

Abstract
State and nonstate health programs in developing countries are often influenced by priorities that are defined in the Millennium Development Goals (MDGs). In the wake of recessionary pressures, policy makers in the health sector are often seen to divert significant budgets to some specific health programs and make only token allocations for other health problems that are important but do not fall under the traditional MDG box of health priorities. This paper illustrates the economic argument for investment in one such program: The eye health program and employs a country case study of Pakistan to demonstrate that there are significant economic gains that are being foregone by not addressing the needs of the blind in poverty reduction strategies. By applying appropriate growth and discounting factors and using the average wage rate, the paper estimates the total productivity gains that are realizable over a period of 10 years if the blind population in Pakistan is rehabilitated and their carers released to participate in the mainstream economic activity. Our findings indicate that significant productivity gains accumulated over 10 years, range from  61 billion (US$ 709 million) to 421 billion (US$ 4.9 billion) depending upon whether the entire blind population or only those affected by a specific cause are rehabilitated. The per annum productivity gains of rehabilitating the entire blind population represents 0.74% of the current gross domestic product of Pakistan, which is higher than the total public spending on health. In order to reap these benefits, the subsequent absorption of the rehabilitated blind and their carers into mainstream economic activity is as important as their effective rehabilitation.
61 billion (US$ 709 million) to 421 billion (US$ 4.9 billion) depending upon whether the entire blind population or only those affected by a specific cause are rehabilitated. The per annum productivity gains of rehabilitating the entire blind population represents 0.74% of the current gross domestic product of Pakistan, which is higher than the total public spending on health. In order to reap these benefits, the subsequent absorption of the rehabilitated blind and their carers into mainstream economic activity is as important as their effective rehabilitation.
Keywords: Blindness, disability, equity, health economics, health policy, health and development, social exclusion
Today when the media addresses global health issues, one is immediately confronted by stark images and statistics of human immunodeficiency virus infection/acquired immunodeficiency syndrome (HIV/AIDS), tuberculosis, malaria, maternal mortality, and child mortality. In recent times, neglected tropical diseases (NTDs) have also begun to attract major global attention due to the vast numbers of people affected and the feasibility of mass drug administration to tackle more than one disease. Indeed, reduction in these conditions constitutes some of the important Millennium Development Goals (MDGs). Unarguably, these scourges must be prevented from decimating populations, and as such we need a united global front to fight them.
But at the same time, a critical question is : Should governments and donors continue to ignore other health issues that may not be as binding as those addressed by the MDGs, yet have a profound impact on people's quality of life, social well-being and economic viability? Can we convince health planners, policy makers and donors to look beyond the debt-aid cycle toward other health problems wherein, with a little investment, we can reap huge gains?
The ability to live long, healthy, and productive lives is a basic human right. From the perspective of equity, justice, and fairness, governments have an altruistic and ethical imperative to provide health services in an equitable manner so as to promote equality of opportunities and enable all its citizens to exercise their full potential. This mandate of the government extends, in particular, to disabled as well as other less privileged members of society. However, since public resources are scarce and often there are competing ends on which these resources can be expended, policies and projects are judged more in terms of tangible material return and less in terms of ethical concerns. Projects that fetch higher economic returns are, in general, preferred over those that fetch lower or no economic returns. Persistent and worsening economic conditions such as those prevailing in low to some middle-income countries mean that many of these projects with noble aims remain unfulfilled and targets unachieved as one moves from one period to the next.
In such a scenario, Non Governmental Organizations (NGOs) are often called in to help. Their sources of funds are diverse, and include voluntary contributions from local as well as expatriate citizens and international donors and NGOs. Again, however, the expense incurred is generally viewed as humane and ethical, but without any economic benefit.
One is therefore inclined to view health interventions through a development lens that seeks sound economic arguments. In the sub-sector of eye health, where community studies may highlight the burden of blindness in terms of people affected or demonstrate a plethora of eye problems at community level, policy makers and health planners may not be completely or easily convinced of the need to enhance public spending toward eye problems as opposed to training of community midwives, for instance, in a resource constrained environment. An economics of blindness perspective provides a context of economic benefits that are needlessly being foregone by a country when eye health is not taken into account in development interventions especially health-related initiatives.
