

Abstract
Health inequities are related to social determinants based on gender, socioeconomic status, ethnicity, race, living in a specific geographic region, or having a specific health condition. Such inequities were reviewed for blindness and visual impairment by searching for studies on the subject in PubMed from 2000 to 2011 in the English and Spanish languages. The goal of this article is to provide a current review in understanding how inequities based specifically on the aforementioned social determinants on health influence the prevalence of visual impairment and blindness. With regards to gender inequality, women have a higher prevalence of visual impairment and blindness, which cannot be only reasoned based on age or access to service. Socioeconomic status measured as higher income, higher educational status, or non-manual occupational social class was inversely associated with prevalence of blindness or visual impairment. Ethnicity and race were associated with visual impairment and blindness, although there is general confusion over this socioeconomic position determinant. Geographic inequalities and visual impairment were related to income (of the region, nation or continent), living in a rural area, and an association with socioeconomic and political context was suggested. While inequalities related to blindness and visual impairment have rarely been specifically addressed in research, there is still evidence of the association of social determinants and prevalence of blindness and visual impairment. Additional research should be done on the associations with intermediary determinants and socioeconomic and political context.
Keywords: Visual impairment, blindness, inequality, social class, income, educational status, gender and ethnic groups
Health inequity refers to differences or inequalities in health among social groups that are unnecessary, avoidable, unfair, and intolerable.[1] These inequalities are related to social determinants based on gender, socioeconomic status, ethnicity, race, living in a specific geographic region, or having a specific health condition. Inequality, poverty, exploitation, violence, and injustice are causes of illness and death of the poor and marginalized.[2] However, instead of focusing solely on reducing global poverty to improve health equity, greater attention should be given to improving the socioeconomic conditions of global society.[3]
Health inequalities can be reproduced at any level associated with the effect of the relative versus absolute socioeconomic position of individuals and patterning of the social gradient in health.[4] Indeed, there is a common social gradient across global society–the lower the socioeconomic position of an individual, the poorer is their health.[5] Social determinants of health are structured along three major levels: structural determinants focusing on socioeconomic and political context (governance, macroeconomic policies, social policies, public policies, and culture and social values); socioeconomic position structural determinants (class, power, prestige, and discrimination); and intermediary determinants.[5,6]
In this review, we examine how the socioeconomic factors of gender, income, education, occupation, and ethnicity/race related to an individual's social position influence visual impairment and blindness. A review on socioeconomic status and blindness[7] was published 10 years ago, which focused only on blindness, even though there are six times as many people with visual impairment. However, previous literature usually did not discuss how social inequalities influenced visual health. There is literature on visual impairment and blindness that stratified outcomes on income, education, employment status, social class, gender, and race/ethnicity. Geopolitical area is also considered to have an influence on the socioeconomic and political context. The goal of this article is to provide a current review to understand how inequities based on socioeconomic determinants of health influence prevalence of visual impairment and blindness.
Materials
Literature was searched on PubMed using combinations of the following two groups of keywords: Ocular outcome (visual impairment, blindness, cataract, diabetic retinopathy, glaucoma, eye health, eye care, ophthalmology, and prevalence) and structural determinants of socioeconomic position (socioeconomic status, social class, income, educational status, gender, poverty areas, ethnic groups, race, inequality, disparity, inequity, and access). Causes of blindness and visual impairment were included as key words to capture publications that produce secondary results on visual impairment or blindness. The search included original population-based studies, reviews, and meta-analysis from 2000 to 2011 in the English and Spanish languages. There were no other limitations specified. There were 565 publications found: 101 for gender, 53 for income, 42 for education, 12 for social class, 109 for inequality, 109 for socioeconomic factor, and 95 for race/ethnicity. A total of 312 publications were found for visual impairment and 253 for blindness prevalence outcomes. Three reviewers independently examined the title and the abstract of each article, classifying the articles in six fields: gender, income, education, employment status and social class, geographic, and race/ethnicity. Full text and tables of all the articles that had results on visual impairment or blindness outcomes were reviewed. Two inclusion criteria were evaluated: (1) present empirical findings related to outcomes of prevalence of visual impairment or blindness in population-based studies on adult populations and; (2) a gender, income, educational level, employment status and social class, or race stratifying measure. A manual search of the references of these studies, an additional 16 articles were identified. Given that publication dates included in the review range from 2000 to the present, when the articles found in this review did not fill the gap on the knowledge previously documented additional material was sought from study references and literature collections conducted in earlier years by the authors.
