

Abstract
In 1925, Calvé described vertebra plana as an aseptic necrosis of bone involving a single vertebral body of the spinal column. This theory was set aside in 1954 by Compere, who concluded that vertebra plana is caused by eosinophilic granuloma and not by osteochondritis as suggested by Calvé. It has been well documented in literature that many factors other than eosinophilic granuloma can cause vertebra plana-like destruction of the vertebral body. However, the definition of the terms was not clear, and there was no consensus on whether to call these cases vertebra plana or not. Some authors did, some did not. Anyhow, no publication so far has reported on osteochondritis as a rare cause of vertebra plana. The case of a 12-year-old girl, presented here by the authors, suggests this explanation. Some important conclusions can be drawn from this regarding the nomenclature, the diagnosis, and the therapy.
Keywords: Vertebra plana, Calvé’s disease, Osteochondritis, Eosinophilic granuloma
Introduction
Vertebra plana is an affliction of childhood: it usually appears between 6 and 12 years of age. The most frequent clinical symptoms are thoracolumbar pain, short-segment kyphosis and loss of interest in playing. Radiologically, the flattening of the anterior part of the vertebral body is seen. For long, the affliction (described by Calvé as “osteochondritis”) was considered a form of aseptic, avascular bone necrosis, involving a single vertebral body. In 1954, Compere argued that Calvé’s theory was not correct and the affliction was caused instead by eosinophilic granuloma [3]. Many other publications and a large number of cases presented later supported his views [5–8]. However, the case presented here is to prove that osteochondritis is a possible, even if possibly rare, cause of vertebra plana.
Case Report
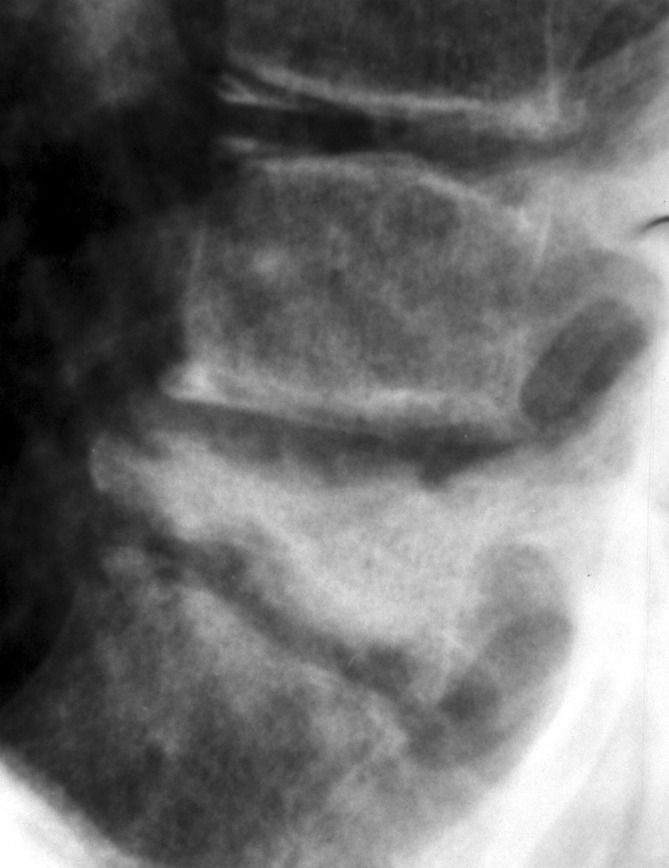
A 12-year-old girl was hospitalized because of severe thoracolumbar pain. Her general health was good; there was no history of trauma; she did not have elevated body temperature. The findings of her general examination were within normal limits. There was no detectable neural deficit or paraplegia. The muscle strength and sensation in the lower limbs were intact. She was continent of urine and of faeces. Other than an elevated alkaline phosphatase level (491 U/l) and a slightly out of range erythrocyte sedimentation rate (29 mm/h), laboratory findings (including CRP, procalcitonin) were normal. There was no palpable swelling locally. Roentgenograms showed vertebra plana of the eleventh thoracic segment (Figs. 1, 2, 3, 4, 5, 6, 7, and 8). A skeletal survey failed to reveal any other abnormalities. The bone scan (400 MBq Tc-99m, i.v.) showed increased uptake in the 11th thoracic segment but was otherwise normal. She was initially treated in a plaster jacket and weight bearing was not allowed. As a consequence of the progressively increasing pain the patient refused to walk or even stand. She was given selective COX-2 inhibitor (2000 mg Ibuprofen per day), which was only temporarily helpful in easing the pain. Thus, she was confined to bed, resisting the slightest movement. Biopsy was done through an open transpedicular approach of the involved vertebral body. The histological examination of the bone marrow clearly showed necrotic bone (empty lacunae, absent of osteoblast rim at the trabecules), infiltrated by a few lymphocytes. Normal erythropoietic tissue was seen in some parts of the bone marrow. Neither giant cells nor eosinophilic cells were detected by the pathologists; nor were there signs of granulomatosis or malignant tissue. Thus, eosinophilic granuloma and malignant tumor were ruled out (Fig. 9). A few days post-operation, the pain started to decrease and day-by-day the patient started to sit up, stand up, and walk. Three months later she was absolutely free of any pain or other symptoms.
Fig. 1.

