

Abstract
Background and purpose
Ilizarov’s technique and intramedullary rodding have often been used individually in congenital pseudarthrosis of the tibia. In this series, we attempted to combine the advantages of both methods while minimizing the complications.
Methods
We reviewed 15 cases of congenital pseudoarthrosis of the tibia (CPT) who were treated with a combination of Ilizarov’s apparatus and antegrade intramedullary nailing between 2003 and 2008. The mean age at surgery was 7.5 (3–12) years and the mean limb length discrepancy was 2.5 (1.5–5) cm. At a mean follow-up time of 4.5 (1.6–7.2) years after the index surgery, the patients were evaluated clinically and radiographically for ankle function (AOFAS score) and for malalignment, signs of union, limb length discrepancy, and complications.
Results
14 patients achieved union, in 6 patients primary union and in 8 patients after secondary procedures. The AOFAS score improved from a preoperative mean of 40 (20–57) to 64 (47–75). The main complication was refracture in 1 patient, and non-union in 1 patient.
Interpretation
The combination of the Ilizarov technique and conventional antegrade intramedullary nailing was successful in achieving union with few complications, though this should be shown in long-term studies lasting until skeletal maturity.
Congenital pseudarthrosis of the tibia (CPT), also called congenital tibial dysplasia, is difficult to treat with a substantial risk of non-union, refractures, leg length discrepancy (LLD), and malalignment of the tibia and the ankle (Plawecki et al. 1990, Paley et al. 1992). Treatment procedures can be broadly classified into 3 groups: (1) Intramedullary rodding (usually trans-ankle) with bone grafting (Johnston 2002, Dobbs et al. 2004), (2) microvascular fibular transfer (Ohnishi et al. 2005), and (3) the Ilizarov technique with its various modifications (Paley et al. 1992, Boero et al. 1997, Johnston and Birch 2008). However, no single treatment has been shown to be uniformly effective.
Intramedullary rodding, usually retrograde through the calcaneum to the tibia, has been used relatively widely with success in achieving union and protection against refracture (Johnston 2002, Shah et al. 2011). However, concerns still exist about ankle stiffness and arthritic changes in the ankle following the nailing (Dobbs et al. 2005). On the other hand, various series using the Ilizarov technique have shown high union rates with good ankle function (Paley et al. 1992, Boero et al. 1997). However, there is a risk of refracture with this technique. We therefore wanted to make use of the advantages of both techniques. We have found only 1 report on this combined method (Mathieu et al. 2008) involving 10 cases.
We report the clinico-radiographical outcomes of 15 patients with CPT who were treated with a combination of the Ilizarov technique and intramedullary rodding.
Patients and methods
We retrospectively analyzed all 15 patients (10 males) with CPT who had been treated at our institute using a combination of Ilizarov’s technique and intramedullary rodding between 2003 and 2008, after receiving institutional review board approval. Mean age at presentation was 6 (3–12) years and mean age at surgery was 7.5 (4.5–12) years. The right side was involved in 10 patients and none had bilateral involvement. According to Boyd’s classification (Boyd 1982), 12 were type I and 3 were type II. Signs of neurofibromatosis could be confirmed in 7 patients. Detailed preoperative clinical examination was performed, which included knee and ankle range of motion, limb length discrepancy, operative scars, limb alignment, and functional evaluation using the validated AOFAS score (Kitaoka and Patzer 1997). The mean preoperative LLD of the patients was 2.5 (1.5–5) cm. 7 patients had undergone surgery prior to our combination treatment, without success (Table 1).
Table 1.
