

Abstract
The incidence of obesity has increased dramatically during recent decades. Obesity increases the risk for metabolic and cardiovascular diseases and may therefore contribute to premature death. With increasing fat mass, secretion of adipose tissue derived bioactive molecules (adipokines) changes towards a pro-inflammatory, diabetogenic and atherogenic pattern. Adipokines are involved in the regulation of appetite and satiety, energy expenditure, activity, endothelial function, hemostasis, blood pressure, insulin sensitivity, energy metabolism in insulin sensitive tissues, adipogenesis, fat distribution and insulin secretion in pancreatic β-cells. Therefore, adipokines are clinically relevant as biomarkers for fat distribution, adipose tissue function, liver fat content, insulin sensitivity, chronic inflammation and have the potential for future pharmacological treatment strategies for obesity and its related diseases. This review focuses on the clinical relevance of selected adipokines as markers or predictors of obesity related diseases and as potential therapeutic tools or targets in metabolic and cardiovascular diseases.
Keywords: Adipokines; Adipose tissue; Biological markers; Cardiovascular diseases; Diabetes mellitus, type 2; Fat distribution; Insulin resistance; Obesity
INTRODUCTION
It is widely accepted that obesity and abdominal fat distribution contribute to the individual risk for type 2 diabetes, dyslipidemia, fatty liver disease, chronic subclinical inflammation, hypertension, and cardiovascular disease [1-3]. Dissection of the molecular mechanisms underlying obesity and its relationship to metabolic and cardiovascular diseases are essential for developing new strategies for prevention and treatment of these disorders. However, we are only at the beginning to understand the mechanistic link between obesity and its associated metabolic and vascular diseases. In the past two decades, advances in obesity research have led to the recognition that adipose tissue is an active endocrine organ that secretes more than 600 bioactive factors termed adipokines [4]. Adipokines play important roles in the regulation of appetite and satiety control, fat distribution, insulin sensitivity and insulin secretion, energy expenditure, inflammation, blood pressure, hemostasis, and endothelial function [5-11]. In an autocrine and paracrine manner, adipokines contribute to the modulation of adipogenesis, immune cell migration into adipose tissue, adipocyte metabolism and function [5,6]. Most importantly, adipokines have significant systemic effects on target organs including the brain, liver, muscle, vasculature, heart and pancreatic β-cells (Fig. 1) [5,6]. The adipokine secretion pattern reflects adipose tissue function and seems to be important for determining the individual risk to develop metabolic and cardiovascular comorbidities of obesity [1,3-6]. When adipose tissue inflammation and dysfunction have developed, adipokine secretion is significantly changed towards a diabetogenic, proinflammatory, and atherogenic pattern [1,3-6].
Fig. 1.

Effects of adipokines. Adipokines regulate adipogenesis, adipocyte metabolism, immune cell migration into adipose tissue via autocrine and paracrine signalling. In addition, adipokines have endocrine/systemic effects on appetite and satiety control, regulation of energy expenditure and activity, influence insulin sensitivity and energy metabolism in insulin sensitive tissues, such as liver, muscle and fat as well as insulin secretion in pancreatic β-cells. IL, interleukin; TNFα, tumour necrosis factor alpha; MCP-1, monocyte-chemotactic-protein-1; FABP4, fatty acid binding protein 4; RBP4, retinol-binding-protein-4.
In 1987, adipose tissue was identified as a major site for sex steroid metabolism [8] and production of adipsin, an endocrine factor that is negatively correlated with obesity in rodents [9]. The discovery of leptin as an adipokine [7] further stimulated the discovery of new adipose tissue derived signals [3-5]. Since then, the search for novel adipokines, but more importantly the molecular characterization of newly identified adipokines with unknown function represents a major topic in obesity research. Secretion of adipokines (e.g., leptin, chemerin, monocyte-chemotactic-protein-1 [MCP-1], retinol-binding-protein-4 [RBP4]) may either closely reflect body fat mass and body weight dynamic or be related to other factors including adipose tissue function or dietary pattern (e.g., adiponectin, fetuin-A, C-reactive protein [CRP], progranulin, vaspin) [10,11].
However, there remains a major challenge to characterize the function, mode of action and molecular targets for the growing list of newly identified adipokines. Recently, 44 novel adipokines with unknown function have been identified using and unbiased protein profiling approach of the secretome of primary human adipocytes [12,13]. Among the more of 600 putative adipokines [4], there are molecules which play a role inflammatory response including interleukins (IL)-1, -6, -8, -10, tumour necrosis factor alpha (TNFα), transforming growth factor β (TGFβ), interferon-γ, CRP, plasminogen activator inhibitor-1, and chemerin (Table 1). Several adipokines including RBP4, chemerin, vaspin, fetuin-A, omentin, and fatty acid binding protein 4 have been associated with insulin resistance and fatty liver disease (Table 1), whereas adiponectin positively correlates with insulin sensitivity [reviewed in 3,5]. Other adipokines may cause or reflect adverse fat distribution including RBP4 [14], dipeptidyl peptidase-4 (DPP-4) [15], chemerin [16,17], apelin [reviewed in 18], vaspin [19,20], endocannabinoids [21], fetuin-A [22], omentin [23], and progranulin [24] (Table 1) [5]. Adipokines may represent the link between obesity and hypertension (e.g., angiotensinogen), endothelial function (e.g., omentin, apelin), hemostasis (e.g., fibrinogen), immune cell infiltration in adipose tissue (e.g., MCP-1, progranulin and macrophage inflammatory protein-1α) [3-5]. For several adipokines including resistin, visfatin/PBEF/Nampt, progranulin, fractalkine the clinical relevance of altered serum concentrations is either not clear or controversial [3-5]. The role of the adipokines leptin and adiponectin as mediators linking increased fat mass and/or impaired adipose tissue function to metabolic and cardiovascular diseases has been extensively characterized during the past years [25-29]. In addition to the discussion of these classical adipokines, this review focuses on the clinical importance of more recently identified adipokines [3-5,14-17,22-24,30] as biomarkers and therapeutic tools or targets for obesity related diseases.
Table 1.
