

Abstract
Takotsubo cardiomyopathy (TC) was initially recognized in Japan in 1990. The typical patient is a postmenopausal woman with symptoms that mimic an acute coronary syndrome generally following physical or emotional stress. The EKG will typically have dynamic ST segment changes, while the angiogram will usually show normal coronary arteries. In classic TC, the left ventriculogram typically shows akinesis and ballooning of the apex with a normal or hyperdynamic base. Several variants of TC have been described. In this case report, we describe a midventricular variant of TC in a 64-year-old Hispanic female. The patient had chest pain, shortness of breath, elevated cardiac enzymes, and ST-segment elevations in leads II, aVF, and V5-V6. Coronary angiography revealed normal coronary arteries. Left ventriculogram showed hypokinesis of the midventricular segment and hyperdynamic apical and basal regions. Although the exact mechanism of TC is unknown, several theories include loss of estrogen, catecholamine or neurohumoral stimulation, coronary artery spasm, and left ventricular outflow tract (LVOT) obstruction.
Keywords: Takotsubo cardiomyopathy, mid-ventricular variant, broken-heart syndrome


Introduction
Takotsubo cardiomyopathy (TC) was first described in Japan in 1990.1 Takotsubo in Japanese means octopus trap. The trap has a narrow neck and round bottom that resembles the heart shape in TC. TC is also known as stress-induced or broken-heart syndrome since it is commonly seen after a stressful event. It usually affects postmenopausal women between ages 58–75.2 Clinical features of this syndrome mimic those of an acute coronary syndrome, namely chest pain, dyspnea, ST-T changes with or without a prolonged QT interval, and mild elevations of cardiac enzymes.2-4 On angiography patients will have normal-appearing coronary arteries. Left ventriculogram will show wall motion abnormalities, which is the basis in defining the different variants. 2
Case Report
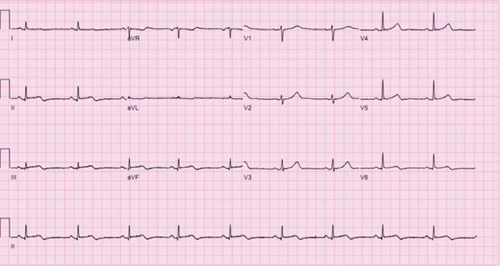
We report a case of a 64-year-old Hispanic female with a significant past medical history of hypertension, hyperlipidemia, depression, and gastroesophageal reflux disease who presented to the emergency room with intermittent substernal chest pain that began about an hour after having an argument with her son. Troponin was 7.69 and creatine kinase-MB was 39.7 on admission. Electrocardiography (EKG) showed ST-segment elevations in leads II, III, aVF, V5, and V6 that were consistent with acute ischemia (Figure 1). Her coronary angiogram revealed normal coronary arteries. Left ventriculogram showed hypokinesis of the midventricular section with a hyperdynamic base and apex (Figures 2 and 3). Cardiac magnetic resonance imaging showed mild hypokinesis of the midinferior and lateral walls and a left ventricular ejection fraction of 70%. The following day, the patient also had a prolonged QTc of 478 ms, which is commonly seen in patients with nonapical TC.5 The patient was treated with an aspirin, statin, beta blocker, and angiotensin converting enzyme inhibitor. The next day, the patient had sinus bradycardia that was probably secondary to the beta blocker. By day two the patient improved clinically and the acute ischemic changes on EKG had resolved (Figure 4).
Figure 1.
EKG on initial presentation. ST-segment elevations in leads II, III, aVF, V5, and V6. QTc is prolonged (478 ms).
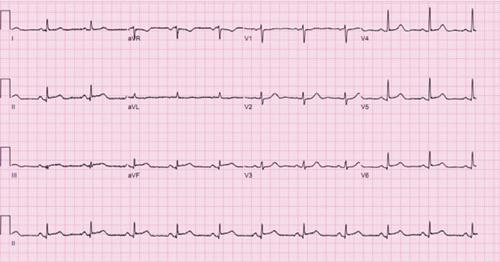
Figure 2.
