

Abstract
Aripiprazole is the third generation atypical antipsychotic and a dopamine serotonin system stabilizer (DSS) effective against positive and negative symptoms of schizophrenia. It has a low propensity for extrapyramidal side effects, causes minimal weight gain or sedation, produces no elevation in serum prolactin levels, and does not cause prolongation of QTc interval. This case report is of a patient suffering from schizophrenia (paranoid). The patient developed oculogyric crisis (acute dystonia) with aripiprazole dose uptitration. Dystonic reaction resolved with promethazine administration. Naranjo's causality assessment reveals probable association of aripiprazole with oculogyric crisis. A thorough workup and vigilance is required prior to initiation of aripiprazole in the case of schizophrenia.
Keywords: Aripiprazole, oculogyric crisis, promethazine
INTRODUCTION
Aripiprazole is the third generation atypical antipsychotic and a dopamine serotonin system stabilizer (DSS) that is effective against positive and negative symptoms of schizophrenia. It has a low propensity for extrapyramidal side effects, causes minimal weight gain or sedation, produces no elevation in serum prolactin levels and does not cause prolongation of QTc interval. It is partial agonist at D2 and 5HT1A and blocks 5HT2A receptors.[1–3] The most common adverse reactions in adult patients reported in clinical trials with dosage of 10–15 mg per day were fatigue, insomnia, headache, nausea, vomiting, tremors, rigidity, akathisia, and constipation.[3,4] Overall incidence of acute dystonic reactions with antipsychotic medications is 2.5–5%, majority of which are due to typical and high potency antipsychotics.[5] The following case report is of aripiprazole-induced oculogyric crisis (acute dystonia).
CASE REPORT
A 28-year-old single female was brought by her relatives to the psychiatry outpatient clinic. For last 8–9 months, she was interacting less with family. As per history, she was suspicious towards family members that they would poison her and also feared that few strangers would come and kill her. In addition, she was talking to herself, was occasionally irritable and had sleep disturbance. After psychiatric evaluation, her mental status examination revealed delusion of persecution which was primary, well systematized, complete, and intermittent and associated with intense fear of being harmed palpitations and irritability. She also had auditory hallucinations of an unknown male, commenting on her day-to-day work and occasionally criticizing her; associated with the patient replying to the voice. She was diagnosed as schizophrenia (paranoid).[6] Her weight was 70 kg, and she had a family history (mother) of diabetes mellitus. Her baseline investigations of hemogram, liver function and renal function tests, chest X-ray, and electrocardiogram were within the normal range. She was prescribed aripiprazole 10 mg orally in two divided dosages per day, eszopiclone 2 mg orally at nighttime dosage and was advised follow-up after 2 weeks. During her first follow-up visit, she showed improvement in sleep. For improvement in psychotic symptoms, aripiprazole was increased to 20 mg orally in two divided dosages and was advised follow-up after 2 weeks.
After 5 days of dose increment, she was brought with complaints of upward rolling of eye balls suddenly, unexpected, occurring five to seven times a day, which were difficult to bring back to original position by the patient. It persisted for half an hour approximately and resolved on its own. After evaluation for conversion disorder, tardive dystonia, epileptic encephalopathy, anti epileptic drug intake,[7] she was diagnosed of having oculogyric crisis (acute dystonia).[6] The patient was admitted in psychiatry ward. Aripiprazole was withdrawn and immediately injection promethazine 50 mg intramuscularly was given, which was repeated after half an hour.[7] Her symptoms improved in next 1 hour and the patient was prescribed 25 mg promethazine orally in night time dosage. Within 3 days of admission, she completely recovered from oculogyric symptoms. On discharge, she was put on aripiprazole 10 mg orally in two divided dosages for her psychotic symptoms, while continuing eszopiclone with promethazine 25 mg nocte. The patient was advised to follow up after a week. The repeat challenge with aripiprazole 20 mg orally in two divided dosages resulted into oculogyric crisis within 4 days. This was again successfully treated with intramuscular promethazine. The patient was advised cap ziprasidone 20 mg orally in two divided doses per day (i.e., 40 mg per day) with food and was asked to follow up 2 weeks later with electrocardiogram done. Later uptitration of cap ziprasidone to 20 mg orally in three divided doses per day (i.e., 60 mg per day) with food was done. She improved in her psychotic symptoms over 2 months with no extrapyramidal symptoms, normal electrocardiogram, and other baseline investigations.