Relevance of selected adipokines as biomarkers or therapeutic tools
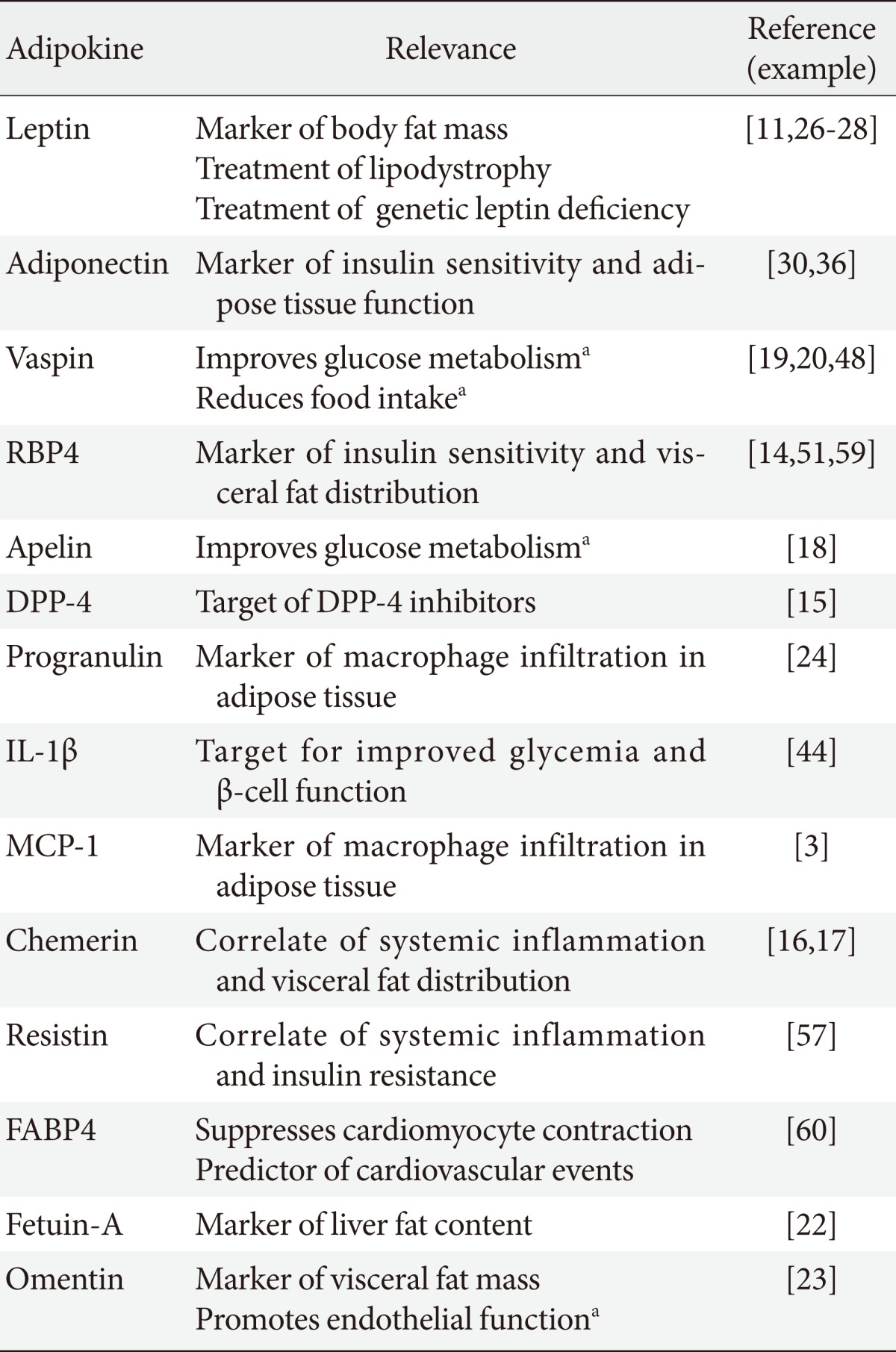
RBP4, retinol-binding-protein-4; DPP-4, dipeptidyl peptidase-4; IL, interleukin; MCP-1, monocyte-chemotactic-protein-1; FABP4, fatty acid binding protein 4.
aDemonstrated in animal models only.
LEPTIN
Leptin was discovered in 1994 as the protein product of the ob gene mutation, which causes extreme obesity in the ob/ob mouse model [7]. The importance of altered leptin signalling for the development of obesity and diabetes is further supported by the discovery that a mutation in the leptin receptor gene causes obesity and diabetes in db/db mice [reviewed in 25]. Leptin is almost exclusively secreted from adipocytes, controls food intake and energy expenditure and has atherogenic and growth properties [25]. Leptin decreases orexigenic and increases anorexigenic peptide synthesis in the hypothalamus thereby decreasing appetite [25]. Obesity is associated with increased leptin serum concentrations, which potentially contribute to the development of insulin resistance and the metabolic syndrome [25]. Interestingly, exogenous administration of leptin does not significantly influence appetite and body weight in obese patients, a phenomenon which has been attributed to central leptin resistance [26]. It has been suggested that leptin exerts insulin sensitizing effects by increasing fatty acid oxidation and decreasing triglyceride storage in muscle [25]. In addition to the effects of leptin on insulin sensitivity, there may be a direct link between high circulating leptin concentrations and increased cardiovascular risk [1,5,25]. Leptin may enhance platelet aggregation and arterial thrombosis, promote angiogenesis, impair arterial distensibility and induce proliferation and migration of vascular smooth muscle cells [25].
In addition, to its potential role as mediator of insulin resistance, leptin has been identified as an important regulator of β-cell mass and cell survival [31]. Studies in the leptin receptor-deficient Zucker diabetic fatty (ZDF) rats reveal that the reduction in β-cell mass is primarily due to increased rate of β-cell death and not related to proliferation [32].
ADIPONECTIN
Adiponectin has been discovered in 1995 and was originally named Acrp30 [33]. Several groups identified this protein in a different context and referred to it as adipoQ [34], and apM1 [35], until the consensus name 'adiponectin' found widespread acceptance [36]. Since its discovery, several different functions have been found for adiponectin. There is consensus that adiponectin generally exerts insulin sensitising, anti-inflammatory and anti-apoptotic actions on a number of different cell types [36]. Consistent with these properties, adiponectin release from adipocytes is down-regulated under adverse metabolic conditions, resulting in reduced circulating adiponectin levels [36]. Furthermore, adiponectin expression and secretion increase upon improved insulin sensitivity and weight loss [36]. Insulin-sensitizing TZDs probably mediate part of their effect via adiponectin since they increase plasma concentrations of this adipokine in both, subjects with normal insulin sensitivity and type 2 diabetes in vivo [36]. In contrast, various hormones associated with insulin resistance and obesity including catecholamines, insulin, glucocorticoids, TNFα and IL-6 down-regulate adiponectin expression and secretion in fat cells in vitro [37]. Besides its peripheral effects, adiponectin acts in the brain to increase energy expenditure and cause weight loss [3,5,36].
The role of adiponectin as an endogenous insulin sensitizer was discovered using experimental down-regulation of the adiponectin gene in knockout mice [29]. Two independent studies demonstrate impaired insulin sensitivity in adiponectin knockout mice as compared to wild type controls [29, reviewed in 36]. In mice with transgenic overexpression, adiponectin was shown to have anti-obesity effects due to enhanced energy expenditure and impairment of adipocyte differentiation [38].