Roentgenogram taken 6 weeks after the onset of symptoms (lateral view)
Fig. 2.

Roentgenogram taken 5 months after the onset of symptoms (lateral view)
Fig. 3.
Roentgenogram taken 10 months after the onset of symptoms (lateral view)
Fig. 4.

Roentgenogram taken 19 months after the onset of symptoms (lateral view)
Fig. 5.

Sagittal section MRI taken 3 months after the onset of symptoms
Fig. 6.

Sagittal section MRI taken 9 months after the onset of symptoms
Fig. 7.

Sagittal section CT taken 10 months after the onset of symptoms
Fig. 8.

The 3D reconstruction CT view 9 months after the onset of symptoms
Fig. 9.
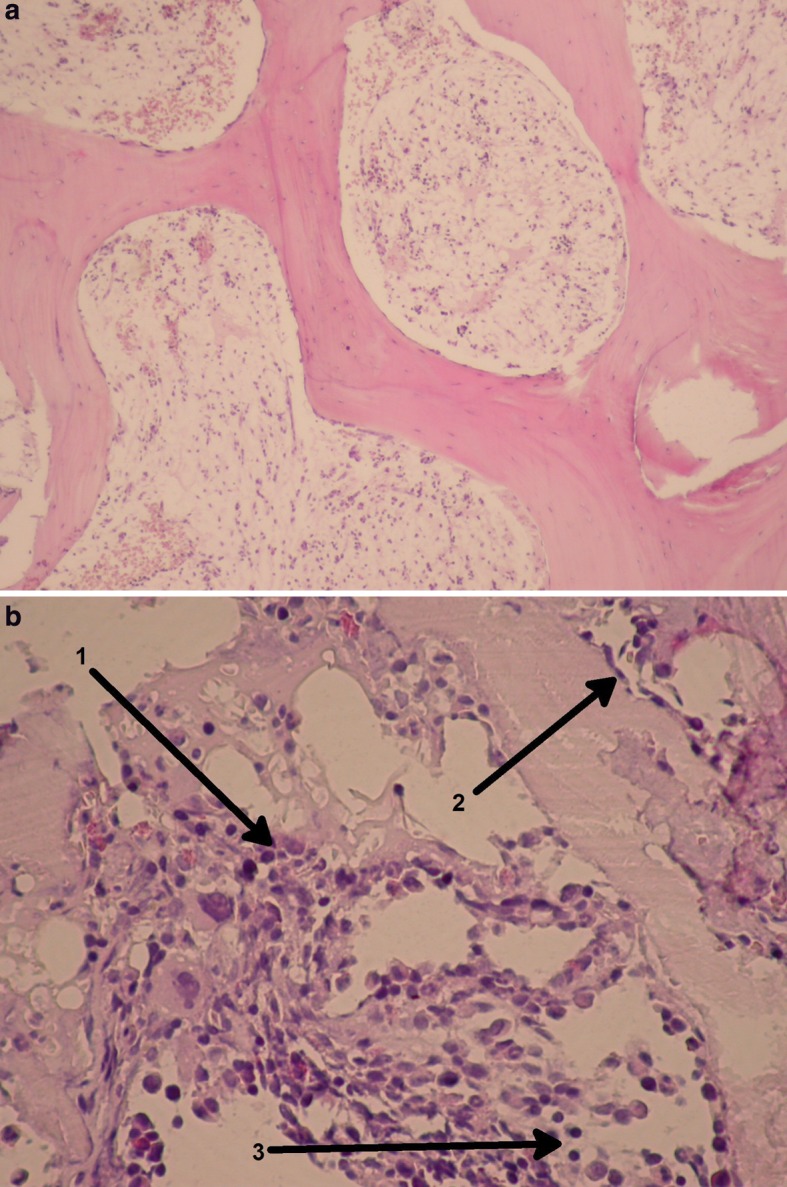
a, b Microscopic picture: 1 normal erythropoietic cells, 2 osteoblasts, 3 lymphocytes
Discussion
In his report in 1925, Calvé included the case of a 7-year-old patient with a condition he described as “osteochondritis” of a vertebral body. He also laid down the criteria of the disease: (1) total collapse of only one vertebra (2) no involvement of the intervertebral disc (3) the intervertebral space wider than normal at least by one-third and (4) increased density of the involved vertebra [2]. Calvé concluded, “The affection [...] is, I believe, to the spinal column what coxa plana is to the hip, and what Koehler’s disease is to the foot” [2]. Buchman, suggested the name “vertebra plana” for this condition in 1927 [1].
Sir Thomas Fairbank, in a lecture in 1952, called attention to a case reported by Snapper, who described a patient with multiple eosinophilic granuloma. The roentgenograms showed the collapse of the sixth thoracic vertebral body. Fairbank stated, “Personally, I feel that eventually vertebra plana will be proved to be one manifestation of granulomatosis, and not a clinical entity”. Two years later, in 1954, Compere reported four cases of vertebra plana with the same radiological changes as described by Calvé. Open biopsy was done and the surgical pathologist’s diagnosis was eosinophilic granuloma in all four patients. Calvé states: “[The cases] ... are herewith presented in support of the theory that vertebra plana is caused by eosinophilic granuloma”. Compere concludes that this clinical entity is certainly not due to osteochondritis, as suggested by Calvé, nor is it due to tuberculosis, metastasis, neuroblastoma, or fracture from trauma [3]. “I would like to make it clear that we are not by any means suggesting that it [eosinophilic granuloma] is the only cause of vertebra plana: but it is the only one that we know about” [3]. Others had a different understanding of the terms; thus we have seen publications presenting cases of vertebra plana due to a variety of conditions: eosinophilic granuloma [3, 4, 5, 12], malignant lymphoma [11], aneurysmal bone cyst [10], chronic recurrent multifocal osteomyelitis [7], Ewing’s sarcoma [9], trauma, osteoporosis, and inflammation [6, 8, 11]. The case presented in this paper is to support the fact that the above list is not complete without the long-denied etiological factor: “osteochondritis” or “aseptic necrosis” of a vertebral body, as described by Calvé. This condition is certainly one of the rare causes of vertebra plana. Interestingly, Compere, in the last paragraph of his paper in 1954, included a case reported