In order to illustrate the socio-economic argument for looking beyond the traditional MDG box of health priorities, we use a country case study of one such program that addresses issues of social inclusion in rehabilitation of the blind population in Pakistan. It represents an example of a developing country with a struggling economy, high debt burden, and off-track targets of MDGs beset by geo-political challenges. This paper focuses on estimating the potential economic gains of implementing this particular program and shows that the rehabilitation of the blind into mainstream economic activity in Pakistan is justified not only on ethical grounds but also on economic grounds. People with blindness forego their wage earnings thereby leading to a decline in overall national income. People who provide care to the blind and look after them also earn less income due to fewer hours available to them to participate in the labor market. The paper shows that if those who suffer from avoidable causes of blindness are treated and cured, and those who are incurably blind are rehabilitated and their carers released to participate in the labor market, substantial economic gains can be reaped.
The Prevalence of Blindness in Pakistan
According to a nationwide survey conducted in 2002–2004 by the Pakistan National Eye Survey Study Group, the results of which are reported in Jadoon et al.,[1] the prevalence of blindness in Pakistan among adults aged 30 years and above is 2.7%. Using the 2011 population estimate of the corresponding age groups this translates into 1.7 million blind adults in Pakistan at present. Of these 85.5% suffer from avoidable causes of blindness and the remaining 14.5% are unavoidably blind. Fifty-five percent of the total blind population in Pakistan is estimated to be cataract blind [Tables 1–3].[2]
Table 1.
The prevalence of adult blindness (30 years and above) in Pakistan by cause
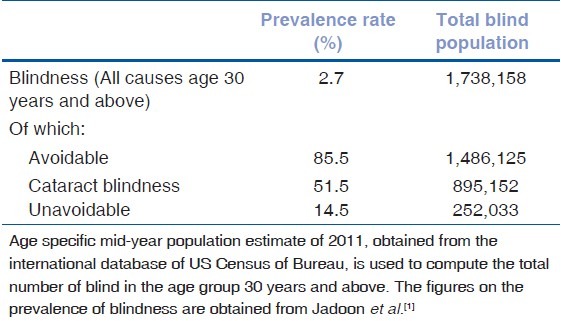
Table 3.
Age specific blind population by cause
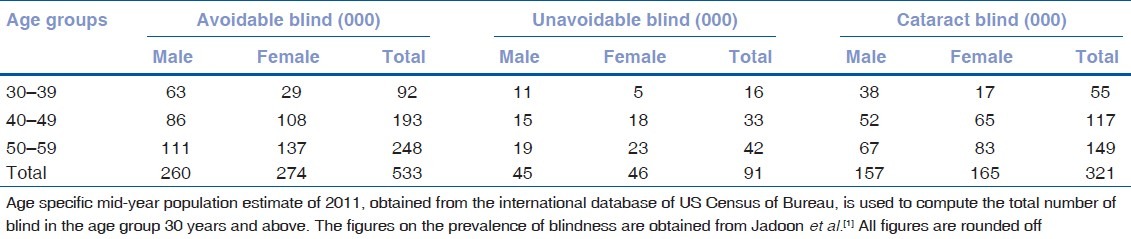
Table 2.
Age specific blind population by all causes in Pakistan
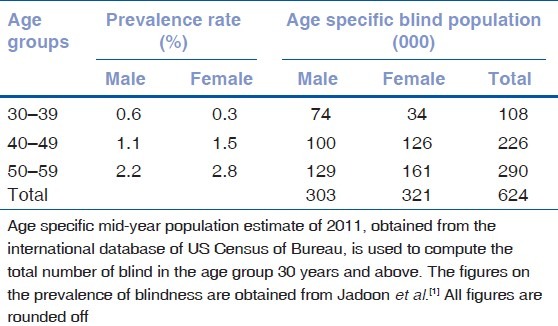
The prevalence of blindness is observed to be higher among older age groups compared with the younger age cohorts. With respect to sex, the prevalence of blindness is lower among females than males in the younger age group of 30–39 years. In older age groups of 40–59 years, the prevalence of blindness is higher among females than among males. Overall there are around 624,000 people blind in Pakistan in the productive age group of 30–59 years.