Results
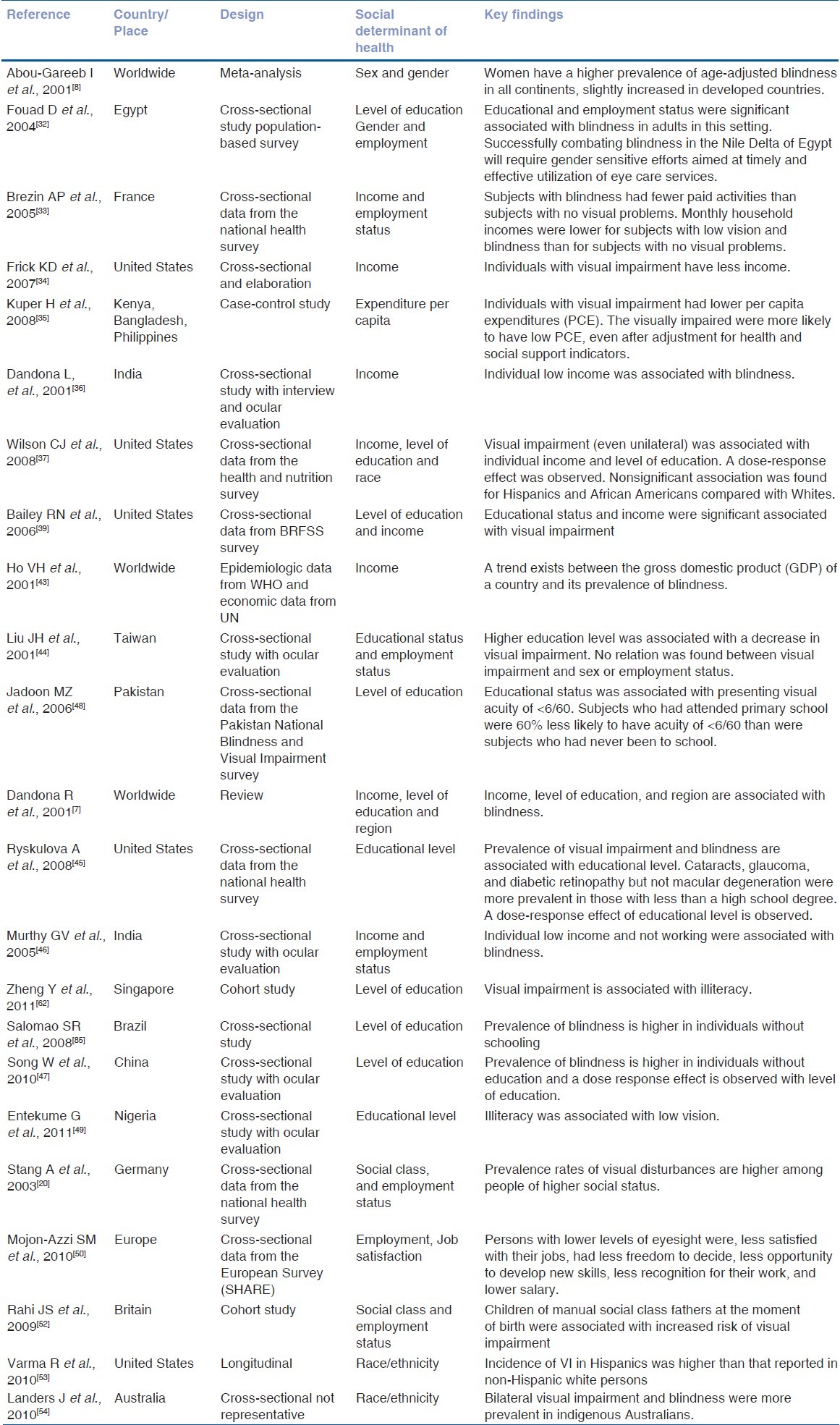
A table has been generated that summarizes the literature review of publications in the last 12 years. A total of 23 studies were found that stratified the results of prevalence of blindness or visual impairment with the structural social determinants of health: gender, income, educational level, employment status, social class, and ethnicity/race [Table 1].
Table 1.
Selected articles on social determinants of health and visual impairment or blindness
Although important inequalities in the prevalence of blindness and sex have been reported, no gender review has been published.[8] A meta-analysis conducted by Abou-Gareeb ten years ago found that women accounted for nearly two-thirds of the population with blindness.[6] After age adjustment, the overall odds ratio (OR) of blind women to men was remarkably consistent by geographical area, being 1.39 for Africa, 1.41 for Asia, and 1.63 for industrialized countries. Research continued to highlight this gender inequity with respect to blindness and visual impairment.[9,10] Later studies on the prevalence of visual impairment and blindness reported a prevalence ratio of more than 1.5 for women in high-income countries, which is surprisingly higher than in low-income countries.[11–14]
Women generally have a longer life expectancy than men. Since many eye diseases are age-related, we would expect women to have a higher burden of visual impairment and blindness.[6] However, even after age adjustment, inequities still persisted.[15]
Access to the health care system was an intermediary determinant and played a role in exposure and vulnerability.[6] Through the analysis of women's access to services, differences between countries at low, middle, and high levels of the Human Development Index (HDI) were observed.[16] In high HDI countries such as the United States (US), Australia, and Germany, women reported more visits to the eye care specialist.[17–20] All age groups of women in the US had better ocular health care utilization than men for all three racial/ethnic groups.[21] No differences in eye care service utilization were found between men and women in the middle HDI countries of Asia, such as Oman, and similar access to cataract surgical services was noted in Latin America.[22,23] In the low HDI countries of Africa and Asia, access to cataract surgical services was lower for women compared with men.[13,24–29] Reasons for not seeking eye care showed different gender patterns for people with some visual impairment; “no need” was the main reason for men and “cost/insurance” for women in the US.[30] Indirect costs of service was a more relevant barrier for women in Ethiopia.[31] Attitudinal differences in seeking health care were also suggested as reasons to explain gender differences in access to eye health care services.[17,32]
Studies in France and the US showed that people with low vision had less income.[33,34] In low HDI countries, such as Kenya, the Philippines, and Bangladesh, multivariate analyses showed that case participants were consistently poorer than controls when assessed using three different measures of poverty even after adjustment for health and social support indicators.[35] Only one article evaluated risk of blindness and individual income and found that low income was associated with blindness in India.[36] Visual impairment, even unilateral, was associated with household income (>$75,000 a year) in the US, and both high rates of blindness and visual impairment were found in the elderly of the US.[37–39]
Increased risk for visual problems was documented in the impoverished neighborhoods with the worst economic indicators in the US and Australia (we must bear in mind, however, that these data are relatively old).[40,41] In addition, the prevalence of blindness and visual impairment was higher in low-income countries when compared with high-income countries.[42] There was also a gradient between the gross domestic product (GDP) of a country and its prevalence of blindness.[43]
Although only a few articles addressed the association of blindness or visual impairment with income, the results were consistent in that lower income was associated with visual problems. Not one article, analyzed in this review, stratified association of income with visual outcomes by sex.
