

Summary
Background
The nonselective 5-HT4 receptor agonists, cisapride and tegaserod have been associated with cardiovascular adverse events (AEs).
Aim
To perform a systematic review of the safety profile, particularly cardiovascular, of 5-HT4 agonists developed for gastrointestinal disorders, and a nonsystematic summary of their pharmacology and clinical efficacy.
Methods
Articles reporting data on cisapride, clebopride, prucalopride, mosapride, renzapride, tegaserod, TD-5108 (velusetrag) and ATI-7505 (naronapride) were identified through a systematic search of the Cochrane Library, Medline, Embase and Toxfile. Abstracts from UEGW 2006–2008 and DDW 2008–2010 were searched for these drug names, and pharmaceutical companies approached to provide unpublished data.
Results
Retrieved articles on pharmacokinetics, human pharmacodynamics and clinical data with these 5-HT4 agonists, are reviewed and summarised nonsystematically. Articles relating to cardiac safety and tolerability of these agents, including any relevant case reports, are reported systematically.
Two nonselective 5-HT4 agonists had reports of cardiovascular AEs: cisapride (QT prolongation) and tegaserod (ischaemia). Interactions with, respectively, the hERG cardiac potassium channel and 5-HT1 receptor subtypes have been suggested to account for these effects. No cardiovascular safety concerns were reported for the newer, selective 5-HT4 agonists prucalopride, velusetrag, naronapride, or for nonselective 5-HT4 agonists with no hERG or 5-HT1 affinity (renzapride, clebopride, mosapride).
Conclusions
5-HT4 agonists for GI disorders differ in chemical structure and selectivity for 5-HT4 receptors. Selectivity for 5-HT4 over non-5-HT4 receptors may influence the agent's safety and overall risk–benefit profile. Based on available evidence, highly selective 5-HT4 agonists may offer improved safety to treat patients with impaired GI motility.
Introduction
Disorders of gastrointestinal (GI) motility are considered a major pathophysiological mechanism underlying symptoms of functional GI disorders.2008 Therapeutic agents have been designed to stimulate muscle activity to address the underlying hypomotility associated with disorders such as slow-transit constipation, gastroparesis and ineffective oesophageal motility.2008 Activation of 5-HT4 receptors on cholinergic nerve endings in the enteric nervous system enhances the release of acetylcholine from motor neurons, thereby stimulating GI propulsive motility.2, 3 From these pharmacological observations, 5-HT4 receptor agonists have been developed for the treatment of hypomotility disorders. Nonselective 5-HT4 receptor agonists such as cisapride and tegaserod were successfully developed for the treatment of hypomotility disorders of the upper and lower GI tract, respectively.4, 5 Although both drugs saw broad clinical use, they were associated with cardiovascular adverse events (AEs).6, 7, 8 Cisapride was subsequently withdrawn from the global market in 2000 and, since 2009, tegaserod, which never received approval in the European Union (EU), has been limited to emergency use in the United States.9, 10 These cardiovascular AEs, which may be more related to a lack of selectivity of certain compounds or classes of compounds, rather than to genuine 5-HT4 receptor-mediated effects, have strongly impacted the perceived risk–benefit ratio of 5-HT4 receptor agonists. Meanwhile, a newer generation of selective 5-HT4 receptor agonists is being developed for the treatment of GI motility disorders. In this article, we review the safety profile of older and newer 5-HT4 receptor agonists developed for GI disorders, focusing on their cardiovascular risk profile.
Pharmacology of 5-HT4 Receptor Agonists
Structure of 5-HT4 receptors
5-HT4 receptors are heptahelical receptors, which primarily couple to the stimulatory protein Gs and activate the 3′,5′ cyclic adenosine monophosphate-dependent protein kinase A pathway.11, 12 Most of the 5-HT4 receptor splice variants are identical up to leucine 358, but their intracellular C-terminal tails differ.1998 The splice variants 5-HT4(a) and 5-HT4(b) have been found in all species studied thus far, with 5-HT4(b) being the dominant splice variant in human tissues.2001 Additional splice variants have also been identified in human (h5-HT4(c), h5-HT4(d), h5-HT4(g), h5-HT4(i) and h5-HT4(n)), mouse (m5-HT4(e) and m5-HT4(f)) and rat (r5-HT4(c1) and r5-HT4(e))13, 15, 16 and more recently in porcine tissue.2008 The physiological implication of the multitude of splice variants and their differential coupling to signal transduction cascades remains unclear.
Furthermore, several observations suggest that there is cell type-, tissue-specific or disease-state-specific expression (e.g. in gastroparesis) of certain splice variants.13, 18, 19, 20, 21 However, currently, there are no drugs which reliably discriminate among 5-HT4 receptor splice variants, but such drugs could provide an interesting alternative opportunity for tissue-specific drug targeting.
Tissue distribution of 5-HT4 receptors
5-HT4 receptors are localised to neurons in the central nervous system, including the prefrontal cortex,22, 23 hippocampus12, 22 and mesolimbic and nigrostriatal dopamine systems.2007 Functional 5-HT4 receptors are also found in the GI tract, bladder and heart.25, 26, 3
In the GI tract, 5-HT4 receptors are expressed in enteric neurons2008 as well as smooth muscle cells.28, 29, 30 As a major consequence of 5-HT4 receptor activation, acetylcholine is released from interneurons and motor neurons, thus increasing propulsive motility.30–37
Classes of 5-HT4 receptor agonists
Several different classes of 5-HT4 receptor agonists have been developed for the treatment of GI disorders. We review those classes here, focusing on their affinity and selectivity for the 5-HT4 receptor, as well as any tissue-dependent agonism (partial or full agonism) that might arise (in part) from differences in receptor reserve or coupling efficiency between different tissues.2006 Whether or not a drug is a full or partial agonist in a given tissue may depend on the receptor concentration or the efficiency of the receptor-effector coupling. Thus, it may be feasible to obtain a certain degree of tissue selectivity with a low efficacy agonist or low doses of a high efficacy agonist (in favour of tissues with high receptor reserve for the given agonist, such as the GI tract), as tissues with no receptor reserve for the agonist would not be stimulated by this drug.
Benzamides
The substituted benzamides, including metoclopramide, cisapride, renzapride, mosapride, clebopride and naronapride (ATI-7505) are 5-HT4 receptor agonists with moderate affinity and poor selectivity for the 5-HT4 receptor (Figure 1).1995 Metoclopramide is also an antagonist at D2 dopamine receptors and at 5-HT3 receptors, while cisapride blocks 5-HT2 and 5-HT3 receptors and the human ether-a-go-go-related gene (hERG)-encoded K+ channel.39, 40 The consequences of these interactions are clearer for some than for others; for example, the prolongation of cardiac action potential repolarisation and, thus, QT (the time elapsing from the beginning of the QRS complex to the end of the T wave in an electrocardiogram) interval, due to the blockade of the hERG channel by cisapride, is likely to underlie the arrhythmogenic potential of this nonselective 5-HT4 receptor agonist.7, 41 These non-5-HT4 receptor sites of action, coupled with their tissue-dependent pharmacodynamics, complicate the description of the actions of benzamides in vivo.
Figure 1.
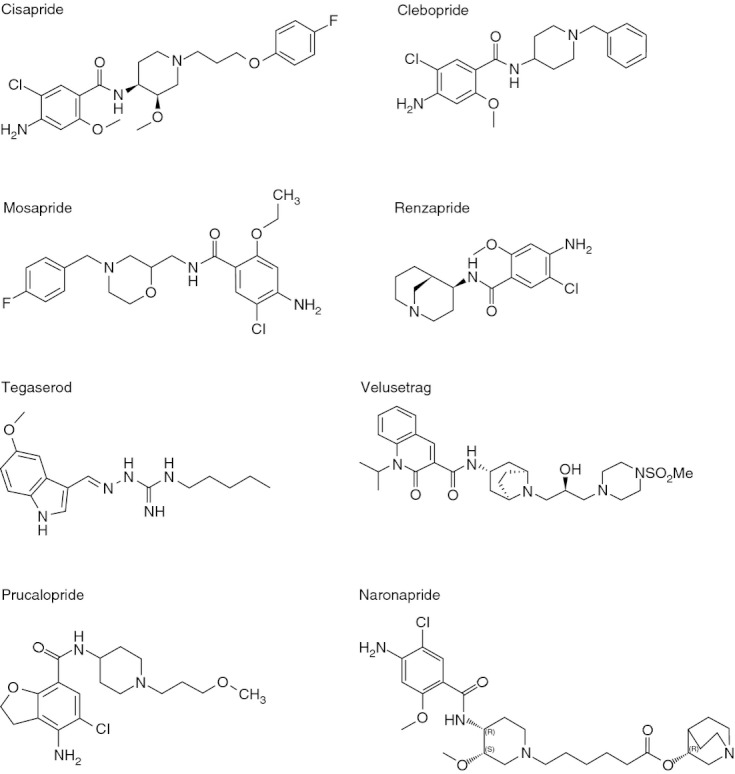
Molecular structure of 5-HT4 agonists.