Materials and Methods
In order to estimate the potential economic gains of rehabilitating the blind in Pakistan, we use the average earnings to calculate the productivity gains that can be realized if the blind population in the productive age group (30–59 years) is rehabilitated and facilitated to become productive members of society. These productivity gains are analyzed for a short run scenario comprising of a year to a long run horizon spanning over 10 years through appropriate growth and discounting techniques. Long-term benefits are computed because health care and rehabilitation programs have an immediate sizeable effect on resources, but their effect on health and other indicators of social wellbeing extend well beyond a year to a lifetime benefit.
The estimation of productivity gains was done in several steps. In the first step, data on average monthly wage earnings were obtained for 2003 (which corresponds to the year of blindness data). A disaggregated data of wage rates by sex were used in order to take into account the substantial difference between the average wages of the two sexes.
These monthly wage earnings were converted into per annum average wage earnings of an individual. The per annum individual wage earnings were then extrapolated for the next 10 years by applying the official growth rate in nominal wages for the corresponding year and by deflating the nominal wage earnings by the corresponding inflation rate. For this purpose, GDP deflator, which is commonly used to deflate output, was used as a measure of inflation. Since we do not have the inflation figures for 2011–2013, we used the moving average of inflation in the past 5 years preceding 2011. In the second step, the extrapolated wage earnings over the 10-year period were aggregated and discounted to estimate the net present value of the future stream of income over the 10-year period. The standard discounting formula was applied to compute the present value of future earnings:
![]()
where PV denotes present value of future income. Yi represents per annum individual wage earning in year i. The discount rate r=0.04 and n=10 is used. The discount rate is based upon the weighted average rate of return on long-term deposits (5 years and over) in 2004 as published by the State Bank of Pakistan.[3]
In the third step, the present value of individual wage earnings over the 10 year period was multiplied by the total number of blind adults in the productive age group of 30–59 years to compute the aggregate level of income achieved by rehabilitating the blind population and enabling them to participate in the labor market. As a consequence of this, the rehabilitation of blind would also release the carers productive time, which they can use for wage earnings. In order to estimate that, we first estimated the average hours that carers spend on the care of the disabled. This was done by making use of the recently available data on Time Use Survey conducted by the Finance Division of Pakistan.[4]
The survey contains detailed data on unpaid care work that includes housework by women as well as time spent on caring for children, old people, the sick, and disabled, as well as time spent in assisting the community. The survey covered a randomly selected sample of 19,600 household from all four provinces of the country. According to the survey, the mean length of time spent by the carers on physical care and supervision of sick or disabled adults is 119 minutes or 2 hours. This is equal to one-fourth of the total productive time per day (assuming that the total productive time is 8 hours per day). This includes the following activities: Physical care of sick or disabled adult (activity code 541); accompany sick and disabled (activity code 551); supervising sick and disabled adult (activity code 562); and travel related to care of sick and disabled adult (activity code 582).
The average number of hours spent on care for disabled is multiplied by the hourly wage rate, which was then converted into monthly and yearly income. The hourly wage rate is derived from average monthly earnings of both sexes and the key assumption made in the computation is that the average hours worked per week are 48 hours as reported in the Labor Force Survey of Pakistan. The hourly wage computed in this way turns out to be 21 (about US $0.25).
