

Abstract
Lipomas are capsulated benign tumours that are commonly found in all body parts. A lipoma is a well-defined mesenchymal tumour that arises from the adipose tissue. Although giant lipomas are rare in the head and neck regions, when they are located here, they are most commonly found in the subcutaneous posterior neck area. Recurrence as well as invasion is very rare after total surgical excision. In this article, we present two rare cases of giant lipomas in the posterior occipitocervical region, which is an exceptional location.
KEYWORDS: Cervical, giant, lipoma, occipital
INTRODUCTION
Lipomas are benign, encapsulated tumours of mesenchymal origin, arising from the adipose tissue. They are frequently encountered in the back, shoulder and neck regions. The clinical picture usually comprises of an asymptomatic, slow growing and painless mass.[1,2] They are mostly located subcutaneously in all parts of the head and neck regions. They are not invasive, and recurrence is very rare following enucleation surgery. Superficial, simple lipomas can grow for many years without causing any functional problems, and they rarely reach very large dimensions.[2,3] Giant lipomas in the occipital and cervical prevertebral muscle tissue are rare. The surgical excision of giant occipitocervical lipomas is necessary for aesthetic concerns, pain and limitation of neck motion, especially in the recumbent position.[4,5]
CASE REPORTS
Case 1
A 52-year-old male patient was admitted to our clinic due to swelling at the back of his head. The history revealed that the swelling had been present for 10 years; it had grown gradually from the size of a small hazelnut. During the patient's general physical examination, a large, mobile mass of 10 × 10 cm was found, localized in the left occipitocervical region. The neurological examination revealed no pathology. The laboratory values were within normal limits. The patient’ magnetic resonance imaging (MRI) revealed a mass of 10 × 10 cm in the left occipitocervical region that had adhered to the adjacent bone structure, causing a thickening of the scalp; however, there was no bone defect or destruction. There was no lesion in the intracranial distance. The patient was operated on, and the subcutaneous mass was totally excised [Figure 1]. During the pathological examination the excised soft tissue mass was classified as a lipoma. There was no recurrence in the follow-up of the patient.
Figure 1.
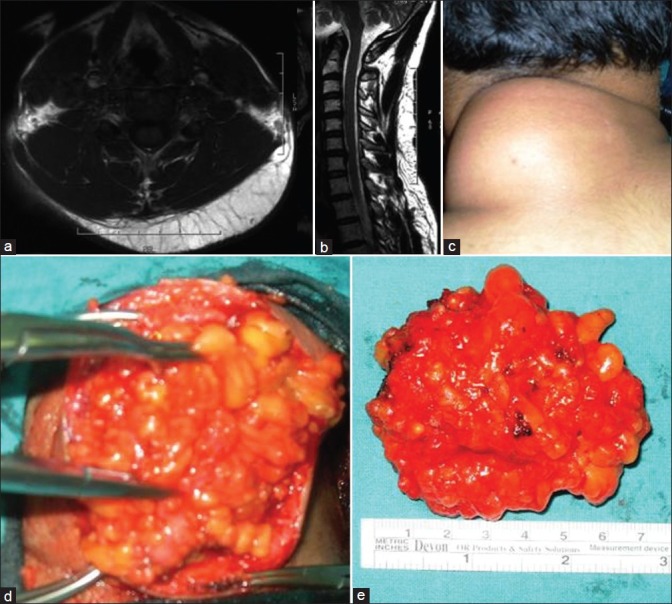
(a) Axial and (b) sagittal T2-weighted MR imaging shows the large lipoma; (c) the lipoma in the occipitocervical region; (d) the resected lipoma; (e) picture of the completely resected lipoma
Case 2
A 56-year-old male patient was admitted to our clinic due to a swelling at the back of the head. The physical examination revealed a giant, painful mass covering the entire left occipital region. His history revealed that the lesion had been growing for the past five years. The neurological examination was normal. An MRI showed a 11 × 10 cm mass, with a smooth, lobulated contour, and subcutaneous localization in the occipital region extending halfway down the neck, hyperintense on the T1-T2-weighted sequences with a thin septal contrast enhancement after contrast administration, which was adherent to the surrounding muscle tissue and bone. The mass was excised [Figure 2]. The pathological examination of the mass revealed a tumour covered with a thin, fibrous, connective tissue capsule that consisted of thin vascular structures formed by mature adipocytes of large vacuolated cytoplasm. There was no recurrence in the follow-up of the patient.
Figure 2.
