

Abstract
INTRODUCTION
The development of empyema as a result of an intra-abdominal pathology is a rare condition.
PRESENTATION OF CASE
We present a 31-year-old woman at 28 weeks’ gestation who was referred to our hospital with diagnosis of pneumonia with pleural effusion. She presented with signs of septicemia and fetal distress. A thoracic-abdominal-pelvic CT-scan showed a right pleural effusion with a retroperitoneal collection in contact with the pleural space. Due to her critical condition, immediate surgical exploration and pregnancy interruption was decided. The fetus was delivered by cesarean with satisfactory vitality. After abdominal exploration, a retrocecal appendicular abscess was evidenced and appendectomy was performed. Subsequently, the right chest was accessed through a posterolateral thoracotomy. An empyema with lung abscess and purulent fluid accessing from the retroperitoneum at the posterior pleural space was found. Due to parenchymal compromise, a right inferior lobectomy was performed. The patient had an uneventful recovery and was discharged at postoperative day 10.
DISCUSSION
A septic condition in a pregnant patient with significant thoraco-abdominal infection requires an aggressive approach, with interruption of pregnancy and urgent exploration of the chest and abdomen.
CONCLUSION
When an empyema is developed in absence of lung disease or other intrathoracic cause, intra-abdominal origin should be considered.
Keywords: Appendicitis, Empyema, Pregnant woman
1. Introduction
An empyema is the result of the accumulation of infected fluid in the pleural space. Most frequently, it occurs due to infection spread by contiguity of intrathoracic disease (pneumonia, mediastinitis, etc.). The secondary infection due to intra-abdominal pathology is less common. In the absence of lung disease or other intrathoracic focus, intra-abdominal origin should be considered.
The main objective of this work is to present a unique case of a pregnant patient who developed an empyema due to an acute appendicitis (AA), and review the pathophysiological mechanisms that explain this extremely atypical presentation of a common disease.
2. Case report
We present a 28 weeks pregnant 31-year-old woman, who was referred from another institution with diagnosis of pneumonia complicated with pleural effusion. The patient had no relevant medical or surgical history. She reported a back pain of several weeks duration which was interpreted as a urinary tract infection, receiving 3-days of empirical antibiotic treatment. Within 2 weeks, and without significant clinical improvement, she developed cough and fetid expectoration. A chest X-ray showed pleural effusion with an image of consolidation in the inferior lobe of the right lung. Due to the complexity and severity of the patient, she was referred to our medical center.
At the initial evaluation, the patient presented dyspnea, tachycardia (135 beats/min), hypotension (90/60 mmHg) and hemoglobine oxygen saturation of 85% while breathing room air. Physical examination revealed decreased breath sounds with dullness on percussion of right lung base. The abdominal evaluation was normal, without any pathological findings. Blood tests showed leukocytosis (15,320 WBC/mm3) without other significant features. Chest X-ray confirmed the right pleural effusion and a ultrasound guided thoracocentesis was performed. The fluid obtained was consistent with empyema (LDH 5000 UI/ml, PH 6.2 Glucose < 20 mg/dl, and Gram-positive coccus in direct bacteriological examination). The obstetric evaluation revealed signs of fetal distress with decreased variability of fetal heart rate and late decelerations. A thoracic multislice CT-scan evidenced condensation of the right inferior lobe associated with pleural effusion and a collection in the upper retroperitoneum in contiguity with the pleural space (Fig. 1). After this unexpected finding, it was decided to add an abdomino-pelvis scan at the same time, that showed the extension of the retroperitoneal collection and findings consistent with a complicated appendicitis. Due to the patient's clinical and fetal health condition, prompt interruption of pregnancy and an emergency surgical exploration of abdominal cavity and thorax were decided.
Fig. 1.
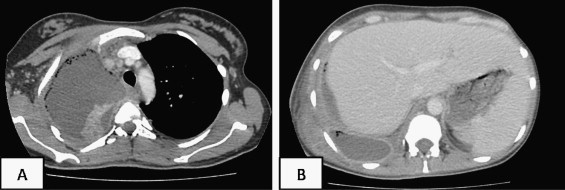
(A) Right lung consolidation image and homolateral pleural effusion. (B) Abscess in retrocural space in contact with pleura.