Left ventriculogram during systole.

Figure 3.
Left ventriculogram during diastole.
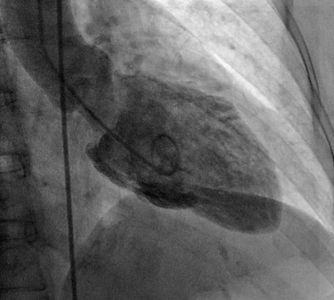
Figure 4.
EKG on day 2 of admission. ST-segment elevations resolved. QTc interval is 443 ms.
Discussion
Typical and Atypical Takotsubo Cardiomyopathy
Typical or classic TC is much more common than the atypical variants. It is characterized by transient apical hypokinesis and basal hyperkinesis.3, 4 Several variants of TC have been described. In reverse or inverted TC, the apex is hyperdynamic and the base is akinetic.6 The midventricular type is characterized by akinesis with or without ballooning of the midventricular segment and a hyperdynamic base and apex.7-11 Akinesis of other LV and RV segments have also been described.3, 12 Patients may also have repeated episodes of TC manifesting in the classic and atypical forms.11, 13, 14
Pathophysiology
Although the pathophysiology of TC is still not well established, a few theories have been proposed. Emotional or physical stress is considered to be a trigger. Since the syndrome is more commonly seen in postmenopausal women, estrogen may play a role.2, 4, 5, 15-17 Other proposed mechanisms are elevated catecholamines that cause cardiotoxicity and coronary artery spasm, which lead to myocardial stunning.3-5, 15, 17
Role of Estrogen
Estrogen is thought to promote vasodilation through endothelial nitric oxide synthase.5 Postmenopausal women lose this protective effect, which may predispose them to coronary spasm and myocardial stunning in the setting of elevated catecholamine levels.3, 5
Catecholamines and Neurohumoral Stimulation
Excessive stress-induced catecholamines in TC may share a similar mechanism with pheochromocytoma, which likewise can result in myocardial dysfunction. Its pathogenesis may be similar to intracranial hemorrhage, which results in neurally mediated myocardial dysfunction.4, 18
Coronary Artery Spasm
Coronary spasm with resultant myocardial stunning has been noted in TC and has been postulated as a mechanism.2-5, 15, 17 However, this has not been a consistent finding.
LVOT Obstruction
Another theory is that LVOT obstruction results in Takotsubo cardiomyopathy. During stressful situations, the increase in catecholamines may cause LVOT obstruction that leads to ischemia, in turn causing regional wall motion abnormalities and release of cardiac enzymes.17
Variable Distribution of Wall Motion Abnormalities
There may be a difference in density of cardiac adrenoceptors in the mid and apical portions, giving rise to the typical TC.5 Moreover, it has been postulated that typical TC is more common in postmenopausal women since there is a higher concentration of adrenoceptors at the apex than the base.19 Alternatively, regional wall motion abnormalities could be due to local release of catecholamines or to greater autonomic innervation of the LV anterior wall when compared to the apex and inferior wall.20 In addition, different variants have been described in the same patient, which may be due to differences in stress, catecholamine levels, and adrenergic receptor sensitivity.4, 11, 21
Clinical Features and Prognosis in Takotsubo Variants
The clinical features of classical TC differ from the variants. Compared with the variants, patients with classical TC tend to be older and have more ST-segment elevation, a lower ejection fraction, higher cardiac enzymes and a greater incidence of cardiogenic shock.3, 15, 19 Treatment is supportive to allow recovery of heart function. It should be emphasized that hospital mortality in classical TC and its variants is low, and heart function usually starts recovering in a few days.3 Although TC has been known to recur (sometimes as a different variant), this is not common.