Demographics of the patients with congenital pseudoarthrosis of the tibia who were treated with combination of Ilizarov apparatus and intramedullary nailing
| A | B | C | D | E | F | G | H | I | J | K | L | M |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | L | M | 5 | 6 | 5 | 50 | I | N | 40 | 65 | 1.5 | 1 |
| 2 | R | F | 5 | 7 | 8 | 75 | II | N | 57 | 70 | 2 | 1 |
| 3 | L | M | 7 | 7 | 3 | 38 | I | Y | 30 | 65 | 4 | 3.2 |
| 4 | R | M | 3.5 | 5 | 4.5 | 40 | I | N | 48 | 60 | 2 | 1 |
| 5 | R | F | 7.5 | 7.5 | 3.5 | 44 | I | Y | 44 | 70 | 5 | 3 |
| 6 | R | M | 12 | 12 | 5 | 65 | II | Y | 20 | 60 | 2.5 | 2 |
| 7 | R | M | 3 | 5 | 6 | 50 | I | N | 54 | 65 | 1.5 | 1.5 |
| 8 | L | M | 4.5 | 8 | 9.5 | 72 | I | N | 30 | 65 | 2 | 2 |
| 9 | R | F | 6 | 9 | 4 | 18 | I | Y | 30 | 58 | 2 | 1 |
| 10 | R | M | 5 | 9 | 8 | 50 | I | N | 44 | 66 | 2 | 1.6 |
| 11 | L | M | 7 | 7 | 3 | 40 | II | Y | 35 | 65 | 2.5 | 1.5 |
| 12 | R | F | 7.5 | 9 | 8.5 | 88 | I | Y | 30 | 55 | 2 | 2 |
| 13 | L | M | 4.5 | 4.5 | 3.5 | 46 | I | Y | 44 | 75 | 2.5 | 2 |
| 14 | R | F | 6 | 8 | 6 | 50 | I | Y | 38 | 47 | 2.5 | 1.9 |
| 15 | R | M | 5 | 6 | 5 | 54 | I | N | 56 | 75 | 1.5 | 1.5 |
A No
B Side
C Sex
D Age at presentation (years)
E Age at surgery (years)
F Follow-up from presentation (years)
G Follow-up from index surgery (months)
H Boyd classification
I Previous surgery
J AOFAS score preoperatively
K AOFAS score postoperatively
L Pre-op LLD (cm)
M LLD at final follow-up (cm)
Operative procedure
All surgeries were performed by one senior surgeon (HRS). The patients were operated keeping in mind some basic principles: i.e. excision of the pseudoarthrosis with the abnormal periosteum and surrounding tissues, removal of the dead and sclerotic bone ends until bleeding ends appear, and bone grafting in the intervening space. 1 flexible titanium elastic nail (10 patients) or 2 of them (5 patients) were inserted by the antegrade method through the proximal tibia, passed through the “fracture” until the level of the ankle. The decision to pass 1 or 2 intramedullary nails depended on the diameter of the intramedullary canal at the thinnest region. The configuration for a single nail was a linear one with entry at the center of the anterior corner of the knee, while double nails were used in a spindle manner. A close watch was kept over the axial alignment throughout this procedure. The sclerotic portion of the fibula, if present, was dealt with similarly and retrograde intramedullary nailing was performed from the lateral malleolus in 2 patients.
The Ilizarov frame was then mounted. The decision to apply the external fixator in compression mode or in bone transport mode was taken with respect to the limb length discrepancy. If the limb length discrepancy was less than 2.5 cm, we used compression at the pseudoarthrotic site while if it was more than 2.5 cm or when there was a lot of fibrosis around the pseudoarthrosis due to previous surgery, a proximal corticotomy was performed with bone transport in order to prevent further LLD. Usually, 2 rings proximally and 1 ring distally were applied in the compression mode.
Bone transport (when needed) was started after 7 days of surgery at the rate of 1 mm/day. The patient was taught pin-tract care and partial weight bearing. Physiotherapy with active and passive motion of the knee and ankle, and resting of the foot in shoes attached by elastic bands to the Ilizarov apparatus were advised to prevent joint contracture. The patients were followed every 15 days for the first 3 months, every month for the next 3 months, and then every 3 months until clinico-radiographic union was obtained. The Ilizarov fixator was removed after radiographs had shown corticalization of at least 3 cortices, seen in radiographs taken in 2 planes. Long leg cast was applied for 6 weeks, after which an above-the-knee anteroposterior orthosis was recommended for continuous use until skeletal maturity. The patients required a nail exchange procedure every four years approximately until skeletal maturity.
Evaluation
At final follow-up, patients were evaluated for union, knee and ankle motion, and limb length discrepancy. Union was labeled as being “primary” when it united after the present surgery without any need for secondary surgeries (excluding external fixator removal and casting or change of wire, which was done under general anesthesia in some patients) and secondary when additional surgery was required to obtain union.
The lengthening at the upper tibial osteotomy site, the evaluation of the distal pseudarthrotic site, status of union, external fixator index, and the healing index were calculated using radiographs. The external fixation index (EFI) was calculated as the time for which the external fixator was applied divided by the length of bone gained (days per cm). The healing index (HI) was defined as the time required for 1 cm of the bone to fully consolidate, and was calculated by dividing the total length of time in days the fixator was applied by the total amount of distraction performed.
The need for additional procedures to achieve union was noted. Complications were categorized as minor or major. Minor complications were defined as being those complications or adverse effects that did not require any additional surgery or those that required only minor surgeries. Major complications were defined as being those that required complex surgeries for correction and those that adversely affected the final surgical outcome.
The results were classified as good, fair, or poor based on the presence or absence of these minor or major complications. A good result meant no or only minor complications that could be treated non-surgically, a fair result meant the presence of 1 or more minor complications that had to be treated surgically or the presence of a major complication after which the final surgical goal could be still achieved, and a poor result meant the presence of 1 or more major complications because of which the final surgical goal could not be achieved.