Again, these per annum individual wage earnings were extrapolated for the next 10 years by applying the official growth rate in nominal wages for the corresponding year and the discount rate. The total individual wage earnings thus computed over the 10-year period were multiplied by the total number of carers, which is assumed to be equal to the total number of blind in both the productive as well as nonproductive age group. Since we do not have data on the division of carers by sex, we applied the wage rate of both sexes as reported in the Labor Force Survey and in Table 4. In the final step, the total potential earnings of the blind as well as the carers were added and expressed as a percentage of the current GDP of Pakistan.[5]
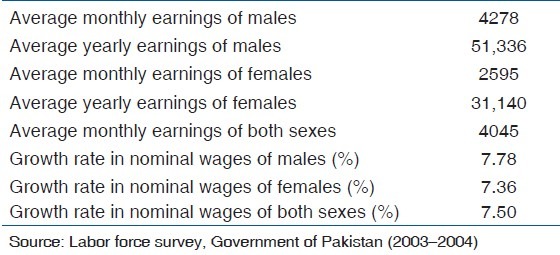
Table 4.
Estimates of average earnings and growth rates in 2003–2004 used in the study (Pak )
By taking average labor earnings as a proxy for average productivity, the present paper uses a much more rigorous and accurate methodology compared with earlier studies.[6,7] that take per capita GNP as a proxy for average earnings and hence productivity, in estimating the burden of blindness. It is important to note the GNP per capita includes income from many sources including labor and nonlabor sources. Income from nonlabor sources may include rental income or returns on financial investments. While income from nonlabor sources may not be directly affected by blindness, it is the wage income that is mostly foregone by the blind population. In short, average wage is a much more reasonable proxy of average productivity than GNP per capita.
Key Assumptions
The following key assumptions were made to estimate the gains in productivity of rehabilitating the blind in Pakistan:
The productivity gains were estimated for individuals in the economically productive age group for which we have data on the prevalence of blindness: 30–59 years of age. Although the productive age starts from 18 years, however, we do not have data on the prevalence of blindness for age groups below 30 years. Our estimates of productivity gains of rehabilitating may therefore be downward biased. The inclusion of younger age groups in the computation is likely to increase further the estimates of economic gains. Furthermore, as only those with ‘blindness’ were considered for this paper, there is likely to be an underestimation as those with moderate or severe visual impairment were not included in the calculations.
The foregone earnings of the blind population were computed assuming full utilization of their productive time in case of rehabilitation. This may not appear to be a realistic assumption as all blind persons may not be able to fully utilize their productive time. The possible upward bias in our estimates from this assumption is, however, likely to cancel out with the downward bias of our estimates due to noninclusion of less than 30 years of population in our productive age group.
The estimates of average monthly earnings for males, females, and both sexes are taken from the Labor Force Survey (2003–2004) of Pakistan. These are shown in Table 4. The growth rate of wages is also taken from the same survey.
The foregone earnings of the carers were computed based upon the evidence from Time Use Survey (conducted by the Ministry of Finance, Pakistan) according to which they devote 2 hours of their productive time per day for the care of disabled persons.
Since we are not aware of the precise division of carers by sex, we used the average hourly wage rate of both sexes as reported in the Labor Force Survey of Pakistan (2003–2004).
The total number of carers is assumed to be equal to the total number of blind population that includes the blind people in both the productive and unproductive age group.
The discount rate used for computing the present value of future stream of income is 4%, which is based upon the weighted average rate of return on long-term deposits (5 years and over) in 2004 as published by the State Bank of Pakistan.[3]
Sources of Data
Data on the prevalence of blindness by age group and by sex was obtained from the Pakistan National Eye Survey Study Group that conducted a nationally representative survey of blindness in Pakistan, the results of which are reported in Jadoon et al.[1] The latest demographic data on Pakistan, disaggregated by age and sex, was obtained from the international database of US Census of Bureau. Data corresponding to average earnings was obtained from the Labor Force survey of Pakistan. Finally data on current GDP of Pakistan and inflation rate was obtained from the Economic Survey of Pakistan.[5]
Results
Table 5 illustrates our computation results regarding the potential productivity gains of rehabilitating the blind in Pakistan, disaggregated by sex and by causes.
Table 5.