The effects of adiponectin on glucose homeostasis may be mediated both via effects on peripheral insulin sensitivity and insulin secretion [31]. Adiponectin plays a direct role in improving insulin sensitivity on the whole body level [36]. One mechanism how adiponectin directly improves insulin sensitivity is that the globular C-terminal fragment reduces glucose levels by increasing fatty acid combustion in myocytes [reviewed in 36]. Moreover, adiponectin exerts significnant anti-inflammatory effects [36]. In addition, adiponectin improves insulin sensitivity by paracrine action in fat cells [37] and most likely also in hepatocytes [36]. Potential effects of adiponectin on insulin secretion in β-cells, has been examined in several recent studies [31,36]. Transgenic ob/ob mice overexpressing the globular domain of adiponectin have increased insulin sensitivity and increased insulin secretion independently of body weight compared to control mice [39]. These results suggest that adiponectin has in addition to its insulin-sensitizing properties protective effects on β-cells [31]. Adiponectin is able to mitigate the apoptotic effects of either palmitate- or ceramide-induced cell death-an effect that may critically depend on the formation of the downstream conversion product of ceramide, sphingosine-1 phosphate in β-cells in vitro [36]. Further in vivo studies in C57BL/6 mice demonstrated that systemic adiponectin administration results in increased insulin secretion [40]. Adiponectin has additional anti-atherogenic effects and low adiponectin serum concentrations are associated with increased risk for cardiovascular disease [36]. Endothelium dependent vasoreactivity is impaired in people with low adiponectin levels, which could contribute to the development of hypertension in visceral obese individuals [36]. In addition, it has been suggested that adiponectin protects plaque rupture by the inhibition of matrix metalloproteinase function [41], because adiponectin increases the expression of tissue inhibitor of metalloproteinase in macrophages and selectively suppresses endothelial cell apoptosis [41].
ADIPOKINES AS THERAPEUTIC TOOLS
Leptin as therapy of lipodystrophy and leptin deficiency
Adipokines may be clinically relevant both as therapeutic tools or targets in the treatment of obesity and its related diseases. The clinical use of leptin is an example how basic adipokine research may be translated into novel treatment concepts. Although chronic leptin administration does not significantly reduce body weight in common human obesity, exogenous leptin can significantly improve insulin resistance, glucose and lipid metabolism when endogenous leptin levels are low such as in patients with lipodystrophy [26]. Moreover, in rare cases of genetically-based leptin deficiency in morbidly-obese patients, leptin treatment is able to rescue the morbidly obese phenotype [27]. In women with hypothalamic amenorrhea, recombinant leptin therapy improved reproductive, thyroid, and growth hormone axes, as well as markers of bone formation [28]. Taken together, leptin can serve as a model that adipokines can be successfully used in the treatment of diseases.
DPP-4: an adipokine target
Another example for the role adipokines in the treatment of metabolic diseases has been recently provided by the discovery, that adipose tissue secretes DPP-4 [15]. DPP-4 is a 766 amino acid membrane-associated, serine-protease enzyme [42]. The enzyme is widely detected in numerous tissues such as kidney, liver, intestine, spleen, lymphocytic organs, placenta, adrenal glands, and vascular endothelium [42]. Increased DPP-4 expression and secretion from adipose tissue in obesity may impair insulin sensitivity in an autocrine and paracrine fashion [15]. Lamers et al. [15] further demonstrated that DPP-4 release significantly correlates with adipocyte size, suggesting that DPP-4 may be involved in linking adipose tissue to impaired glucose homeostasis. Increased DPP-4 activity and serum concentrations in obesity may serve as a model how altered adipokine secretion may be successfully used as therapeutic target in the treatment of obesity related diseases.
Inhibition of DPP-4 is now a well-established therapeutic principle to lower hyperglycemia in patients with type 2 diabetes. The glucose lowering properties of DPP-4 inhibitors are due to the mechanism that under normal physiological conditions, DPP-4 rapidly degrades glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) [42]. Nutrient intake stimulates the release of the incretin hormones GIP and GLP-1 into the circulation [42]. Important functions of both incretins include potentiating glucose-dependent insulin secretion from pancreatic β-cells and inhibiting glucagon secretion, which in turn reduces hepatic gluconeogenesis [42]. The effect of incretins is significantly reduced in patients with type 2 diabetes and contributes to impaired insulin secretion and chronic hyperglycemia [42].
IL-1β as an adipokine target
Adipose tissue expresses and releases IL-1β [43]. IL-1β is a proinflammatory cytokine which has been proposed to play a role in inflammatory pancreatic β-cell destruction leading to type 1 diabetes [44]. IL-1β inhibits the function and promotes the apoptosis of β-cells [44]. The blockade of IL-1 with a recombinant human IL-1-receptor antagonist (anakinra) has been shown to improve glycemia and β-cell function and reduced markers of systemic inflammation in a double-blind, parallel-group clinical trial involving 70 patients with type 2 diabetes [44]. Therefore IL-1β represents a model that in addition to the direct use of adipokines as therapeutic strategy, adipokines may be indirectly used as target molecules for the treatment of obesity comorbidities.
However, for most adipokines, effects of acute and chronic treatment have only been tested in the context of animal studies and there is no clinical application yet. Among several adipokines with a potential for future use as pharmacological treatment strategy, apelin and vaspin have been recently extensively studied [18-20].
Apelin
Apelin is an adipokine which plays a role in the regulation of glucose homeostasis and may contribute to the link between increased adipose tissue mass and obesity related metabolic diseases [18]. Apelin, a 36 amino-acid peptide endogenous ligand of the G-protein-coupled receptor APJ receptor, has been identified in a variety of tissues, including central nervous system with high expression in the hypothalamus, stomach, heart, skeletal muscle, and white adipose tissue [reviewed in 18]. Apelin serum concentration was shown to be higher in patients with obesity and insulin resistance [18]. Recently, higher apelin serum concentrations were found to be associated with liver cirrhosis both in rats and humans [18]. Moreover, treatment of rats with cirrhosis with an apelin receptor antagonist showed diminished hepatic fibrosis and loss of ascites suggesting the hepatic apelin system as a novel therapeutic target in liver disease [45]. Apelin serum concentrations correlate with hyperinsulinemia and obesity, suggesting that apelin may be another adipokine mediator of impaired adipose tissue function in obesity [18]. Interestingly, apelin administration has been shown to have glucose-lowering effects associated with enhanced glucose utilization in skeletal muscle and fat [46]. Moreover, apelin restored glucose tolerance and increased glucose utilization in obese and insulin-resistant mouse models [46]. Collectively, data obtained from apelin treatment in different rodent models indicate that apelin influences glucose homeostasis and may contribute to the link between increased adipose tissue mass and obesity related metabolic and inflammatory diseases [18].