Lower levels of education were associated with higher prevalence of visual impairment in Australia, Taiwan, and the US, as well as blindness in the US, India, and China.[38,39,44–47] In 1991, a reverse association with years of education and prevalence of visual impairment and blindness was observed, and prevalence increased at a much faster rate when illiteracy in India, Pakistan, Nigeria, and the US was taken into consideration.[34,38,39,44,48,49] A higher association with the level of education was found for bilateral (as compared with unilateral) visual impairment in the US.
Reasons for not seeking eye care in the US were based on educational level, with “no need” as the main reason for the highly educated and “cost/insurance” for the lower educated. However, highly educated individuals (32%) still reported “cost/insurance” as a reason for not seeking eye care, although this factor decreased among the high-income population (22%).[28]
People with visual impairment in Europe were at higher risk of not having a paid job, being unemployed, suffering from permanent disability, belonging to a manual social class (with less job satisfaction), having less opportunity to develop new skills, having less recognition for their work, and having an inadequate salary.[50] In France, individuals without visual problems had a chance of having a paid job five times greater than that of blind people and twice than those with low vision.[30] In India, people without work had twice the risk of visual impairment.[44]
The concept of social class derived from occupation was also associated with health indicators. For coding social class, each individual was assigned to their occupation, and each occupation was assigned to one of the six social classes. The first three corresponded to nonmanual workers, and the last three to manual workers. Social class based on occupation integrated the level of training required for a job, income, and the level of responsibility.[51]
In Britain, the risk of poor vision was associated with social class (unskilled manual workers). For each increment in social class grade on a scale of I through V, the risk of poor vision increased by 28%, with a prevalence of 1.9% in social class I (professional) and 5% in social class V (unskilled manual workers). Additionally, children with manual social class fathers at the moment of birth had an increased risk of far and near visual impairment at adulthood.[52] However, prevalence of low vision and blindness for workers was similar to that of the unemployed in the US.[37]
After adjusting for age and socioeconomic position, no association with visual impairments was found among Hispanics, African Americans, and Caucasians in the US.[34] However, Hispanics had a higher incidence of visual impairment than that reported in non-Hispanic White persons and the highest reported in a population-based study in the US.[53] In Australia, bilateral visual impairment and blindness were found to be four to seven times more frequent in the indigenous population.[54] However, it is often difficult to evaluate the prevalence of visual impairment or blindness that might be truly inherent in a racial or ethnic population in addition to the social determinants that a specific racial group were exposed to due to low socioeconomic position and marginalization.
Many studies in the US, but not all, showed no significant differences between ethnic or racial minorities when compared with Caucasian populations, although differences were not always adjusted for socioeconomic position variables.[52,55,56]
Geographic inequalities were found among continents, countries, and regions within a country.[57] In 2000, Africa and India bore the highest prevalence of blindness, followed by the rest of Asia, China, and Latin America.[40] However, Asia led the burden of disability-adjusted life years (DALYs), and cataract was the principal cause of blindness with 95% of the burden in low-income countries.[58] Other studies showed that 87% of the visually impaired and 90% of blind people lived in low-income countries but differences in prevalence persisted between countries in the same region or continent and were inversely correlated with GDP per capita of each country.[40,41,59,60]
In France, geographic inequalities were also found between regions within the country for age-adjusted visual impairment and blindness prevalence.[61] Geographic inequalities were found after occupational social class adjustment, and they were evident for age-adjusted low vision between regions of Nigeria.[45] Differences in the prevalence of visual impairment were similarly found for five states in the US.[62] In Singapore, an ecologic effect of socioeconomic determinants of the community was found to have an independent association with visual impairment, even when considering individual socioeconomic determinants.[62] In Canada, ecologic research found that prevalence of blindness registration correlated with medium household income of districts after evaluating the five geopolitical regions of the country. However, when the model did not consider geopolitical region, medium household income was not statistically correlated. Those results suggested that the geopolitical region played a role in blindness independent of district income. Moreover, income derived from government transfer payments had a negative correlation with blindness registration prevalence.[63]
Discussion
The review produced four main findings: (1) women had a higher prevalence of visual impairment and blindness, which was not fully explained by age or by access to services, (2) socioeconomic status measured as higher income, higher educational status, or nonmanual occupational social class was inversely associated with prevalence of blindness or visual impairment, (3) ethnicity and race were associated with visual impairment, although other social determinants of health can be associated, and (4) geographic inequalities and visual impairment (of the region, nation or continent) were observed to be related to income, and living in a rural area. An association with socioeconomic and political context was additionally suggested.
Results bearing the evidence of the association between socioeconomic position determinants and prevalence of visual impairment and blindness were found in this review, even if this relationship has rarely been addressed in research (23 articles in the last 12 years). However, the effect of an individual's socioeconomic position on his/her health may not be only direct, but may also emerge from intermediary determinants that remain, pending investigation.[4] Possible social determinant pathways that lead to the social gradient should be explored.[3] Future research should be done measuring how exposure or vulnerability explain the pattern of inequalities regarding a specific social stratification such as educational level or income.