Economic benefits of rehabilitating the blind in Pakistan (All causes)
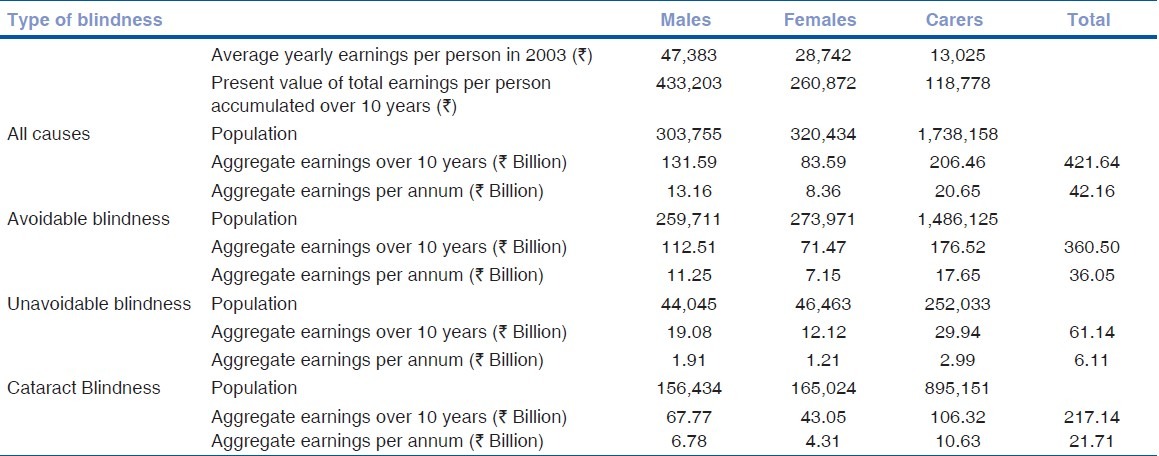
The results show that if the entire blind population in Pakistan (by all causes) is rehabilitated, the total economic benefit/productivity gain of 422 billion (US$ 4.9 billion) is realizable over a period of 10 years. This translates into 42.2 billion (US$ 490 million) per annum. If only the avoidable blindness is treated, the aggregate economic benefit of 361 billion (US$ 4.25 billion) over a period of 10 years and an average of 36 billion (US$ 425 million) per annum is realizable. The rehabilitation of incurably blind results in the aggregate benefits of 61 billion (US$ 718 million) over a period of 10 years and an average of 6.1 billion (US$ 71.8 million) per year. Similarly, the treatment of cataract blindness results in 217 billion (US$ 2.55 billion) over 10 years and an average of 21.7 billion (US$ 255 million) per annum.
In Table 6, these economic benefits are expressed in terms of the total current GDP of Pakistan. Table 6 shows that if the entire blind population in Pakistan is rehabilitated, economic benefits per annum amount to 0.7% of GDP. This is a significant economic gain that is roughly equal to the total government spending on health in Pakistan. If only those people are treated who are blind due to avoidable causes, the economic benefit achieved per annum is equal to 0.6% of GDP.
Table 6.
Economic benefits of rehabilitating the blind in Pakistan
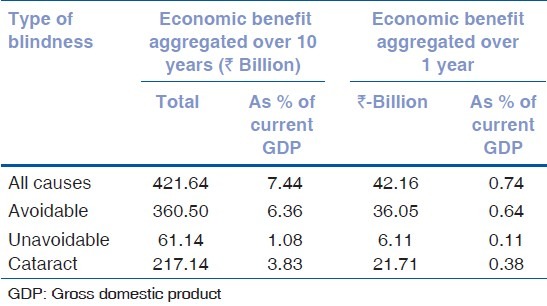
The results in Table 6 show that even if the rehabilitation of the blind in Pakistan costs 0.7% of the GDP per annum, it is still justified on economic grounds. In future, it would be useful to estimate the total cost of rehabilitating the blind in Pakistan which can then be compared with the total economic benefits computed in terms of productivity gain above so as to estimate the net economic gain of rehabilitating the blind in Pakistan.
Discussion
The World Health Organization states that there are 285 million people visually impaired and 39 million blind globally.[8] These conditions by themselves may not be life threatening but they have a significant impact on quality of life, and are associated with poverty and social exclusion. Of those who are visually impaired, 153 million are in need of a simple pair of spectacles to correct their refractive error. Twelve million school children aged between 5 and 15 years are visually impaired for want of a pair of spectacles. At least half of all the people who are blind have cataracts which can be treated easily by surgery.