Vaspin
Visceral adipose tissue-derived serpin (vaspin) gained a lot of attention since it has been identified as a member of serine protease inhibitor family, which was expressed in visceral adipose tissue of Otsuka Long-Evans Tokushima Fatty (OLETF) rats at the age when obesity and insulin plasma concentrations reach a peak [19]. We found vaspin expression in adipose tissue [47], stomach and rodent pancreatic islets [48], however the mechanisms how vaspin secretion may be linked to deterioration of glucose metabolism and insulin sensitivity are not entirely understood. In OLETF rats, tissue expression of vaspin and its serum levels decrease with worsening of diabetes and body weight loss at 50 weeks and could be normalized with insulin or pioglitazone treatment [19]. Administration of vaspin to obese mice improves glucose tolerance, insulin sensitivity and altered gene expression of candidate genes for insulin resistance [19]. Moreover, we could recently show that treatment of different mouse models with recombinant vaspin leads to sustained glucose lowering and reduction of food intake [48], suggesting vaspin as a treatment target for future pharmacological therapies of obesity and its related metabolic diseases.
ADIPOKINES AS BIOMARKERS
Adipokines have a potential clinical relevance as biomarkers for fat mass, fat distribution, adipose tissue function, liver fat content, insulin sensitivity, and subclinical chronic inflammation associated with metabolic diseases. As a prominent example, circulating leptin levels are highly correlated with adipose tissue mass, and can thus be used as a surrogate for changes in the amount of adipose tissue [3,10,11]. Leptin may be one example for additional adipokines that signal the functional status of adipose tissue to other tissues and frequently reflect weight changes. Using an unbiased proteomics approach, we recently detected differential abundance of proteins associated with fat mass for antithrombin-III, clusterin, complement C3 and complement C3b, pigment epithelium-derived factor, RBP4, serum amyloid P, and vitamin-D binding protein [49].
In clinical practice measurement of adipokines which only reflect weight changes will not improve individual therapeutic decisions. However, there is a need in the monitoring of weight loss therapies for novel biomarkers, which predict how successful an individual can loose weight, which weight loss strategy may be the best and weight regain. In addition, there is no biomarker which distinguishes whether weight regain during diet interventions is due to diet failure or occurs despite healthy dieting. Adipokine biomarkers may also be promising candidates to predict the individual weight loss outcome with regard to improved cardiovascular function, insulin sensitivity, inflammation, liver function and steatosis, and adipose tissue function. In line with this, we recently described two distinct adipokine biomarker patterns [11] among 322 participants of the 2-year Dietary Intervention Randomized Controlled Trial (DIRECT) of low-fat, Mediterranean or low-carbohydrate diets for weight loss [50]. One pattern includes biomarkers (insulin, triglycerides, leptin, chemerin, MCP-1, and RBP4) whose dynamics tightly correspond to changes in body weight [11], whereas a different pattern was observed for adiponectin, high density lipoprotein cholesterol, hsCRP, fetuin-A, progranulin, and vaspin. The latter pattern reflected lifestyle factors such as physical activity and healthier diet beyond simple associations with body fat mass [11].
Fat distribution
The search for adipokines which are exclusively expressed in distinct fat depots has not revealed a specific fat depot marker so far. However, there are several candidate adipokines, for which circulating levels strongly correlate with visceral fat distribution. Circulating biomarkers for abdominal visceral fat accumulation include adiponectin, RBP4, vaspin, chemerin, progranulin, omentin, fetuin-A and others [30]. We and others have recently shown that adiponectin serum concentration negatively correlates with visceral fat mass [30], whereas RBP4 [51], vaspin [20], chemerin [17], fetuin-A [22], omentin [23], and progranulin [24] are predictors of increased visceral fat distribution.
As a potential marker for visceral fat mass, visfatin, which has been previously identified as a protein involved in B-cell maturation (pre-B colony enhancing factor), caught much attention, because it was suggested to be exclusively expressed in visceral adipose tissue and have insulin mimetic effects [5]. With several subsequent studies it became clear that visfatin is expressed in many cells and tissues and represents the enzyme nicotinamide phosphoribosyltransferase (Nampt, EC 2.4.2.12) [52]. Although visfatin/PBEF/Nampt is clearly not exclusively expressed in visceral fat [52], a positive correlation between visceral adipose tissue visfatin/PBEF/Nampt gene expression and body mass index (BMI), was supported by a number of subsequent studies demonstrating that plasma visfatin levels in humans correlate with obesity and visceral fat mass [52].
We have recently extended the original finding that vaspin expression is higher in visceral depots of OLETF rats [19] by demonstrating fat depot-specific vaspin expression in obese individuals [47]. Elevated vaspin serum concentrations are associated with obesity, impaired insulin sensitivity and fitness level [20]. Analyses of vaspin serum concentrations in the 2-year DIRECT study [50] further revealed vaspin as a novel biomarker for a continuous beneficial response to switching to healthier dietary patterns [11].
RBP4 is predominantly secreted from the liver, but also expressed in adipocytes [14]. However, increased RBP4 serum concentrations have been shown to be the result of increased RBP4 expression in visceral adipose tissue of patients with insulin resistance [51]. RBP4 has gained a lot of attention after the first notion that it is elevated in the serum of insulin resistant humans and mice and that increased RBP4 serum concentrations are associated with obesity, insulin resistance, and abdominal fat distribution [14,51]. Therefore, increased RBP4 serum concentrations might causally link (visceral) obesity to insulin resistance and its associated metabolic diseases. We recently showed that RBP4 serum concentration patterns closely follow the body weight pattern in response to different diet regimens, suggesting that RBP4 rather reflect than cause changes in body weight and glucose homeostasis [11].
Analyses of chemerin concentrations in portal, hepatic and systemic venous blood revealed that visceral fat is not a major site of chemerin release, and elevated systemic levels of chemerin in obesity and type 2 diabetes seem to be associated with inflammation rather than BMI [17]. We recently postulated an important role of chemerin in the initiation of adipose tissue inflammation and dysfunction and suggested that reduced adipose tissue chemerin expression may contribute to improved insulin sensitivity and subclinical inflammation beyond significant weight loss [17].
Progranulin is a secreted protein with important functions in several processes, including immune response and embryonic development [53]. In adipose tissue, progranulin is secreted both from adipocytes and infiltrating macrophages [24]. We recently found that elevated progranulin serum concentrations are associated with visceral obesity, elevated plasma glucose, and dyslipidemia [24]. Taken together, adipokine serum concentrations may serve as biomarkers for visceral fat mass and could therefore be clinically important to avoid expensive direct measurement of visceral fat mass using magnetic resonance imaging scans.