A few articles analyzed in this review, upon publication, were categorized as social determinant(s) of health, although the tag was an intermediary factor mostly related to accessibility of services. Additionally, some of the articles considered only psychosocial factors, which are related to occupational health and environmental factors, as determinants for producing inequalities. Although psychosocial consequences of socioeconomic inequality were an important intermediary determinant, interpretation of links between socioeconomic status and health must begin with the structural causes of inequalities.[4] An “ecosocial” approach is a needed consideration to better understand the mechanism of how differences are produced by integrating social and biological factors in a dynamic, historical, and ecological perspective.[64] A possible effect of the first level of social determinants of health–the determinants of socioeconomic and political context–might be considered for future research, since the few results produced thus far consistently suggested this concept.[58,60]
Perceived gender discrimination by women was associated with their poor health outcomes.[65] A greater awareness of gender discrimination behaviors could explain differences between the outcomes of men and women if the slightly increased gender inequalities in prevalence are confirmed for high-income countries versus low-income countries. In addition, gender discrimination patterns affected the decision-making authority, which not only influenced access to services, but also, differences in psychosocial and environmental risk exposure.[66] Further research is necessary. Women also accumulated more working hours than men, and their additional domestic chores negatively affected their health.[67] This could also influence risk of diabetic retinopathy, glaucoma, and cataract if those health issues were related to stress.[68] More research is needed to identify if perceived gender discrimination, decision-making authority, and working hours are associated with gender inequalities in blindness and visual impairment. A study performed in Saudi Arabia, a country with significant gender discrimination, found an extremely high gender inequality of visual impairment between men and women attending primary care (lower for women), and there was lower registration for government allowances provided for blindness in Kuwait.[69,70]
It is worthy to note that with other pathologies, women generally put less therapeutic effort in seeking treatment with regard to organ transplants, coronary problems, emergency treatments, and pharmaceutical spending.[71–75] More research would be needed to assess if there are gender differences in therapeutic efforts regarding ophthalmological procedures, and if so, whether those differences could explain why women, despite having had more access to a specialist in high-income countries, had higher prevalence of blindness and visual impairment than men.
Sex differences in the distribution of pathologies that cause blindness and visual impairment were not broadly described.[76,77] (It should be clarified that sex refers to the biological construct/characteristics, whereas gender is a social construct concerning behaviors, roles, and interactions between men and women.) Genetic, hormonal, and other biological factors associated with ocular pathologies could lead women to greater risk of blindness and visual impairment. Reporting sex-stratified data in publications could allow more accurate knowledge on gender inequalities. However, biological factors cannot be considered alone.[78]
Income, educational level, and social class measure socioeconomic position and act in similar, although not equal, ways to produce visual impairment and blindness. More research should be done to understand performance and how influences vary in relation to visual outcomes. Although only a few articles addressed the association of blindness or visual impairment and income, the results consistently showed correlation between lower income and higher risk for visual problems. However, even when considering that women were at a significantly greater risk of developing visual impairment or blindness, none of the articles analyzed in this review stratified association of income and visual outcomes by sex. There were more articles that disaggregated the prevalence of visual impairment and blindness according to level of education, rather than income. Educational level was associated with knowledge and awareness of eye conditions and eye care services and poor behavior toward eye care, but education might have a different effect than income in seeking eye care when needed.[79] However, more research is needed to identify whether lack of knowledge and poor behavior explains this association or if other socioeconomic factors can be implicated. Complex behavior in seeking and receiving eye care services may be embedded in socioeconomic determinants, and more research needs to be done to confirm those findings.[80–82]
The father's social class at time of birth of an individual had a direct effect on that individual's embodiment of social class and affected middle-age risk of developing visual impairment.[51] However, more research is required for measuring the direct or reverse effect of blindness and socioeconomic position, as well as the role of gender.
While many studies demonstrated that ethnic or racial groups have a different prevalence of visual impairment, often due to specific eye diseases, it can be difficult to ascertain how much was intrinsic to the race or ethnicity and how much was associated to socioeconomic position or the lack of eye care for various reasons. More sophisticated research will be needed to determine this conclusion.
Eye care inequities exist in a variety of ways around the world. While some studies suggested that eye care access is a major barrier even in the presence of national health care systems, substantial numbers of subjects did not utilize services where they were available.[37,53,83] In these instances, the lack of education and perhaps more importantly, the lack of basic literacy and/or knowledge of eye diseases provide some explanation.[84] Poverty by itself or combined with educational factors (social deprivation) is also another reason why many patients cannot access services.
As a final note to the discussion, a limitation of the review was that most of the publications were not correctly tagged with adequate keywords when searching for inequalities. As a recommendation, it would be important that future publications should be classified in terms of inequities or social determinants in order to facilitate knowledge-sharing of work that has already been produced.
More research and interpretation needs to be done to better understand the social and biological mechanisms that produce the social inequalities patterns in the prevalence of blindness and visual impairment. Publications, even those not focused on inequalities, should stratify and interpret findings separately by sex and socioeconomic status to provide better understanding of gender inequalities. Associations with determinants of socioeconomic and political context should be further explored.
Acknowledgments
We acknowledge the financial support of ORBIS International in the preparation of this manuscript.[85]
Footnotes
Source of Support: ORBIS International
Conflict of Interest: Rius: none; Lansingh: employee of the International Association for the Prevention of Blindness (IAPB); Guisasola: none; Carter: paid consultant to IAPB; Eckert: paid consultant to Strategic Solutions
References
- 1.Whitehead M. The concepts and principles of equity and health. Int J Health Serv. 1992;22:429–45. doi: 10.2190/986L-LHQ6-2VTE-YRRN. [DOI] [PubMed] [Google Scholar]
- 2.People's Health Movement. People's Charter for Health [Internet] c2012. [Last cited on 2012 Feb 9]. Available from: http://www.phmovement.org/sites/www.phmovement.org/files/phm-pch-english.pdf .