Trachoma and onchocerciasis (River Blindness) are two of the NTDs.[9] Trachoma, a blinding disease spread by flies affects 84 million people in 56 countries and 8 million are blind or visually impaired. River Blindness affects 37 million people of whom 750,000 are severely visually impaired or blind.
A total of 1.4 million children are estimated to be blind.[10] Children who are born blind or who become blind and survive have a lifetime of blindness (70 million blind years) ahead of them, with all the associated emotional, social and economic costs to the child, the family and society. It affects their access to education and severely limits their livelihood options in developing countries. Indeed, many of the conditions associated with blindness in children are also causes of child mortality, for example, premature birth, measles, vitamin A deficiency, meningitis, and Congenital Rubella Syndrome. Control of blindness in children is, therefore, closely linked to child survival. Infant mortality has been found to be 63% higher in night-blind mothers.[11] Women have been found to have a 30% higher risk of blindness than men.[3]
In this paper, we have tried to demonstrate, through a country case-study, the opportunity cost of not addressing the needs of the blind in poverty reduction strategies. We have used the average earnings approach to calculate the productivity gains that can be obtained if the blind population in the productive age group (30–59 years) is rehabilitated and facilitated to become productive members of society. This approach is based upon the assumption that each person represents a productive resource to society and illness or disability diminishes that person's productive capacity, which in turn is valued by his or her loss of earning.[12] It is important to note that labor earnings is a much more accurate proxy for average productivity compared with GNP per capita used by earlier studies. In this sense, the present study evaluates the economic benefits in a much more rigorous and accurate manner.
The results of our analysis indicate that the rehabilitation of the blind can potentially result in significant productivity gains in the form of increase in earnings by both the blind and their carers. Our estimates suggest that the aggregate economic benefits spread over a 10-year period represent 0.7% of current GDP per annum, which is roughly equal to the total public spending on health. Our results clearly show that the rehabilitation of the blind in Pakistan is not only justified on ethical and humanitarian grounds but also on economic grounds. However, in order to reap these benefits, an effective rehabilitation is not adequate; subsequent absorption into mainstream economic activity must also be facilitated.
Sensitivity analysis
Although our results are sensitive to the assumptions we made, it turns out that the negative and positive biases that are most likely to be created by two of our most critical assumptions tend to outweigh each other and there is no significant deviation from the results otherwise obtained. More specifically, let us examine the impact of two of our most critical assumptions:
The first assumption is the consequence of our data limitation : The estimates of blind population in Pakistan are available only for ages 30 years and above, however, the productive age group starts from 18 years and above.
We assumed full utilization of the productive time of the blind in case of rehabilitation. Our first assumption is likely to produce a downward bias in our estimates.
Our sensitivity analysis indicates that if we include the population from 20–29 years and above and apply the same incidence of blindness as that prevailing in the age group of 30-34 year, our estimates of economic gains for the 10-year period increase from 421 billion to 688 billion; a difference of about 267 billion. If on the other hand, we apply the assumption that only 50% of the blind are able to participate in the labor market after being rehabilitated, our estimates of aggregate economic earning decrease from 421 billion to 210 billion : A reduction of 210 billion. The positive bias turns out to be slightly higher that the negative bias thereby bringing in a net increase of about 57 billion in our estimates of economic gain over the 10-year period (421-210+267=478). This translates into 8% of the current GDP.
The estimates arrived are conservative for two reasons. The first is the issue of age alluded to earlier. Secondly, we have used the average wage rate and it is possible that many of the people who are blind, if equipped with education and skills, are able to earn more than the average wage rate.
