

A 85-year-old woman was admitted to the Intensive Care Unit with severe hypotension following a reintervention for bleeding occurring two days after major abdominal surgery.
Medical history included diabetes mellitus under treatment and systemic hypertension; a preoperative cardiac risk assessment revealed no signs of myocardial ischemia.
Patient was mechanically ventilated and supported by inotropic agents.
Electrocardiogram showed sinus tachicardia and right bundle branch block. Physical examination revealed reduced lung vescicular murmur and phlebitis at jugular venous access without fever. Laboratory findings showed leukocitosis, increased C-reactive protein, D-dimer, troponin I (2 ng/ml) and creatine kinase level of 126 U/L.
A transthoracic echocardiography examination (TTE) showed severe right chambers dilation, tricuspid regurgitation, severe pulmonary hypertension and paradoxical septal motion (Panel A, white arrows).
Figure 1.
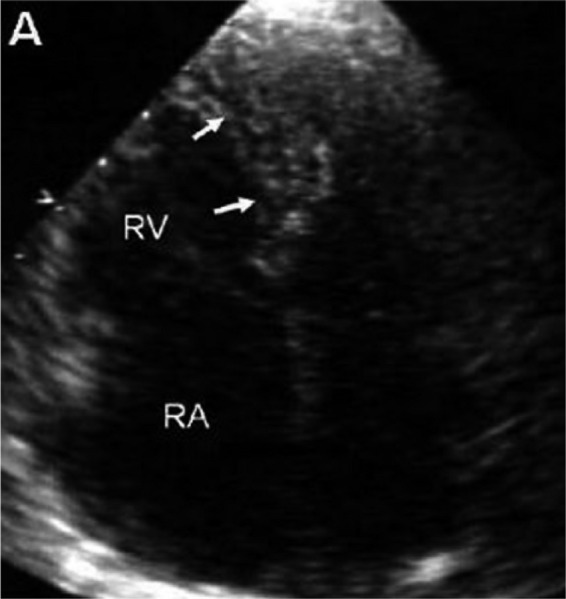
Panel A. Standard Echocardiographic Transthoracic 4-Chamber View showing severe dilation of right chambers and paradoxical septal motion (white arrows). RV = Right Ventricle; RA = Right Atrium.
Left Ventricle was hyperdynamic with an akinetic apex.
The clinical suspicion of acute pulmonary embolism was ruled out by CT-scan notwithstanding the remarkable right chambers and pulmonary artery dilation with moderate pericardial and pleural effusion (Panel B,C). The hypothesis of a Stress (Tako-Tsubo) Cardiomyopathy was not consistent with the finding of right chambers dilation.
Figure 1.

Panel B-C. CT-scan imaging of severe right chambers and pulmonary artery dilation and pericardial effusion. RV = Right Ventricle; RA = Right Atrium; LV =Left Ventricle; LA = Left Atrium; PA = Pulmonary Artery.
A new TTE was repeated, and a large left-to-right shunt was clearly detected at apical ventricular septum (Panel D, white arrows).
Figure 1.
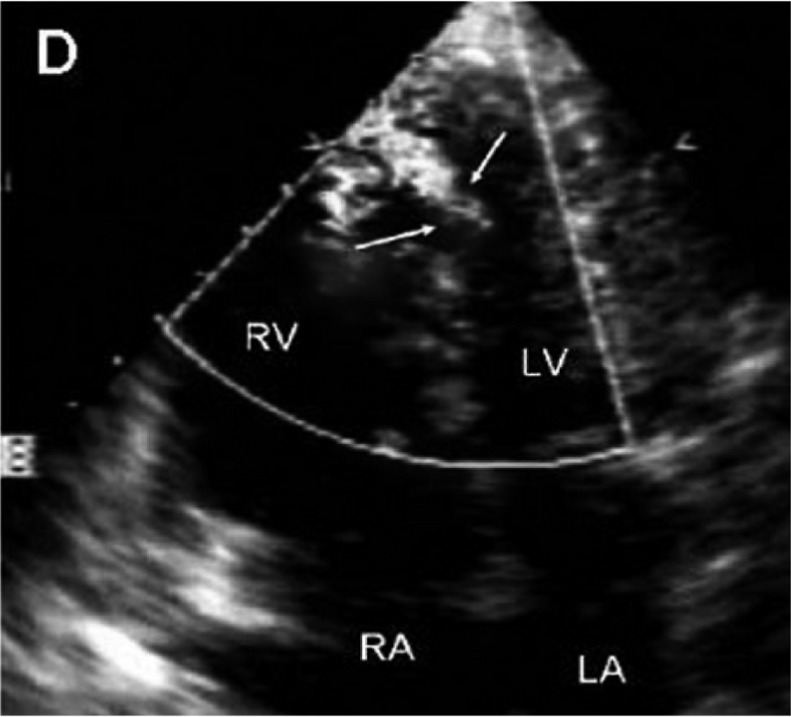
Panel D. Echocardiographic detection of a significant left-to-right shunt at apical ventricular septum (white arrows).
An unrecognized post-bleeding (Hb 6 mg/dl) small myocardial infarction (2 days after main surgery) was supposed to determine a ventricular septal defect responsible for the sudden hypotension, acute right chambers overload and unloaded hyperdynamic left ventricle.
Surgical option was excluded and the woman died the day after.
Footnotes
Source of Support Nil.
Conflict of interest None declared.
Cite as: Grimaldi A, Ammirati E, Piraino D, Vermi A.C, Arendar I, Sacco F, La Canna G, Alfieri O. Sudden hypotensive syndrome mimicking acute pulmonary embolism after major abdominal surgery. HSR Proceedings in Intensive Care and Cardiovascular Anesthesia 201