- 3.Marmot MG. Policy making with healthy equity at its heart. JAMA. 2012;307:2033–4. doi: 10.1001/jama.2012.3534. [DOI] [PubMed] [Google Scholar]
- 4.Marmot MG. Understanding social inequalities in health. Perspect Biol Med. 2003;46(3 Suppl):S9–23. [PubMed] [Google Scholar]
- 5.Closing the gap in a generation: Health equity through action on the social determinants of health. Geneva: WHO; c2008. [Last cited on 2012 May 22]. Commission on Social Determinants of Health [Internet] Available from: http://www.who.int/social_determinants/thecommission/finalreport/en/index.html . [DOI] [PubMed] [Google Scholar]
- 6.Solar O, Irwin AS. Social determinants of health discussion paper 2 (Policy and Practice) Geneva: World Health Organization; 2010. A conceptual framework for action on the social determinants of health. [Google Scholar]
- 7.Dandona R, Dandona L. Socioeconomic status and blindness. Br J Ophthalmol. 2001;85:1484–8. doi: 10.1136/bjo.85.12.1484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abou-Gareeb I, Lewallen S, Bassett K, Courtright P. Gender and blindness: A meta-analysis of population-based prevalence surveys. Ophthalmic Epidemiol. 2001;8:39–56. doi: 10.1076/opep.8.1.39.1540. [DOI] [PubMed] [Google Scholar]
- 9.Kyari F, Gudlavalleti MV, Sivsubramaniam S, Gilbert CE, Abdull MM, Entekume G, et al. Prevalence of blindness and visual impairment in Nigeria: The national blindness and visual Impairment Study. Invest Ophthalmol Vis Sci. 2009;50:2033–9. doi: 10.1167/iovs.08-3133. [DOI] [PubMed] [Google Scholar]
- 10.Berhane Y, Worku A, Bejiga A, Adamu L, Alemayehu W, Bedri A, et al. Prevalence and causes of blindness and low vision in Ethiopia. Ethiop J Health Dev. 2007;21:204–10. [Google Scholar]
- 11.Cedrone C, Nucci C, Scuderi G, Ricci F, Cerulli A, Culasso F. Prevalence of blindness and low vision in an Italian population: A comparison with other European studies. Eye (Lond) 2006;20:661–7. doi: 10.1038/sj.eye.6701934. [DOI] [PubMed] [Google Scholar]
- 12.Istituto Nazionale di Statistica. ‘Condizioni di salute e ricorso ai servizi sanitari’ Anni 1999–2000. Roma, Italia: ISTAT; 2002. Indagine multiscopo sulle famiglie. [Google Scholar]
- 13.Gunnlaugsdottir E, Arnarsson A, Jonasson F. Prevalence and causes of visual impairment and blindness in Icelanders aged 50 years and older: The Reykjavik eye study. Acta Ophthalmol. 2008;86:778–85. doi: 10.1111/j.1755-3768.2008.01191.x. [DOI] [PubMed] [Google Scholar]
- 14.Laitinen A, Koskinen S, Härkänen T, Reunanen A, Laatikainen L, Aromaa A. A nationwide population-based survey on visual acuity, near vision, and self-reported visual function in the adult population in Finland. Ophthalmology. 2005;112:2227–37. doi: 10.1016/j.ophtha.2005.09.010. [DOI] [PubMed] [Google Scholar]
- 15.Mganga H, Lewallen S, Courtright P. Overcoming gender inequity in prevention of blindness and visual impairment in Africa. Middle East Afr J Ophthalmol. 2011;18:98–101. doi: 10.4103/0974-9233.80695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.United Nations Development Program [Internet] Human Development Index (HDI) c2012. [Last cited on 2012 Feb 10]. Available from: http://hdr.undp.org/en/statistics/hdi/
- 17.Zhang X, Saaddine JB, Lee PP, Grabowski DC, Kanjilal S, Duenas MR, et al. Eye care in the United States: Do we deliver to high-risk people who can benefit most from it? Arch Ophthalmol. 2007;125:411–8. doi: 10.1001/archopht.125.3.411. [DOI] [PubMed] [Google Scholar]
- 18.Tseng CL, Sambamoorthi U, Rajan M, Tiwari A, Frayne S, Findley P, et al. Are there gender differences in diabetes care among elderly Medicare enrolled veterans? J Gen Intern Med. 2006;21(Suppl 3):47–53. doi: 10.1111/j.1525-1497.2006.00374.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Harris B, Sampson G. Gender differences in the utilisation of optometric services in Victoria. Clin Exp Optom. 2005;88:109–12. doi: 10.1111/j.1444-0938.2005.tb06676.x. [DOI] [PubMed] [Google Scholar]
- 20.Stang A, Jöckel KH. Visual disturbances in a population-based survey of 6962 subjects: The German national health examination survey 1998. Eur J Public Health. 2003;13:202–9. doi: 10.1093/eurpub/13.3.202. [DOI] [PubMed] [Google Scholar]
- 21.Lee DJ, Lam BL, Arora S, Arheart KL, McCollister KE, Zheng DD, et al. Reported eye care utilization and health insurance status among US adults. Arch Ophthalmol. 2009;127:303–10. doi: 10.1001/archophthalmol.2008.567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Khandekar R, Mohammed AJ. Gender inequality in vision loss and eye diseases: Evidence from the Sultanate of Oman. Indian J Ophthalmol. 2009;57:443–9. doi: 10.4103/0301-4738.57153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Carter MJ, Limburg H, Lansingh VC, Silva JC, Resnikoff S. Do gender inequities exist in cataract surgical coverage. Meta-analysis in Latin America? Clin Experiment Ophthalmol. 2012;40:458–66. doi: 10.1111/j.1442-9071.2011.02722.x. [DOI] [PubMed] [Google Scholar]