Adipose tissue inflammation and dysfunction
Adipose tissue dysfunction and ectopic fat accumulation belong to the early abnormalities in the development of obesity and seem to be important factors determining the individual risk to develop metabolic and cardiovascular comorbidities of obesity [1,3-6]. With the development of adipose tissue dysfunction, adipokine secretion is significantly altered. These changes in adipokine secretion are very likely to link impaired adipose tissue function to insulin resistance and cardiovascular disease [1,3-6]. Hotamisligil et al. [54] first discovered the existence of an inflammatory state involving adipose tissue and its potential role in obesity by demonstrating the secretion of TNFα by the adipose tissue [54]. TNFα expression increases in adipocytes of obese animals, and the neutralisation of TNFα by a TNFα soluble antibody leads to an improvement of insulin sensitivity [54]. These observations exhibit the existence of a strong link between a proinflammatory cytokine, produced and secreted by adipose tissue, and the development of insulin resistance associated with obesity progression. These findings opened a new field of research in the domain of inflammation and obesity [1,3-6].
In addition to adipocytes, macrophages in human adipose tissue may contribute to enhance the obesity-related 'low-grade' chronic inflammation [3]. Various observations support the hypothesis of a potential deleterious role for adipose-infiltrated macrophages in the pathogenesis of obesity-associated diseases [3]. Indeed, increased number of macrophages in adipose tissue might cause increased systemic concentrations of pro-inflammatory cytokines. The action of these inflammatory molecules may represent the molecular link between adipose tissue and the metabolic, cardiovascular or even hepatic complications of obesity. In particular, increased levels of TNFα, IL-6, progranulin and MCP-1, produced by activated macrophages may directly contribute to the mechanisms of change in the insulin sensitivity in different adipose depots [3]. Due to the significant overlap between visceral fat distribution and adipose tissue inflammation, which is typically more pronounced in omental compared to subcutaneous fat [3], the same factors which may predict visceral fat mass are predictors of adipose tissue inflammation. Such molecules include MCP-1 [55,56], chemerin [17], omentin [23], progranulin [24], and others. Noteworthy, disruption of MCP1 action by knockout of either MCP1 or its receptor CC chemokine receptor 2 is associated with protection against insulin resistance further supporting the notion that increased adipose tissue macrophage infiltration may causally link obesity with insulin resistance [55,56]. In addition, we recently found that progranulin may contribute to immune cell attraction into adipose tissue and could therefore be a novel marker of chronic inflammation in obesity and type 2 diabetes. Progranulin closely reflects omental adipose tissue macrophage infiltration and improved insulin sensitivity after physical training significantly reduces elevated circulating progranulin in patients with type 2 diabetes [24].
Insulin sensitivity and glucose homeostasis
Obesity does not necessarily translate into increased risk for comorbidities and ~15% of obese individuals do not develop obesity associated disorders [30]. Therefore the pathogenic link between increased adipose tissue mass and higher risk for obesity related disorders including impaired insulin sensitivity is not necessarily directly related to fat mass. Adipose tissue dysfunction and ectopic fat accumulation seem to be important factors determining the individual risk to develop insulin resistance as comorbidity of obesity. To identify adipokines, which are independently of body fat mass are associated with impaired insulin sensitivity, we systematically characterized paired samples from abdominal subcutaneous and intraabdominal omental adipose tissue of insulin sensitive obese individuals compared with BMI-, age-, and gender-matched insulin resistant obese individuals without significant comorbidities including type 2 diabetes [30]. Increased circulating concentrations of RBP4 [14,51], vaspin [20], MCP-1 [55,56], visfatin/PBEF/Nampt [52], chemerin [17], progranulin [24] and fetuin-A [22] and decreased adiponectin serum concentrations [36] have been shown to be associated with either insulin resistance, obesity or both. However, it has been difficult to dissect the effects of obesity and insulin resistance on increased serum concentrations of these molecules. Comparison of insulin sensitive versus insulin resistant obese patients provided new evidence for a significant body fat mass independent role for adiponectin, chemerin, progranulin, RBP4 and fetuin-A in the development or at least as markers of insulin resistant obesity [30]. Among those markers, adiponectin has been shown to be a sensitive biomarker for insulin sensitivity in extensive studies [36]. In addition to these potential biomarkers of insulin resistance, increased activity of circulating DPP-4 derived from adipose tissue expression may impair insulin sensitivity in an autocrine and paracrine fashion [15]. Resistin has originally been suggested as an adipokine upregulated during weight gain, impairing insulin sensitivity, and linking insulin resistance with obesity in mice [57]. A recent large study involving the Framingham offspring cohort confirmed a significant relationship between insulin resistance and circulating resistin in humans, but found that this relationship was not independent of BMI [58].
A relationship between RBP4, insulin resistance and impaired glucose homeostasis has been first reported in mice lacking glucose transporter 4 in adipose tissue and has been subsequently confirmed in human cohorts [14,51]. These mice exhibit significantly higher RBP4 serum concentrations as their control littermates [59]. The effects of RBP4 are mediated through retinol-dependent or retinol-independent mechanisms [59]. It has been demonstrated that RBP4 can induce the retinoid-regulated gene encoding the gluconeogenic enzyme phosphoenolpyruvate carboxykinase (PEPCK), increase basal glucose production, and reduce insulin action to suppress glucose production in hepatocytes in vitro [59]. Recombinant RBP4 treatment in mice causes an impaired suppression of hepatic glucose production in response to maximal insulin concentrations [59] providing another mechanistic link between RBP4 induced insulin resistance, which might lead to increased fat accumulation [51].
CONCLUSIONS
Adipose tissue is an active endocrine organ, which produces a number of bioactive molecules, so called adipokines. Altered adipokine secretion may represent a link between adipose tissue dysfunction in obesity and metabolic and cardiovascular obesity-related disorders. Adipokines are important modulators of glucose metabolism, because they may primarily contribute to adverse fat distribution (e.g., chemerin, RBP4), altered appetite and satiety (e.g., leptin, vaspin), impaired insulin sensitivity (e.g., adiponectin, leptin, RBP4) or insulin secretion (e.g., leptin, adiponectin), and to inflammation (e.g., resistin, IL-6, TNFα, MCP-1, chemerin, progranulin). Functional characterization of newly identified adipokines which may link obesity to glucose homeostasis represents a main research focus. The identification of adipokine related mechanisms will be a prerequisit for translation into novel pharmacological treatment approaches of obesity, insulin resistance and type 2 diabetes.
ACKNOWLEDGMENTS
This work was supported by the Kompetenznetz Adipositas (Competence Network for Obesity) funded by the Federal Ministry of Education and Research (FKZ 01GI0829).
