

Abstract
CONTEXT:
Survivors of the Bhopal gas disaster still suffer from various respiratory ailments. We examined the effects of exposures among a cross-section of current residents suffering from COPD by ISSR-PCR.
AIMS:
Molecular screening of the gas-affected population of Bhopal with COPD for microsatellite instability due to exposure of MIC.
SETTINGS AND DESIGN:
The isocyanate-exposed population of Bhopal city suffering from chronic obstructive pulmonary disorder.
MATERIALS AND METHODS:
Inter-(SSR) analysis was used to characterize microsatellite instability in 52 MIC victims of Bhopal, suffering from COPD using (CA)8RG and (CA)8R[Y-Q] primer.
STATISTICAL ANALYSIS USED:
Association analyses were performed using regression analysis.
RESULTS:
The study on the MIC-affected population in Bhopal showed weak association between microsatellite instability and age (r = + 0.37); exposure distance from site (r = −0.44); and smoking status(r = + 0.12); while regression analysis of the above parameters displayed supporting evidence.
CONCLUSIONS:
The high prevalence of smoking coupled with aging and poor living habits threatens, to further increase COPD incidences among this population, highlighting the need for enhanced screening efforts.
Keywords: Bhopal gas tragedy, chronic obstructive pulmonary disorder, genomic instability, inter-(simple sequence repeat), microsatellite
Introduction
An aerial spill of approx. 40 tones of toxic methyl isocyanate (MIC) gas put the entire city of Bhopal to an uncertain future. It is 25 years after this world's biggest industrial disaster, we examined the effects of the gas among a cross-section of current residents suffering from chronic obstructive pulmonary disorder (COPD). It is an ‘umbrella’ term for people with chronic bronchitis, emphysema, or both. Human studies carried out at various periods after an exposure to the toxic gas suggest that COPD is one of the major sequel of this disaster. It is possible that a wide spectrum of lung diseases can result from gas exposure.[1] The etiology of the airway obstruction and emphysematous destruction that cause airflow limitation is the persistent lung tissue injury produced by the chronic inhalation of toxic particles and gases.[2]
Thus, subsequent scientific challenges posed by this have been almost fulfilled by the coordinated studies.[3] Human microsatellites are regions of the genome present between inverted abundant repetitive elements.[4] Inter- (simple sequence repeat) PCR (ISSR-PCR) simultaneously sample numerous diverse regions of the genome.
Subjects with diabetes, acute infection, and respiratory disease other than COPD were excluded beforehand.
Here, we present a molecular overview of the microsatellite banding patterns in patients in relation to age, gender, extent of exposure to gas and other cited stress parameters. In order to investigate this hypothesis, we compared smokers who developed COPD with smokers who did not develop COPD (referred to as non-COPD smokers).
Other causes include occupational exposure to dusts, indoor pollution from wood-burning and coal-burning stoves, air pollution, and certain inherited diseases.[5]
Materials and Methods
Subjects
In this study, molecular screening of 52 gas-victims was evaluated, suffering from mild to severe airway obstruction, medically diagnosed as suffering from COPD. There were 07 severely, 11 moderately, and 34 mildly-affected patients. Their mean age was 55 (range 25-85) years, and 40 patients were males [Table 1]. Smokers with airflow limitation (n = 25), and age-matched control smokers (n = 12) and control never-smokers (n = 07) without airflow limitation were included in the present study. 52 patients (40 males and 12 females) with a history of exposure to toxic gas on 2-3 December, 1984, and presenting with respiratory symptoms, were included in the study.
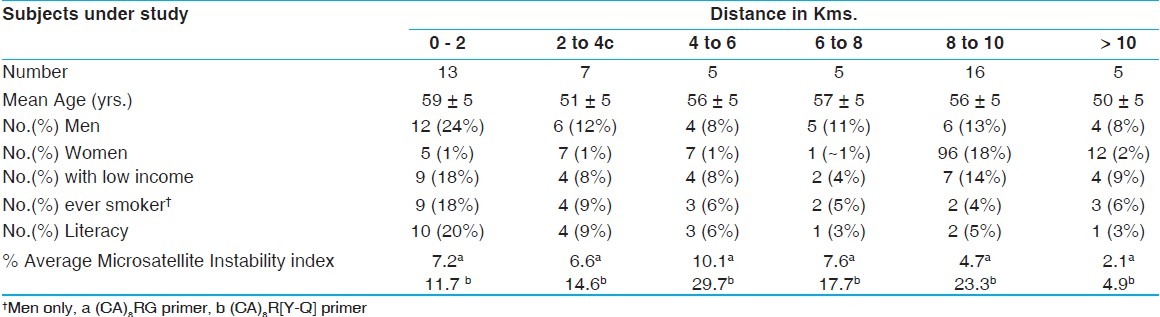
Table 1.