- 24.Brilliant CE, Lepkowski JM, Zwita B, Thulasiraj RD. Social determinants of cataract surgery utilization in South India. Arch Ophthalmol. 1991;109:584–9. doi: 10.1001/archopht.1991.01080040152048. [DOI] [PubMed] [Google Scholar]
- 25.Fletcher AE, Monoghue M, Devavaram J, Thulasiraj RD, Scott S, Abdallah M, et al. Low uptake of eye services in rural India. Arch Ophthalmol. 1999;117:1393–9. doi: 10.1001/archopht.117.10.1393. [DOI] [PubMed] [Google Scholar]
- 26.Upadhyay MP. Rethinking eye care: From exclusion to equity. Nepal J Ophthalmol. 2010;2:1–2. doi: 10.3126/nepjoph.v2i1.3696. [DOI] [PubMed] [Google Scholar]
- 27.Lewallen S, Mousa A, Bassett K, Courtright P. Cataract surgical coverage remains lower in women. Br J Ophthalmol. 2009;93:295–8. doi: 10.1136/bjo.2008.140301. [DOI] [PubMed] [Google Scholar]
- 28.Nirmalan PK, Padmavathi A, Thulasiraj RD. Sex inequities in cataract blindness burden and surgical services in south India. Br J Ophthalmol. 2003;87:847–9. doi: 10.1136/bjo.87.7.847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nkomazana O. Disparity in access to cataract surgical services leads to higher prevalence of blindness in women as compared to men: Results of a national survey of visual impairment. Health Care Women Int. 2009;30:228–9. doi: 10.1080/07399330802662010. [DOI] [PubMed] [Google Scholar]
- 30.Centers for Disease Control and Prevention. Reasons for not seeking eye care among adults aged ≥40 years with moderate-to-severe visual impairment-21 States, 2006-2009. MMWR Morb Mortal Wkly Rep. 2011;60:610–3. [PubMed] [Google Scholar]
- 31.Melese M, Alemayehu W, Friedlander E, Courtright P. Indirect costs associated with accessing eye care services as a barrier to service use in Ethiopia. Trop Med Int Health. 2004;9:426–31. doi: 10.1111/j.1365-3156.2004.01205.x. [DOI] [PubMed] [Google Scholar]
- 32.Fouad D, Mousa A, Courtright P. Sociodemographic characteristics associated with blindness in a Nile Delta governorate of Egypt. Br J Ophthalmol. 2004;88:614–8. doi: 10.1136/bjo.2003.026997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Brezin AP, Lafuma A, Fagnani F, Mesbah M, Berdeaux G. Prevalence and burden of self-reported blindness, low vision, and visual impairment in the French community: A nationwide survey. Arch Ophthalmol. 2005;123:1117–24. doi: 10.1001/archopht.123.8.1117. [DOI] [PubMed] [Google Scholar]
- 34.Frick KD, Gower EW, Kempen JH, Wolff JL. Economic impact of visual impairment and blindness in the United States. Arch Ophthalmol. 2007;125:544–50. doi: 10.1001/archopht.125.4.544. [DOI] [PubMed] [Google Scholar]
- 35.Kuper H, Polack S, Eusebio C, Mathenge W, Wadud Z, Foster A. A case-control study to assess the relationship between poverty and visual impairment from cataract in Kenya, the Philippines, and Bangladesh. PLoS Med. 2008;5:e244. doi: 10.1371/journal.pmed.0050244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dandona L, Dandona R, Srinivas M, Giridhar P, Vilas K, Prasad MN, et al. Blindness in the Indian state of Andhra Pradesh. Invest Ophthalmol Vis Sci. 2001;42:908–16. [PubMed] [Google Scholar]
- 37.Wilson CJ, Rust G, Levine R, Alema-Mensah E. Disparities in vision impairment Among adults in the United States. Ethn Dis. 2008;18(Suppl 2):S242–6. [PubMed] [Google Scholar]
- 38.Salive ME, Guralnik J, Christen W, Glynn RJ, Colsher P, Ostfeld AM. Functional blindness and visual impairment in older adults from three communities. Ophthalmology. 1992;99:1840–7. doi: 10.1016/s0161-6420(92)31715-4. [DOI] [PubMed] [Google Scholar]
- 39.Bailey RN, Indian RW, Zhang X, Geiss LS, Duenas MR, Saaddine JB. Visual impairment and eye care among older adults - five States, 2005. MMWR Morb Mortal Wkly Rep. 2006;55:1321–5. [PubMed] [Google Scholar]
- 40.Tielsch JM, Sommer A, Katz J, Quigley H, Ezrine S. Socioeconomic status and visual impairment Among urban Americans.Baltimore Eye Survey Research Group. Arch Ophthalmol. 1991;109:637–41. doi: 10.1001/archopht.1991.01080050051027. [DOI] [PubMed] [Google Scholar]
- 41.Livingston PM, McCarty CA, Taylor HR. Visual impairment and socioeconomic factors. Br J Ophthalmol. 1997;81:574–7. doi: 10.1136/bjo.81.7.574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Resnikoff S, Pascolini D, Etya’ale D, Kocur I, Pararajasegaram R, Pokharel GP, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–51. [PMC free article] [PubMed] [Google Scholar]
- 43.Ho VH, Schwab IR. Social economic development in the global prevention of blindness. Br J Ophthalmol. 2001;85:653–7. doi: 10.1136/bjo.85.6.653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Liu JH, Cheng CY, Chen SJ, Lee FL. Visual impairment in a Taiwanese population: Prevalence, causes, and socioeconomic factors. Ophthalmic Epidemiol. 2001;8:339–50. doi: 10.1080/09286586.2001.11644261. [DOI] [PubMed] [Google Scholar]
