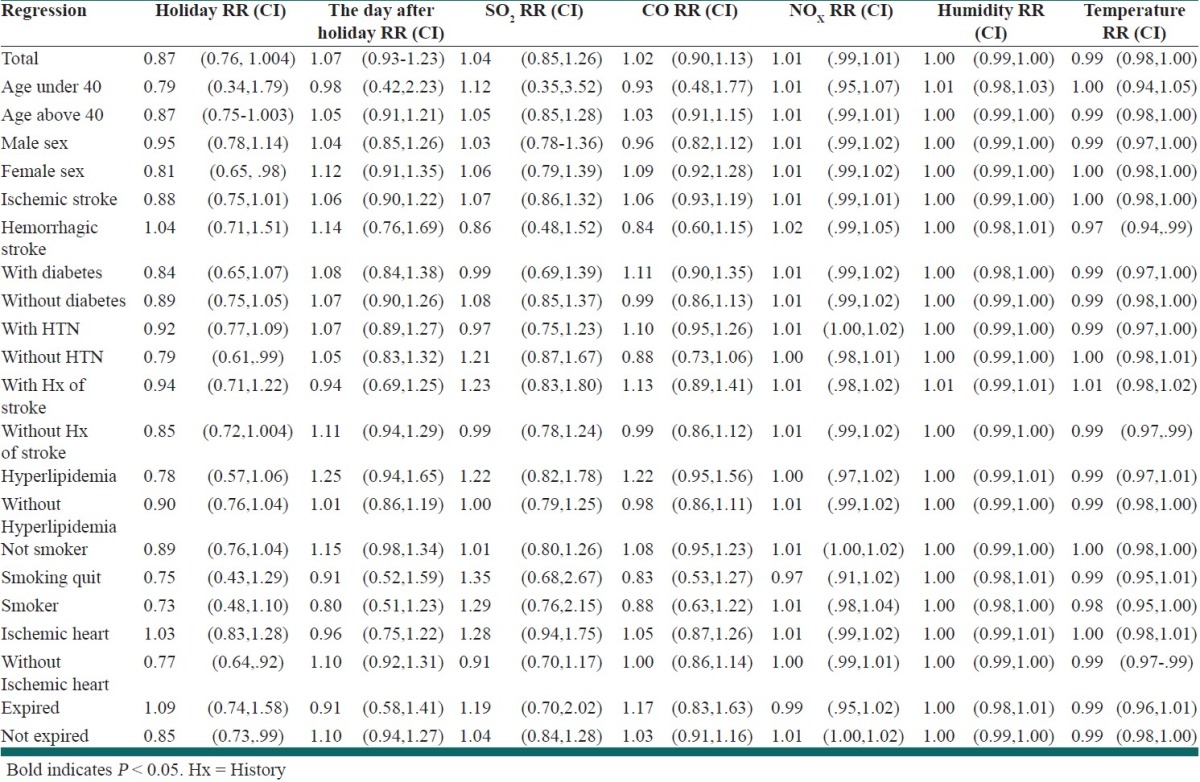
Table 5.
Association between the 48 h before stroke level of the pollutants and stroke admission in the different variables strata through multivariate poisson regression
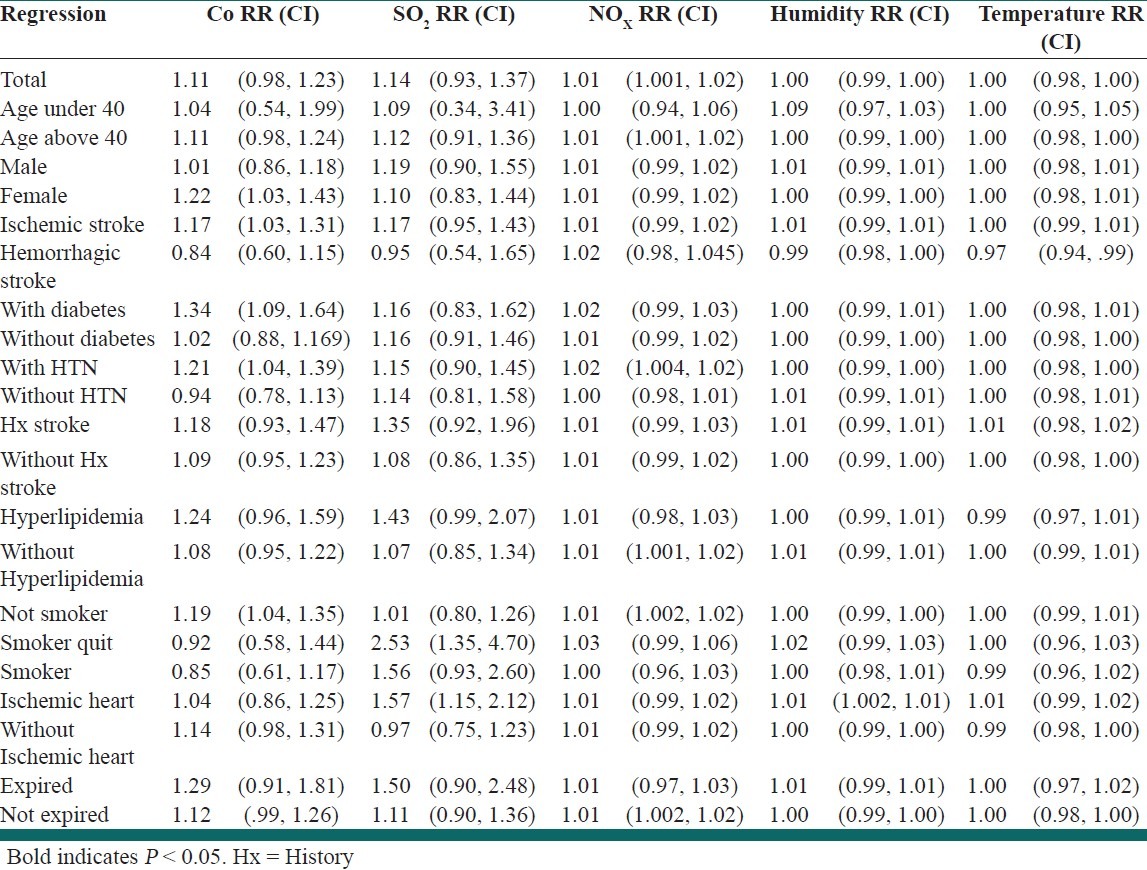
As shown in Tables 4 and 5, multivariate Poisson regression was used to assess the association of same-day and 48 hours before stroke pollutant levels in different variables strata. Same-day temperature had a significant reverse association with hemorrhagic stroke admission (P = 0.034), and in patients without a history of heart disease (P = 0.046) or previous stroke (P = 0.043). Also, temperature at 48 hours before had a significant reverse association with hemorrhagic stroke admission (P = 0.017). The humidity level 48 hours before had a direct significant association with the stroke admission of patients with the history of heart disease (P = 0.007). Same-day nitrogen oxide level had a significant direct association with the stroke admission of patients with the history of hypertension (P = 0.031). The nitrogen oxide level 48 hours before stroke had a significant direct association with stroke admission of patients aged over 40 years (P = 0.025), patients with the history of hypertension (P = 0.005), and in patients without history of hyperlipidemia (P = 0.032). The carbon monoxide (CO) level 48 hours before stroke had a significant direct association with stroke admission in female cases (P = 0.019), with ischemic stroke admission (P = 0.013), stroke admission in patients with the history of hypertension (P = 0.005), diabetics (P = 0.009), and non-smoking cases (P = 0.008). The sulfur dioxide level 48 hours before had a significant direct association with admission of patients with a history of heart disease (P = 0.004) and past smokers (P = 0.003).