Demographic description of subjects (gas-effected chronic obstructive pulmonary disorder patients) visiting the hospital and various mini-units for treatment, according to distance lived from Union Carbide plant
The main presenting symptoms were cough and dyspnea on exertion. Patients were selected partly from the out-patient clinic exclusively established for toxic gas victims at Bhopal Memorial Hospital and Research Centre, Bhopal, and partly from the patients’ homes, which were visited by the investigators. Each individual was examined by a physician along with a case history to follow-up the patient's progress. Our control populations were of 3 types; namely, normal lungs-no isocyanate exposure, normal lungs and isocyanate-exposed, and COPD with no isocyanate exposure.
A piloted structured questionnaire would be administered in Hindi to enquire into variety of potentially confounding factors including socio-economic variables such as literacy, income, and employment. Literacy was defined as the completion of 8th level in school. A preliminary assessment of the area of exposure and the effects suffered was made by talking to people who lived at varying distances and directions from the plant. From this, it was possible to map out preliminary exposure zones according to reports of human and animal deaths, symptoms, and perceptions of the presence of the gas. Place of residence at the time of the gas leak would be confirmed from official records held by each of those interviewed. Subjects would be defined as dyspneic if they reported breathlessness either when walking on level ground or on climbing hills. Literacy was defined as the completion of at least primary education. Men with low incomes were those with no paid work or a monthly wage of less than 500 rupees.
Classification of Severity of Exposure
The patients were categorized into 3 groups depending upon the severity of exposure of the gas, which were not the same in all subjects. The 3 categories were as follows:
Severe exposure - If 1 member of the family had died due to toxic gas exposure or the patient had severe ophthalmic and respiratory symptoms, including unconsciousness on the day of exposure, requiring immediate hospitalization, the patient was classified as having had severe exposure.
Moderate exposure - Patients with respiratory and ophthalmic symptoms on the day of exposure, requiring only outpatient management, were classified as having had moderate exposure.
Mild exposure - Patients with mild respiratory symptoms on the day of exposure, and not seeking immediate medical relief because of mild symptoms, were classified as having had mild exposure.[6]
Polymorphism of microsatellites was determined in effected COPD patients using (CA)8RG primer and (CA)8R[Y-Q]. COPD was diagnosed in these patients (n = 28) admitted at Bhopal Memorial Hospital and Research Centre (BMHRC). Control group included age-matched control smokers (n = 22) and control never-smokers (n = 20). The patients were divided into sex- and age-matched groups (40-85 years). DNA was isolated from 5 ml blood collected in EDTA containing vacutainers, using DNA isolation kit for mammalian blood (QIAmp DNA Blood Maxi and Mini kits; QIAGEN, Inc., Valencia, CA, USA). DNA samples were stored at -20°C (Roche version 3). Microsatellite inter- (short sequence repeats) polymorphism was studied using polymerase chain reaction (PCR- PTC-200 thermal cycler, M.J. Research, Inc., Watertown, MA, USA) as described elsewhere.[7]
Inter-(Simple-Sequence-Repeat) PCR
The inter-SSR PCR method and its reproducibility in multiple independent assays have been described.[4,7,8] Dinucleotide repeats and anchored at the 3’ end by two no repeat nucleotides were used in a PCR to amplify the sets of genomic sequences present between the repeat elements. PCR was in a volume of 25 μl containing 100 pM primer, 100 ng genomic DNA, and 0.75 unit of Taq polymerase (Qiagen Taq PCR Core Kit -QIAGEN, Inc.) in 1× PCR buffer (200 mMTris-HCl, pH 8.4, 500 mM KCl). Amplification conditions were a 3-min initial denaturation at 94°C, followed by 35 cycles of (30 s at 94°C denaturation, 30 s at 52°C annealing, and 2 min at 72°C elongation), and then a final 7 min at 72°C for extension and terminated at 4°C. The PCR products were analyzed on non-denaturing 7% PAGE at 120 V for 20 min. The gels were then viewed under UV illumination at λ260 nm. The genomic instability index was computed by dividing the number of altered bands seen in the PCR products amplified from the COPD patients by the total number of products generated from the corresponding normal tissue DNA.