- 45.Ryskulova A, Turczyn K, Makuc DM, Cotch MF, Klein RJ, Janiszewski R. Self-reported age-related eye diseases and visual impairment in the United States: Results of the 2002 national health interview survey. Am J Public Health. 2008;98:454–61. doi: 10.2105/AJPH.2006.098202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Murthy GV, Gupta SK, Bachani D, Jose R, John N. Current estimates of blindness in India. Br J Ophthalmol. 2005;89:257–60. doi: 10.1136/bjo.2004.056937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Song W, Sun X, Shao Z, Zhou X, Kang Y, Sui H, et al. Prevalence and causes of visual impairment in a rural North-east China adult population: A population-based survey in Bin County, Harbin. Acta Ophthalmol. 2010;88:669–74. doi: 10.1111/j.1755-3768.2009.01768.x. [DOI] [PubMed] [Google Scholar]
- 48.Jadoon MZ, Dineen B, Bourne RR, Shah SP, Khan MA, Johnson GJ, et al. Prevalence of blindness and visual impairment in Pakistan: The Pakistan National Blindness and Visual Impairment Survey. Invest Ophthalmol Vis Sci. 2006;47:4749–55. doi: 10.1167/iovs.06-0374. [DOI] [PubMed] [Google Scholar]
- 49.Entekume G, Patel J, Sivasubramaniam S, Gilbert CE, Ezelum CC, Murthy GV, et al. Prevalence, causes, and risk factors for functional low vision in Nigeria: Results from the national survey of blindness and visual impairment. Invest Ophthalmol Vis Sci. 2011;52:6714–9. doi: 10.1167/iovs.11-7293. [DOI] [PubMed] [Google Scholar]
- 50.Mojon-Azzi SM, Sousa-Poza A, Mojon DS. Impact of low vision on employment. Ophthalmologica. 2010;224:381–8. doi: 10.1159/000316688. [DOI] [PubMed] [Google Scholar]
- 51.Alonso J. Una propuesta de medida de la clase social. Aten Primaria. 2000;25:132–51. Spanish. [PubMed] [Google Scholar]
- 52.Rahi JS, Cumberland PM, Peckham CS. Visual function in working-age adults: Early life influences and associations with health and social outcomes. Ophthalmology. 2009;116:1866–71. doi: 10.1016/j.ophtha.2009.03.007. [DOI] [PubMed] [Google Scholar]
- 53.Varma R, Chung J, Foong AW, Torres M, Choudhury F, Azen SP. Four-year incidence and progression of visual impairment in Latinos: The Los Angeles Latino Eye Study. Am J Ophthalmol. 2010;149:713–27. doi: 10.1016/j.ajo.2009.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Landers J, Henderson T, Craig J. The prevalence and causes of visual impairment in indigenous Australians within central Australia: The central Australian ocular health study. Br J Ophthalmol. 2010;94:1140–4. doi: 10.1136/bjo.2009.168146. [DOI] [PubMed] [Google Scholar]
- 55.Brown AF, Gregg EW, Stevens MR, Karter AJ, Weinberger M, Safford MM, et al. Race, ethnicity, socioeconomic position, and quality of care for adults with diabetes enrolled in managed care. The Translating Research Into Action for Diabetes (TRIAD) study. Diabetes Care. 2005;28:2864–70. doi: 10.2337/diacare.28.12.2864. [DOI] [PubMed] [Google Scholar]
- 56.Bailey RN, Indian RW, Zhang X, Geiss LS, Duenas MR, Saaddine JB. Centers for disease control and prevention.Visual impairment and eye care among older adults - five States, 2005. MMWR Morb Mortal Wkly Rep. 2006;55:1321–5. [PubMed] [Google Scholar]
- 57.Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. doi: 10.1136/bjophthalmol-2011-300539. [DOI] [PubMed] [Google Scholar]
- 58.Ono K, Hiratsuka Y, Murakami A. Global inequity in eye health: Country-level analysis from the global burden of disease study. Am J Public Health. 2010;100:1784–8. doi: 10.2105/AJPH.2009.187930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.London: IAPB; c2012. [Last cited on 2012 Jan 31]. International Agency for the Prevention of Blindness [Internet]. 2010 Report. Available from: http://www.vision2020.org/documents/publications/SotWS%20Report_wth_Stop_Press.pdf . [Google Scholar]
- 60.Pascolini D, Mariotti SP, Pokharel GP, Pararajasegaram R, Etya’ale D, Négrel AD, et al. 2002 global update of available data on visual impairment: A compilation of population-based prevalence studies. Ophthalmic Epidemiol. 2004;11:67–115. doi: 10.1076/opep.11.2.67.28158. [DOI] [PubMed] [Google Scholar]
- 61.Lafuma AJ, Brézin AP, Fagnani FL, Mesbah M, Berdeaux GH. Prevalence of visual impairment in relation to the number of ophthalmologists in a given area: A nationwide approach. Health Qual Life Outcomes. 2006;4:34. doi: 10.1186/1477-7525-4-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Zheng Y, Lamoureux E, Finkelstein E, Wu R, Lavanya R, Chua D, et al. Singapore Eye Research Institute, Singapore National Eye Centre, Singapore.Independent impact of area-level socioeconomic measures on visual impairment. Invest Ophthalmol Vis Sci. 2011;52:8799–805. doi: 10.1167/iovs.11-7700. [DOI] [PubMed] [Google Scholar]
- 63.Sit AJ, Chipman M, Trope GE. Blindness registrations and socioeconomic factors in Canada: An ecologic study. Ophthalmic Epidemiol. 2004;11:199–211. doi: 10.1080/09286580490514504. [DOI] [PubMed] [Google Scholar]