Statistics
A difference between preoperative AOFAS score and postoperative AOFAS score (at last follow-up) was evaluated using the Student t-test and the difference between the 2 treatment groups was calculated using the independent-samples t-test. Any p-value of < 0.05 was taken as being significant.
Results
The patients were divided into 2 groups: group I had had no surgery performed prior to the index surgery and group II included those patients in whom 1 or more operations had been performed prior to the index operation. Group I included 7 patients with a mean age at index surgery of 6.5 years while group II included 8 patients with a mean age at surgery of 8 years. The 2 groups were compared with each other regarding the union obtained (primary or secondary), limb alignment, and AOFAS scores (Tables 1 and 2).
Table 2.
Patient-related data in the two groups. In group I, no surgery had been performed prior to index surgery and in group II one or more operations had been performed before the index surgery
| Group I | Group II | |
|---|---|---|
| Previous surgery | No | Yes |
| No. of patients | 7 | 8 |
| Boyd classification | ||
| type I | 6 | 6 |
| type II | 1 | 2 |
| Average age at presentation, years | 4.4 | 7.2 |
| Average age at index surgery, years | 6.5 | 8.0 |
| Average age at final follow-up, years | 11 | 12 |
| Average follow-up, months | 55 | 47 |
| Union | ||
| primary | 6 | 0 |
| secondary | 1 | 7 |
| non-union | 0 | 1 |
| AOFAS score preoperatively | 47 | 34 |
| AOFAS score postoperatively | 67 | 62 |
Union
The patients were evaluated at a mean follow-up time of 4.5 (1.6–7.2) years after the index operation. Tibial union was achieved in 14 of the 15 cases, with primary union in 6 cases and secondary union in 8 (Figure 1). All but 1 of 7 patients in group I had primary union while the remaining patient required bone grafting for union. In group II, all the patients required additional bone grafting, which led to union in 7 of the 8 patients.
Figure 1.
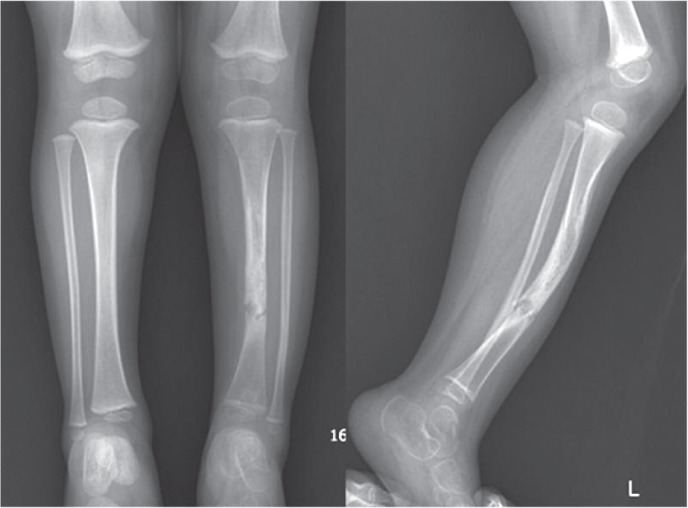

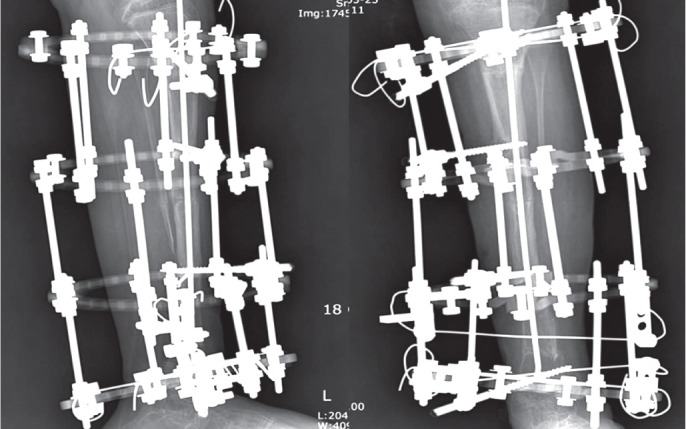
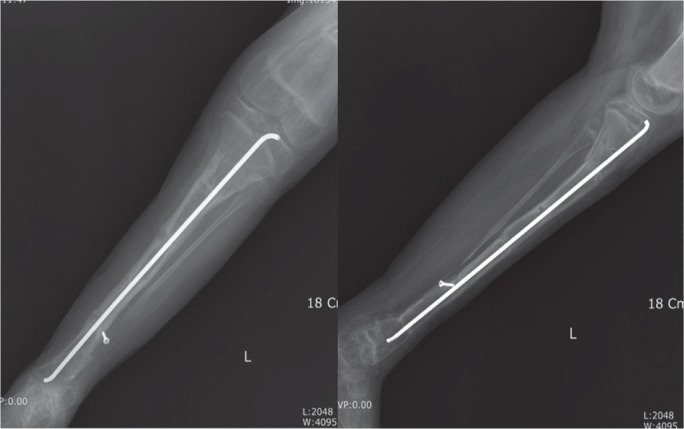
A. Anteroposterior and lateral radiographs from a 6-year-old boy with Boyd type-I congenital pseudoarthrosis of the tibia. B. Anteroposterior and lateral radiograph of the same patient who was operated elsewhere with attempted four-in-one fusion. At presentation, the child had minimal discharge of pus over the lateral fibular non-union, and had abnormal mobility at the distal third of the tibia. [OK???] Radiographs showed persistent non-union and 40° valgus deformity. C. Anteroposterior and lateral radiographs of the child after excision of sclerotic bone ends, antegrade nailing, and application of the Ilizarov method. D. Anteroposterior and lateral radiographs of the child 2 years after surgery, showing well-united tibia with acceptable axial alignment.