Ethics
Institutional Research Ethics Committee of the hospital approved the present study, and patients gave their informed consent.
Statistical Analysis
Genomic instability index results in normal subjects and patients were compared using ± SD, correlation, and χ2-test. The relationship between genomic instability index and age along with patients’ age, exposure distance in kms., and smoking history was analyzed using regression analysis.
The possibility that the exposed population at a later date may develop some hitherto unsuspected complications cannot be ruled out, the study has said, adding that there is an urgent need for keeping the exposed population under constant medical surveillance.
Results
A total of 528 methyl isocyanate-exposed COPD patients with mean ± SD 31 years with an average mean age of 59 years were studied. Of them, only 46% were literate, and 61% of the sampled population belonged to very low-income level. Only men were smokers consuming approximately 10 cigarettes per day, comprising of 48% of the sampled population [Table 1].
The microsatellite banding pattern with (CA)8RG primer revealed a banding pattern of COPD patients when compared to that of control was found to match control viz. COPD and no isocyanate-exposed [Figure 1]. On the other hand, (CA)8R[Y-Q] generated a banding pattern similar to that of isocyanate-exposed and normal lung control [Figure 2].
Figure 1.
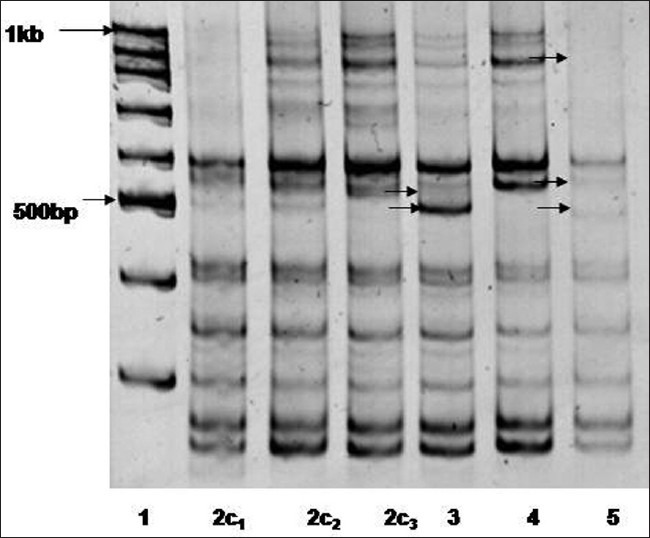
Microsatellite instability displayed using (CA)8RG microsatellite primer in MIC-gas victim with chronic obstructive pulmonary disorder (lane 3-5) as compared to non gas-exposed with normal lung functioning (lane 2c1), non gas-victim with COPD (lane2c2) and gas-victim with normal lung functioning (lane 2c3) ; lane 1 is 100 bp marker
Figure 2.
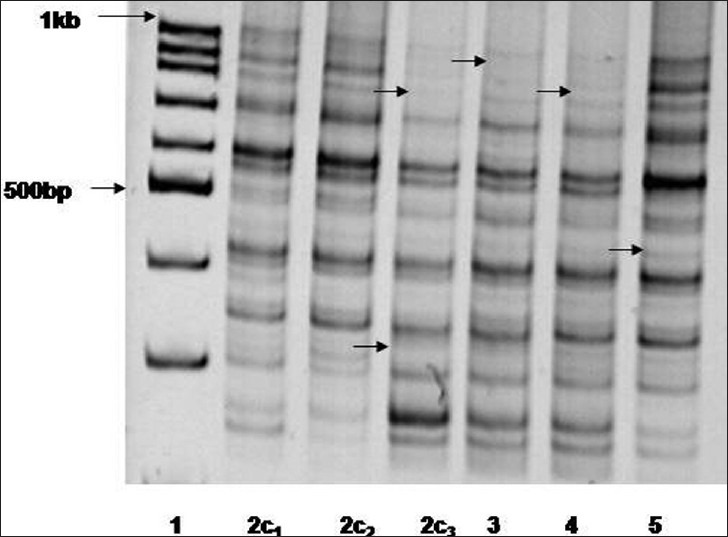
Microsatellite instability displayed using (CA)8R[Y-Q] microsatellite primer in MIC-gas victim with chronic obstructive pulmonary disorder (lane 3-5) as compared to non gas-exposed with normal lung functioning (lane 2c1), non gas-victim with COPD (lane2c2) and gas-victim with normal lung functioning (lane 2c3); lane 1 is 100 bp marker
Thus, from the above observations in the former case, altered bands were attributed to age, smoking history, and various other socio-economic factors. Whereas, alterations with the later primer might be due to stress factors associated with MIC gas spread combined with other factors viz. alcohol consumption, other eating and living habits, health condition etc.
