

Abstract
Introduction
Inversion of the impacted tooth is a rare condition. The purpose of this article is to review this rare condition in detail on the basis of available literature. In addition, this article also explores the various multidisciplinary approaches varying from space creation to prosthodontic rehabilitation and reimplantation to endodontic treatment for inverted impacted teeth.
Discussion
A very few cases of inverted and impacted third molars have been reported in the literature. We describe few rare cases of inverted impacted teeth which presented to us in the Dept. Of Oral Surgery, K.D. Dental College and Hospital over a period of 2 years approx. we report of four cases presented to us with inverted maxillary third molars (Figs. 1, 2), inverted supernumerary tooth in anterior maxilla (Figs. 3, 4).
Result
The first and second case of maxillary third molar and third case, of supernumerary tooth, the patients presented were asymptomatic, hence patient opted for conservative management and continued follow up, in the fourth case, the supernumerary tooth was removed for orthodontic reasons.
Conclusion
On the basis of literature available, it has been noticed that related complications particularly depend on justification on whether the tooth follicle is with a pathology or is pathology-free. Pathology-free and asymptomatic cases can be treated in a conservative manner. Possible treatment protocol for impacted inversion is entirely dependent on patient’s needs, findings and surgeons skills.
Keywords: Inverted, Impacted, Conservative treatment, Surgical removal, Reimplantation
Introduction
Impacted teeth may therefore be non-functional, abnormal, or pathological [1, 2]. An impacted tooth is one, which is prevented from its normal path of eruption in the dental arch due to lack of space in the arch or obstruction in the eruptive pathway of the tooth [3]. Maxillary and mandibular third molars as well as the maxillary cuspids are the most frequently impacted teeth in permanent dentition [4]. In the mandible, the most common location of such 3rd molars is in the ascending ramus. In the maxilla the teeth may be displaced as far as the floor of the orbit. Primary teeth are rarely impacted, in 1:10,000 times most commonly involving the primary second molars [5].
Unusual proliferation of odontogenic epithelium before the development of tooth germ leads the 3rd molars to deviate from their normal location.
Case Reports
A very few cases of inverted and impacted third molars have been reported in the literature. We describe few rare cases of inverted and impacted unilateral mandibular as well as maxillary 3rd molars which presented to us in the Department of oral surgery K.D Dental College and hospital over a period of 2 years approx.
We report of four cases presented to us with inverted third molars, two maxillary (Figs. 1, 2), inverted supernumerary tooth in anterior maxilla (Figs. 3, 4). The first and second case of maxillary third molar and third case with supernumerary tooth patient presented with were asymptomatic, hence patient opted for conservative management and continues follow up, in the fourth case, the supernumerary tooth was removed due to orthodontic reasons.
Fig. 1.

A case of inverted maxillary 3rd molar on right side showing no pathological change in dental follicle and was asymptomatic. Subsequently treated by conservative method that is tooth left in bone as such
Fig. 2.
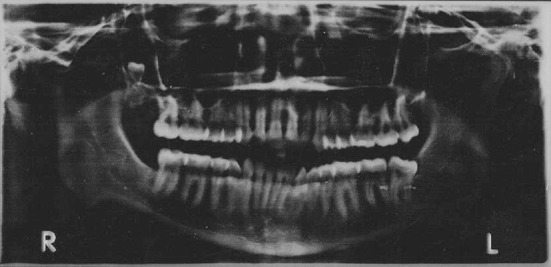
OPG depicting a inverted impacted right upper third molar
Fig. 3.

IOPA shows an inverted impacted supernumerary tooth present between the roots of central incisors, which was co-incidentally diagnosed during treatment of fractured central incisor
Fig. 4.