DISCUSSION
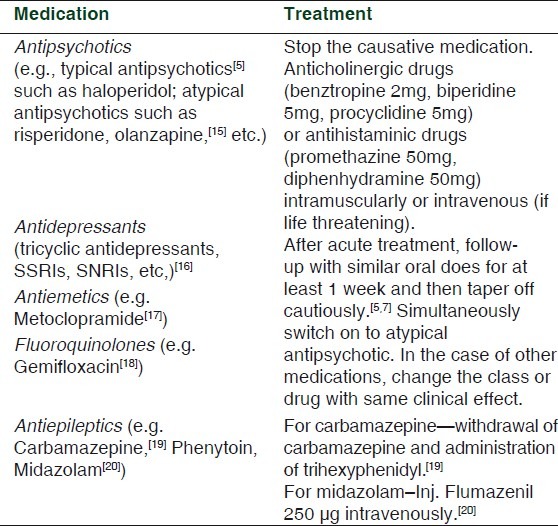
Various case reports of aripiprazole-induced acute dystonia report symptoms of neck extension, torticollis, rigidity, and tongue movements.[8–10] In addition, various studies describe medications causing acute dystonic reactions and their management which are described in the Table 1. Case reports of acute dystonic reactions in patients on medications such as antimalarials (chloroquinone, hydroxychloroquine, and amodiaquine[11], antivertigo agents (cinnarizine, and flunarizine), cocaine, buspirone, diazepam, sumatriptan, phenylpropanolamine, and ecstasy (3,4-methylenedioxymethamphetamine) have also been reported.[7]
Table 1.
Drugs causing acute dystonia and its management
In this case, oculogyric crisis is the symptom of attention. This case, a female patient on third generation antipsychotic medicine (aripiprazole) has least propensity for dystonia.[1–3] The risk factor for developing acute dystonia in this case is history of acute dystonia.[7]
Acute dystonia occurred after 5 days on increasing aripiprazole from 10 mg to 20 mg per day orally in two divided dosage. It regressed completely with stopping of aripiprazole and administration of promethazine. On repeat challenge it reappeared with the same severity. Hence, on causality assessment scale by Naranjo et al., the score is 7. This clearly depicts probable association of oculogyric crisis with aripiprazole.[12,13]
Numerous studies report mechanisms of acute dystonia being dopamine hypofunction resulting in a relative overactivity of cholinergic mechanisms. Since aripiprazole lacks protective anticholinergic action, it can have a potential to precipitate dystonia. This was supported by the fact that, in this case, dystonia resolved with promethazine (an antihistaminic with anticholinergic property). In addition, aripiprazole's action on the D3 receptor and antagonism of 5-HT6 and 5-HT7 receptors is still unknown and hence it may play a role in oculogyric crisis. Preclinical studies found that inhibitory action of aripiprazole on the serotonin transporter, which may have a potential to alter the dopamine balance in the basal ganglia region. Studies mention paradoxical dopaminergic hyperfunction by either preferentially blocking presynaptic receptors or exposing the postsynaptic receptors to the natural release of dopamine from the presynaptic terminals as the DBA levels drop which may result in dystonia.[9,14]
Oculogyric crisis in this case was treated and then prevented by promethazine. This justifies the judicious use of medications for treatment and prophylaxis of acute dystonia due to antipsychotics. This case outlines a significant side effect of aripiprazole, which a practitioner should be vigilant about before initiating the medication.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Stahl SM. Dopamine system stabilizers, Aripiprazole and next generation antipsychotics part 1, “Goldilocks” action at dopamine receptors. J Clin Psychiatry. 2001;62:841–2. doi: 10.4088/jcp.v62n1101. [DOI] [PubMed] [Google Scholar]
- 2.Burris KD, Molski TF, Xu C, Ryan E, Tottori K, Kikuchi T, et al. Aripiprazole, a Novel Antipsychotic, Is a High-Affinity Partial Agonist at Human Dopamine D2 Receptors. J Pharmacol Exp Ther. 2002;302:381–9. doi: 10.1124/jpet.102.033175. [DOI] [PubMed] [Google Scholar]