The mean time to primary union was 5.6 (4–8) months and for secondary union it was 11 (8–13) months. The average duration of Ilizarov treatment was 6 (4–7) months for primary union and 9 (7–10) months for secondary union. The average amount of lengthening/bone transport performed was 3.8 (2.6–4.5) cm, with a mean postoperative limb length discrepancy of 1.9 (1–3.2) cm. The mean EFI was 39 (32–58) days/cm while the mean HI was 64 (41–85) days/cm.
Limb alignment and status of fibula
There was persistent non-union with proximal migration of the distal fibula seen in 7 patients (Figure 1). This was seen in patients in group II in whom bone transport had been performed. All 7 patients had resultant tibial valgus malalignment (mean 10° (5–25)). Angulations of less than 5° were accepted while more severe valgus malalignments required surgical correction. Thus, 5 of these patients had a minor amount of valgus angulation while 2 patients had malalignments of 20° and 25°, which required corrective osteotomy and refixation. One of them had a proximal angulation and was treated with a tibial corrective osteotomy and renailing, while the other had a distal third valgus deformity with severe ankle valgus. A supramalleolar osteotomy with Ilizarov application was performed, with good results.
Knee and ankle motion
All the patients required vigorous physiotherapy before and after frame removal to achieve good range of motion in the knee and ankle. 15° of knee flexion contracture was seen in 2 patients immediately after frame removal, but it could be corrected by prolonged physiotherapy. The other patients had full knee motion. Ankle stiffness occurred in 3 patients who required multiple operations for attainment of union and who had relatively distal pseudoarthrosis. The other patients had normal ankle motion.
Grading of results and AOFAS scores
6 patients had a good result, 8 patients had a fair one, and 1 patient had a poor result. All the patients who had achieved primary union and 4 of the remaining 8 patients who had achieved secondary union could walk without pain with an orthosis. The remaining 4 patients who had achieved secondary union could walk with mild to moderate pain, while the 1 patient in whom union was not achieved could not walk.
The mean pretreatment AOFAS score for all 15 patients was 40 (SD 11), which increased to 64 (SD 7) at the time of the last follow-up (p ≤ 0.001). The patients in group I (those not previously operated) fared better than those in group II, with the AOFAS score increasing from 47 (SD 10) preoperatively to 67 (SD 5) at the last follow-up (p = 0.03). As expected, the patients in group II had a lower AOFAS score before surgery, 34 (SD 8), which increased to 62 (SD 9) after surgery (p = 0.001).
Complications
There were 12 major complications in 8 patients and 22 minor complications in 15 patients (Table 3). Of the major complications, the commonest was delayed consolidation: in 7 of the pseudarthrotic patients and in 1 patient regarding the bone transport site. Bone grafting was required in all 8 patients, although additional procedures were also required in 5 of them. Of these 8 patients, 7 had also been operated before the index operation. The previous procedures were intramedullary rodding and contralateral tibial bone grafting in 4 and Ilizarov surgery in 3. Ipsilateral autogenous iliac crest bone grafting was enough to obtain union in 6 patients, while 2 patients required additional demineralized bone matrix (DBM) and 1 of them required supplemental allogenous bone graft. 2 patients required additional plate fixation for added stability for bony union, 1 for the pseudarthrotic site (Figure 2) and another for the bone transport site. When done at the docking site, bone grafting was not done at the time of the acute docking, but was done later on, depending on the union at the site.
Table 3.