- 64.Krieger N. Methods for the scientific study of discrimination and health: An ecosocial approach. Am J Public Health. 2012;102:936–44. doi: 10.2105/AJPH.2011.300544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Borrell C, Artazcoz L, Gil-González D, Pérez K, Pérez G, Vives-Cases C, et al. Determinants of perceived sexism and their role on the association of sexism with mental health. Women Health. 2011;51:583–603. doi: 10.1080/03630242.2011.608416. [DOI] [PubMed] [Google Scholar]
- 66.Courtright P, Lewallen S. Why are we addressing gender issues in vision loss? Community Eye Health. 2009;22:17–9. [PMC free article] [PubMed] [Google Scholar]
- 67.Artazcoz L, Escribà-Agüir V, Cortès I. [Gender, paid work, domestic chores and health in Spain] Gac Sanit. 2004;18(Suppl 2):24–35. doi: 10.1157/13061992. [DOI] [PubMed] [Google Scholar]
- 68.Saaddine J, Benjamin S, Pan L, Narayan K, Tierney E, Kanjilal S, et al. Prevalence of visual impairment and selected eye diseases among persons aged >/=50 years with and without diabetes-United States, 2002. MMWR Morb Mortal Wkly Rep. 2004;53:1069–71. [PubMed] [Google Scholar]
- 69.Al-Shaaln FF, Bakrman MA, Ibrahim AM, Aljoudi AS. Prevalence and causes of visual impairment among Saudi adults attending primary health care centers in northern Saudi Arabia. Ann Saudi Med. 2011;31:473–80. doi: 10.4103/0256-4947.84624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Al-Merjan JI, Pandova MG, Al-Ghanim M, Al-Wayel A, Al-Mutairi S. Registered blindness and low vision in Kuwait. Ophthalmic Epidemiol. 2005;12:251–7. doi: 10.1080/09286580591005813. [DOI] [PubMed] [Google Scholar]
- 71.Neugarten J, Silbiger SR. The impact of gender on renal transplantation. Transplantation. 1994;58:1145–52. [PubMed] [Google Scholar]
- 72.Schaubel DE, Stewart DE, Morrison HI, Zimmerman DL, Cameron JI, Jeffery JJ, et al. Sex Inequality in kidney transplantation rates. Arch Intern Med. 2000;160:2349–54. doi: 10.1001/archinte.160.15.2349. [DOI] [PubMed] [Google Scholar]
- 73.Steingart RM, Packer M, Hamm P, Coglianese ME, Gersh B, Geltman EM, et al. Sex differences in the management of coronary artery disease. Survival and Ventricular Enlargement Investigators. N Engl J Med. 1991;325:226–30. doi: 10.1056/NEJM199107253250402. [DOI] [PubMed] [Google Scholar]
- 74.Heston TF, Lewis LM. Gender bias in the evaluation and management of acute nontraumatic chest pain. Fam Pract Res J. 1992;12:383–9. [PubMed] [Google Scholar]
- 75.Ruiz-Cantero MT, Verdú-Delgado M. Gender bias in treatment. Gac Sanit. 2004;18(Suppl 1):118–25. doi: 10.1157/13062260. Spanish. [DOI] [PubMed] [Google Scholar]
- 76.Vajaranant TS, Nayak S, Wilensky JT, Joslin CE. Gender and glaucoma: What we know and what we need to know. Curr Opin Ophthalmol. 2010;21:91–9. doi: 10.1097/ICU.0b013e3283360b7e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Chakravarthy U, Wong TY, Fletcher A, Piault E, Evans C, Zlateva G, et al. Clinical risk factors for age-related macular degeneration: A systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31. doi: 10.1186/1471-2415-10-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Krieger N. Embodiment: A conceptual glossary for epidemiology. J Epidemiol Community Health. 2005;59:350–5. doi: 10.1136/jech.2004.024562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Ayanniyi AA, Olatunji FO, Adeboye A, Ayanniyi RO. Awareness and knowledge of eye care providers among government workers in Ilorin, Nigeria. Niger Postgrad Med J. 2010;17:133–7. [PubMed] [Google Scholar]
- 80.Baker RS, Bazargan M, Bazargan-Hejazi S, Calderón JL. Access to vision care in an urban low-income multiethnic population. Ophthalmic Epidemiol. 2005;12:1–12. doi: 10.1080/09286580590921330. [DOI] [PubMed] [Google Scholar]
- 81.Hollands H, Brox AC, Chang A, Adilman S, Chakraborti B, Kliever G, et al. Correctable visual impairment and its impact on quality of life in a marginalized Canadian neighbourhood. Can J Ophthalmol. 2009;44:42–8. doi: 10.3129/i08-167. [DOI] [PubMed] [Google Scholar]
- 82.Ndegwa LK, Karimurio J, Okelo RO, Adala HS. Barriers to utilization of eye care services in Kibera slums of Nairobi. East Afr Med J. 2005;82:506–8. doi: 10.4314/eamj.v82i10.9347. [DOI] [PubMed] [Google Scholar]
- 83.Leese GP, Boyle P, Feng Z, Emslie-Smith A, Ellis JD. Screening uptake in a well-established diabetic retinopathy screening program. Diabetes Care. 2008;31:2131–5. doi: 10.2337/dc08-1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Dandona R, Dandona L, John RK, McCarty CA, Rao GN. Awareness of eye diseases in an urban population in southern India. Bull World Health Organ. 2001;79:96–102. [PMC free article] [PubMed] [Google Scholar]
- 85.Salomao SR, Cinoto RW, Berezovsky A, Araujo-Filho A, Mitsuhiro MR, Mendieta L, et al. Prevalence and causes of vision impairment and blindness in older adults in Brazil: the Sao Paulo Eye Study. Ophthalmic Epidemiol. 2008;15:167–75. doi: 10.1080/09286580701843812. [DOI] [PMC free article] [PubMed] [Google Scholar]