IOPA showing inverted impacted supernumerary tooth, with its incisal edge encroaching into the nasal fossa
Discussion
Involvement of inverted third molars and a few other teeth were also reported randomly. Two cases of primary incisors have been reported wherein the first case, maxillary incisors were inverted and impacted in a 5 year old boy, subsequently treated with multidisciplinary approach [surgical exposure and orthodontic treatment] [5]. In the second case, lower primary incisors were reported in a 4 year old child, which was considered as microform of ectodermal dysplasia on the basis of family history [6]. Literature shows very few incidences of premolar involvement, only two cases have been reported so far, one case with inverted lower second premolar germ [7]. Other reported case showed involvement of upper second premolar [8]. Although inverted impaction is a rare condition faced in daily practice, but decision about its treatment protocol is of utmost importance. It is clear in literature there are no exact treatment protocols for removing inverted teeth. The most conservative treatment is considered as the safest protocol. The surgical intervention for inverted molars is more complicated than other types of impactions because the abnormal position of the crown makes it greatly inaccessible and requires exhaustive bone removal, loss of excessive bone and nerve damage is the major disadvantage in such cases [9, 10]. With the recent advents in armamentarium and surgeons skills, apart from removal of involved tooth other modes of surgical interventions were also reported. Reimplantation of inverted tooth or inverted tooth germ in upright position is one of the possible treatment protocols [7, 8]. Reimplantation is always accompanied with multidisciplinary approach. Justification of carrying out conservative treatment protocol or surgical intervention is dependent on ruling out whether the tooth follicle is with pathological changes or without pathology, and, secondly on the patient’s need in terms of esthetics, function and behavior. In case of inverted impacted incisors, extraction followed by prosthetic rehabilitation is considered to fulfill esthetic needs and restore normal speech. As far as inverted premolars are concerned, reimplantation of tooth is considered as a better protocol. One case reported multidisciplinary approach where the adjacent first molar was endodontically treated and distalised orthodontically to create space, after which upper inverted premolar was surgically removed and reimplanted in an upright position [8]. Another case of impacted inverted lower second premolar tooth germ and its treatment protocol includes surgical uprighting of inverted tooth germ preserving primary lower second molar [7]. Interestingly, follow- up in both cases showed maintenance of vitality in reimplanted teeth [7, 8]. In literature two rarer cases have been reported, one showing a symptomatic inverted molar 17 mm long, in the left nasal cavity [11]. Other showing extra oral eruption of inverted mandibular molars along left inferior border of mandible [12]. Both cases were symptomatic and therefore treated by surgical intervention. The former case was treated under general anesthesia [11].
Conclusion
On the basis of literature available, it has been noticed that related complications particularly depend on justification that whether the tooth follicle has a pathology or is pathology-free. Pathology-free and asymptomatic cases can be treated in a conservative manner. Conservative treatment may include leaving molars as such in the bone, reimplantation in cases of incisors and premolars because they show sufficient accessibility for surgical intervention. In cases of reimplantation of incisors esthetics is prime concern. If follicle shows pathological changes then surgical intervention is required so as to reduce the associated risks. The advent of fibro-optic endoscope in dentistry, which can be used to remove such tooth from sinus or nasal cavity, has greatly reduced morbidity [13]. So in the present era the consideration of possible treatment protocol for impacted inversion is entirely dependent on patient’s need, findings and surgeons skills.
Contributor Information
Shishir Mohan, Email: drshishirdent@yahoo.co.in.
Hasti Kankariya, Email: drhasti81@gmail.com.
Sandeep Fauzdar, Email: drsandeep_fauzdar@yahoo.com.
References
- 1.Waite PD, Raynolds RR. Surgical management of impacted third molars. Semin Orthod. 1998;4:2–113. doi: 10.1016/S1073-8746(98)80008-X. [DOI] [PubMed] [Google Scholar]
- 2.Killy HC, Kay LW. The impacted wisdom tooth. 3. London: Churchill Livingstone; 1978. pp. 18–19. [Google Scholar]
- 3.Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 4. Philadelphia: WB Saunders; 1983. pp. 66–68. [Google Scholar]
- 4.Dachi SF, Howell FV. A survey of 3874 routine full-mouth radiographs. II. A study of impacted teeth. Oral Surg. 1961;14:1165. doi: 10.1016/0030-4220(61)90204-3. [DOI] [PubMed] [Google Scholar]
- 5.Kapur A, Goyal A, Jaffri S. Management of inverted impacted primary incisors: an unusual case. J Indian Soc Pedod Prev Dent. 2008;26(1):26–28. doi: 10.4103/0970-4388.40318. [DOI] [PubMed] [Google Scholar]
- 6.Uzamiş M, Olmez S, Er N. Unusual impaction of inverted primary incisor: report of case. ASDC J Dent Child. 2001;68(1):67–69. [PubMed] [Google Scholar]
- 7.Engel M, Katsaros C. Replantation of an inverted lower second premolar germ. J Orofac Orthop. 1997;58(5):282–285. [PubMed] [Google Scholar]
- 8.Ulusoy AT, Akkocaoglu M, Akan S, Kocadereli I, Cehreli ZC. Reimplantation of an inverted maxillary premolar: case report of a multidisciplinary treatment approach. J Clin Pediatr Dent. 2009;33(4):279–282. doi: 10.17796/jcpd.33.4.f141658760372j12. [DOI] [PubMed] [Google Scholar]
- 9.Pai V, Kundabala M, Sequier PS, Rao A. Inverted and impacted maxillary and mandibular 3rd molars; a very rare case. J Oral Health Comm Dent. 2008;2(1):8–9. [Google Scholar]
- 10.Kugelberg CF, Ahlstrom U, Ericson S, Hugoson A, Kvint S. Periodontal healing after impacted lower third molar surgery in adolescents and adults. A prospective study. Int J Oral Maxillofac Surg. 1991;20(1):18–24. doi: 10.1016/S0901-5027(05)80689-7. [DOI] [PubMed] [Google Scholar]
- 11.Kuroda H, Tsutsumi K, Tomisawa H, Koizuka I. A case of an inverted tooth in the nasal cavity. Auris Nasus Larynx. 2003;30(Suppl):S127–S129. doi: 10.1016/S0385-8146(02)00131-1. [DOI] [PubMed] [Google Scholar]
- 12.Kumar Dash J, Mohapatra M, Mishra L. Extraoral inverted teeth eruption: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(1):37–39. doi: 10.1016/j.tripleo.2004.02.060. [DOI] [PubMed] [Google Scholar]
- 13.Salim T, Khalid U, Hamid A, Ghaffar S. Supernumerary, ectopic tooth in the maxillary antrum presenting with recurrent haemoptysis. Head Face Med. 2010;6:26. doi: 10.1186/1746-160X-6-26. [DOI] [PMC free article] [PubMed] [Google Scholar]