In the rat oesophagus, 5-HT4 receptors are localised to the muscularis mucosae (smooth muscle), where they mediate relaxation. In this tissue, cisapride, renzapride and mosapride have 80–90% of the intrinsic activity of 5-HT.28, 42 In the guinea-pig distal colon, cisapride, renzapride and mosapride mediate a contractile response and have 80–100% of the intrinsic activity of 5-HT.1993 Therefore, in both the guinea pig colon and rat oesophagus, benzamides are full agonists. In contrast, in the guinea pig ileum, cisapride, renzapride and mosapride have only 50–60% of the intrinsic activity of 5-HT.42, 32 Similarly, cisapride has <60% of the intrinsic activity of 5-HT in relaxing circular muscle strips of the canine rectum.1999
Little preclinical information is available on naronapride, another substituted benzamide 5-HT4 receptor agonist designed to have the same therapeutic benefit as cisapride, but without the side effects. Naronapride is structurally similar, but more selective, than cisapride, with minimal hERG channel activity as well as minimal-to-no activity at 5-HT3 receptors.2007 Naronapride stimulates GI motility in vivo in dogs2004 and in humans.2007
Carbazimidamides
Tegaserod is an indole carbazimidamide agonist with high affinity for the 5-HT4 receptor, but it is also a 5-HT2(a) and 5-HT2(b) receptor antagonist and 5-HT1 receptor agonist (Figure 1).46, 47, 13 The contribution of 5-HT2B receptor antagonism to the therapeutic actions of tegaserod on gut motility remains unknown. Early studies showed that tegaserod facilitates the peristaltic reflex in vitro in human small intestine, and guinea pig and rat colonic preparations.1998 When agonist-evoked contractions of the guinea pig ileum were studied, tegaserod was equipotent with 5-HT, but had only 30% of the intrinsic activity of 5-HT.49, 50 In vitro studies comparing 5-HT4 receptor-mediated relaxation of canine rectal smooth muscle showed that tegaserod was 10-fold less potent than 5-HT and had only 55% of the intrinsic activity of 5-HT.1999 In the porcine stomach, tegaserod had approximately the same intrinsic activity as 5-HT when increases in cholinergic neurogenic contractions were measured.2006 These data indicate that tegaserod is a potent 5-HT4 receptor agonist in all tissues tested. While tegaserod is frequently identified as a partial receptor agonist, this property is tissue-dependent.27, 38
Benzofurancarboxamides
Prucalopride belongs to the class of benzofurancarboxamide agonists, which have high affinity and selectivity for the 5-HT4 receptor, and tissue-specific agonist activity (Figure 1).27, 38 The most pronounced effect of prucalopride is stimulation of colonic motility.50–53 Prucalopride is 10-fold less potent than 5-HT in causing relaxation of canine rectum circular muscle, with 82% of the intrinsic activity of 5-HT.1999 In guinea pig colon, prucalopride is approximately 10-fold less potent than 5-HT in stimulating peristalsis, but was equally effective as 5-HT (i.e. the maximal effect reached at high concentrations is similar to that of 5-HT) in this assay.2001 In vivo, prucalopride dose-dependently stimulated high-amplitude clustered contractions in the proximal colon and inhibited contractile activity in the distal colon.2001 Prucalopride also induced giant migrating contractions, the canine equivalent of mass movements.2001
Other agonists
Velusetrag (TD-5108) is a dihydroquinoline-carboxylic acid derivative that has high affinity and selectivity for 5-HT4 receptors in a number of in vitro assays, and is an effective stimulant of GI motility in vivo (Figure 1). Velusetrag has comparable intrinsic activity with 5-HT in the guinea pig colon and rat oesophagus tunica muscularis mucosa preparations, and has little or no activity at heterologously-expressed sodium channels or potassium channels.2008 Velusetrag is more potent than tegaserod, cisapride and mosapride at stimulating colonic transit in conscious guinea pigs, and approximately equipotent with tegaserod at stimulating small intestinal motility in conscious dogs or relaxing the oesophagus in anaesthetised rats.2008
Several other 5-HT4 receptor agonists have been developed for use in GI disorders, but development has ceased or limited data are available, so they will not be reviewed here. These agents include cinitapride (LAS17177), lintopride (STIL 2875), lirexapride (JL17454/CHF17454), PF885706 and E3620.
Conclusions on pharmacology of 5-HT4 agonists
5-HT4 receptors are a widely expressed and dynamic class of receptors and 5-HT4 receptor agonists are effective stimulants of GI motility. Differences in the pharmacology of 5-HT4 receptor agonists originates mainly from differences in their selectivity for 5-HT4 over other receptor types, such as 5-HT1 and 5-HT2 receptors, and the hERG channel (Table 1), or by their degree of tissue-specific agonism.
Table 1.
Receptor binding profile of 5-HT4 agonists for GI disorders, at therapeutic concentrations
| Receptor binding profile at therapeutic concentrations | ||||||
|---|---|---|---|---|---|---|
| Drug | 5-HT4 | 5-HT3 | 5-HT2 | 5-HT1 | D2 | hERG |
| Cisapride | + | + | + | + | ||
| Tegaserod | + | + | + | + | ||
| Renzapride | + | + | ||||
| Clebopride | + | + | + | |||
| Mosapride | + | + | ||||
| Prucalopride | + | |||||
| Velusetrag | + | |||||
| Naronapride | + | |||||
GI, gastrointestinal.
+ indicates affinity for this receptor (as either agonist or antagonist) that is likely to be clinically relevant at concentrations necessary for 5-HT4 agonism (i.e. for therapeutic action). Information from De Maeyer et al.2008
Methods
The purpose of this review was to comprehensively search and systematically review the evidence on the safety of 5-HT4 receptor agonists developed for GI disorders, with particular reference to cardiovascular safety. Literature on pharmacokinetics, human pharmacodynamics and clinical data was also collected systematically, but summarised nonsystematically and therefore not presented here in full.
An independent researcher at the Royal Society of Medicine Library Search Services performed a comprehensive search of the Cochrane Library (including the Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects, the Cochrane Central Register of Controlled Trials, the Health Technology Assessment Database and the NHS Economic Evaluation Database), Medline (1949 – April 2009), Embase (1974 – April 2009) and ToxFile (1900 – April 2009) in June 2009. The search encompassed all types of clinical trials as well as systematic reviews, meta-analyses and case reports, using the terms ‘cisapride’ OR ‘clebopride’ OR ‘prucalopride’ OR ‘mosapride’ OR ‘renzapride’ OR ‘tegaserod’ OR ‘TD-5108’ OR ‘ATI-7505’, including derivatives of these terms and other names used for these drugs. Limits applied were: English language, humans and adults. No date limitation was imposed. The searches were repeated in June 2010 to identify any new reports that emerged during the time taken to develop the manuscript. Upon revision of the manuscript in December 2011, an additional search for pharmacokinetic information was conducted and relevant references were obtained. Authors also contacted the medical information departments of relevant pharmaceutical companies to request further unpublished information or abstracts presented at conferences. The reference lists of retrieved articles were also reviewed.
Abstracts presented at UEGW 2006–2008 and at DDW 2008–2010 (i.e. for all years where abstracts were searchable electronically) were also searched by medical writing support staff, for mention of the drugs of interest (listed above), and those reporting data not already published in the retrieved articles were included in the analysis.
The Royal Society of Medicine use an automated duplicate checker, followed by hand-screening by the researcher to remove duplicates before records were reviewed. The remaining abstracts were filtered for relevance according to predefined eligibility criteria: studies had to relate to GI disorders, to the study drug (listed above), be either clinical studies or systematic reviews (including meta-analyses) and case reports were only included if they related to cardiac safety. Resulting abstracts were then hand-searched against the same eligibility criteria by a second reviewer, and relevant abstracts were segregated into pharmacokinetics, human pharmacodynamics, clinical studies and safety/tolerability, and full-text of these articles obtained. Full text was then reviewed independently by the authors. Cardiac-related safety/tolerability information was systematically reviewed and data retrieved from the full text by the authors were included in the manuscript, as the study authors had originally reported (without using any specific summary measures or additional analyses). Any discrepancies were discussed with the authors. No specific form was used to extract data, risk of bias of individual studies was not formally assessed and data from individual studies were not combined.
Results
The literature searches, after removal of duplicates, returned a total of 1164 articles. A total of 61 conference abstracts were identified.
The original cisapride search returned 582 articles. Of these, 381 were selected for full-text review (20 pharmacokinetic, 141 pharmacodynamic, 183 clinical efficacy, 37 safety). Of these, 75 were considered relevant and cited in this article; 31 additional articles were identified and included. In the 2010 update to the search, four articles were identified, two of which met inclusion criteria. None of the three conference abstracts identified were considered relevant.
The tegaserod search returned 162 articles in the original search, and 13 in the update. Of these, 100 were selected for full-text review and 22 were considered relevant and cited in this article; nine additional articles were identified and included. Upon revision of the manuscript in 2011, one additional article was identified in the search and included in the manuscript. None of the 19 conference abstracts identified was included in this report.
The renzapride search returned 105 articles in the original search and two in the update. Of these, 17 were selected for full-text review and seven were considered relevant and cited in this article; two additional articles were identified and included. Upon revision of the manuscript in 2011, one additional article was identified in the search and included in the manuscript. No renzapride conference abstracts were identified.
The clebopride search returned 58 results, of which 38 were selected for full-text review. Of these, eight were included in this report (two of these were originally excluded for not meeting inclusion criteria, but provided useful supporting information so were included by the author). Of the 16 safety-related articles selected for full-text review, none related to cardiac safety; two representative articles (movement disorders) were included in this report. Four additional articles, as well as the clebopride prescribing information and an in vitro report were identified and included. Upon revision of the manuscript in 2011, three additional articles were identified in the search and included in the manuscript. No clebopride conference abstracts were identified.
The original mosapride search identified 120 results, and the second search an additional four items. Of these, 41 were selected for full-text review (including three articles relating to safety). Sixteen were selected to report here, including the two relevant safety reports. An additional seven reports were identified through other sources and included, as well as six background articles (including the mosapride prescribing information). Upon revision of the manuscript in 2011, one additional article was identified in the search and included in the manuscript. None of the 17 mosapride conference abstracts identified were included in this report.
The prucalopride search returned 121 articles in the original search, and seven in the update. Of these, 32 were selected for full-text review and 16 considered relevant and cited in this article; four additional articles were identified and included. Of the 20 conference abstracts identified, five presented relevant information from studies not already covered by full publications, so were included in this report. One related to cardiac safety.
The ATI-7505 search returned 11 articles in the original search and one in the update. Of these, one was selected for full-text review and one considered relevant and cited in this article; four additional articles were identified and included. Upon revision of the manuscript in 2011, one additional article was identified in the search and included in the manuscript. No conference abstracts were identified.
The TDI-5108 search returned five articles in the original search and three in the update. Of these, three were selected for full-text review and two considered relevant and cited in this article; two additional articles were identified and included. Two conference abstracts were identified and included in this report.
Nonselective 5-HT4 receptor agonists
Historically, metoclopramide was the first 5-HT4 receptor agonist to be used for the treatment of hypomotility disorders. The drug is also a D2 receptor antagonist, an action which underlies the well-established, potentially irreversible, neurological side effects that may occur with metoclopramide intake,2010 and therefore will not be described in detail.
Cisapride
Cisapride, an agonist at 5-HT4 receptors and an antagonist at 5-HT3 and 5-HT2 receptors, was introduced worldwide in the 1990s, and has widespread prokinetic effects throughout the GI tract. Although originally employed in a wide range of motility disorders, cisapride was approved for the treatment of acute and severe exacerbations of demonstrated chronic idiopathic or diabetic gastroparesis after failure of other treatment options in the EU, and was approved by the U.S. Food and Drug Administration (FDA) for nocturnal heartburn only.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of cisapride are summarised in Tables 2 and 3 respectively.