Complications and results for patients with congenital pseudoarthrosis of the tibia who were treated with Ilizarov technique and intramedullary nailing
| No | Minor complication | Treatment | Major complication | Treatment | Final outcome | Clinical grade |
|---|---|---|---|---|---|---|
| 1 | Pin-tract infection | Non-operative | – | – | Primary union | Good |
| Ankle stiffness | Non-operative | – | – | – | – | |
| 2 | Pin-tract infection | Non-operative | Delayed consolidation | Corrective osteotomy | Secondary union | Fair |
| Equinus | Non-operative | Valgus malalignment | with bone graft | – | – | |
| 3 | Pin-tract infection | Wire change | Delayed consolidation | – | Secondary union | Fair |
| 4 | Pin-tract infection | Non-operative | – | – | Primary union | Good |
| 5 | Pin-tract infection | Wire change | Delayed consolidation | Supramalleolar osteotomy | Secondary union with | Fair |
| Knee flexion contracture |
Non-operative | Valgus malalignment | with bone graft | good alignment | ||
| 6 | Pin-tract infection | Non-operative | – | Primary union | Good | |
| 7 | Pin-tract infection | Non-operative | Delayed consolidation | DBM application | Secondary union | Fair |
| Ankle stiffness | Non-operative | – | – | – | – | |
| 8 | Pin-tract infection | Non-operative | – | – | Primary union | Good |
| 9 | Pin-tract infection | Wire change | Delayed consolidation | Bone grafting with refixation | Secondary union | Fair |
| Knee flexion contracture |
Non-operative | – | – | – | – | |
| Equinus | Non-operative | – | – | – | – | |
| 10 | Pin-tract infection | Non-operative | – | Fair | ||
| 11 | Pin-tract infection | Non-operative | Delayed consolidation (bone transport) |
Bone grafting with plating | Secondary union | Fair |
| 12 | Pin-tract infection | Wire change | Delayed consolidation | Bone grafting with plating | Secondary union | Fair |
| Ankle stiffness | Non-operative | Refracture | ||||
| 13 | Pin-tract infection | Non-operative | – | – | Primary union | Good |
| 14 | Pin-tract infection | Removal of apparatus |
Non-union | Amputation advised | Non-union | Poor |
| 15 | Pin-tract infection | Non-operative | – | – | Primary union | Good |
Figure 2.

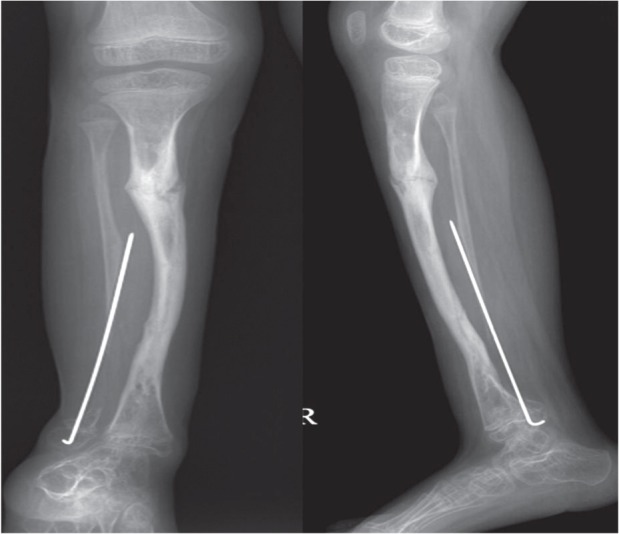
A. Anteroposterior and lateral radiographs from an 8-year-old boy with Boyd type-I congenital pseudoarthrosis of the tibia who was operated multiple times with Ilizarov apparatus and attempted four-in-one fusion. At presentation, the child had frank non-union with sclerotic bone ends with 2.5 cm shortening. B. Anteroposterior and lateral radiographs from the child after attempted Ilizarov fixation with intramedullary rodding. The intramedullary rod had to be removed due to infection, and there was severe ankle valgus.
Residual malalignment, a major complication, was seen in 2 patients who developed severe valgus deformity of the tibia along with signs of impending refracture of the pseudarthrotic site around 2 years after primary surgery. In 1 of these patients, the pseudoarthrosis was slightly proximal, and corrective tibial osteotomy with bone grafting and Ilizarov fixator was used with union and acceptable alignment. The other patient had a distal tibial pseudoarthrosis and required a supramalleolar osteotomy and refixation, along with Ilizarov technique with bone grafting to create union.
Refracture or impending refracture was seen in 1 patient 4 years after index surgery, after trivial trauma. The broken nail was removed, renailing and bone grafting was done, and the patient was kept in a cast for around 4 months postoperatively and obtained union.