- 3.Ozdemir V, Fourie J, Ozdener F. Aripi-prazole (Otsuka Pharmaceutical Co) Curr Opin Investig Drugs. 2002;3:113–20. [PubMed] [Google Scholar]
- 4.Sarin A, Nagpal J, Bohra NK, Jiloha RC, Rao GP, Sharma SK, et al. Open labeled, randomized, switch over study of two fixed doses (10/15 mg) of aripiprazole: To evaluate its safety and efficacy in Indian patients of schizophrenia. Indian J Psychiatry. 2004;46:64–71. [PMC free article] [PubMed] [Google Scholar]
- 5.Rich SS. Drug induced movement disorders. Rhode Island Med. 1993;76:556–62. [PubMed] [Google Scholar]
- 6.American Psychiatric Association Diagnostic and Statistical Manual of mental disorders. 4th ed. Washington DC: American Psychiatric Association; 2000. [Google Scholar]
- 7.van Harten P N, Hoek HW, Kahn RS. Acute dystonia induced by drug treatment. BMJ. 1999;319:623–6. doi: 10.1136/bmj.319.7210.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sanghadia M, Pinninti NR. Aripiprazole associated acute dystonia. J Neuropsychiatry Clin Neurosci. 2007;19:89–90. doi: 10.1176/jnp.2007.19.1.89. [DOI] [PubMed] [Google Scholar]
- 9.Desarkar P, Thakur A, Sinha VK. Aripiprazole induced acute dystonia. Am J Psychiatry. 2006;163:1112–3. doi: 10.1176/ajp.2006.163.6.1112a. [DOI] [PubMed] [Google Scholar]
- 10.Zacher JL, Hatchett AD. Aripiprazole induced movement disorder. Am J Psychiatry. 2006;163:160–1. doi: 10.1176/appi.ajp.163.1.160-a. [DOI] [PubMed] [Google Scholar]
- 11.Fajolu IB, Lesi FE. Drug-induced acute dystonia in a 7 year old child following the use of artesunate-amodiaquine: A case report. Int J Risk Saf Med. 2010;22:111–4. [Google Scholar]
- 12.Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–45. doi: 10.1038/clpt.1981.154. [DOI] [PubMed] [Google Scholar]
- 13.Holloway K, Green T. Drug and therapeutics committees: A practical guide. Geneva: World Health Organization; 2003. pp. 62–70. [Google Scholar]
- 14.Sethi KD. Movement disorders induced by dopamine blocking agents. Semin Neurol. 2001;21:59–68. doi: 10.1055/s-2001-13120. [DOI] [PubMed] [Google Scholar]
- 15.Mendhekar DN. Recurrent oculogyric crisis and retrocollis after re exposure with a low dose of olanzapine. Indian J Pharmocol. 2005;37:337. [Google Scholar]
- 16.Madhusoodanan S, Alexeenko L, Sanders R, Brenner R. Extrapyramidal symptoms associated with antidepressants-A review of the literature and an analysis of spontaneous reports. Ann Clin Psychiatry. 2010;22:148–56. [PubMed] [Google Scholar]
- 17.İncecik, Metoclopramide induced acute dystonic reaction: Two case reports. Marmara Med J. 2008;21:159–61. [Google Scholar]
- 18.Sharma DD, Aggarwal A, Sharma RC, Kumar R. A Probable association of acute dystonia with gemifloxacin administration. Indian J Med Sci. 2009;63:557–60. [PubMed] [Google Scholar]
- 19.Fadare JO, Owolabi LF. Carbamazepine-induced dystonia: A case report. Neurol Asia. 2009;14:165–6. [Google Scholar]
- 20.Stolarek IH, Ford MJ. Acute dystonia induced by midazolam and abolished by flumazenil. BMJ. 1990;300:614. doi: 10.1136/bmj.300.6724.614. [DOI] [PMC free article] [PubMed] [Google Scholar]