Table 2.
Pharmacokinetics of 5-HT4 agonists
| 5-HT4 receptor agonist | Bioavailability | Plasma levels (tmax) | Protein binding | T1/2 | Metabolism and elimination (hepatic) | Metabolism and elimination (renal) |
|---|---|---|---|---|---|---|
| Nonselective 5-HT4 receptor agonists | ||||||
| Cisapride | ∼40–50% (absolute)2002 | 1–2 h1998 | ∼98%1998 | ∼10 h2002 (potentially prolonged in patients with hepatic impairment/elderly)1998 | P450 enzyme system2002 | Unchanged renal or faecal recovery are <10% of the ingested dose following oral administration |
| Tegaserod | 11 ± 3% (absolute)1999 | 1.3 h1999 | ∼98% | 11 ± 5 h (terminal)1999 | In vitro studies suggest that CYP-mediated metabolism plays an insignificant role in the elimination of tegaserod2001 | Transported by P-glycoprotein efflux pump2/3 excreted unchanged in faeces; 1/3 excreted in urine as main metabolite after acid-catalysed hydrolysis in the stomach and glucuronidation |
| Renzapride | Good2008 | ∼1.4 h2008 | ∼6 h (plasma)2008 | Not metabolised through major CYP drug-metabolising enzymes and does not inhibit CYP450-mediated metabolism of other drugs2008 | Renal excretion2006; eliminated unchanged in the urine2008 | |
| Clebopride | Good1991 | 1.5–1.6 h | 36.5 (0.5 mg) and 26.5 (1 mg) h (serum) | CYP3A4 metabolisation2011 Excreted in faeces (maximal excretion 2–3 h after ingestion)1991 |
About 50% renal excretion1990 | |
| Mosapride | 8% (in dogs) and 14% (in monkeys; oral)1993 | 0.5–1.0 h1993 | Hepatic metabolism2003; first-pass in the liver (principal metabolite M1), excreted in both urine and faeces53, 54 | Elimination via urine and faeces2011 | ||
| Selective 5-HT4 receptor agonists | ||||||
| Prucalopride | >90% (oral) | 2.1 ± 0.9 h | 28–33% | 21.2 ± 3.7 h (terminal) | No hepatic metabolisation At least 6% excreted unchanged in faeces | ∼60% excreted unchanged in urine |
| Velusetrag | ∼30% (estimate; oral) | 4–6 h | ∼13 h | Hepatic metabolisation, substrate of CYP3A4 and P-glycoprotein2008 | Major metabolite (THRX-830449) has equivalent potency to parent; elimination t1/2 16 h (single dose) & 35 h (multiple dose) | |
| Naronapride | No CYP450 metabolisation2007 | Excretion in faeces (one third, unchanged) and urine (metabolite)2011 | ||||
Table 3.
Pharmacodynamics of 5-HT4 agonists
| Cisapride | Tegaserod | Renzapride | Clebopride | Mosapride | Prucalopride | Velusetrag | Naronapride | |
|---|---|---|---|---|---|---|---|---|
| Oesophagus | ||||||||
| Salivary flow | ↑ in GERD158–168 Amplitude +/− in HV160, 169, 170 | |||||||
| Oesophageal peristalsis/amplitude | ↑ in GERD158–170 | –171, 172 | ↑1989 | ↑ in GERD2003 | ||||
| Oesophageal emptying | ↑ in GERD158–168 Amplitude +/− in HV160, 169, 170 | |||||||
| Oesophageal acid clearance | ↑ in GERD158–168 Amplitude +/− in HV160, 169, 170 | |||||||
| Oesophageal acid exposure time | Reduced in GERD1998 | |||||||
| No. of reflux events, and no. >5min | Reduced in GERD1998 | |||||||
| LES pressure | ↑ in HV161, 169, 170, 179 ↑or – in GERD160-162, 168, 171 | – in HV2006 | ||||||
| LES tone | ↑173, 179 | |||||||
| No. of TLESRs | +/− in HV177, 180 | – in HV2006 | ||||||
| Stomach & duodenum | ||||||||
| Post-prandial acid secretion/gastric acidity | +/− in GERD165, 177, 181, 182 | |||||||
| Electrogastrographic patterns | Improved in FD2000 1998 | |||||||
| Gastric tone | ↑ in GP1999 | |||||||
| Gastric emptying time | ↓ in HV186, 187, 188, 189 and patients164, 185, 188, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199, but inconsistent200, 201, 202 | ↓ in HV2005 | ↓ in DGp (solid and liquid)1991 | ↓ | Improved2007 in HV1991, DPAN1992, PD2005 | – in HV1999 | ↓ in HV2010 | ↓ in HV2007 |
| Amplitude of gastric contractions | ||||||||
| Gastric compliance/gastric accommodation | +/− in HV208, 209 | ↑ in FD and HV2007 | ||||||
| Gastric transit time | ↓ in C2001 | |||||||
| Gastro–duodenal transit time | ↓ in Gp1982 | |||||||
| Relaxation of pyloric sphincter | ||||||||
| Antroduodenal motility | ↑ in HV188, 209, 213, and patients197, 200, 214, 215, 216, but inconsistent182, 185, 188 | |||||||
| Duodenal and jejunal contractions | ||||||||
| Gall bladder emptying | ↑ in HV217, 218 | |||||||
| Stomach & intestines | ||||||||
| Gastrointestinal transit time | ↓ in IBS-C2006 | |||||||
| Small & large intestine | ||||||||
| Small intestine motility | ↑ in HV219, 220, 221, 222 and IBS220, 223 | |||||||
| Small intestine transit time | – in HV,1987 ↓ in CIIP1986 | ↓ in HV2005 | ||||||
| Colonic filling | ↑ in HV2010 | |||||||
| Ascending colon emptying | ↓ in HV2010 | |||||||
| Colonic transit time | ↓ in HV1987 and constipation226, 227, 228, 229 | ↓ in HV and IBS-C171, 172 | ↓ in IBS-C96, 99 | ↓ in HV1999 and C2001 | ↓ in HV2010 | ↓ in HV2007 | ||
| Colonic motor activity | ↑ after resection1995 | |||||||
| Anorectal function | – in HV051, 231 and C2002 | |||||||
| Anorectal sensation | ↑ in HV2003 | – in HV051, 231 and C2002Heightened in C (mechanical and electrical)2002 | ||||||
| Stools | ||||||||
| Stool consistency | ↓ in HV2010 | ↓ in HV2007 | ||||||
| Bowel frequency | ↑ in HV2010 | |||||||
| Whole gut transit | ↓ in HV1999 and C2001 | |||||||
↑, increased; ↓, decreased; –, no effect; +/−, mixed effects; AN, anorexia nervosa; C, constipation; CI, critical illness; CIIP, chronic idiopathic intestinal pseudo-obstruction; DPAN, diabetic patients with autonomic neuropathy; DGp, diabetic gastroparesis; FD, functional dyspepsia; Gp, gastroparesis; HV, healthy volunteers; IBS-C, constipation-predominant irritable bowel syndrome; LES, lower oesophageal sphincter; PD, Parkinson's disease; TLESR, transient lower oesophageal sphincter relaxations.
Clinical trials
Clinical trials, summarised in Supplementary Table S1, have explored the efficacy of cisapride in a number of GI conditions, including GERD, functional dyspepsia, gastroparesis, chronic intestinal pseudo-obstruction, post-operative ileus and chronic constipation, but evidence of an effect was not robust enough to obtain regulatory approval for indications other than nocturnal heartburn. In 2000, cisapride was withdrawn from the market worldwide, due to concerns over cardiovascular safety (see safety and tolerability section).
Safety and tolerability
Initial experience with cisapride, including post-marketing data from two study populations totalling over 23 000 patients, suggested that the drug was remarkably safe, with diarrhoea (incidence 4.1%), abdominal pain (1.6%), nausea or vomiting (1.5%), headache (1.4%) and constipation (1.2%) being the most frequently reported AEs.1997 In an epidemiological study of almost 37 000 patients prescribed cisapride in the UK and Canada, serious cardiac rhythm disorders were not found to be inordinately associated with cisapride use; however, the 95% confidence interval was large (0.2–9.8), such that an increase in risk could not be ruled out definitively.1999 In children without underlying cardiac disease or electrolyte imbalance, cisapride was found to have no significant effect on cardiac electrical function,2001 and a meta-analysis of randomised, controlled clinical trials among children with GERD found that although there was no evidence of adverse or harmful events, there were no significant clinical benefits.2003
Reports of cardiac events began to accumulate, including palpitations1992 and instances of an unusual tachyarrhythmia, torsades de pointes, as well as ventricular fibrillation and sudden death started to appear.2000 It soon came to be recognised that cisapride use could result in prolongation of the QT interval and, thereby, increase the risk of arrhythmia, a phenomenon well described in association with a number of other drugs, most notably quinidine, but including procainamide, sotalol, amiodarone, disopyramide, macrolide antibiotics (including erythromycin), astemizole, terfenadine, phenothiazines and tricyclic antidepressants. An increased risk was present when cisapride levels were higher, e.g. through concomitant use of CYP450 inhibitors. Indeed, the majority of cardiac AEs occurred when cisapride was used in patients with other risk factors, which included co-administration with other drugs (e.g. triazole antifungals and retrovirals) and foods such as grapefruit juice,1999 which inhibit hepatic cytochrome (CYP) P450 3A4 resulting in high plasma levels of cisapride, or that also caused QT prolongation, as listed above. It also became clear that the likelihood of arrhythmia in association with cisapride use was greater among those with serious underlying disease states such as heart disease, heart failure, respiratory failure, renal failure, hypokalaemia or hypomagnesaemia.