Union could not be obtained in 1 patient (patient 7). This patient had already been operated several times at another hospital and presented to us with a very atrophic non-union with dead sclerotic bone ends. Freshening of bone ends, bone grafting with application of DBM, intramedullary nail insertion, and Ilizarov fixator application was performed. Unfortunately the patient developed severe pin-tract infection that progressed to deep intramedullary infection within a few days despite receiving antibiotic therapy. The Ilizarov apparatus and the intramedullary nail were removed after thorough debridement and the leg was put in a cast. Considering the severe intramedullary infection with non-union of the pseudoarthrotic site, amputation was advised. However, the patient and caregivers did not accept this and the patient was given a permanent protection orthosis. At the last follow-up, 1 year after the last surgery, the infection had healed but the non-union persisted.
The commonest minor complication was pin-tract infection, which was seen in all 15 patients, 10 had grade-I, 4 had grade-II and 1 patient had grade-III pin-tract infection according to the classification of Paley et al. (1990). Wires had to be changed or withdrawn in 5 patients with grade-II and grade-III infections. The patient who had the severe grade-III infection (patient 7) was treated with debridement and implant removal. Even after repeated surgeries, he did not achieve union until the end of the 4.2-year follow-up.
There were no other complications such as neurovascular compromise, peroneal nerve injury, or compartment syndrome in any patient.
Discussion
The treatment of CPT is controversial. Most series are small, non-comparative, and composed of heterogenous groups of patients (Choi et al. 2011).
Over the last few decades, intramedullary rodding with bone grafting and Ilizarov’s technique have emerged as the 2 most commonly used methods (Plawecki et al. 1990, Paley et al. 1992, Guidera et al. 1997, Grill et al. 2000, Ohnishi et al. 2005, Mathieu et al. 2008, Choi et al. 2011). The Ilizarov technique, first introduced in the western world in the 1980s, has been widely used for CPT and has gained acceptance in various centers (Choi et al. 2011). This method allows treatment of not only the pseudoarthrosis but also LLD, angular tibial abnormalities, proximal fibular migration, and foot contractures (Plawecki et al. 1990, Guidera et al. 1997). According to the multicenter study of the European Paediatric Orthopaedic Society (EPOS), the Ilizarov method has been found to be the gold standard for treatment of CPT (Grill et al. 2000).
The Ilizarov procedure is, however, associated with a high union rate, and also with a substantial refracture rate. In his series of 16 cases of pseudoarthrosis, Paley et al. (1992) reported on refractures in 5 patients after initial union. Inan et al. (2006) reported on 16 patients treated with Ilizarov. All the patients united but 10 patients had late axial malalignments and refractures. Cho et al. (2008) reported on 23 patients with atrophic type of CPT who were treated with Ilizarov’s technique. 20 of them suffered from refractures within 5 years of surgery.
The other important complication of the Ilizarov method is the late axial malalignment that may develop after radiographic union (Mathieu et al. 2008). In one of the earliest series, Ilizarov and Gracheva (1971) had axial malalignments in 5 of 16 patients who were treated by the method. Kristiansen et al. (2003) also noted similar rates of residual axial deformities. Our series has shown comparable results, with substantial symptomatic malalignments in 2 of 15 patients.
The relationship between these axial malalignments and refractures and the exact cause of refracture has been studied in great detail by several authors. Young age at surgery with a low cross-sectional area of the united segment of the pseudoarthrosis, ankle valgus due to fibular non-union, and non-compliance with bracing are all thought to cause refractures (Paley et al. 1992, Cho et al. 2008, Choi et al. 2011). However, we feel that there are only 3 important causes of refractures, namely (1) axial deviations leading to stress risers and fractures, (2) loss of intramedullary support after removal of nails, and (3) non-compliance with external bracing regimen. Insufficient resection of the pseudarthrotic site is in itself a poor prognostic factor, but usually the poor result is because of a non-united pseudarthosis rather than a refracture.
Thus, in our series we have added a supplemental antegrade intramedullary nail to support the bone as an internal splint. Though this nail cannot prevent the biological process of refracture, it still acts as an effective intramedullary strut to prevent further refracture. We obtained good solid union without refracture in 11 of 15 patients and only 1 patient suffered from refracture, which required refixation and additional bone grafting. This rate was similar to or better than that reported in most earlier series (Table 4).
Table 4.
Comparison of the present series with other series
| Author (year) | No. of patients |
Method used | Follow-up, years |
Delayed/ non-union |
Refracture | Malalignment | Amputation |
|---|---|---|---|---|---|---|---|
| Dobbs et al. (2004) | 21 | Intramedullary nailing, bone grafting | 14.2 | 3 | 12 | – | 5 |
| Cho et al. (2008) | 43 | Ilizarov | 9.2 | 1 | 19 | – | – |
| Shah et al. (2011) | 11 | Retrograde IM nailing, bone grafting | 15.2 | 2 | 6 | 8 | – |
| Mathieu et al. (2008) | 10 | Ilizarov + ante/retrograde nailing | 4.0 | 2 | 1 | 3 | – |
| Present series (2012) | 15 | Ilizarov + antegrade nailing + plating | |||||
| in some cases | 4.5 | 8 | 1 | 2 | 1 advised |
The relationship between the fibular status and ankle malalignment has been investigated by numerous authors. Fibular union has to be looked for, and proximal migration of the fibula has to be looked for and prevented. Proximal migration of the distal fibula was seen in 7 of our patients, all of whom had undergone bone transport. In these 7 patients, we transfixed the distal tibiofibular joint, at least during the period of bone transport. We also looked for residual ankle valgus malalignments and identified 7 patients with ankle valgus. We corrected ankle valgus exceeding 5°, similarly to Inan et al. (2006).
