

Abstract
Ganglioneuroma is a benign neurogenic tumor. These tumors are originating from neuroepithelium along sympathetic ganglia. Main localization is the mediastinum in children older than 10 years. An association with malignant neuroblastoma is rarely observed and it still remains a topic under current discussion. We describe the clincal course of a 17 year-old female patient with a large presacral mass causing amenorrhoea and weight loss. Eleven years before presentation, an incidental urine test showed an elevation of vanillylmandelic acid (VMA) and homovanillic acid (HMA) and a neuroblastoma was suspected. However, further investigations showed no tumor and the test results turned out to be normal within 1 year. Now, a malignant neurogenic tumor was again suspected, but a CT-guided biopsy revealed a benign tumor. The mass was originating from the left sacral nerve roots. A tumor resection via a dorsal approach was performed. Final histology showed a differentiated ganglioneuroma. This is, to our knowledge, the first report describing a patient with elevated VMA/HMA and suspected neuroblastoma who developed a ganglioneuroma 11 years later. The association of ganglioneuroma and neuroblastoma and the abnormal urine tests pointing toward a neuroblastoma 11 years ago remains unclear and the possible answers are discussed in our report.
Keywords: Ganglioneuroma, HMA, Neuroblastoma, Neurogenic tumor, Presacral tumor, Urine test, VMA
Introduction
Ganglioneuromas, ganglioneuroblastomas and neuroblastomas, are neurogenic tumors with different biological behavior. Ganglioneuromas are thought to arise from sympathetic ganglia and their histology differs clearly from other neurogenic tumors, especially from neuroblastoma. Despite these facts, an association of ganglioneuroma and neuroblastoma appears to be existing. A metachronous occurence of ganglioneuroma and neuroblastoma is described in literature and the possibility of maturation of a maligant neuroblastoma to a benign ganglioneuroma is strongly suspected [3]. Curative treatment of ganglioneuroma is a complete tumor resection, whereas the treatment of neuroblastoma is dependant on the stage of disease and includes surgery, chemotherapy, radiotherapy [1, 2].
Case report
At the age of 6, our patient was found to have abnormal urine test results for vanillylmandelic acid (VMA) and homovanillic acid (HMA) in a routine examination. No systemic or local changes were noticed. The family history was unremarkable. The highly suspected neuroblastoma was excluded using magnetic resonance imaging studies and a bone marrow biopsy. Within 1 year, the test results returned to normal values. Now, aged 17, she sought medical advice because of amenorrhoea and weight loss of 10 kg within 6 months. No further complaints were noticed. An initial abdominal ultrasound showed a pelvic mass and additional imaging studies revealed a large intrapelvic mass, probably arising form the second and third sacral nerve root (Fig. 1). A mass effect was cleary visible, but no infiltration into adjacent structures was seen. The appearance of the lesion suggested a neurogenic tumor. Further investigations staged were normal, especially the blood and urine tests for catecholamines. A CT-guided biopsy showed a ganglioneuroma. A tumor resection was performed. The patient was in a prone position and a partial right-sided resection of the sacrum was the initial step. The sacral nerve roots were identified via laminectomy. Obviously, the tumor was rising from the second and third nerve root. The roots were resected to provide a complete tumor removal. In the following step, the encapsulated tumor mass was mobilized within the pelvic cavity. An additional anterior approach was avoided. The histology showed a benign ganglioneuroma with matured neural tissue and ganglion cells (Fig. 2). No neuroblastoma cell components were identified. Postoperatively, a minimal perianal loss of sensation was observed, but bladder and sphincter function were normal. Full weight-bearing was allowed and the patient left the hospital 14 days after the operation. A follow-up schedule in accordance with to our Interdisciplinary Tumor Board’s recommendations, was established. Follow-up of 24 months including MRI was uneventful.
Fig. 1.
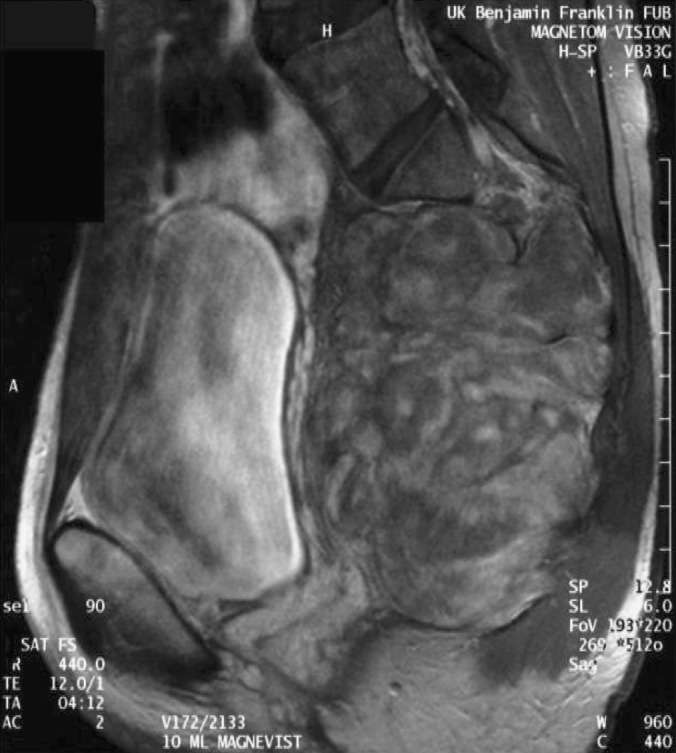
MRI of the presacral tumor
Fig. 2.