Subsequently, the cellular and molecular basis for the arrhythmogenic potential of cisapride was revealed. In vitro studies found cisapride to be a potent and dose-dependent blocker of the hERG channel,1997 which is the main channel responsible for the repolarisation phase of the cardiac action potential,1998 such that hERG blockade (or channel mutations) prolong the duration of the action potential by delaying the repolarisation phase.2008 Other studies suggested that it was not QT prolongation per se, but rather, the increase in dispersion of repolarisation that usually accompanies QT prolongation, which provides the arrhythmogenic substrate.2003
Although some studies suggested that cisapride had a low arrhythmogenic potential among neonates regardless of gestational age,2002 others drew attention to the low levels of CYP 3A4 in the neonatal liver2001 and the consequent effects on cisapride metabolism. Indeed, a pharmacokinetic study in premature infants demonstrated increased serum concentrations of cisapride and parallel prolongations of the QT interval.2003
Unfortunately, around the same time, the prokinetic properties of erythromycin had begun to be widely appreciated and its co-administration with cisapride, or the sequential use of i.v. erythromycin and oral cisapride, was not uncommon; thus, increasing the potential for QT prolongation, through its own effects on the QT interval as well as through its inhibition of CYP450.070, 071, 072 Others at risk were those with congenital prolongation of the QT interval, a family history of the long QT syndrome or those with significant bradycardia.
As large surveys in adults, children and neonates had indicated that such events were rare058, 073, 074, 075, 076 and that risks could be managed by an appropriate awareness programme, the initial response was a risk management programme identifying those at risk, as well as drugs that should not be co-administered with cisapride. Accordingly, in 1995, a ‘black box’ warning contraindicating the use of cisapride among those taking drugs that affected its metabolism was issued by the FDA. At that time, 34 cases of torsades de pointes, 23 of prolonged QT interval and 4 deaths had been reported.2000 In 1996, further warnings were issued in relation to concomitant medications that also prolonged the QT interval and in conditions that predisposed to cardiac arrhythmias. As a result, the ‘black box’ was expanded in 1998. However, the subsequent realisation that serious cardiac AEs could occur among low-risk groups, including children, coupled with the documentation of continued cisapride use in contraindicated situations2001 led to the commercial, worldwide withdrawal of the drug in July 2000.
Tegaserod
Tegaserod is a 5-HT4 receptor agonist with a high affinity for 5-HT4 receptors, but also relevant affinity for 5-HT2(a/b), and 5-HT1(a/b/d) receptors.27, 77 Tegaserod was approved in many countries for the treatment of IBS-C and chronic idiopathic constipation. In March 2007, tegaserod was withdrawn from most markets owing to an increased risk of cardiovascular AEs. It was reintroduced in the USA in July 2007 under a treatment investigational new drug protocol for IBS-C and chronic idiopathic constipation in women younger than 55 who are not at risk for certain cardiovascular events. Tegaserod was not approved for use in the EU as the Committee for Medicinal Products for Human Use was of the opinion that the benefit of tegaserod treatment did not outweigh its risks.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of tegaserod are summarised in Tables 2 and 3 respectively.
Clinical studies
While the benefit of tegaserod therapy in patients with IBS-C has been fairly well demonstrated, evidence of efficacy in chronic idiopathic constipation and functional dyspepsia has been less convincing (summarised in Supplementary Table S2).
Safety and tolerability
The frequency of reported AEs in the 3-month trials with tegaserod varies considerably (e.g. 50–60% of US patients reported AEs),2006 whereas only 4% of the patients in an Asia-Pacific trial2007 and 38% (13% drug-related) in a European trial did so.2005 As this can be explained neither by different doses nor by trial design, cultural differences in the willingness to complain are the most likely explanation.
The most common AEs were diarrhoea, headache and abdominal pain,078, 079, 080, 081 and were graded as mild, sometimes as moderate.2005 Only diarrhoea was reproducibly more prevalent in the tegaserod than in the placebo groups, but this was not dose-related.2006 Diarrhoea occurred mainly in the first week of treatment and was often transient, resolving with continued treatment.2006 The safety profile did not change over a 12-month period with open treatment2006: headache became the most prevalent AE (10–15%); all other AEs, in particular diarrhoea, ranged below 10%.
Three AEs potentially attributable to tegaserod have gained particular attention, namely an increased rate of abdominal surgery, ischaemic colitis and cardiac events. They occurred so infrequently that they are unlikely to be identified in Phase III trials and may only come up in pooled analyses or during post-marketing surveillance, but they are severe enough to warrant concerns.2004 Regarding abdominal surgery in patients with IBS-C, a meta-analysis of 13 controlled trials was conducted, which found no significant difference in the rates of abdominal and pelvic surgery between patients receiving tegaserod (0.44%) and those on placebo (0.41%).2004
Patients with IBS have a higher risk of developing colonic ischaemia than the general population.2004 No cases of ischaemic colitis occurred in over 11 600 patients participating in clinical trials with tegaserod.2004 Although post-marketing reports have noted cases of ischaemic colitis86, 87 and intestinal ischaemia2004 in patients taking tegaserod, the incidence appears to be similar to the general population and is less than estimates for the IBS patient population.2004 Moreover, no mechanism has been identified through which tegaserod might predispose to ischaemic colitis.
The pre-marketing data of systematic cardiac safety assessment may be summarised as follows: in three randomised, double-blind, controlled, parallel-group clinical studies with more than 2500 IBS patients, prolongation of the QTc interval was similarly frequent between groups, as was the frequency of overall electrocardiographic abnormalities. No ventricular or supraventricular tachycardia was observed. In healthy volunteers, tegaserod at i.v. doses resulting in plasma concentrations up to 100 times those measured after therapeutic doses (6 mg b.d.) did not influence electrocardiographic variables.2002
Data collected from over 18 000 patients demonstrated cardiovascular AEs (myocardial infarction, unstable angina pectoris, stroke and one sudden death) in 13 of 11 614 patients treated with tegaserod (a rate of 0.11%) compared with 1 of 7031 patients treated with placebo (a rate of 0.01%). Therefore, in 2007, the FDA requested withdrawal from the market, citing a relationship between prescriptions of the drug and increased risks of heart attack or stroke. However, this was denied by the manufacturer, as all affected patients were said to have pre-existing cardiovascular disease or risk factors for such. Thus, no causal relationship between tegaserod use and cardiovascular events had been demonstrated. Indeed, a matched case–control study of tegaserod-treated patients with untreated patients found no association between tegaserod and adverse cardiovascular outcomes.2009
A hypothetical mechanism for tegaserod-related cardiac events was proposed involving interaction at 5-HT1(b/d) receptors on coronary arterioles.2004 However, as tegaserod does not behave as a 5-HT1(b) receptor agonist in a recent study of human isolated proximal and distal coronary arterioles, the mechanisms involved remain unclear.2009
Renzapride
Renzapride, a 5-HT4 receptor agonist and a 5-HT3 receptor antagonist,2008 has been evaluated in the treatment of IBS-C, but has not been approved in any part of the world.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of renzapride are summarised in Tables 2 and 3 respectively.
Clinical studies
Clinical studies with renzapride have focused mainly on IBS (summarised in Supplementary Table S3). However, therapeutic margins were only minimal (5–6% over placebo), and this led to the discontinuation of the drug development programme.
Safety and tolerability
Renzapride was well tolerated; most AEs were mild-to-moderate in intensity and equally distributed across active or placebo treatment groups. The most common AEs were GI, with diarrhoea and abdominal pain being the most commonly associated with renzapride treatment.096, 097, 098, 099
In vitro cardiac conductivity studies in isolated Purkinje fibres showed no significant QT prolongation by renzapride. In transfected cells, renzapride was a 1000-fold less potent inhibitor of the hERG channel compared with cisapride.2007 In the clinical trial programme, no significant ECG alterations were observed (in particular no evidence of prolongation of the QT interval).095, 096, 097, 098, 099, 101
Clebopride
Clebopride is a D2 receptor antagonist, as well as a 5-HT4 receptor agonist and a 5-HT3 receptor antagonist. Clebopride is available in Italy and Spain as a gastroprokinetic drug.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of clebopride are summarised in Tables 2 and 3 respectively.
Clinical studies
To our knowledge, the effects of clebopride on lower GI motility and therapeutic potential in lower GI indications have not been explored. Controlled studies investigating the effects of clebopride have primarily focused on FD, but are dated and are generally underpowered with methodological flaws compared with current requirements of good clinical practice (summarised in Supplementary Table S4).
Safety and tolerability
Antagonism of dopamine receptors in the GI tract promotes coordinated motor activity and accelerates transit, while blockade of D2 receptors in the area postrema exerts an anti-nausea, anti-emetic effect.103, 104 However, central D2 receptor blockade is also responsible for AEs, including extrapyramidal dystonic reactions and hyperprolactinaemia.2004 Comparative studies among prokinetics have demonstrated that clebopride is most associated with dystonic reactions106, 107 that are not limited to reversible Parkinsonian-like symptoms, but also include tardive, potentially irreversible, dyskinesia.1993 The calculated prevalence of movement disorders associated with chronic use of other antidopaminergics is around 1%,1982 but it is 4-fold higher for clebopride.1996 Conversely, clebopride exerts a less pronounced hyperprolactinaemic effect compared with any other antidopaminergic drug.2004
Substituted benzamides have been associated with dose-dependent cardiac AEs. Thus, although overt cardiotoxicity has not been reported in clinical studies on clebopride, the effects of the drug on cardiac action potential duration, hERG channel, and sodium channel currents were investigated in vitro.2007 Clebopride (10 μm) prolonged the action potential duration at 90% (but not 50%) repolarisation. Furthermore, an IC50 value of 0.62 ± 0.30 μm for hERG channel currents was determined. No effect was observed on sodium channel currents.2007 It was concluded that clebopride is sufficiently safe at therapeutic doses, but overdosing or impaired metabolism might be associated with torsadogenic effects.
Mosapride
Mosapride is primarily a selective 5-HT4 receptor agonist in the GI tract.112, 113, 114 Its principal metabolite is approximately 50% as potent as the parent compound at stimulating gastric motility, however, it is also a potent 5-HT3 receptor antagonist.1993 Mosapride is available as a prokinetic agent in a number of Asian countries.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of mosapride are summarised in Tables 2 and 3 respectively.