The method of nailing has also been a matter of considerable debate in CPT. Retrograde intramedullary rodding has been used by many authors, with good results. In their long-term study of 11 patients, Shah et al. (2011) showed union in all patients with 6 refractures occurring in 5 patients. Dobbs et al. (2005)_ENREF_15 showed satisfactory long-term results in 16 of their 21 patients treated with transankle Williams rod stabilization, with 12 cases of refracture. However, ankle joint function and stiffness is an important drawback with this type of fixation. Shah et al. (2011) showed no ankle joint motion in those patients in whom the rod was retained. Ankle function was satisfactory only in the 3 patients in whom the rods were stopped just above the ankle. We anticipated this problem and therefore used the antegrade method of intramedullary nailing in all patients, and found satisfactory ankle motion in most of the patients. However, the direction of nailing is relatively dependent on the location of the CPT, since extremely distal location of the pseudarthrosis, and those very near the distal tibial physis, may still require a transplantar nail; these patients are known to have poor ankle function. We could, however, obtain good results in almost all our patients with antegrade direction of the nail; complete union occurred in all but 3 of the patients. 2 of the patients had to be supplemented with a plate to achieve union while 1 of them had not achieved union at the last follow-up.
Our patients had some residual limb length discrepancy after the surgery, with a mean value of 1.9 (1–3.2) cm at the last follow-up (as compared to 2.5 (1.5–5) cm preoperatively). However, union is the most important parameter, and limb length discrepancy can be tackled later on, if necessary. Even when the Ilizarov method was used for lengthening, the initial resection was so extensive in some patients, and even after substantial lengthening, some residual shortening was present. Since most of the patients had a residual LLD of less than 2 cm, repeated distraction osteogenesis was not done in any of the patients.
The present study is quite similar to that of Mathieu et al. (2008), who published a series of 10 patients with CPT who were treated with a combination of intramedullary nailing and the Ilizarov technique. At a mean follow-up of 1.2–6.6 years (comparable to our series), they had good results in 9 cases, with 14 complications. There were a few notable differences. Firstly, Mathieu et al. used different kinds of nails (Elastic nails, Kirschner wires, and telescoping rods) and also different configurations (antegrade or retrograde). The other difference is that we measured the functional outcomes by the validated AOFAS score.
The present study has some limitations. It is a pilot study with very good medium-term results. Long-term studies until skeletal maturity are needed to evaluate the benefit of this method. In addition, our group was not homogenous as almost half of the patients had been operated previously, some of them several times.
In conclusion, our method combines the qualities of two techniques and appears to provide lower refracture rates, fewer axial malalignments, and comparable functional outcomes than the methods used in other series.
Acknowledgments
MVA, KWP, and MAR: implementation, manuscript preparation, editing. HRS: study design, manuscript preparation, editing. SHS: study design, data analysis, implementation, and editing.
This study was supported by a grant from the Korea Healthcare Technology R&D Project, the Ministry of Health, Welfare, and Family Affairs, Republic of Korea (A110416).
No competing interests declared.