Conclusion
TC has several variants, but all present in a similar fashion in which the clinical features, lab, and EKG abnormalities resemble an acute coronary syndrome. TC and its variants are categorized by the regional wall motion abnormalities noted. Although TC generally has a good outcome, classic TC is more likely to present with ST-segment elevation in multiple leads and cardiogenic shock.3, 15 Although the exact mechanism is unknown, several theories include loss of estrogen, catecholamine excess, neurohumoral stimulation, coronary artery spasm, and LVOT obstruction.3-5, 15, 17
Conflict of Interest Disclosure: All authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Funding/Support: The authors have no funding disclosures.
Contributor Information
Pradnya Velankar, Methodist DeBakey Heart & Vascular Center, Houston, Texas
John Buergler, Methodist DeBakey Heart & Vascular Center, Houston, Texas
References
- 1.Sato H, Tateisha H, Uchida T. Takotsubo-type cardiomyopathy due to multivessel spasm. In: Kodama K Haze K, Hon M, editors. Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure (in Japanese). Tokyo: Kagakuhyouronsya; 1990. p. 56-64. [Google Scholar]
- 2.Takotsubo cardiomyopathy (broken-heart syndrome). Harv Womens Health Watch. 2010 Nov;18(3):6–7. [PubMed] [Google Scholar]
- 3.Zeb M, Sambu N, Scott P, Curzen N. Takotsubo cardiomyopathy: a diagnostic challenge. Postgrad Med J. 2011 Jan;87(1023):51–9. doi: 10.1136/pgmj.2010.102475. [DOI] [PubMed] [Google Scholar]
- 4.Lee YP, Poh KK, Lee CH, Tan HC, Rakak A, Chia BL, et al. Diverse clinical spectrum of stress-induced cardiomyopathy. Int J Cardiol. 2009 Apr 3;133(2):272–5. doi: 10.1016/j.ijcard.2007.11.039. [DOI] [PubMed] [Google Scholar]
- 5.Balkin DM, Cohen LS. Takotsubo Syndrome. Coron Art Dis. 2011 May;22(3):206–14. doi: 10.1097/MCA.0b013e328342532c. [DOI] [PubMed] [Google Scholar]
- 6.Caccioti L, Camastra GS, Musarò S, Proietti I, Semeraro R, Martina C, et al. Stress cardiomyopathy: transient basal ballooning. J Cardiovasc Med (Hagerstown). 2010 Oct;11(10):764–7. doi: 10.2459/JCM.0b013e328334466c. [DOI] [PubMed] [Google Scholar]
- 7.Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, et al. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest. 2007 Sep;132(3):809–16. doi: 10.1378/chest.07-0608. [DOI] [PubMed] [Google Scholar]
- 8.Cacciotti L, Camastra GS, Beni S, Giannantoni P, Musarò S, Proietti I, et al. A new variant in Tako-tsubo cardiomyopathy: transient mid-ventricular ballooning. J Cardiovasc Med. 2007 Dec;8(12):1052–4. doi: 10.2459/JCM.0b013e32803cab4a. [DOI] [PubMed] [Google Scholar]
- 9.Fazio G, Novo G, Azzarelli S, Evola S, Barbaro G, Sutera L, et al. Transient mid-ventricular dyskinesia: a variant of Takotsubo syndrome. Int J Cardiol. 2008 Sep 26;129(2):272–3. doi: 10.1016/j.ijcard.2007.07.155. [DOI] [PubMed] [Google Scholar]
- 10.Gerbaud E, Jaussaud J, Lederlin M, Reant P. Transient left ventricular non-apical ballooning syndrome: Diagnosis with multiple imaging modalities. Arch Cardiovasc Dis. 2010 Apr;103(4):270–2. doi: 10.1016/j.acvd.2009.08.013. [DOI] [PubMed] [Google Scholar]