A caesarean section was performed by an infraumbilical midline incision. The fetus was delivered with good vitality (APGAR 8/10) and taken to the Neonatal Intensive Care Unit. An extended supraumbilical incision was performed to complete the exploration of the whole abdominal cavity. There was no free abdominal fluid, collections or signs of local inflammation. The retroperitoneum was accessed after mobilizing the right colon. Retrocecal perforated appendicitis with a contiguous abscess was identified and drained. Appendectomy was therefore performed. A right posterolateral thoracotomy was the approach chosen to explore the thorax. The pleural space showed purulent fluid ascending from the retroperitoneum, pleural peel and the presence of an inferior lobe abscess, which involved the whole parenchyma.
Due to the findings mentioned above, a right inferior pulmonary lobectomy was performed. The patient had an uneventful postoperative course, stayed 4 days at the Intensive Care Unit (ICU) and then was transferred to the general ward. A control CT-scan showed evacuated collections in thorax and abdomen (Fig. 2). She was discharged at postoperative day 10.
Fig. 2.
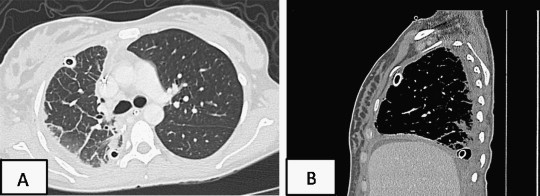
(A) Absence of pleural effusion after surgery. (B) Improvement and decrease in size of retroperitoneal collection.
The newborn presented hyaline membrane disease due to insufficient surfactant factor given by the gestational age. She was treated in Neonatal ICU with a favorable recovery and was discharged 1 month after birth without complications.
Pathology study confirmed the diagnosis of AA and Bronchopneumonia.
3. Discussion
Acute appendicitis is a recognized cause of acute surgical abdomen and the most common non-obstetrical surgical condition of the abdomen complicating pregnancy. Prompt diagnosis and early treatment are necessary for a successful resolution and to prevent complications. However, some patients do not present typical signs and symptoms, causing delays in diagnosis with an increased risk of complications such as perforation of the appendix, retroperitoneal abscess or generalized peritonitis.
This diverse clinical presentation is given by the different anatomical positions of the appendix. As reported in the literature, the most frequent location of the appendix is retrocecal (65%).4 AA in these patients often developed often an atypical presentation, simulating biliary colic, kidney or urinary tract infections.5 This results in a delayed diagnosis, with the consequent risk of appendicle perforation, which reaches 20% according to different series.6
Despite the standardization and scientific evidence of safety, specificity and sensitivity of the various imaging work-up techniques,7–9 the diagnosis of AA in these patients is still challenging.
In pregnancy, the anatomic and physiologic changes that may mask and delay the diagnosis of acute appendicitis include a cephalic displacement of the appendix from the right lower quadrant by the uterus enlargement, an increased leukocyte count and a physiologic increase in blood volume that makes it difficult to recognize tachycardia or hypotension.
Our patient presented non-specific symptoms, resulting in delayed diagnosis and the consequent complications. The perforation of a retrocecal appendix, as presented in our patient, might result in a large retroperitoneal abscess as a complication of the disease.
After a literature review, we found few reports of some rare cases regarding AA with retroperitoneal abscesses formation, however the presentation of empyema as a complication of appendicitis due to the extension of a retroperitoneal abscess is exceptional.1–3 As far as we know, this is the first report of an empyema as a complication of appendicitis in a pregnant woman.
The retrocrural space connects the thoracic cavity with the retroperitoneum. This fact, in association with the different pressures between the thorax and the abdomen as well as the lymph flow direction, explains the development of an empyema following an abdominal infection.10
When a pregnant patient with a suspected AA is presented, an abdominal ultrasound should be the first imaging study to complement the clinical evaluation as recommended in the algorithm proposed by Patel et al.8 When the abdominal US findings are unclear, the MRI is currently considered the gold standard for the diagnosis of AA in pregnancy.7–9 Despite this, due to the lack of abdominal signs or symptoms of AA in our patient and her critical overall condition, we choose a CT-scan since we required a faster study that provides information of the thorax and the upper abdominal cavity. The use of this complex imaging method allowed us to suspect the abdominal origin of the patient's condition and rapidly confirm an AA after completing the study with an abdominal scan.
Finally, with the clinical features and imaging findings, the need of a prompt and efficient treatment, was clear. The abdominal approach through a midline incision allowed us to perform the cesarean operation as well as a complete abdominal exploration. In order to achieve a satisfactory resolution of the thoracic disease in the surgical scenario, we found that the presence of an experienced thoracic surgeon is essential, who decides the lobar resection and adequate drainage of the thoracic cavity.