Frick and Foster[13] used economic and epidemiologic modeling to estimate the number of blind individuals globally and the associated economic productivity loss from the year 2000 to 2020. They concluded that if significant efforts were made to reduce avoidable blindness, this could result in a reduction of 429 million blind person-years and a minimum saving of $102 billion for unaccommodated blindness alone over the period from 2003 to 2020. Similarly, Taylor et al.[14] in Australia attempted to quantify the economic costs of vision loss in Australia and assess the impact of a costed intervention package to prevent avoidable vision loss. They found that the intervention package, if implemented, could bring about a 4.8-fold return on investment.
Cataract is the most common cause of blindness in Pakistan. Our study shows that if the cataract blind are rehabilitated, this alone will result in an economic benefit aggregated over 1 year of 0.38% of the current GDP. Eye care has a proven range of low-risk, high-success, and highly cost-effective interventions as measured by cost utility and cost-effective analyses.[15] Cataract surgery is one of the most cost-effective interventions in developing countries, costing as little as US $15 to US $23 per disability-adjusted life-year saved.[16]
Despite dismal health indicators, Pakistan spends a meager amount of its GDP on the health sector. Over the past many decades, total public health spending in Pakistan has remained below 0.8% of its GDP. Within the health sector itself, there are multiple increasingly expensive areas, each clamoring for adequate funding. Not all of these areas are expected to reap economic gains nor are all justified on ethical and equity grounds.
The present global financial crisis has impacted developing and developed countries alike but some countries are affected more than others. Some developing countries may be at a higher risk of not spending enough on social sectors due to the fact that they have approached the International Monetary Fund (IMF) for emergency assistance. The IMF may impose additional restrictions on these countries to spend less on social sectors and rather focus on cost recovery, which may not be possible under present circumstances. Populations in countries affected by or emerging from conflict, with few financial reserves, weak institutions and damaged infrastructure, are especially vulnerable.
There is a need to protect health spending in countries where per capita health expenditures are below certain threshold levels, which may be necessary to achieve reasonable health outcomes. Besides, entitlement to better health outcomes is a basic human right. This requires policy coordination from both the government and donors not only in priority health sectors but also in other allied areas as well.
The Rio Declaration of 1992 stated that “Human beings are at the centre of concerns for sustainable development”. Preventing and treating blindness and improving eye health is one of the most cost-effective health interventions that not only improves the quality of life and promotes social inclusion, but also increases productivity. According to VISION 2020–The Right to Sight–globally, about 85% of all visual impairment and 75% of blindness could be prevented or cured through well-tested control interventions.
Conclusion
One of the most important insights that the Human Development Paradigm offers is that poverty is not so much a problem of the lowness of income as of the inadequacy of income to achieve the necessary functioning and the capability (or the freedom) to acquire those functioning.[17] Poverty is obviously seen ‘as a serious deprivation of certain capabilities’.[18] The implication of this approach on development policy is that poverty must be accepted as social evil irrespective of prevailing inter-country and interpersonal disparities between income and expenditure patterns; and that ameliorative action must go well beyond just raising the income of the target group of poor. Everywhere, it would take transforming more resources to the poor and the physically disabled in order to redress interpersonal capability deficits. It provides the basis to infer that an effective eye health system to eradicate visual impairment must be seen in the context of capabilities approach for necessary functioning of human beings for their livelihood and survival.
There are many direct and indirect gains that can be achieved through targeted expenditure in the health and education sector. It is important for these to be documented and used as part of the planning process.
Equally important, the social sector expenditure–that includes spending on education, vocational training as well as spending targeted toward those with special needs–may not realize the true benefit if the mechanisms to absorb the excess capacity are not encouraged and facilitated. Generally, this would include areas as diverse as job creation and industrialization on one hand and sustainable and equitable rural development and economic empowerment on the other hand.
It is important for policy makers at the national level to realize that economic evaluation should be an integral component of the health planning process. Furthermore, rehabilitation of the disabled, including blind, can result in significant economic benefits in terms of increase in overall productivity and thus should be included in poverty reduction strategies. However, it must be recognized that this gain is fully realizable only if those with disabilities, such as the rehabilitated blind, are facilitated in realizing their full employment and livelihood development potential.
Acknowledgments
We acknowledge with grateful thanks the financial support provided by Sightsavers to conduct this study.