References
- Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV. Congenital pseudarthrosis of the tibia associated with neurofibromatosis-1: treatment with Ilizarov’s device. J Pediatr Orthop. 1997;17:675–84. doi: 10.1097/00004694-199709000-00019. [DOI] [PubMed] [Google Scholar]
- Boyd HB. Pathology and natural history of congenital pseudarthrosis of the tibia. Clin Orthop. 1982;(166):5–13. [PubMed] [Google Scholar]
- Cho TJ, Choi IH, Lee SM, Chung CY, Yoo WJ, Lee DY, Lee JW. Refracture after Ilizarov osteosynthesis in atrophic-type congenital pseudarthrosis of the tibia. J Bone Joint Surg (Br) 2008;90:488–93. doi: 10.1302/0301-620X.90B4.20153. [DOI] [PubMed] [Google Scholar]
- Choi IH, Cho TJ, Moon HJ. Ilizarov treatment of congenital pseudarthrosis of the tibia: a multi-targeted approach using the Ilizarov technique. Clin Orthop Surg. 2011;3:1–8. doi: 10.4055/cios.2011.3.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dobbs MB, Rich MM, Gordon JE, Szymanski DA, Schoenecker PL. Use of an intramedullary rod for treatment of congenital pseudarthrosis of the tibia. A long-term follow-up study. J Bone Joint Surg (Am) 2004;86:1186–97. doi: 10.2106/00004623-200406000-00010. [DOI] [PubMed] [Google Scholar]
- Dobbs MB, Rich MM, Gordon JE, Szymanski DA, Schoenecker PL. Use of an intramedullary rod for the treatment of congenital pseudarthrosis of the tibia. Surgical technique. J Bone Joint Surg (Am) (Suppl 1) 2005;87:33–40. doi: 10.2106/JBJS.D.02764. [DOI] [PubMed] [Google Scholar]
- Grill F, Bollini G, Dungl P, Fixsen J, Hefti F, Ippolito E, Romanus B, Tudisco C, Wientroub S. Treatment approaches for congenital pseudarthrosis of tibia: results of the EPOS multicenter study. European Paediatric Orthopaedic Society (EPOS) J Pediatr Orthop B. 2000;9:75–89. doi: 10.1097/01202412-200004000-00002. [DOI] [PubMed] [Google Scholar]
- Guidera KJ, Raney EM, Ganey T, Albani W, Pugh L, Ogden JA. Ilizarov treatment of congenital pseudarthroses of the tibia. J Pediatr Orthop. 1997;17:668–74. doi: 10.1097/00004694-199709000-00018. [DOI] [PubMed] [Google Scholar]
- Ilizarov GA. Gracheva VI. [Bloodless treatment of congenital pseudarthrosis of the crus with simultaneous elimination of shortening using dosed distraction] Ortop Travmatol Protez. 1971;32:42–6. [PubMed] [Google Scholar]
- Inan M, El Rassi G, Riddle EC, Kumar SJ. Residual deformities following successful initial bone union in congenital pseudoarthrosis of the tibia. J Pediatr Orthop. 2006;26:393–9. doi: 10.1097/01.bpo.0000217716.64986.f0. [DOI] [PubMed] [Google Scholar]
- Johnston CE. 2nd. Congenital pseudarthrosis of the tibia: results of technical variations in the charnley-williams procedure. J Bone Joint Surg (Am) 2002;84:1799–810. [PubMed] [Google Scholar]
- Johnston CE, Birch JG. A tale of two tibias: a review of treatment options for congenital pseudarthrosis of the tibia. J Child Orthop. 2008;2:133–49. doi: 10.1007/s11832-008-0084-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitaoka HB, Patzer GL. Analysis of clinical grading scales for the foot and ankle. Foot Ankle Int. 1997;18:443–6. doi: 10.1177/107110079701800713. [DOI] [PubMed] [Google Scholar]
- Kristiansen LP, Steen H, Terjesen T. Residual challenges after healing of congenital pseudarthrosis in the tibia. Clin Orthop. 2003;(414):228–37. doi: 10.1097/01.blo.0000076800.53006.c9. [DOI] [PubMed] [Google Scholar]
- Mathieu L, Vialle R, Thevenin-Lemoine C, Mary P, Damsin JP. Association of Ilizarov’s technique and intramedullary rodding in the treatment of congenital pseudarthrosis of the tibia. J Child Orthop. 2008;2:449–55. doi: 10.1007/s11832-008-0139-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohnishi I, Sato W, Matsuyama J, Yajima H, Haga N, Kamegaya M, Minami A, Sato M, Yoshino S, Oki T, Nakamura K. Treatment of congenital pseudarthrosis of the tibia: a multicenter study in Japan. J Pediatr Orthop. 2005;25:219–24. doi: 10.1097/01.bpo.0000151054.54732.0b. [DOI] [PubMed] [Google Scholar]
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop. 1990;(250):81–104. [PubMed] [Google Scholar]
- Paley D, Catagni M, Argnani F, Prevot J, Bell D, Armstrong P. Treatment of congenital pseudoarthrosis of the tibia using the Ilizarov technique. Clin Orthop. 1992;(280):81–93. [PubMed] [Google Scholar]
- Plawecki S, Carpentier E, Lascombes P, Prevot J, Robb JE. Treatment of congenital pseudarthrosis of the tibia by the Ilizarov method. J Pediatr Orthop. 1990;10:786–90. doi: 10.1097/01241398-199011000-00015. [DOI] [PubMed] [Google Scholar]
- Shah H, Doddabasappa SN, Joseph B. Congenital pseudarthrosis of the tibia treated with intramedullary rodding and cortical bone grafting: a follow-up study at skeletal maturity. J Pediatr Orthop. 2011;31:79–88. doi: 10.1097/BPO.0b013e318202c45d. [DOI] [PubMed] [Google Scholar]