Clinical trials
Several studies have been performed to assess the efficacy of mosapride for the treatment of FD. However, most studies were small and lack controls and, as such, failed to show significant symptomatic improvements (summarised in Supplementary Table S5).2002
Safety and tolerability
In contrast to cisapride, mosapride does not appear to have any significant effect on K+ channels. Using isolated rabbit Purkinje fibres and ventricular muscle, mosapride had little effect on the rapid component of the delayed rectifying K+ channels and no effect in hERG transfected cells.039, 117, 118 Using a rabbit model of the acquired long-QT syndrome, cisapride prolonged the QT interval, while mosapride did not,1997 despite its metabolism by CYP3A4.2000 In a 14-day study of mosapride (15 mg/day) in 10 healthy male volunteers, no ECG changes were noted despite co-administration of erythromycin.2003 In a separate study of 20 healthy volunteers who received a single dose of mosapride (10 mg), pulse, heart rate, QT interval and ECGs were no different after drug administration.2002 Furthermore, in a study of 18 patients who were taking a variety of psychiatric medications, co-administration of mosapride did not change any ECG parameters.2000 However, a case report described a 68-year-old man with sick sinus syndrome, requiring a permanent pacemaker and concomitant flecainide therapy, who developed a prolonged QTc interval after starting mosapride.2001 In summary, the studies published to date demonstrate that mosapride is safe without any significant cardiovascular effects.
Selective 5-HT4 receptor agonists
Prucalopride
Prucalopride is a dihydrobenzofurancarboxamide derivative with distinct structural differences from other 5-HT4 receptor agonists such as cisapride and tegaserod. These differences are likely to account for the greater selectivity for the 5-HT4 receptor observed with prucalopride (>150× for prucalopride vs. <1 for cisapride and tegaserod).1997 Prucalopride was recently approved, on 15 October 2009, by the European Medicines Agency (EMA) for the symptomatic treatment of chronic constipation in women in whom laxatives fail to provide adequate relief.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of prucalopride are summarised in Tables 2 and 3 respectively.
Clinical trials
The majority of clinical studies with prucalopride were conducted in patients with chronic constipation (summarised in Supplementary Table S6). Multiple randomised, controlled trials found that prucalopride at doses of 1–4 mg (q.d.) improved symptoms of chronic constipation, including stool frequency, stool consistency, straining and quality of life.125, 126, 127, 128
To date, no studies addressing the efficacy of prucalopride in the IBS-C or upper GI disorders, such as gastroparesis or FD, have been presented.
Safety and tolerability
Safety assessments were performed as part of the Phase III studies.125, 127, 128 Treatment-associated AEs were reported in 70–80% of patients randomised to placebo, 2 or 4 mg of prucalopride. The most common treatment-associated AEs included headache in 25–30% of prucalopride subjects vs. 12–17% of placebo; nausea (12–24% vs. 8–14%); abdominal pain (16–23% vs. 11–19%); and diarrhoea (12–19% vs. 3–5%). The majority of AEs occurred within the first 24 h of treatment and proved transient.
Pooled results of the three Phase III studies show that serious AEs (SAEs) were reported in 2.7% of patients receiving the recommended dose of 2 mg (n = 661) vs. 2.0% of patients receiving placebo (n = 659).2008 Discontinuation rates from AEs ranged from 4% to 15% among patients receiving prucalopride and from 2% to 7% among patients receiving placebo. Many discontinuations were the consequence of headache, abdominal pain, nausea, vomiting or diarrhoea which occurred on the first day of study drug administration.
Data from an open-label, long-term extension trial were recently reported.2009 In this study, 1775 constipated patients who had completed one of the Phase III studies were followed up for a mean of 231 days (range 1–721 days). Similar to the Phase III trials, the most common AEs were headache (31%), abdominal pain (24%), diarrhoea (20%), flatulence (16%) and nausea (15%). The most common AE rated as ‘severe’ was surgical intervention (3.3%). SAEs were uncommon (<0.5%). The most common AEs leading to discontinuation were abdominal pain (1.5%) and headache (1.5%). Two deaths occurred; one was deemed unrelated to prucalopride and no treatment information was available for the other.2009
Unlike other 5-HT4 receptor agonists, prucalopride has not been found to interact with the hERG channel or 5-HT1(b) receptors, each postulated to be responsible for the development of adverse cardiovascular effects with other 5-HT4 receptor agonists.39, 92 Cardiovascular safety was evaluated in two Phase I, double-blind, controlled, two-way cross-over studies which included 32 and 24 healthy volunteers, in which prucalopride was escalated to a maximum dose of either 10 or 20 mg.2009 No clinically relevant differences in blood pressure or incidence of prolonged QTc were identified between groups. Similarly, no correlation was found between observed shifts in ECG parameters based upon prucalopride concentrations up to 10 times the recommended therapeutic dose. A small, transient increase in mean heart rate and associated decrease in the PQ and QT intervals was observed with prucalopride. Within-subject differences between the groups were not statistically different. Cardiovascular safety was also carefully assessed in the Phase III clinical trials. There were no differences in vital signs or ECG parameters between study participants randomised to placebo or either dose of prucalopride. The incidence of QT interval prolongation (>470 ms) was low (≤2.1%) and similar between groups.125, 127, 128 A single cardiovascular event, an episode of supraventricular tachycardia, occurred in a patient with a history of mitral valve prolapse and cardiac arrhythmias, who was randomised to prucalopride 2 mg.2008
Cardiovascular safety was also assessed as part of a study conducted in a high-risk population. For this study, 89 elderly patients residing in a nursing facility (mean age 83 years) were randomised to prucalopride (0.5, 1 or 2 mg) or placebo. Of the participants, 80% had prior history of cardiovascular disease. There were no differences in vital signs, laboratory results or ECG parameters between groups. Moreover, there were no differences in the incidence of prolonged QTc interval between groups.2009
Velusetrag (TD-5108)
Velusetrag is a high-affinity 5-HT4 receptor agonist, which is being developed for the treatment of chronic constipation.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of velusetrag are summarised in Tables 2 and 3 respectively.
Clinical studies
Clinical studies with velusetrag have focused on patients with chronic constipation. The few trials that have been published have described significant improvements in bowel frequency and constipation-related symptoms vs. placebo (Supplementary Table S7).
Safety and tolerability
In general, there were no SAEs with velusetrag treatment; notable AEs were the predictable GI effects such as diarrhoea or altered bowel movements. In the 401-patient Phase IIb trial, 12–15% of patients developed diarrhoea on velusetrag relative to placebo (1%).2008 Of the three velusetrag doses tested, 15 mg provided the most favourable therapeutic index. The 50-mg dose was associated with higher prevalence of nausea, vomiting and headache than the other velusetrag doses and placebo.
An approximate 10 bpm increase in heart rate was observed following administration of 15 mg velusetrag in healthy volunteers and patients with chronic constipation.2008 However, in the absence of a placebo control group, this observation is difficult to interpret. The significance of the single observations of palpitations (noted with velusetrag at 30 mg) and asymptomatic junctional escape rhythm (with 50 mg dose) noted in the pharmacodynamic transit study2010 is uncertain, considering the limited number of subjects. In ∼540 healthy subjects or patients with chronic constipation treated with velusetrag for up to 28 days, one patient with constipation experienced palpitations in the placebo group and one healthy volunteer had junctional escape rhythm following velusetrag at 70 mg.
In vitro studies show that velusetrag (3 μm, 5-min application, n = 3 cells) had no significant effect on the magnitude of hERG potassium tail currents recorded from Chinese hamster ovary (CHO)-K1 cells expressing hERG channels.2008
Naronapride (ATI-7505)
Naronapride is structurally related to the chemical structure of cisapride, but devoid of significant affinities for other 5-HT receptors or the hERG channel.2004 The drug is under evaluation for treatment of upper and lower GI motility disorders, but only limited data have been published.
Pharmacokinetics and pharmacodynamics
The pharmacokinetics and pharmacodynamics of naronapride are summarised in Tables 2 and 3 respectively.
Clinical trials and indications/approvals
Naronapride has been evaluated in Phase II trials in chronic constipation, GERD and FD. Naronapride (80 mg b.d.) demonstrated significant improvement over placebo in chronic constipation.2010 In the upper GI tract, early Phase II studies indicated potential for reduction of reflux events and FD symptoms.
Safety
The cardiac safety of naronapride has been evaluated in a thorough QT study, which assesses the cardiac safety of a drug vs. both placebo and a positive control (e.g. moxifloxacin), and has confirmed a favourable safety profile at therapeutic or supratherapeutic doses.
Discussion
Patients with symptoms that are potentially attributable to hypomotility of the GI tract constitute an important part of clinical GI practice.2008 These conditions are part of a spectrum that ranges from functional dysphagia and GERD, through FD and gastroparesis, to IBS-C and chronic constipation. Prokinetic drugs are considered the drugs of choice for the treatment of hypomotility disorders, although the correlation between impaired motility and symptoms is inconsistent.2008
The 5-HT4 receptor, with its location on cholinergic nerve endings of interneurons and motor neurons, has been established as a valid target to enhance GI motility. Mechanistic studies have confirmed a stimulatory effect of 5-HT4 receptor agonists on GI motor activity, and clinical efficacy in hypomotility disorders has been established for a number of these drugs. Cisapride, as well as tegaserod, saw broad clinical application after regulatory approval (not in the EU for the latter drug),4, 5 but both drugs were withdrawn (in the US), in part, because of cardiovascular AEs.006, 007, 008, 041 The prevalence of cardiovascular AEs with both drugs was low and likely to fall below the limit of detection in a clinical trial programme.
These events might seriously hamper the clinical development of novel 5-HT4 receptor agonists for the treatment of GI hypomotility disorders, especially when taking into account the ability to establish cardiovascular safety. However, several chemical classes of 5-HT4 receptor agonists have been developed, and the selectivity of different compounds for the 5-HT4 receptor over other targets is highly variable between individual drugs and drug classes. The mechanism through which cisapride promotes cardiac arrhythmias is now clearly established to be unrelated to 5-HT4 receptor agonism. The cardiac risk associated with cisapride use is entirely attributable to its affinity for the hERG channel which results in QT prolongation, and is enhanced by concomitant use of inhibitors of CYP, the principal pathway in cisapride metabolism.007, 008, 041, 059, 060, 062, 063, 064, 065, 066, 067, 068, 069 Hence, 5-HT4 receptor agonists without affinity for the hERG channel are devoid of this particular arrhythmogenic risk. Another risk factor in the case of cisapride was its metabolism through the CYP450 pathway, leading to increased plasma levels when other drugs also metabolised via this same pathway were taken at the same time. The mechanism through which tegaserod use may be associated with increased cardiovascular risk is not clearly established. However, it has been suggested that the affinity of tegaserod for the 5-HT1 or 5-HT2(b) receptors may underlie these AEs.27, 92 This would implicate lack of such risk for novel, highly-selective 5-HT4 receptor agonists.