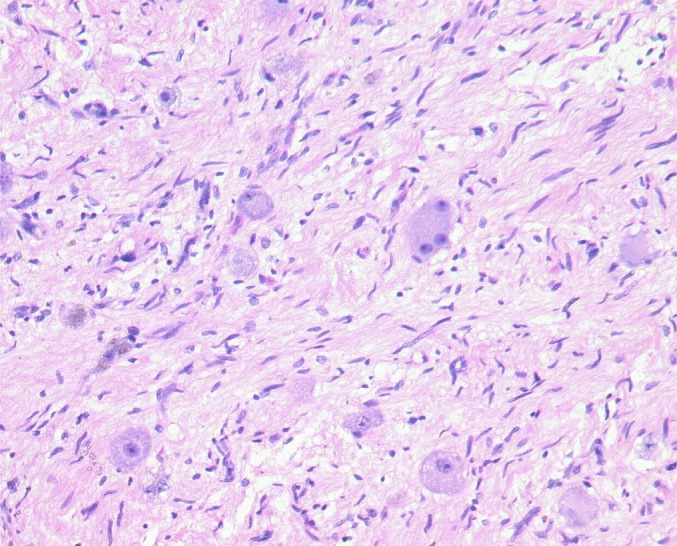
Histology of the resected ganglioneuroma showing mature ganglion cells
Discussion
Ganglioneuroma is an uncommon neurogenic tumor arising from sympathetic ganglia. In general, most of the patients are older than 10 years, as observed in our case report but the tumor has been detected in any age group. The posterior mediastinum is the main localization followed by the retroperitoneum and cervical region. Regarding the localization, various tumor entities have to be excluded, ranging from benign lipomas to malignant neuroblastomas. Ganglioneuromas are asymptomatic in most cases and symptoms are usually caused by mass effects. Imaging studies are showing a partially cystic and calcified mass, and several differential diagnoses have to be considered, for example neurofibroma or chordoma [5]. In rare cases, the tumor is hormonally active and the secretion of vasoactive intestinal polypeptide can cause diarrhoea [5]. In contrast to neuroblastoma, secretion of catecholamines is an uncommon finding in ganglioneuromas. 80% of neuroblastomas are producing elevated levels of VMA and HMA and urine tests are used as screening method. But until now, these tests are not found to reduce the mortality of neuroblastoma, because the additionally detected tumors are in an early stage and may undergo spontaneous regression [1, 4]. Our patient showed elevated urine catecholamine metabolites at the age of 6 years. No further symptoms were found and the family history was negative. A phaeochromocytoma or a neuroblastoma was the suspected malignancy. The lack of systemic symptoms, her age and normal levels of metanephrine were pointing toward a neuroblastoma. However, imaging studies and a bone marrow biopsy displayed normal findings. Within 1 year, her urine tests were normal. Consequently, these abnormalities were explained by a small, probably well-differentiated neuroblastoma, which showed a spontaneous regression. The initial follow-up of our patient was unremarkable until the ganglioneuroma was detected 11 years later.
There are two major explanations of her clinical course. On one hand, the ganglioneuroma can be a primary tumor without any association to her abnormal urine tests. On the other hand, the slow growing ganglioneuroma could be the result of a maturation of the suspected neuroblastoma. Both theories are supported by literature [3]. Spontaneous regression or maturation of neuroblastomas, even of tumors of stage IV was reported [4]. In summary, the clinical course of ganglioneuroma and neuroblastoma and their association appears to be a fluent process in some patients and a long-term follow-up in patients evaluated for a neuroblastoma is strongly suggested.
References
- 1.Brodeur GM. Neuroblastoma: biological insigths into a clinical enigma. Nat Rev Cancer. 2003;3:203–216. doi: 10.1038/nrc1014. [DOI] [PubMed] [Google Scholar]
- 2.Brodeur GM, Azar C, Brother M, Hiemstra J, Kaufmann B, Marshall H, Moley J, Nakagawara A, Saylors R, Scavarda N. Neuroblastoma. Cancer. 1992;70:1685–1694. doi: 10.1002/1097-0142(19920915)70:4+<1685::aid-cncr2820701607>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 3.Christein JD, Kim AW, Jakate S, Deziel DJ. Central pancreatectomy for a pancreatic ganglioneuroma in a patient with previous neuroblastoma. Pancreatology. 2002;2:557–560. doi: 10.1159/000066096. [DOI] [PubMed] [Google Scholar]
- 4.Haas D, Ablin AR, Miller C, Zoger S, Mattay KK. Complete pathologic maturation and regression of Stage IVS neuroblastoma without treatment. Cancer. 1988;62:818–825. doi: 10.1002/1097-0142(19880815)62:4<818::aid-cncr2820620430>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 5.Meyer S, Reinhard H, Ziegler K, Gottschling S, Aliani S, Krenn T, Graf N. Ganglioneuroma: radiological and metabolic features in 4 children. Pediatr Hematol Oncol. 2002;19(7):501–508. doi: 10.1080/08880010290097323. [DOI] [PubMed] [Google Scholar]