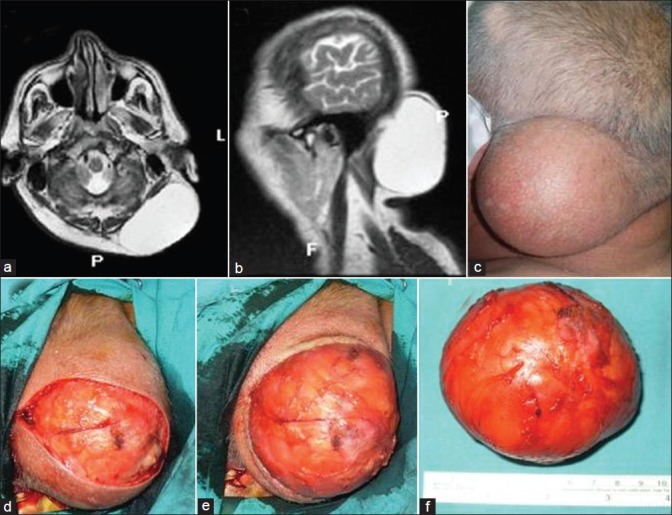
(a) Axial and (b) sagittal T2-weighted MR imaging shows the giant lipoma; (c) the lipoma in the occipital region; (d) the capsule of the lipoma after skin incision; (e) the resected lipoma peeled off from the surrounding tissue and removed together with the capsule; (f) picture of the completely resected lipoma
Surgery
After anaesthesia and intubation, the patient was placed in a prone position. Following this, the capsule of the mass was reached via an elliptical skin incision about half the size of the mass. With careful dissection of the subcutaneous tissues surrounding the capsule, the tumour was peeled off in a single piece. The skin was primarily closed. To prevent the accumulation of blood in the potential space and enhance early adhesion, hemostasis was performed carefully, and a drain was placed for one day. Both patients were discharged on the second postoperative day. The sutures were removed on the tenth day.
DISCUSSION
Lipoma is a benign tumour of mesenchymal origin that is rarely seen in the head and neck region. Only 13% of all lipomas are located in the head and neck region. Lipomas are most commonly encountered between the ages of 50 and 60. They are usually slow-growing nodules with the consistency of solid rubber.[1,2,6] Head and neck lipomas are composed of well-defined elliptical cells. They are usually adherent to the adjacent muscle tissue and skin. The capsules are strongly attached to the surrounding soft tissue and the bone.[2,4] Although the recurrence rate is not high, resection may be difficult due to the large size and adherence to the surrounding tissues. Especially in our second case, resection was difficult due to the hard capsule, which was adherent to the occipital bone.[1,4] Approximately 80% of the lipomas are under 5 cm. Some are larger than 20 cm and may weigh a few kilograms.[2,5,6] The lipomas in both of our cases were over 10 cm. Lipomas are usually asymptomatic, but they can cause pain when they are large and press on the nerves. The two patients in our study were admitted to the hospital due to pain and cosmetic concerns. Lipomas tend to locate in the trunk, shoulders, posterior neck, and axilla. Approximately 80% are in the form of a single lesion, and they are generally seen in women. On the other hand, multiple lesions are more common in young men.[1,2]
In addition to a physical examination, radiological assessment is necessary for the evaluation of the nature of the lipoma and surgical planning.[2,4] Connection with the surrounding tissues and bone can be evaluated by computed tomography (CT) and magnetic resonance imaging (MRI). In the case of suspicious, large lipomas fine needle aspiration biopsy can be performed prior to surgery.[3,5] Occipital or cervical giant lipomas are rare. Patients usually seek medical attention due to malignancy or cosmetic problems. Certain positions of the body and/or some daily physical activities may be restricted due to the size of the tumour. Lipomas that are large, painful, and cause cosmetic problems should be operated on following good preoperative planning.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Casani AP, Marchetti M, Dallan I, Cagno MC, Berretini S. Liposarcoma of the cervico-nuchal region. Otolaryngol Head Neck Surg. 2005;133:641. doi: 10.1016/j.otohns.2004.09.074. [DOI] [PubMed] [Google Scholar]
- 2.Yakubu AA, Edino ST, Mohammed AZ, Sheshe AA, Alhassan SU. Giant and complicated subcutaneous lipoma of the neck. West Afr J Med. 2008;27:44–6. [PubMed] [Google Scholar]
- 3.Derin AT, Güney K, Turhan M, Erdoğan A, Ağirdir BV. Giant cervical lipoma invading carotid artery: A case report. Kulak Burun Bogaz Ihtis Derg. 2009;19:28–31. [PubMed] [Google Scholar]
- 4.Maheshwari P, Gupta DK. A huge intramuscular lipoma of occipito cervical region - A case report. Indian J Orthop. 2006;40:125–7. [Google Scholar]
- 5.Ahuja AT, King AD, Kew J, King W, Metreweli C. Head and neck lipomas: Sonographic appearance. AJNR Am J Neuroradiol. 1998;19:505–8. [PMC free article] [PubMed] [Google Scholar]
- 6.Verma S, Varma M, Kala S, Singh R. Giant lipoma of posterior neck with bleeding decubitus ulcer: A rare entity. J Cutan Aesthet Surg. 2010;3:119–21. doi: 10.4103/0974-2077.69027. [DOI] [PMC free article] [PubMed] [Google Scholar]