The link between cardiovascular risk, the CYP450 metabolic pathway and lack of selectivity of previously used 5-HT4 receptor agonists supports the development of selective 5-HT4 receptor agonists for the treatment of GI hypomotility disorders, as was the case with prucalopride for chronic constipation.2008 The recent EMEA approval of prucalopride for the treatment of chronic constipation confirms that 5-HT4 receptor agonists are still considered a valid therapeutic target at the regulatory level.2008 Although no link between 5-HT4 agonism and cardiovascular AEs has been established, standards for establishing cardiovascular safety for this class of drugs may still be elevated at the regulatory level. Indeed, the cardiovascular safety profile of prucalopride was assessed in great detail, both in vitro and in the clinical trial programme.130, 131, 132, 038, 026
Although this review may be limited by incomplete retrieval of relevant research, by bias in reporting such research, and by inherent risk of bias at the study level, our analysis of the literature has revealed a wealth of evidence that 5-HT4 receptor agonists have clinical efficacy in the treatment of GI disorders and no evidence of cardiovascular safety concerns with selective 5-HT4 receptor agonists. Nevertheless, caution is warranted as the number of patients exposed to the newer 5-HT4 agonists is still relatively low (number of exposed patients can be derived from the Supplementary Tables for each drug), and adequate post-marketing surveillance will help to further establish the favourable cardiovascular risk profile of these agents.
Conclusions
5-HT4 receptor agonists have clear-cut prokinetic effects in the gut. These agonists differ in many aspects that are either related or unrelated to their interaction with 5-HT4 receptors. Differences that are unrelated to the 5-HT4 receptor, such as affinity at non-5-HT4 receptors, may influence the agent's safety and overall benefit–risk profile. 5-HT4 receptor-related differences have an impact on the agonists overall activity in a given tissue. Together, these differences affect the therapeutic potential for the treatment of GI motility disorders. Based on available evidence, a highly selective 5-HT4 receptor agonist, such as prucalopride, may offer improved efficacy and safety to treat patients with impaired GI motility, such as severe chronic constipation.
Declaration of personal interests
Jan Tack has served as a scientific advisor for Addex pharma, AGI Therapeutics, Almirall, Aryx, AstraZeneca, Danone, Ipsen, Menarini, Movetis, Norgine, Novartis, Nycomed, Ocera, Rose Pharma, SK Life Sciences, Smartpill, Sucampo, Theravance, Tranzyme, Xenoport and Zeria, and a speaker for Abbott, AstraZeneca, Menarini, Movetis, Novartis and Nycomed. Michael Camilleri has served as a consultant and an advisory board member for Adolor, Albireo Pharma, Alkermes, Ardelyx, ARYx Therapeutics, Ascent, Astellas, AstraZeneca, BioKier, Biomedical Insights, Domain, GlaxoSmithKline, Ikaria, Ironwood, Johnson & Johnson, NovaSecta, Ocera, Procter & Gamble, Shire, SK Bio, Synergy, Takeda, Theravance and Tranzyme, and has received research funding from Albireo, NIH, Rose Pharma, Tsumura and Wyeth. Lin Chang has served as a consultant or an advisory board member for Prometheus Laboratories, Takeda, Albireo, Rose Pharma, GlaxoSmithKline, Ironwood, Forest, Salix, Marathon Pharmaceuticals, Novo Nordisk, Lexicon and Movetis, and has received research funding from Prometheus, Rose Pharma, Takeda, Ironwood and Shire. William D. Chey has served as a consultant and an advisory board member for Albireo, AstraZeneca, Forest, Ironwood, Procter & Gamble, Prometheus, Salix, Smartpill, Takeda, and has received research funding from Ardelyx and Ironwood. James J. Galligan has served as a consultant for Faegre and Benson (now Faegre, Baker, Daniels), and LLP. Brian E. Lacy has served as a speaker for Novartis, Prometheus and Takeda, and an advisory board member for Prometheus, Takeda, Ironwood and Movetis. Dr Lacy has received investigator-initiated, unrestricted funding from Takeda. Stefan Müller-Lissner has served as a speaker, a consultant and an advisory board member for Axcan, Boehringer Ingelheim, Falk Foundation, Janssen, Movetis, Menarini Farmaceutica, Movetis, Mundipharma GmbH, Novartis, Pfizer, Procter & Gamble, Sucampo Pharma and Zeria Pharma. Eamonn M. M. Quigley has served as a consultant and an advisory board member for Movetis. Dr Quigley has also served as an advisory board chair for Janssen. Jan Schuurkes is an employee of Shire. Joris H. De Maeyer is an employee of Shire. Vincenzo Stanghellini has served as speaker and advisory board member for Axcan, Danone, Janssen, Movetis, Nycomed, Norgine, Novartis, Pfizer, Sofar and Valeas. Declaration of funding interests: The writing or preparation of this paper was funded in part by Movetis; writing support (conducting searches and editing the manuscript) was provided by Kate Carpenter and Victoria Harvey of Choice Pharma, and was funded by Movetis.
Supporting Information
Additional Supporting Information may be found in the online version of this article:
Table S1. Clinical trials on the efficacy of cisapride in GI conditions.
Table S2. Clinical trials on the efficacy of tegaserod in GI conditions.
Table S3. Clinical trials on the efficacy of renzapride in irritable bowel syndrome.
Table S4. Clinical trials on the efficacy of clebopride in GI conditions.
Table S5. Clinical trials on the efficacy of mosapride in GI conditions.
Table S6. Clinical trials on the efficacy of prucalopride in GI conditions.
Table S7. Clinical trials on the efficacy of velusetrag in chronic constipation.
Please note: Wiley-Blackwell are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
References
- Sanger GJ, Alpers DH. Development of drugs for gastrointestinal motor disorders: translating science to clinical need. Neurogastroenterol Motil. 2008;20:177–84. doi: 10.1111/j.1365-2982.2008.01084.x. [DOI] [PubMed] [Google Scholar]
- Briejer MR, Akkermans LM, Schuurkes JA. Gastrointestinal prokinetic benzamides: the pharmacology underlying stimulation of motility. Pharmacol Rev. 1995;47:631–51. [PubMed] [Google Scholar]
- Langlois M, Fischmeister R. 5-HT4 receptor ligands: applications and new prospects. J Med Chem. 2003;46:319–44. doi: 10.1021/jm020099f. [DOI] [PubMed] [Google Scholar]
- Evans BW, Clark WK, Moore DJ, Whorwell PJ. Tegaserod for the treatment of irritable bowel syndrome and chronic constipation. Cochrane Database Syst Rev. 2007:CD003960. doi: 10.1002/14651858.CD003960.pub3. [DOI] [PubMed] [Google Scholar]
- McCallum RW, Prakash C, Campoli-Richards DM, Goa KL. Cisapride. A preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use as a prokinetic agent in gastrointestinal motility disorders. Drugs. 1988;36:652–81. doi: 10.2165/00003495-198836060-00002. [DOI] [PubMed] [Google Scholar]
- Novartis. Press release: Novartis suspends US marketing and sales of Zelnorm in response to request from FDA. Available at: http://hugin.info/134323/R/1116336/204121.pdf. Accessed December 14, 2010.
- Drolet B, Khalifa M, Daleau P, Hamelin BA, Turgeon J. Block of the rapid component of the delayed rectifier potassium current by the prokinetic agent cisapride underlies drug-related lengthening of the QT interval. Circulation. 1998;97:204–10. doi: 10.1161/01.cir.97.2.204. [DOI] [PubMed] [Google Scholar]
- Jones JK, Fife D, Curkendall S, Goehring E, Jr, Guo JJ, Shannon M. Coprescribing and codispensing of cisapride and contraindicated drugs. JAMA. 2001;286:1607–9. doi: 10.1001/jama.286.13.1607. [DOI] [PubMed] [Google Scholar]
- US Food & Drug Administration. Zelnorm (tegaserod maleate). April 2009. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm103223.htm. Accessed December 14, 2010.
- Department of Health. Medicines Control Agency announces withdrawal of Cisapride July 2000. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Pressreleases/DH_4005066. Accessed December 14, 2010.