Footnotes
Source of Support: Sightsavers
Conflict of Interest: None declared
References
- 1.Jadoon MZ, Dineen B, Bourne RR, Shah SP, Khan MA, Johnson GJ, et al. Prevalence of blindness and visual impairment in Pakistan: The Pakistan National Blindness and Visual Impairment Survey. Invest Ophthalmol Vis Sci. 2006;47:4749–55. doi: 10.1167/iovs.06-0374. [DOI] [PubMed] [Google Scholar]
- 2.Dineen B, Bourne RR, Jadoon Z, Shah SP, Khan MA, Foster A, et al. Causes of blindness and visual impairment in Pakistan.The Pakistan national blindness and visual impairment survey. Br J Ophthalmol. 2007;91:1005–10. doi: 10.1136/bjo.2006.108035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.State Bank of Pakistan. ‘Handbook of Statistics on Pakistan's Economy’. 2010. [Last accessed 2012 Jan 25]. Available from: http://www.sbp.org.pk/departments/stats/PakEconomy_HandBook/index.htm .
- 4.Valuation of Unpaid Care Work in Pakistan. Government of Pakistan, Finance Division, Strengthening PRS Monitoring Project. 2009 [Google Scholar]
- 5.Government of Pakistan. Economic Survey of Pakistan. 2010 [Google Scholar]
- 6.Shamanna BR, Dandona L, Rao GN. Economic burden of blindness in India. Indian J Ophthalmol. 1998;46:169–72. [PubMed] [Google Scholar]
- 7.Smith AF, Smith JG. The economic burden of global blindness: A price too high! Br J Ophthalmol. 1996;80:276–7. doi: 10.1136/bjo.80.4.276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Visual impairment and blindness: Fact Sheet N 282. Geneva: World Health Organization; 2011. Oct, [Google Scholar]
- 9.First WHO report on neglected tropical diseases. Working to Overcome the Global Impact of Neglected Tropical Diseases. Geneva: World Health Organization; 2010. World Health Organization. [Google Scholar]
- 10.Gilbert C, Foster A. Childhood blindness in the context of VISION 2020-the right to sight. Bull World Health Organ. 2001;79:227–32. [PMC free article] [PubMed] [Google Scholar]
- 11.Christian P, West KP, Jr, Khatry SK, LeClerq SC, Kimbrough-Pradhan E, Katz J, et al. Maternal night blindness increases risk of mortality in the first 6 months of life among infants in Nepal. J Nutr. 2001;131:1510–2. doi: 10.1093/jn/131.5.1510. [DOI] [PubMed] [Google Scholar]
- 12.Jefferson T, Demicheli V, Mugford M. British Medical Journal. London: Publishing Group; 1996. Elementary economic evaluation in health care. [Google Scholar]
- 13.Frick KD, Foster A. The magnitude and cost of global blindness: An increasing problem that can be alleviated. Am J Ophthalmol. 2003;135:471–6. doi: 10.1016/s0002-9394(02)02110-4. [DOI] [PubMed] [Google Scholar]
- 14.Taylor HR, Pezzullo ML, Nesbitt SJ, Keeffe JE. Costs of interventions for visual impairment. Am J Ophthalmol. 2007;143:561–5. doi: 10.1016/j.ajo.2006.10.055. [DOI] [PubMed] [Google Scholar]
- 15.Brown MM, Brown GC. How to interpret a healthcare economic analysis. Curr Opin Ophthalmol. 2005;16:191–4. [PubMed] [Google Scholar]
- 16.Global initiative for the elimination of avoidable blindness. 1997PBL/97.61. Geneva: World Health Organization; 1997. World Health Organization. [Google Scholar]
- 17.Sen AK. Inequality, Re-examined? New York: Clarendon Press; 1992. Inequality of what. Chap 1. [Google Scholar]
- 18.Sen AK. The possibility of social choice. Am Econ Rev. 1999;89:3,349–78. Reprinted in Amartya Sen (2002), Rationale and Freedom. New Delhi: Oxford University Press. [Google Scholar]