DISCUSSION
Stroke is a multi-factorial disease that is influenced by several genetic and environmental factors including life style and environmental conditions.[18] The level of NOX on the same day had a significant association with the occurrence of stroke, and factors including CO, SO2, and NOX, temperature and humidity 48 hours before stroke had a significant association with stroke admission.[19] These associations were different among different subgroups of age, sex, history of underlying diseases, and type of stroke. It could be concluded that the effect of pollutants on stroke 48 hours before stroke was higher than its effect on the same day as stroke which might be due to a requirement for an incubation time of these pollutants at least 48 hours before influencing the brain. In this study, in comparison with other similar studies, more pollutants were used for studying this relationship. In a study conducted by Lokken in the U.S.A. published in 2009, upon examining 1 101 patients with proven stroke, it was shown that observing hospitalized patients and not having a control group may have resulted in an underestimation of the relationship between air pollution and stroke.[20] Therefore, it might be inferred that the true associations are stronger than the associations which were shown in this study. In a study conducted by Hu in the U.S.A. in 2008, it was determined that for people who live in polluted areas and areas without any green space, the risk of mortality is higher in cases of stroke. In our study, we found a similar result in that there was a relationship between mortality as a result of stroke with pollutants including carbon monoxide and ozone on the day of stroke and carbon dioxide 48 hours before stroke.[21] In a study that was conducted by Oudin in Sweden in 2009, upon studying 556 912 persons (contrasting our study and most previous studies), it was shown that there was no association between air pollution, especially between the NOX index and hospitalizations due to stroke.[22] In a study conducted by Wang in Australia, it was found that there was a significant association between temperature and hospitalization due to stroke and even there was association between the type of stroke with temperature,[23] similar to the results of our study. In a study conducted by Henrotin in Dordjon, France from 1994-2004, it was found that there was a positive relationship between increasing amounts of O3 and PM10 and ischemic stroke, but there was no important relationship with hemorrhagic stroke.[24] However, in our study, there was a significant relationship between ischemic stroke and carbon monoxide 48 hours before stroke and a significant relationship between hemorrhagic stroke and temperature on the same day and 48 hours before stroke in which temperature was a protective factor. The hazards of air pollution should be considered in all age groups even in young adults[25], and the impacts on elderly should be underscored. In terms of limitations, one weak point of our study was some missing information in the files. Also, it was not a study on the individual level, i.e., it was performed on the ecologic level and the results were analyzed on the group level, so there may be bias in this study. On the other hand, since Tehran is a big city and there are few stations for assessing air pollutants, it was not possible to determine accurate amounts of dangerous pollutants in persons with stroke. Also, the time of stroke was not accessible as an exact hour. In this study, potential confounding factors may have been due to risk factors which were dependent on time (time-varying), day, month, or climate conditions in which these confounding factors were considered in the multivariate analysis. Since diagnosis of stroke was performed in this study without having any information of the air pollution status by the physicians, patients, and even the research team, a considerable bias is not expected.
CONCLUSION
Based on our findings and compared to previous studies, we can infer that air pollution and temperature are effective factors in the occurrence of cerebral stroke. However, they do not have any effect on mortality from stroke. Although this study was conducted in 2004, but considering the large sample size and as the findings of this study are not time-dependant, they can be generalized to different population in different times. According to the significant relationship indicated in this study, it can be concluded that policies should be considered for decreasing air pollution and consequently decreasing stroke, complications, and the mortality rate due to stroke. This could be regarded as an effective step on behalf of the organizations responsible for a healthy environment. We suggest conducting more studies at individual level to describe the role of each pollutant in causing stroke in the future.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kliment V, Kubínová R, Kazmarová H, Kratzer K, Sisma P, Ruprich J. Five years of the system of monitoring the environmental impact on population health of the Czech Republic. Cent Eur J Public Health. 2000;8:198–205. [PubMed] [Google Scholar]