On statistical analysis of the existing data, there existed a positive correlation +0.37 and +0.11 between percent MSI vs. age and smoking habits of patients, a negative correlation (−0.44) between exposure distance and percent MSI [Figure 3].
Figure 3.
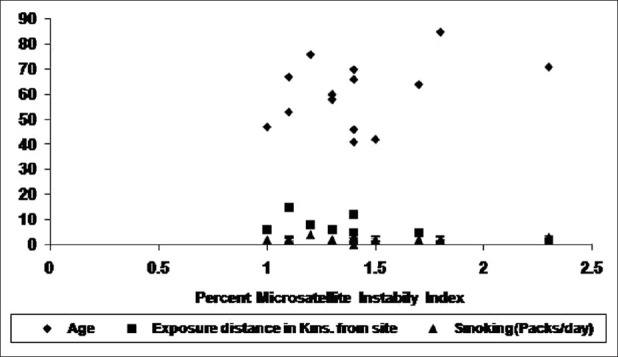
Percent Microsatellite Instability -its association with age, exposure distance, smoking parameter of gas victims with chronic obstructive pulmonary disorder
The association between percent microsatellite instability, age, exposure distance, and smoking status was statistically significant for both the primers as depicted on χ2 analysis at 0.05 P value. These displayed a linear trend as ascertained by equation yAge = 14.602x + 39.673, yExposure Dist. = -5.2269x + 12.93, and ySmoking = 0.2977x + 1.7911 at P, 0.05 [Figure 4]. The slope was found out to be 0.009, 0.042, and −0.04 for age, smoking status, and exposure distance respectively against percent MSI.
Figure 4.
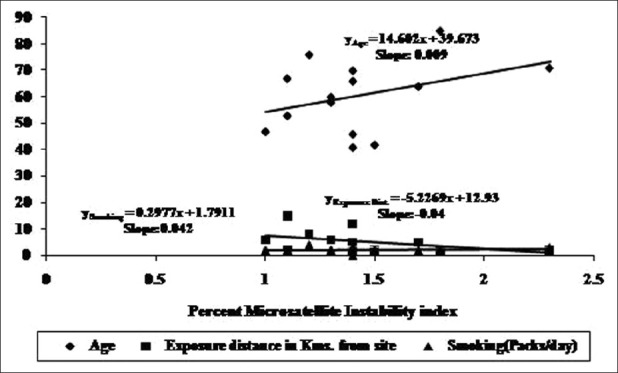
Regression analysis of various factors effecting microsatellite instability in gas-victims with chronic obstructive pulmonary disorder
The lung is probably the critical target organ for long-term effects from acute exposure, although adverse effects on other organs (e.g., eye, reproductive, and gastrointestinal) also exist. The chemical identity of the ultimate toxicant MIC is unknown and may be more than one of its intermediates.[9] Cigarette smoking initiates a disease process by producing progressive irreversible damage. In this case, the total effect would be approximately proportional to the total accumulated dosage experienced over the years. Cessation of smoking leaves impaired function, which does not improve appreciably but does not continue to deteriorate from continued exposure to cigarette smoke. However, such function may deteriorate through aging or through exposure to other harmful agents. It appears that such a relationship probably exists for chronic obstructive lung disease.
In conclusion, the instability of the microsatellite sequences that have been investigated indicates a destabilization of the genome in chronic obstructive pulmonary disease patients. Oxidative stress due to smoking, residence, or work place near plant area may damage the DNA of lung cells, probably at the microsatellite level, leading to acquired somatic mutations. These mutations, expressed as microsatellite instability, permanently alter DNA auto-repair ability.[10]
Thus, in addition to exposure to exogenous factors, like air pollution and work conditions, several host factors such as health status, eating habits, socio-economic conditions are important in determining whether smokers develop lung disease. It has not been established whether these “susceptible” smokers who develop COPD are genetically predetermined or whether environmental (type of tobacco), dietary, or other factors affect the development of the disease. In addition, the genetic basis of COPD is poorly understood.[11]
Studies on MIC-exposed subjects at Bhopal revealed that incidences of lung-related ailments such as asthma, chronic obstructive pulmonary disorder, pulmonary fibrosis were on the rise as time passed.