by Mezzari in 1938. Mezarri observed an 8-year-old boy suffering from “Calvé’s disease”. At the time of death from an intercurrent infection, the microscopic examination of the vertebra showed no evidence of eosinophilic granuloma. Compere’s explanation was that “... the patient had had symptoms for a year and a half prior to death and that roentgenographically the involved vertebral body appeared to be healing when he died” [3]. Our alternative explanation is that the patient might not have had eosinophilic granuloma at all.
However, with a growing list of conditions that might cause vertebra plana-like roentgenograms, we believe that clear definitions of the terms are essential. We suggest that vertebra plana be a clinical term. Any case in which the flattening of a single vertebral body with the typical “coin on edge” [3] appearance is shown on the radiographs (as first described by Calvé) is to be called vertebra plana, regardless of the etiology. We also suggest using the term “Calvé’s disease” only in cases of vertebra plana that are due to osteochondritis (aseptic necrosis), as this is one true cause of this condition and Calvé was the first one to describe it.
Thus, we conclude that Calvé’s disease is a rare cause of vertebra plana.
References
- 1.Buchman J. Osteochondritis of the vertebral body. J Bone Joint Surg (Am) 1927;9:55–66. [Google Scholar]
- 2.Calvé J. A localized affection of the spine suggesting osteochondritis of the vertebral body, with the clinical aspects of Pott’s disease. J Bone Joint Surg (Am) 1925;7:41–49. [Google Scholar]
- 3.Compere EL, Johnson WE, Coventry MB. Vertebra plana (Calvé’s disease) due to eosinophilic granuloma. J Bone Joint Surg (Am) 1954;36:969–978. [PubMed] [Google Scholar]
- 4.Fowles JV, Bobechko WP. Solitary eosinophilic granuloma in bone. J Bone Joint Surg (Br) 1970;52(2):238–243. [PubMed] [Google Scholar]
- 5.Green NE, Robertson WW, Jr, Kilroy A. Eosinophilic granuloma of the spine with associated neural deficit. Report of three cases. J Bone Joint Surg (Am) 1980;62:1198–1202. [PubMed] [Google Scholar]
- 6.Ippolito E, Farsetti P, Tudisco C. Vertebra plana. Long term follow-up in five patients. J Bone Joint Surg (Am) 1984;66:1364–1368. [PubMed] [Google Scholar]
- 7.Leisure Y, Kasser JR, O’Rourke E, Kozakewich H. Chronic recurrent multifocal osteomyelitis. Association with vertebra plana. J Bone Joint Surg (Am) 1989;71:105–112. [PubMed] [Google Scholar]
- 8.Nesbit ME, Kieffer S, D’Angio GJ. Reconsruction of vertebral height in histiocytosis. X: A long-term follow-up. J Bone Joint Surg (Am) 1969;51:1360–1368. doi: 10.2106/00004623-196951070-00014. [DOI] [PubMed] [Google Scholar]
- 9.Poulsen JO, Jensen JT, Thommesen P. Ewing’s sarcoma simulating vertebra plana. Acta Orthop Scand. 1975;46:211–215. doi: 10.3109/17453677508989210. [DOI] [PubMed] [Google Scholar]
- 10.Schachar J Bone Joint. 1974;Surg:586. [Google Scholar]
- 11.Solgaard S, Kristiansen B. Vertebra plana due to a malignant lymphoma. Acta Orthop Scand. 1980;51:267–269. doi: 10.3109/17453678008990797. [DOI] [PubMed] [Google Scholar]
- 12.Yabsley RH, Harris WR. Solitary eosinophilic granuloma of a vertebral body causing paraplegia. Report of a case. J Bone Joint Surg (Am) 1966;48:1570–1574. [PubMed] [Google Scholar]