

Abstract
Ossification of the stylohyoid ligament is very common in the Caucasian population. More than 9000 descriptions of apparently isolated case reports on PubMed have been cited over the last 20 years, often associated with an incidental finding on imaging after neck trauma. No cases of familial ossification have been described. We document a family with several affected members, each with an ossified stylohyoid ligament, confirming that ossification may be hereditary in some families and is most likely due to an autosomal dominant gene.
Ossification of the stylohyoid ligament (Eagle syndrome) [1] is a common disorder in the Caucasian population. More than 9000 descriptions of apparently isolated case reports on PubMed have been cited over the last 20 years, often associated with neck trauma. Surprisingly, no cases of familial ossification have been described. We present a family with several affected members, each with an ossified stylohyoid ligament, confirming that Eagle syndrome may be hereditary in some families and is most likely due to an autosomal dominant gene.
Phenotype description
We identified a 56-year-old female (Figure 1 III.2) who was noted to have an ossified stylohyoid ligament on radiological imaging at the age of 30 years (Figure 2) when she developed a swallowing difficulty. She previously had a difficult intubation during anaesthesia for surgery when aged 22 years, which is thought to be coincidental. Radiological investigation of all the family members in generations III and IV confirmed that her identical twin sister (III.3) was affected along with her mother (II.5) (Figure 3) and her two children IV.1 (Figure 4) and IV.2 (Figure 1). All the imaging (including II.5′s films, which are a little fainter generally given her age and the film exposure) shows the same degree and extent of calcification of the stylohyoid ligament. This is consistent with a single autosomal dominant gene, with limited expression symptom-wise but consistent penetrance on imaging, and no evidence of anticipation (progressively earlier onset of a disorder owing to expansion of a gene in successive generations) [2].
Figure 1.
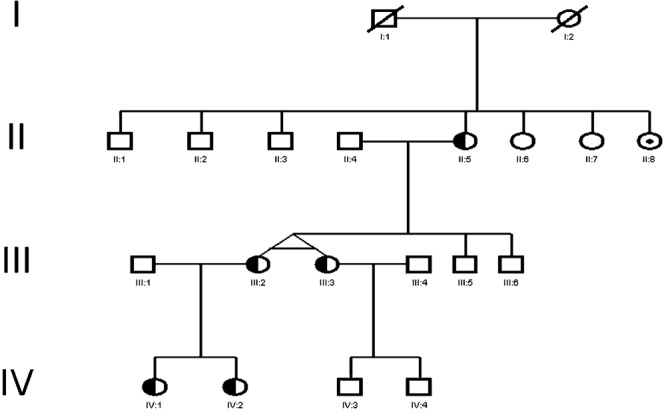
Pedigree showing three generations of affected cases (shaded) and those with a history of throat trouble (dot), and unaffected cases (unshaded).
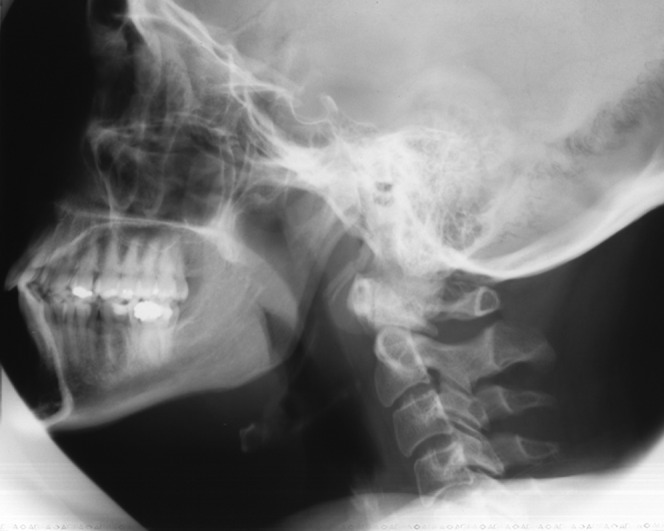
Figure 2.

Radiograph of III.2 showing calcification extending from the styloid process towards the hyoid bone at age 57 years.
Figure 3.

Radiograph of II.5 showing similar calcification extending from the styloid process towards the hyoid bone at age 82 years.
Figure 4.
Radiograph of IV.1 showing similar calcification extending from the styloid process towards the hyoid bone at age 56 years.
All were asymptomatic with no particular history of trauma or throat or ear pain. An aunt (II.8) had throat trouble in her early 30s but no further clinical details or imaging was available as all relatives in generation II are deceased.
Discussion
Eagle syndrome is thought to be present in 4–28% of the population [3]. A similar condition—ossification of the posterior longitudinal ligament of the spine (OPLLS)—is prevalent in 2–4% of the Japanese population, causing myelopathy and spinal stenosis, and COL6A1 gene polymorphisms have been associated, although no definitive genes have been identified [4]. Familial studies on OPLLS confirmed a higher increase in relatives, but it is unclear whether this is due to an autosomal dominant or autosomal recessive gene or both [5]. Ossification has been noted in other cervical spine ligaments including the flaval ligament [6], but the aetiology of the ossification process is unclear.
The inheritance in this family is clearly autosomal dominant, with three generations affected. A gene may therefore be responsible for some cases of familial ossification of the styloid ligament, and identification of further families may allow research in this area. Several members of this family were asymptomatic, suggesting limited expression of the disorder, although all had consistent features of calcification on imaging, suggesting that the effect of the gene is about the same in all cases. This condition may be more common in relatives of apparently sporadic cases than previously thought, as none of the relatives in whom an ossified stylohyoid ligament was detected had any symptoms or signs.
Conclusion
Familial ossification of the stylohyoid ligament is a discrete clinical entity and displays autosomal dominant inheritance. Not all cases of this condition may be sporadic as previously thought.
References
- 1.Eagle WW. Elongated styloid process: report of two cases. Arch Otolaryngol 1937;25:584–7 [DOI] [PubMed] [Google Scholar]
- 2.Morrison PJ, Johnston WP, Nevin NC. The epidemiology of Huntington disease in Northern Ireland. J Med Genet 1995;32:524–30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Omnell KH, Ghandi C, Omnell ML. Ossification of the human stylohyoid ligament. Med Oral Pathol Oral Radiol Endod 1998;85:226–32 [DOI] [PubMed] [Google Scholar]
- 4.Kong Q, Ma X, Li F, Guo Z, Qi Q, Li W, et al. COL6A1 polymorphisms associated with ossification of the ligamentum flavum and ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976) 2007;32:2834–8 [DOI] [PubMed] [Google Scholar]
- 5.Terayama K. Genetic studies on ossification of the posterior longitudinal ligament of the spine. Spine (Phila Pa 1976) 1989;14:1184–91 [DOI] [PubMed] [Google Scholar]
- 6.Guo JJ, Yang HL, Cheung KM, Tang TS, Luk KD. Classification and management of the tandem ossification of the posterior longitudinal ligament and flaval ligament. Chin Med J 2009;122:219–24 [PubMed] [Google Scholar]