4. Conclusion
An empyema or lung abscess caused by an abdominal infection is a rare entity, especially as consequence of acute appendicitis. However, when a retroperitoneal infection is established, it may eventually compromise the thoracic cavity by contiguous spread.
The septic condition of a pregnant patient with a significant thoraco-abdominal infection requires an initial aggressive approach, with the interruption of pregnancy and urgent exploration of the chest and abdominal cavity. In such a critical situation, it is important to provide a multidisciplinary assessment, where thoracic and general surgeons together with obstetricians and ICU specialists work by means of a team effort for a better result and safety of the newborn and mother.
Conflict of interest
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient's next of kin for publication of this case report and accompanying images.
Author contributions
Agustin Dietrich and Matias Nicolas made data collection along with Jose Iniesta and the two authors (A.D. and M.N.) prepared the documentation, David Eduardo Smith set the study design and prepared the documentation.
References
- 1.Law D.K., Murr P., Bailey W.C. Empyema. A rare presentation of perforated appendicitis. JAMA. 1978;240(23):2566–2567. doi: 10.1001/jama.240.23.2566. [DOI] [PubMed] [Google Scholar]
- 2.Herline A., Burton E.M., Hatley R. Thoracic empyema in a patient with acute appendicitis: a rare association. Journal of Pediatric Surgery. 1994;29(December (2)):1623–1625. doi: 10.1016/0022-3468(94)90243-7. [DOI] [PubMed] [Google Scholar]
- 3.García Marín A., Martín Gil J., Nofuentes Riera C., Vaquero Rodríguez A., Pérez Díaz M.D., Turégano Fuentes F. Thoracic empyema due to subphrenic appendicitis: an infrequent presentation. Acta Gastroenterologica Latinoamericana. 2010;40(September (3)):276–277. [PubMed] [Google Scholar]
- 4.Wakeley C.P. The position of the vermiform appendix as ascertained by an analysis of 10,000 cases. Journal of Anatomy. 1933;67(January (Pt 2)):277–283. [PMC free article] [PubMed] [Google Scholar]; Ahmed I., Asgeirsson K.S., Beckingham I.J., Lobo D.N. The position of the vermiform appendix at laparoscopy. Surgical and Radiologic Anatomy. 2007;29(March (2)):165–168. doi: 10.1007/s00276-007-0182-8. [Epub 2007 February 23] [DOI] [PubMed] [Google Scholar]
- 5.Ong E.M.W., Venkatesh S.K. Ascending retrocecal appendicitis presenting with right upper abdominal pain: utility of computed tomography. World Journal of Gastroenterology. 2009;15(28):3576–3579. doi: 10.3748/wjg.15.3576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hale D.A. Appendectomy a contemporary appraisal. Annals of Surgery. 1997;225(3):252–261. doi: 10.1097/00000658-199703000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wieseler K.M., Bhargava P., Kanal K.M., Vaidya S., Stewart B.K., Dighe M.K. Imaging in pregnant patients: examination appropriateness. Radiographics. 2010;30(September (5)):1215–1229. doi: 10.1148/rg.305105034. [discussion 1230-3] [DOI] [PubMed] [Google Scholar]
- 8.Patel S.J., Reede D.L., Katz D.S., Subramaniam R., Amorosa J.K. Imaging the pregnant patient for nonobstetric conditions: algorithms and radiation dose considerations. Radiographics. 2007;27(November–December (6)):1705–1722. doi: 10.1148/rg.276075002. [DOI] [PubMed] [Google Scholar]
- 9.Pedrosa I., Lafornara M., Pandharipande P.V., Goldsmith J.D., Rofsky N.M. Pregnant patients suspected of having acute appendicitis: effect of MR imaging on negative laparotomy rate and appendiceal perforation rate. Radiology. 2009;250(3):749–757. doi: 10.1148/radiol.2503081078. [DOI] [PubMed] [Google Scholar]
- 10.Panicek D.M., Benson C.B., Gottlieb R.H., Heitzman E.R. The diaphragm: anatomic, pathologic, and radiologic considerations. RadioGraphics. 1988;8(May (3)) doi: 10.1148/radiographics.8.3.3289099. [DOI] [PubMed] [Google Scholar]