- 2.Campbell-Lendrum D, Corvalán C. Climate change and developing-country cities: Implications for environmental health and equity. J Urban Health. 2007;84:109–17. doi: 10.1007/s11524-007-9170-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Reziaee S, Nuri K, Kazemnezhad A. The effects of CO of air pollution on pregnancy. Babol J Med Sci. 2004;7:19–22. [Google Scholar]
- 4.Mohammadi H. Association between geographic factors and airpollutants in Tehran with the cardiac disorders mortality rates. Geo Res. 2005;38:47–66. [Google Scholar]
- 5.Kermani M, Naddafi K, Shariat M, Mesbah A. TSP and PM1o measures in the air around Shariatihospital of Tehran. J Health Res (TUMS) 2004;2:37–46. [Google Scholar]
- 6.Ardakani S, Esmaele A, Cheraqi M, Tayebi L, Ghasempuri M. Quality assessment of air in Tehran in 2003. J Sci Tech Ecol. 2005;4:33–6. [Google Scholar]
- 7.Ghorbani M, Yunesian M, Fotuhi A, Zeraati H, Sadeqian S, Rashidi Y. Association between air pollution exposure and the onset of acute cardiac syndrome in Tehran heart center. Iran J Epidemiol. 2007;2:53–9. [Google Scholar]
- 8.Baccarelli A, Martinelli I, Zanobetti A, Grillo P, Hou LF, Bertazzi PA, et al. Exposure to particulate air pollution and risk of deep vein thrombosis. Arch Intern Med. 2008;168:920–7. doi: 10.1001/archinte.168.9.920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tubek S, Bunio A, Szyguła R, Tubek A. Frequency of hospitalization for angina pectoris, stroke, and peripheral venous thrombosis and its relationship to elements in rainwater in OpoleVoivodship, Poland, during 2000-2002. Biol Trace Elem Res. 2010;133:243–50. doi: 10.1007/s12011-009-8434-6. [DOI] [PubMed] [Google Scholar]
- 10.Nogueira JB. Air pollution and cardiovascular disease. Rev Port Cardiol. 2009;28:715–33. [PubMed] [Google Scholar]
- 11.Poursafa P, Kelishadi R, Lahijanzadeh A, Modaresi M, Javanmard SH, Assari R, et al. The relationship of air pollution and surrogate markers of endothelial dysfunction in a population-based sample of children. BMC Public Health. 2011;11:115. doi: 10.1186/1471-2458-11-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Poursafa P, Kelishadi R, Moattar F, Rafiee L, Amin MM, Lahijanzadeh A, et al. Genetic variation in the association of air pollutants with a biomarker of vascular injury in children and adolescents in Isfahan, Iran. J Res Med Sci. 2011;16:733–40. [PMC free article] [PubMed] [Google Scholar]
- 13.Brook RD. Is air pollution a cause of cardiovascular disease? Updated review and controversies. Rev Environ Health. 2007;22:115–37. doi: 10.1515/reveh.2007.22.2.115. [DOI] [PubMed] [Google Scholar]
- 14.Bukowski J. Do pollution time-series studies contain uncontrolled or residual confounding by risk factors for acute health events? Regul Toxicol Pharmacol. 2008;51:135–40. doi: 10.1016/j.yrtph.2007.12.003. [DOI] [PubMed] [Google Scholar]
- 15.Galimanis A, Mono ML, Arnold M, Nedeltchev K, Mattle HP. Lifestyle and stroke risk:A review. Curr Opin Neurol. 2009;22:60–8. doi: 10.1097/WCO.0b013e32831fda0e. [DOI] [PubMed] [Google Scholar]
- 16.Lisabeth LD, Escobar JD, Dvonch JT, Sanchez BN, Majersik JJ, Brown DL. Ambient air pollution and risk for ischemic stroke and transient ischemic attack. Ann Neurol. 2008;64:53–9. doi: 10.1002/ana.21403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jewell NP. Statistics for Epidemiology. Seattle, Washington, United States: Amazon publication; 2003. [Google Scholar]
- 18.Villeneuve P, Chen L, Stieb D, Rowe B. Association between outdoor air pollution and emergency department visits for stroke in Edmonton, Canada. Eur J Epidemiol. 2006;21:689–700. doi: 10.1007/s10654-006-9050-9. [DOI] [PubMed] [Google Scholar]
- 19.Nabavi SM, Sadat Jalali M, Nedjat S, Ashrafi K, Salahesh A. Is air pollution a risk factor for stroke? Int J Stroke. 2012;7:100. doi: 10.1111/j.1747-4949.2011.00720.x. [DOI] [PubMed] [Google Scholar]
- 20.Lokken RP, Wellenius GA, Coull BA, Burger MR, Schlaug G, Suh HH. Air pollution and risk of stroke: Underestimation of effect due to misclassification of time of event onset. Epidemiology. 2009;20:137–42. doi: 10.1097/ede.0b013e31818ef34a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hu Z, Liebens J, Rao KR. Linking stroke mortality with air pollution, income, and greenness in northwest Florida: An ecological geographical study. Int J Health Geogr. 2008;7:20. doi: 10.1186/1476-072X-7-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oudin A, Stroh E, Stromberg U, Jakobsson K, Bjork J. Long-term exposure to air pollution and hospital admissions for ischemic stroke. A register-based case-control study using modeled NOx as exposure proxy. BMC Public Health. 2009;9:301. doi: 10.1186/1471-2458-9-301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wang XY, Barnett AG, Hu W, Tong S. Temperature variation and emergency hospital admissions for stroke in Brisbane, Australia, 1996-2005. Int J Biometeorol. 2009;53:535–41. doi: 10.1007/s00484-009-0241-4. [DOI] [PubMed] [Google Scholar]
- 24.Henrotin J, Besancenot JP, Bejot Y, Giroud M. Short- term effects of ozone air pollution on ischemic stroke occurrence. Occup Environ Med. 2007;64:439–45. doi: 10.1136/oem.2006.029306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kargarfard M, Poursafa P, Rezanejad S, Mousavinasab F. Effects of exercise in polluted air on the aerobic power, serum lactate level and cell blood count of active individuals. Int J Prev Med. 2011;2:145–50. [PMC free article] [PubMed] [Google Scholar]