- Dumuis A, Sebben M, Bockaert J. The gastrointestinal prokinetic benzamide derivatives are agonists at the non-classical 5-HT receptor (5-HT4) positively coupled to adenylate cyclase in neurons. Naunyn Schmiedebergs Arch Pharmacol. 1989;340:403–10. doi: 10.1007/BF00167041. [DOI] [PubMed] [Google Scholar]
- Markstein R, Matsumoto M, Kohler C, Togashi H, Yoshioka M, Hoyer D. Pharmacological characterisation of 5-HT receptors positively coupled to adenylyl cyclase in the rat hippocampus. Naunyn Schmiedebergs Arch Pharmacol. 1999;359:454–9. doi: 10.1007/pl00005375. [DOI] [PubMed] [Google Scholar]
- Blondel O, Gastineau M, Dahmoune Y, Langlois M, Fischmeister R. Cloning, expression, and pharmacology of four human 5-hydroxytryptamine 4 receptor isoforms produced by alternative splicing in the carboxyl terminus. J Neurochem. 1998;70:2252–61. doi: 10.1046/j.1471-4159.1998.70062252.x. [DOI] [PubMed] [Google Scholar]
- Medhurst AD, Lezoualc'h F, Fischmeister R, Middlemiss DN, Sanger GJ. Quantitative mRNA analysis of five C-terminal splice variants of the human 5-HT4 receptor in the central nervous system by TaqMan real time RT-PCR. Brain Res Mol Brain Res. 2001;90:125–34. doi: 10.1016/s0169-328x(01)00095-x. [DOI] [PubMed] [Google Scholar]
- Claeysen S, Faye P, Sebben M, Taviaux S, Bockaert J, Dumuis A. 5-HT4 receptors: cloning and expression of new splice variants. Ann N Y Acad Sci. 1998;861:49–56. doi: 10.1111/j.1749-6632.1998.tb10172.x. [DOI] [PubMed] [Google Scholar]
- Ray AM, Kelsell RE, Houp JA, et al. Identification of a novel 5-HT(4) receptor splice variant (r5-HT(4c1)) and preliminary characterisation of specific 5-HT(4a) and 5-HT(4b) receptor antibodies. Eur J Pharmacol. 2009;604:1–11. doi: 10.1016/j.ejphar.2008.11.056. [DOI] [PubMed] [Google Scholar]
- De Maeyer JH, Aerssens J, Verhasselt P, Lefebvre RA. Alternative splicing and exon duplication generates 10 unique porcine 5-HT 4 receptor splice variants including a functional homofusion variant. Physiol Genomics. 2008;34:22–33. doi: 10.1152/physiolgenomics.00038.2008. [DOI] [PubMed] [Google Scholar]
- Bender E, Pindon A, van Oers I, et al. Structure of the human serotonin 5-HT4 receptor gene and cloning of a novel 5-HT4 splice variant. J Neurochem. 2000;74:478–89. doi: 10.1046/j.1471-4159.2000.740478.x. [DOI] [PubMed] [Google Scholar]
- Claeysen S, Sebben M, Becamel C, Bockaert J, Dumuis A. Novel brain-specific 5-HT4 receptor splice variants show marked constitutive activity: role of the C-terminal intracellular domain. Mol Pharmacol. 1999;55:910–20. [PubMed] [Google Scholar]
- Liu M, Geddis MS, Wen Y, Setlik W, Gershon MD. Expression and function of 5-HT4 receptors in the mouse enteric nervous system. Am J Physiol Gastrointest Liver Physiol. 2005;289:G1148–63. doi: 10.1152/ajpgi.00245.2005. [DOI] [PubMed] [Google Scholar]
- van Lelyveld N, Ter Linde J, Schipper M, Samsom M. Serotonergic signalling in the stomach and duodenum of patients with gastroparesis. Neurogastroenterol Motil. 2008;20:448–55. doi: 10.1111/j.1365-2982.2007.01068.x. [DOI] [PubMed] [Google Scholar]
- Matsumoto M, Togashi H, Mori K, et al. Evidence for involvement of central 5-HT(4) receptors in cholinergic function associated with cognitive processes: behavioral, electrophysiological, and neurochemical studies. J Pharmacol Exp Ther. 2001;296:676–82. [PubMed] [Google Scholar]
- Yan Z. Regulation of GABAergic inhibition by serotonin signaling in prefrontal cortex: molecular mechanisms and functional implications. Mol Neurobiol. 2002;26:203–16. doi: 10.1385/MN:26:2-3:203. [DOI] [PubMed] [Google Scholar]
- Alex KD, Pehek EA. Pharmacologic mechanisms of serotonergic regulation of dopamine neurotransmission. Pharmacol Ther. 2007;113:296–320. doi: 10.1016/j.pharmthera.2006.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brattelid T, Qvigstad E, Lynham JA, et al. Functional serotonin 5-HT4 receptors in porcine and human ventricular myocardium with increased 5-HT4 mRNA in heart failure. Naunyn Schmiedebergs Arch Pharmacol. 2004;370:157–66. doi: 10.1007/s00210-004-0963-0. [DOI] [PubMed] [Google Scholar]
- De Maeyer JH, Schuurkes JA, Lefebvre RA. Selective desensitization of the 5-HT4 receptor-mediated response in pig atrium but not in stomach. Br J Pharmacol. 2009;156:362–76. doi: 10.1111/j.1476-5381.2008.00007.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Maeyer JH, Lefebvre RA, Schuurkes JA. 5-HT4 receptor agonists: similar but not the same. Neurogastroenterol Motil. 2008;20:99–112. doi: 10.1111/j.1365-2982.2007.01059.x. [DOI] [PubMed] [Google Scholar]
- Baxter GS, Craig DA, Clarke DE. 5-Hydroxytryptamine4 receptors mediate relaxation of the rat oesophageal tunica muscularis mucosae. Naunyn Schmiedebergs Arch Pharmacol. 1991;343:439–46. doi: 10.1007/BF00169544. [DOI] [PubMed] [Google Scholar]
- Prins NH, Van Haselen JF, Lefebvre RA, Briejer MR, Akkermans LM, Schuurkes JA. Pharmacological characterization of 5-HT4 receptors mediating relaxation of canine isolated rectum circular smooth muscle. Br J Pharmacol. 1999;127:1431–7. doi: 10.1038/sj.bjp.0702665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prins NH, Shankley NP, Welsh NJ, et al. An improved in vitro bioassay for the study of 5-HT(4) receptors in the human isolated large intestinal circular muscle. Br J Pharmacol. 2000;129:1601–8. doi: 10.1038/sj.bjp.0703254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eglen RM, Swank SR, Walsh LK, Whiting RL. Characterization of 5-HT3 and ‘atypical’ 5-HT receptors mediating guinea-pig ileal contractions in vitro. Br J Pharmacol. 1990;101:513–20. doi: 10.1111/j.1476-5381.1990.tb14113.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kilbinger H, Gebauer A, Haas J, Ladinsky H, Rizzi CA. Benzimidazolones and renzapride facilitate acetylcholine release from guinea-pig myenteric plexus via 5-HT4 receptors. Naunyn Schmiedebergs Arch Pharmacol. 1995;351:229–36. doi: 10.1007/BF00233241. [DOI] [PubMed] [Google Scholar]
- Kilbinger H, Wolf D. Effects of 5-HT4 receptor stimulation on basal and electrically evoked release of acetylcholine from guinea-pig myenteric plexus. Naunyn Schmiedebergs Arch Pharmacol. 1992;345:270–5. doi: 10.1007/BF00168686. [DOI] [PubMed] [Google Scholar]
- Pan H, Galligan JJ. 5-HT1A and 5-HT4 receptors mediate inhibition and facilitation of fast synaptic transmission in enteric neurons. Am J Physiol. 1994;266:G230–8. doi: 10.1152/ajpgi.1994.266.2.G230. [DOI] [PubMed] [Google Scholar]
- Ren J, Zhou X, Galligan JJ. 5-HT4 receptor activation facilitates recovery from synaptic rundown and increases transmitter release from single varicosities of myenteric neurons. Am J Physiol Gastrointest Liver Physiol. 2008;294:G1376–83. doi: 10.1152/ajpgi.00078.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leclere PG, Lefebvre RA. Presynaptic modulation of cholinergic neurotransmission in the human proximal stomach. Br J Pharmacol. 2002;135:135–42. doi: 10.1038/sj.bjp.0704471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leclere PG, Prins NH, Schuurkes JA, Lefebvre RA. 5-HT4 receptors located on cholinergic nerves in human colon circular muscle. Neurogastroenterol Motil. 2005;17:366–75. doi: 10.1111/j.1365-2982.2005.00621.x. [DOI] [PubMed] [Google Scholar]
- De Maeyer JH, Prins NH, Schuurkes JA, Lefebvre RA. Differential effects of 5-hydroxytryptamine4 receptor agonists at gastric versus cardiac receptors: an operational framework to explain and quantify organ-specific behavior. J Pharmacol Exp Ther. 2006;317:955–64. doi: 10.1124/jpet.106.101329. [DOI] [PubMed] [Google Scholar]
- Potet F, Bouyssou T, Escande D, Baro I. Gastrointestinal prokinetic drugs have different affinity for the human cardiac human ether-a-gogo K(+) channel. J Pharmacol Exp Ther. 2001;299:1007–12. [PubMed] [Google Scholar]
- Nagakura Y, Akuzawa S, Miyata K, et al. Pharmacological properties of a novel gastrointestinal prokinetic benzamide selective for human 5-HT4 receptor versus human 5-HT3 receptor. Pharmacol Res. 1999;39:375–82. doi: 10.1006/phrs.1998.0454. [DOI] [PubMed] [Google Scholar]
- Mohammad S, Zhou Z, Gong Q, January CT. Blockage of the HERG human cardiac K+ channel by the gastrointestinal prokinetic agent cisapride. Am J Physiol. 1997;273:H2534–8. doi: 10.1152/ajpheart.1997.273.5.H2534. [DOI] [PubMed] [Google Scholar]
- Mine Y, Yoshikawa T, Oku S, Nagai R, Yoshida N, Hosoki K. Comparison of effect of mosapride citrate and existing 5-HT4 receptor agonists on gastrointestinal motility in vivo and in vitro. J Pharmacol Exp Ther. 1997;283:1000–8. [PubMed] [Google Scholar]
- Wardle KA, Sanger GJ. The guinea-pig distal colon–a sensitive preparation for the investigation of 5-HT4 receptor-mediated contractions. Br J Pharmacol. 1993;110:1593–9. doi: 10.1111/j.1476-5381.1993.tb14006.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camilleri M, Vazquez-Roque MI, Burton D, et al. Pharmacodynamic effects of a novel prokinetic 5-HT receptor agonist, ATI-7505, in humans. Neurogastroenterol Motil. 2007;19:30–8. doi: 10.1111/j.1365-2982.2006.00865.x. [DOI] [PubMed] [Google Scholar]
- Dennis D, Palme M, Irwin I, Druzgala P, Teichman S. ATI-7505 is a novel, selective 5HT(4) receptor agonist that causes gastrointestinal prokinetic activity in dogs. Gastroenterology. 2004;126:A641. [Google Scholar]
- Beattie DT, Smith JA, Marquess D, et al. The 5-HT4 receptor agonist, tegaserod, is a potent 5-HT2B receptor antagonist in vitro and in vivo. Br J Pharmacol. 2004;143:549–60. doi: 10.1038/sj.bjp.0705929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCullough JL, Armstrong SR, Hegde SS, Beattie DT. The 5-HT2B antagonist and 5-HT4 agonist activities of tegaserod in the anaesthetized rat. Pharmacol Res. 2006;53:353–8. doi: 10.1016/j.phrs.2006.01.003. [DOI] [PubMed] [Google Scholar]