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Van Gaal LF, Mertens IL, De Block CE. Mechanisms linking obesity with cardiovascular disease. Nature. 2006;444:875–880. doi: 10.1038/nature05487. [DOI] [PubMed] [Google Scholar]
- 2.LeRoith D, Novosyadlyy R, Gallagher EJ, Lann D, Vijayakumar A, Yakar S. Obesity and type 2 diabetes are associated with an increased risk of developing cancer and a worse prognosis: epidemiological and mechanistic evidence. Exp Clin Endocrinol Diabetes. 2008;116(Suppl 1):S4–S6. doi: 10.1055/s-2008-1081488. [DOI] [PubMed] [Google Scholar]
- 3.Bluher M. Adipose tissue dysfunction in obesity. Exp Clin Endocrinol Diabetes. 2009;117:241–250. doi: 10.1055/s-0029-1192044. [DOI] [PubMed] [Google Scholar]
- 4.Lehr S, Hartwig S, Sell H. Adipokines: a treasure trove for the discovery of biomarkers for metabolic disorders. Proteomics Clin Appl. 2012;6:91–101. doi: 10.1002/prca.201100052. [DOI] [PubMed] [Google Scholar]
- 5.Bluher M. Do adipokines link obesity to its related metabolic and cardiovascular diseases? Clin Lipidol. 2010;5:95–107. [Google Scholar]
- 6.Bays HE. "Sick fat," metabolic disease, and atherosclerosis. Am J Med. 2009;122(1 Suppl):S26–S37. doi: 10.1016/j.amjmed.2008.10.015. [DOI] [PubMed] [Google Scholar]
- 7.Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372:425–432. doi: 10.1038/372425a0. [DOI] [PubMed] [Google Scholar]
- 8.Siiteri PK. Adipose tissue as a source of hormones. Am J Clin Nutr. 1987;45(1 Suppl):277–282. doi: 10.1093/ajcn/45.1.277. [DOI] [PubMed] [Google Scholar]
- 9.Flier JS, Cook KS, Usher P, Spiegelman BM. Severely impaired adipsin expression in genetic and acquired obesity. Science. 1987;237:405–408. doi: 10.1126/science.3299706. [DOI] [PubMed] [Google Scholar]
- 10.Wajchenberg BL. Subcutaneous and visceral adipose tissue: their relation to the metabolic syndrome. Endocr Rev. 2000;21:697–738. doi: 10.1210/edrv.21.6.0415. [DOI] [PubMed] [Google Scholar]
- 11.Bluher M, Rudich A, Kloting N, Golan R, Henkin Y, Rubin E, Schwarzfuchs D, Gepner Y, Stampfer MJ, Fiedler M, Thiery J, Stumvoll M, Shai I. Two patterns of adipokine and other biomarker dynamics in a long-term weight loss intervention. Diabetes Care. 2012;35:342–349. doi: 10.2337/dc11-1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lehr S, Hartwig S, Lamers D, Famulla S, Muller S, Hanisch FG, Cuvelier C, Ruige J, Eckardt K, Ouwens DM, Sell H, Eckel J. Identification and validation of novel adipokines released from primary human adipocytes. Mol Cell Proteomics. 2012;11:M111.010504. doi: 10.1074/mcp.M111.010504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dahlman I, Elsen M, Tennagels N, Korn M, Brockmann B, Sell H, Eckel J, Arner P. Functional annotation of the human fat cell secretome. Arch Physiol Biochem. 2012;118:84–91. doi: 10.3109/13813455.2012.685745. [DOI] [PubMed] [Google Scholar]
- 14.Graham TE, Yang Q, Bluher M, Hammarstedt A, Ciaraldi TP, Henry RR, Wason CJ, Oberbach A, Jansson PA, Smith U, Kahn BB. Retinol-binding protein 4 and insulin resistance in lean, obese, and diabetic subjects. N Engl J Med. 2006;354:2552–2563. doi: 10.1056/NEJMoa054862. [DOI] [PubMed] [Google Scholar]
- 15.Lamers D, Famulla S, Wronkowitz N, Hartwig S, Lehr S, Ouwens DM, Eckardt K, Kaufman JM, Ryden M, Muller S, Hanisch FG, Ruige J, Arner P, Sell H, Eckel J. Dipeptidyl peptidase 4 is a novel adipokine potentially linking obesity to the metabolic syndrome. Diabetes. 2011;60:1917–1925. doi: 10.2337/db10-1707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wittamer V, Franssen JD, Vulcano M, Mirjolet JF, Le Poul E, Migeotte I, Brezillon S, Tyldesley R, Blanpain C, Detheux M, Mantovani A, Sozzani S, Vassart G, Parmentier M, Communi D. Specific recruitment of antigen-presenting cells by chemerin, a novel processed ligand from human inflammatory fluids. J Exp Med. 2003;198:977–985. doi: 10.1084/jem.20030382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chakaroun R, Raschpichler M, Kloting N, Oberbach A, Flehmig G, Kern M, Schon MR, Shang E, Lohmann T, Dressler M, Fasshauer M, Stumvoll M, Bluher M. Effects of weight loss and exercise on chemerin serum concentrations and adipose tissue expression in human obesity. Metabolism. 2012;61:706–714. doi: 10.1016/j.metabol.2011.10.008. [DOI] [PubMed] [Google Scholar]
- 18.Castan-Laurell I, Dray C, Attane C, Duparc T, Knauf C, Valet P. Apelin, diabetes, and obesity. Endocrine. 2011;40:1–9. doi: 10.1007/s12020-011-9507-9. [DOI] [PubMed] [Google Scholar]
- 19.Hida K, Wada J, Eguchi J, Zhang H, Baba M, Seida A, Hashimoto I, Okada T, Yasuhara A, Nakatsuka A, Shikata K, Hourai S, Futami J, Watanabe E, Matsuki Y, Hiramatsu R, Akagi S, Makino H, Kanwar YS. Visceral adipose tissue-derived serine protease inhibitor: a unique insulin-sensitizing adipocytokine in obesity. Proc Natl Acad Sci U S A. 2005;102:10610–10615. doi: 10.1073/pnas.0504703102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Youn BS, Kloting N, Kratzsch J, Lee N, Park JW, Song ES, Ruschke K, Oberbach A, Fasshauer M, Stumvoll M, Bluher M. Serum vaspin concentrations in human obesity and type 2 diabetes. Diabetes. 2008;57:372–377. doi: 10.2337/db07-1045. [DOI] [PubMed] [Google Scholar]