- 11.Mansencal N, Mahmoud RE, Pillière R, Dubourg O. Relationship between pattern of Tako-Tsubo cardiomyopathy and age: from midventricular to apical ballooning syndrome. Int J Cardiol. 2010 Jan 7;138(1):e18–20. doi: 10.1016/j.ijcard.2008.06.009. [DOI] [PubMed] [Google Scholar]
- 12.Eitel I, Schuler G, Gutberlet M, Thiele H. Biventricular stress-induced (takotsubo) cardiomyopathy with left midventricular and right apical ballooning. Int J Cardiol. 2011 Sep 1;151(2):e63–4. doi: 10.1016/j.ijcard.2010.05.017. [DOI] [PubMed] [Google Scholar]
- 13.Koeth O, Mark B, Zahn R, Zeymer U. Midventricular form of takotsubo cardiomyopathy as a recurrence 1 year after typical apical ballooning: a case report. Cases J. 2008 Nov 19;1(1):331.. doi: 10.1186/1757-1626-1-331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wever-Pinzon O, Wever-Pinzon J, Tami L. Recurrent Takotsubo cardiomyopathy presenting with different morphologic patterns. Int J Cardiol. 2011 May 5;148(3):379–81. doi: 10.1016/j.ijcard.2010.10.091. [DOI] [PubMed] [Google Scholar]
- 15.Jabara R, Gadesam R, Pendyala L, Chronos N, King SB, Chen JP. Comparison of the clinical characteristics of apical and non-apical variants of broken heart (takotsubo) syndrome in the United States. J Invasive Cardiol. 2009 May;21(5):216–22. [PubMed] [Google Scholar]
- 16.Ueyama T, Ishikura F, Matsuda A, Asanuma T, Ueda K, Ichinose M, et al. Chronic estrogen supplementation following ovariectomy improves the emotional stress-induced cardiovascular responses by indirect action on the nervous system and by direct action on the heart. Circ J. 2007 Apr;71(4):565–73. doi: 10.1253/circj.71.565. [DOI] [PubMed] [Google Scholar]
- 17.Fang CC, Jao YT, Yi-Chen Y, Yu CL, Chen CL, Wang SP. Transient left ventricular apical ballooning syndrome: the first series in Taiwanese patients. Angiology. 2008 Apr-May;59(2):185–92. doi: 10.1177/0003319707305463. [DOI] [PubMed] [Google Scholar]
- 18.Kurisu S, Sato H, Kawagoe T, Ishihara M, Shimatani Y, Nishioka K, et al. Tako-tsubo-like left ventricular dysfunction with ST-segment elevation: a novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002 Mar;143(3):448–55. doi: 10.1067/mhj.2002.120403. [DOI] [PubMed] [Google Scholar]
- 19.Ramaraj R, Movahed MR. Reverse or inverted takotsubo cardiomyopathy (reverse left ventricular apical ballooning syndrome) presents at a younger age compared with the mid or apical variant and is always associated with triggering stress. Congest Heart Fail. 2010 Nov-Dec;16(6):284–6. doi: 10.1111/j.1751-7133.2010.00188.x. [DOI] [PubMed] [Google Scholar]
- 20.Singh NK, Rumman S, Mikell FL, Nallamothu N, Rangaswamy C. Stress cardiomyopathy: clinical and ventriculographic characteristics in 107 North American subjects. Int J Cardiol. 2010 Jun 11;141(3):297–303. doi: 10.1016/j.ijcard.2008.12.043. [DOI] [PubMed] [Google Scholar]
- 21.Yoshida T, Nishizawa T, Yajima K, Tsuruoka M, Fajimaki T, Oguri M, et al. A rare case of tako-tusbo cardiomyopathy with variable forms of left ventricular dysfunction: a new entity. Int J Cardiol. 2009 May 15;134(2):e73–5. doi: 10.1016/j.ijcard.2007.12.092. [DOI] [PubMed] [Google Scholar]