Smoking along with age, health condition, eating habits, socio-economic status is to blame for COPD in the majority of cases. Smoke from cigarettes causes inflammation in the lungs and destroys the elasticity that allows the lungs to expand and contract as we breathe.
Exposure to MIC was studied as the distance of residence from the plant site. The frequency of symptoms fell as exposure to the gas leak from factory site increased. These findings were further fortified by detail questionnaires accounting for and confounding to factors like smoking, literacy, socio-economic status, and gender, which cannot be ignored.
Therefore, we hypothesize that this genetic alteration may be one of the late effects of the killer gas MIC, thereby increasing the susceptibility to COPD, especially in the gas-hit population of Bhopal. In conclusion, the results of this study showed that MSI is strongly associated with smoking, age, and exposure to isocyanates toxicity, which are instrumental in causing progression in COPD. Therefore, MSI may be a useful marker of the genetic alteration leading to COPD. We anticipate these data along with other studies reported in the literature would help to design better approaches in risk assessment of occupational and accidental exposure to isocyanates.
Acknowledgments
The authors thank the gas-effected patients for their participation in this study and Bhopal Memorial Research Centre, Bhopal for the necessary financial assistance and infrastructure.
Footnotes
Source of Support: Bhopal Memorial Research Centre, Bhopal
Conflict of Interest: No
References
- 1.Vijayan VK. Toxic trauma affecting the lungs with special reference to the Bhopal Disaster. Pulmon. 2006;8:43–50. [Google Scholar]
- 2.Curtis JL, Freeman CM, Hogg JC. The Immunopathogenesis of chronic obstructive pulmonary disease insights from recent research. Proc Am Thorac Soc. 2007;4:512–21. doi: 10.1513/pats.200701-002FM. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sriramachari S. The Bhopal gas tragedy. An environmental disaster. Curr Sci. 2004;86(7):905–920. [Google Scholar]
- 4.Basik M, Stoler DL, Kontzoglou KC, Rodriguez-Bigas MA, Petrelli NJ, Anderson GR. Genomic instability in sporadic colorectal cancer quantitated by inter- (simple sequence repeat) PCR analysis. Genes Chromosomes Cancer. 1997;18:19–29. [PubMed] [Google Scholar]
- 5. http://www.britishlungfoundation.org.uk .
- 6.Vijayan VK, Sankaran K. Relationship between lung inflammation, changes in lung function and severity of exposure in victims of the Bhopal tragedy. Eur Respir J. 1996;9(10):1977–82. doi: 10.1183/09031936.96.09101977. [DOI] [PubMed] [Google Scholar]
- 7.Stoler DL, Chen N, Basik M, Kahlenberg MS, Rodriguez-Bigas MA, Petrelli NJ, et al. The onset and extent of genomic instability in sporadic colorectal tumor progression. Proc Natl Acad Sci U S A. 1999;96:15121–6. doi: 10.1073/pnas.96.26.15121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kahlenberg MS, Stoler DL, Basik M, Petrelli NJ, Rodriguez-Bigas M, Anderson GR. p53 tumor suppressor gene status and the degree of genomic instability in sporadic colorectal cancers. J Natl Cancer Inst. 1996;88:1665–70. doi: 10.1093/jnci/88.22.1665. [DOI] [PubMed] [Google Scholar]
- 9.Vijayan VK, Sankaran K, Sharma SK, Misra NP. Chronic lung inflammation in victims of toxic gas leak at Bhopal. Respir Med. 1995;89:105–11. doi: 10.1016/0954-6111(95)90192-2. [DOI] [PubMed] [Google Scholar]
- 10.Siafakas NM. “In the Beginning” of COPD. Is evolution important? Am J Respir Crit Care Med. 2007;175:1–2. doi: 10.1164/rccm.200612-1800ED. [DOI] [PubMed] [Google Scholar]
- 11.Siafakas NM, Tzortzaki EG, Sourvinos GD, Bouros N, Tzanakis-Kafatos A, Spandidos D. Microsatellite DNA Instability in COPD. Chest. 1999;116:47–51. doi: 10.1378/chest.116.1.47. [DOI] [PubMed] [Google Scholar]