- 21.Bluher M, Engeli S, Kloting N, Berndt J, Fasshauer M, Batkai S, Pacher P, Schon MR, Jordan J, Stumvoll M. Dysregulation of the peripheral and adipose tissue endocannabinoid system in human abdominal obesity. Diabetes. 2006;55:3053–3060. doi: 10.2337/db06-0812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stefan N, Hennige AM, Staiger H, Machann J, Schick F, Krober SM, Machicao F, Fritsche A, Haring HU. Alpha2-Heremans-Schmid glycoprotein/fetuin-A is associated with insulin resistance and fat accumulation in the liver in humans. Diabetes Care. 2006;29:853–857. doi: 10.2337/diacare.29.04.06.dc05-1938. [DOI] [PubMed] [Google Scholar]
- 23.Schaffler A, Neumeier M, Herfarth H, Furst A, Scholmerich J, Buchler C. Genomic structure of human omentin, a new adipocytokine expressed in omental adipose tissue. Biochim Biophys Acta. 2005;1732:96–102. doi: 10.1016/j.bbaexp.2005.11.005. [DOI] [PubMed] [Google Scholar]
- 24.Youn BS, Bang SI, Kloting N, Park JW, Lee N, Oh JE, Pi KB, Lee TH, Ruschke K, Fasshauer M, Stumvoll M, Bluher M. Serum progranulin concentrations may be associated with macrophage infiltration into omental adipose tissue. Diabetes. 2009;58:627–636. doi: 10.2337/db08-1147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ahima RS, Flier JS. Leptin. Annu Rev Physiol. 2000;62:413–437. doi: 10.1146/annurev.physiol.62.1.413. [DOI] [PubMed] [Google Scholar]
- 26.Savage DB, O'Rahilly S. Leptin: a novel therapeutic role in lipodystrophy. J Clin Invest. 2002;109:1285–1286. doi: 10.1172/JCI15326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH, Prentice AM, Hughes IA, McCamish MA, O'Rahilly S. Effects of recombinant leptin therapy in a child with congenital leptin deficiency. N Engl J Med. 1999;341:879–884. doi: 10.1056/NEJM199909163411204. [DOI] [PubMed] [Google Scholar]
- 28.Welt CK, Chan JL, Bullen J, Murphy R, Smith P, DePaoli AM, Karalis A, Mantzoros CS. Recombinant human leptin in women with hypothalamic amenorrhea. N Engl J Med. 2004;351:987–997. doi: 10.1056/NEJMoa040388. [DOI] [PubMed] [Google Scholar]
- 29.Fruebis J, Tsao TS, Javorschi S, Ebbets-Reed D, Erickson MR, Yen FT, Bihain BE, Lodish HF. Proteolytic cleavage product of 30-kDa adipocyte complement-related protein increases fatty acid oxidation in muscle and causes weight loss in mice. Proc Natl Acad Sci U S A. 2001;98:2005–2010. doi: 10.1073/pnas.041591798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kloting N, Fasshauer M, Dietrich A, Kovacs P, Schon MR, Kern M, Stumvoll M, Bluher M. Insulin-sensitive obesity. Am J Physiol Endocrinol Metab. 2010;299:E506–E515. doi: 10.1152/ajpendo.00586.2009. [DOI] [PubMed] [Google Scholar]
- 31.Lee YH, Magkos F, Mantzoros CS, Kang ES. Effects of leptin and adiponectin on pancreatic beta-cell function. Metabolism. 2011;60:1664–1672. doi: 10.1016/j.metabol.2011.04.008. [DOI] [PubMed] [Google Scholar]
- 32.Pick A, Clark J, Kubstrup C, Levisetti M, Pugh W, Bonner-Weir S, Polonsky KS. Role of apoptosis in failure of beta-cell mass compensation for insulin resistance and beta-cell defects in the male Zucker diabetic fatty rat. Diabetes. 1998;47:358–364. doi: 10.2337/diabetes.47.3.358. [DOI] [PubMed] [Google Scholar]
- 33.Scherer PE, Williams S, Fogliano M, Baldini G, Lodish HF. A novel serum protein similar to C1q, produced exclusively in adipocytes. J Biol Chem. 1995;270:26746–26749. doi: 10.1074/jbc.270.45.26746. [DOI] [PubMed] [Google Scholar]
- 34.Hu E, Liang P, Spiegelman BM. AdipoQ is a novel adipose-specific gene dysregulated in obesity. J Biol Chem. 1996;271:10697–10703. doi: 10.1074/jbc.271.18.10697. [DOI] [PubMed] [Google Scholar]
- 35.Maeda K, Okubo K, Shimomura I, Funahashi T, Matsuzawa Y, Matsubara K. cDNA cloning and expression of a novel adipose specific collagen-like factor, apM1 (AdiPose Most abundant Gene transcript 1) Biochem Biophys Res Commun. 1996;221:286–289. doi: 10.1006/bbrc.1996.0587. [DOI] [PubMed] [Google Scholar]
- 36.Turer AT, Scherer PE. Adiponectin: mechanistic insights and clinical implications. Diabetologia. 2012;55:2319–2326. doi: 10.1007/s00125-012-2598-x. [DOI] [PubMed] [Google Scholar]
- 37.Fasshauer M, Klein J, Neumann S, Eszlinger M, Paschke R. Hormonal regulation of adiponectin gene expression in 3T3-L1 adipocytes. Biochem Biophys Res Commun. 2002;290:1084–1089. doi: 10.1006/bbrc.2001.6307. [DOI] [PubMed] [Google Scholar]
- 38.Bauche IB, El Mkadem SA, Pottier AM, Senou M, Many MC, Rezsohazy R, Penicaud L, Maeda N, Funahashi T, Brichard SM. Overexpression of adiponectin targeted to adipose tissue in transgenic mice: impaired adipocyte differentiation. Endocrinology. 2007;148:1539–1549. doi: 10.1210/en.2006-0838. [DOI] [PubMed] [Google Scholar]
- 39.Yamauchi T, Kamon J, Waki H, Imai Y, Shimozawa N, Hioki K, Uchida S, Ito Y, Takakuwa K, Matsui J, Takata M, Eto K, Terauchi Y, Komeda K, Tsunoda M, Murakami K, Ohnishi Y, Naitoh T, Yamamura K, Ueyama Y, Froguel P, Kimura S, Nagai R, Kadowaki T. Globular adiponectin protected ob/ob mice from diabetes and ApoE-deficient mice from atherosclerosis. J Biol Chem. 2003;278:2461–2468. doi: 10.1074/jbc.M209033200. [DOI] [PubMed] [Google Scholar]
- 40.Okamoto M, Ohara-Imaizumi M, Kubota N, Hashimoto S, Eto K, Kanno T, Kubota T, Wakui M, Nagai R, Noda M, Nagamatsu S, Kadowaki T. Adiponectin induces insulin secretion in vitro and in vivo at a low glucose concentration. Diabetologia. 2008;51:827–835. doi: 10.1007/s00125-008-0944-9. [DOI] [PubMed] [Google Scholar]
- 41.Kobayashi H, Ouchi N, Kihara S, Walsh K, Kumada M, Abe Y, Funahashi T, Matsuzawa Y. Selective suppression of endothelial cell apoptosis by the high molecular weight form of adiponectin. Circ Res. 2004;94:e27–e31. doi: 10.1161/01.RES.0000119921.86460.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nauck MA. Incretin-based therapies for type 2 diabetes mellitus: properties, functions, and clinical implications. Am J Med. 2011;124(1 Suppl):S3–S18. doi: 10.1016/j.amjmed.2010.11.002. [DOI] [PubMed] [Google Scholar]
- 43.Sopasakis VR, Nagaev I, Smith U. Cytokine release from adipose tissue of nonobese individuals. Int J Obes (Lond) 2005;29:1144–1147. doi: 10.1038/sj.ijo.0803002. [DOI] [PubMed] [Google Scholar]
- 44.Larsen CM, Faulenbach M, Vaag A, Volund A, Ehses JA, Seifert B, Mandrup-Poulsen T, Donath MY. Interleukin-1-receptor antagonist in type 2 diabetes mellitus. N Engl J Med. 2007;356:1517–1526. doi: 10.1056/NEJMoa065213. [DOI] [PubMed] [Google Scholar]
- 45.Principe A, Melgar-Lesmes P, Fernandez-Varo G, del Arbol LR, Ros J, Morales-Ruiz M, Bernardi M, Arroyo V, Jimenez W. The hepatic apelin system: a new therapeutic target for liver disease. Hepatology. 2008;48:1193–1201. doi: 10.1002/hep.22467. [DOI] [PubMed] [Google Scholar]
- 46.Dray C, Knauf C, Daviaud D, Waget A, Boucher J, Buleon M, Cani PD, Attane C, Guigne C, Carpene C, Burcelin R, Castan-Laurell I, Valet P. Apelin stimulates glucose utilization in normal and obese insulin-resistant mice. Cell Metab. 2008;8:437–445. doi: 10.1016/j.cmet.2008.10.003. [DOI] [PubMed] [Google Scholar]
- 47.Kloting N, Berndt J, Kralisch S, Kovacs P, Fasshauer M, Schon MR, Stumvoll M, Bluher M. Vaspin gene expression in human adipose tissue: association with obesity and type 2 diabetes. Biochem Biophys Res Commun. 2006;339:430–436. doi: 10.1016/j.bbrc.2005.11.039. [DOI] [PubMed] [Google Scholar]
- 48.Kloting N, Kovacs P, Kern M, Heiker JT, Fasshauer M, Schon MR, Stumvoll M, Beck-Sickinger AG, Bluher M. Central vaspin administration acutely reduces food intake and has sustained blood glucose-lowering effects. Diabetologia. 2011;54:1819–1823. doi: 10.1007/s00125-011-2137-1. [DOI] [PubMed] [Google Scholar]
- 49.Oberbach A, Bluher M, Wirth H, Till H, Kovacs P, Kullnick Y, Schlichting N, Tomm JM, Rolle-Kampczyk U, Murugaiyan J, Binder H, Dietrich A, von Bergen M. Combined proteomic and metabolomic profiling of serum reveals association of the complement system with obesity and identifies novel markers of body fat mass changes. J Proteome Res. 2011;10:4769–4788. doi: 10.1021/pr2005555. [DOI] [PubMed] [Google Scholar]
- 50.Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, Golan R, Fraser D, Bolotin A, Vardi H, Tangi-Rozental O, Zuk-Ramot R, Sarusi B, Brickner D, Schwartz Z, Sheiner E, Marko R, Katorza E, Thiery J, Fiedler GM, Bluher M, Stumvoll M, Stampfer MJ Dietary Intervention Randomized Controlled Trial (DIRECT) Group. Weight loss with a low-carbohydrate, mediterranean, or low-fat diet. N Engl J Med. 2008;359:229–241. doi: 10.1056/NEJMoa0708681. [DOI] [PubMed] [Google Scholar]
- 51.Kloting N, Graham TE, Berndt J, Kralisch S, Kovacs P, Wason CJ, Fasshauer M, Schon MR, Stumvoll M, Bluher M, Kahn BB. Serum retinol-binding protein is more highly expressed in visceral than in subcutaneous adipose tissue and is a marker of intra-abdominal fat mass. Cell Metab. 2007;6:79–87. doi: 10.1016/j.cmet.2007.06.002. [DOI] [PubMed] [Google Scholar]
- 52.Berndt J, Kloting N, Kralisch S, Kovacs P, Fasshauer M, Schon MR, Stumvoll M, Bluher M. Plasma visfatin concentrations and fat depot-specific mRNA expression in humans. Diabetes. 2005;54:2911–2916. doi: 10.2337/diabetes.54.10.2911. [DOI] [PubMed] [Google Scholar]
- 53.Tolkatchev D, Malik S, Vinogradova A, Wang P, Chen Z, Xu P, Bennett HP, Bateman A, Ni F. Structure dissection of human progranulin identifies well-folded granulin/epithelin modules with unique functional activities. Protein Sci. 2008;17:711–724. doi: 10.1110/ps.073295308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hotamisligil GS, Shargill NS, Spiegelman BM. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science. 1993;259:87–91. doi: 10.1126/science.7678183. [DOI] [PubMed] [Google Scholar]
- 55.Kanda H, Tateya S, Tamori Y, Kotani K, Hiasa K, Kitazawa R, Kitazawa S, Miyachi H, Maeda S, Egashira K, Kasuga M. MCP-1 contributes to macrophage infiltration into adipose tissue, insulin resistance, and hepatic steatosis in obesity. J Clin Invest. 2006;116:1494–1505. doi: 10.1172/JCI26498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Weisberg SP, Hunter D, Huber R, Lemieux J, Slaymaker S, Vaddi K, Charo I, Leibel RL, Ferrante AW., Jr CCR2 modulates inflammatory and metabolic effects of high-fat feeding. J Clin Invest. 2006;116:115–124. doi: 10.1172/JCI24335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, Wright CM, Patel HR, Ahima RS, Lazar MA. The hormone resistin links obesity to diabetes. Nature. 2001;409:307–312. doi: 10.1038/35053000. [DOI] [PubMed] [Google Scholar]
- 58.Hivert MF, Sullivan LM, Fox CS, Nathan DM, D'Agostino RB, Sr, Wilson PW, Meigs JB. Associations of adiponectin, resistin, and tumor necrosis factor-alpha with insulin resistance. J Clin Endocrinol Metab. 2008;93:3165–3172. doi: 10.1210/jc.2008-0425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Yang Q, Graham TE, Mody N, Preitner F, Peroni OD, Zabolotny JM, Kotani K, Quadro L, Kahn BB. Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes. Nature. 2005;436:356–362. doi: 10.1038/nature03711. [DOI] [PubMed] [Google Scholar]
- 60.Lamounier-Zepter V, Look C, Alvarez J, Christ T, Ravens U, Schunck WH, Ehrhart-Bornstein M, Bornstein SR, Morano I. Adipocyte fatty acid-binding protein suppresses cardiomyocyte contraction: a new link between obesity and heart disease. Circ Res. 2009;105:326–334. doi: 10.1161/CIRCRESAHA.109.200501. [DOI] [PubMed] [Google Scholar]