- Grider JR, Foxx-Orenstein AE, Jin JG. 5-Hydroxytryptamine4 receptor agonists initiate the peristaltic reflex in human, rat, and guinea pig intestine. Gastroenterology. 1998;115:370–80. doi: 10.1016/s0016-5085(98)70203-3. [DOI] [PubMed] [Google Scholar]
- Buchheit KH, Gamse R, Giger R, et al. The serotonin 5-HT4 receptor. 2. Structure-activity studies of the indole carbazimidamide class of agonists. J Med Chem. 1995;38:2331–8. doi: 10.1021/jm00013a010. [DOI] [PubMed] [Google Scholar]
- Buchheit KH, Gamse R, Giger R, et al. The serotonin 5-HT4 receptor. 1. Design of a new class of agonists and receptor map of the agonist recognition site. J Med Chem. 1995;38:2326–30. doi: 10.1021/jm00013a009. [DOI] [PubMed] [Google Scholar]
- Emmanuel AV, Kamm MA, Roy AJ, Antonelli K. Effect of a novel prokinetic drug, R093877, on gastrointestinal transit in healthy volunteers. Gut. 1998;42:511–6. doi: 10.1136/gut.42.4.511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Briejer MR, Prins NH, Schuurkes JA. Effects of the enterokinetic prucalopride (R093877) on colonic motility in fasted dogs. Neurogastroenterol Motil. 2001;13:465–72. doi: 10.1046/j.1365-2982.2001.00280.x. [DOI] [PubMed] [Google Scholar]
- Bouras EP, Camilleri M, Burton DD, McKinzie S. Selective stimulation of colonic transit by the benzofuran 5HT4 agonist, prucalopride, in healthy humans. Gut. 1999;44:682–6. doi: 10.1136/gut.44.5.682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Briejer MR, Bosmans JP, Van Daele P, et al. The in vitro pharmacological profile of prucalopride, a novel enterokinetic compound. Eur J Pharmacol. 2001;423:71–83. doi: 10.1016/s0014-2999(01)01087-1. [DOI] [PubMed] [Google Scholar]
- Smith JA, Beattie DT, Marquess D, Shaw JP, Vickery RG, Humphrey PP. The in vitro pharmacological profile of TD-5108, a selective 5-HT(4) receptor agonist with high intrinsic activity. Naunyn Schmiedebergs Arch Pharmacol. 2008;378:125–37. doi: 10.1007/s00210-008-0282-y. [DOI] [PubMed] [Google Scholar]
- Beattie DT, Armstrong SR, Shaw JP, et al. The in vivo gastrointestinal activity of TD-5108, a selective 5-HT(4) receptor agonist with high intrinsic activity. Naunyn Schmiedebergs Arch Pharmacol. 2008;378:139–47. doi: 10.1007/s00210-008-0281-z. [DOI] [PubMed] [Google Scholar]
- Rao AS, Camilleri M. Review article: metoclopramide and tardive dyskinesia. Aliment Pharmacol Ther. 2010;31:11–9. doi: 10.1111/j.1365-2036.2009.04189.x. [DOI] [PubMed] [Google Scholar]
- Wager E, Tooley PJ, Pearce GL, Wilton LV, Mann RD. A comparison of two cohort studies evaluating the safety of cisapride: Prescription-Event Monitoring and a large phase IV study. Eur J Clin Pharmacol. 1997;52:87–94. doi: 10.1007/s002280050255. [DOI] [PubMed] [Google Scholar]
- Walker AM, Szneke P, Weatherby LB, et al. The risk of serious cardiac arrhythmias among cisapride users in the United Kingdom and Canada. Am J Med. 1999;107:356–62. doi: 10.1016/s0002-9343(99)00241-7. [DOI] [PubMed] [Google Scholar]
- Levy J, Hayes C, Kern J, et al. Does cisapride influence cardiac rhythm? Results of a United States multicenter, double-blind, placebo-controlled pediatric study. J Pediatr Gastroenterol Nutr. 2001;32:458–63. doi: 10.1097/00005176-200104000-00013. [DOI] [PubMed] [Google Scholar]
- Dalby-Payne JR, Morris AM, Craig JC. Meta-analysis of randomized controlled trials on the benefits and risks of using cisapride for the treatment of gastroesophageal reflux in children. J Gastroenterol Hepatol. 2003;18:196–202. doi: 10.1046/j.1440-1746.2003.02948.x. [DOI] [PubMed] [Google Scholar]
- Olsson S, Edwards IR. Tachycardia during cisapride treatment. BMJ. 1992;305:748–9. doi: 10.1136/bmj.305.6856.748-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smalley W, Shatin D, Wysowski DK, et al. Contraindicated use of cisapride: impact of food and drug administration regulatory action. JAMA. 2000;284:3036–9. doi: 10.1001/jama.284.23.3036. [DOI] [PubMed] [Google Scholar]
- Gross AS, Goh YD, Addison RS, Shenfield GM. Influence of grapefruit juice on cisapride pharmacokinetics. Clin Pharmacol Ther. 1999;65:395–401. doi: 10.1016/S0009-9236(99)70133-5. [DOI] [PubMed] [Google Scholar]
- Hancox JC, James AF. Refining insights into high-affinity drug binding to the human ether-a-go-go-related gene potassium channel. Mol Pharmacol. 2008;73:1592–5. doi: 10.1124/mol.108.047563. [DOI] [PubMed] [Google Scholar]
- Di Diego JM, Belardinelli L, Antzelevitch C. Cisapride-induced transmural dispersion of repolarization and torsade de pointes in the canine left ventricular wedge preparation during epicardial stimulation. Circulation. 2003;108:1027–33. doi: 10.1161/01.CIR.0000085066.05180.40. [DOI] [PubMed] [Google Scholar]
- Chhina S, Peverini RL, Deming DD, Hopper AO, Hashmi A, Vyhmeister NR. QTc interval in infants receiving cisapride. J Perinatol. 2002;22:144–8. doi: 10.1038/sj.jp.7210613. [DOI] [PubMed] [Google Scholar]
- Treluyer JM, Rey E, Sonnier M, Pons G, Cresteil T. Evidence of impaired cisapride metabolism in neonates. Br J Clin Pharmacol. 2001;52:419–25. doi: 10.1046/j.0306-5251.2001.01470.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cools F, Benatar A, Bruneel E, et al. A comparison of the pharmacokinetics of two dosing regimens of cisapride and their effects on corrected QT interval in premature infants. Eur J Clin Pharmacol. 2003;59:17–22. doi: 10.1007/s00228-003-0582-6. [DOI] [PubMed] [Google Scholar]
- Kyrmizakis DE, Chimona TS, Kanoupakis EM, Papadakis CE, Velegrakis GA, Helidonis ES. QT prolongation and torsades de pointes associated with concurrent use of cisapride and erythromycin. Am J Otolaryngol. 2002;23:303–7. doi: 10.1053/ajot.2002.124543. [DOI] [PubMed] [Google Scholar]
- Evans AJ, Krentz AJ. Should cisapride be avoided in patients with diabetic gastroparesis? J Diabetes Complications. 1999;13:314–5. doi: 10.1016/s1056-8727(99)00058-6. [DOI] [PubMed] [Google Scholar]
- Gray VS. Syncopal episodes associated with cisapride and concurrent drugs. Ann Pharmacother. 1998;32:648–51. doi: 10.1345/aph.17288. [DOI] [PubMed] [Google Scholar]
- Hatlebakk JG, Johnsson F, Vilien M, Carling L, Wetterhus S, Thogersen T. The effect of cisapride in maintaining symptomatic remission in patients with gastro-oesophageal reflux disease. Scand J Gastroenterol. 1997;32:1100–6. doi: 10.3109/00365529709002988. [DOI] [PubMed] [Google Scholar]
- Lander A, Redkar R, Nicholls G, et al. Cisapride reduces neonatal postoperative ileus: randomised placebo controlled trial. Arch Dis Child Fetal Neonatal Ed. 1997;77:F119–22. doi: 10.1136/fn.77.2.f119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muller-Lissner SA. Treatment of chronic constipation with cisapride and placebo. Gut. 1987;28:1033–8. doi: 10.1136/gut.28.8.1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nurko S, Garcia-Aranda JA, Worona LB, Zlochisty O. Cisapride for the treatment of constipation in children: A double-blind study. J Pediatr. 2000;136:35–40. doi: 10.1016/s0022-3476(00)90046-5. [DOI] [PubMed] [Google Scholar]
- Tack J, Muller-Lissner S. Treatment of chronic constipation: current pharmacologic approaches and future directions. Clin Gastroenterol Hepatol. 2009;7:502–8. doi: 10.1016/j.cgh.2008.12.006. [DOI] [PubMed] [Google Scholar]
- Quigley EM, Wald A, Fidelholtz J, Boivin M, Pecher E, Earnest D. Safety and tolerability of tegaserod in patients with chronic constipation: pooled data from two phase III studies. Clin Gastroenterol Hepatol. 2006;4:605–13. doi: 10.1016/j.cgh.2006.02.017. [DOI] [PubMed] [Google Scholar]
- Fock-Kwong M, Wagner A. Safety, tolerability and satisfaction with tegaserod therapy in Asia-Pacific patients with irritable bowel syndrome with constipation. J Gastroenterol Hepatol. 2007;22:1190–8. doi: 10.1111/j.1440-1746.2007.04955.x. [DOI] [PubMed] [Google Scholar]
- Fried M, Beglinger C, Bobalj NG, Minor N, Coello N, Michetti P. Tegaserod is safe, well tolerated and effective in the treatment of patients with non-diarrhoea irritable bowel syndrome. Eur J Gastroenterol Hepatol. 2005;17:421–7. doi: 10.1097/00042737-200504000-00005. [DOI] [PubMed] [Google Scholar]
- Tougas G, Snape WJ, Jr, Otten MH, et al. Long-term safety of tegaserod in patients with constipation-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2002;16:1701–8. doi: 10.1046/j.1365-2036.2002.01347.x. [DOI] [PubMed] [Google Scholar]
- Muller-Lissner S, Kamm MA, Musoglu A, Earnest DL, Dunger-Baldauf C, Shetzline MA. Safety, tolerability, and efficacy of tegaserod over 13 months in patients with chronic constipation. Am J Gastroenterol. 2006;101:2558–69. doi: 10.1111/j.1572-0241.2006.00789.x. [DOI] [PubMed] [Google Scholar]
- Schoenfeld P. Systematic review: incidence of abdominal/pelvic surgery amongst patients using tegaserod in randomized controlled trials. Aliment Pharmacol Ther. 2004;19:263–9. doi: 10.1111/j.1365-2036.2004.01864.x. [DOI] [PubMed] [Google Scholar]
- Singh G, Mithal A, Kahler K, Shetzline M, Triadafilopoulos G. Patients with irritable bowel syndrome have a high risk of developing colon ischemia [abstract] Gut. 2004;53(Suppl. VI):A66. [Google Scholar]
- Joelsson B, Shetzline MA, Cunningham S. Tegaserod and ischemic colitis. New Engl J Med. 2004;351:1363. [Google Scholar]
- Brinker AD, Mackey AC, Prizont R. Tegaserod and ischemic colitis. N Engl J Med. 2004;351:1361–4. doi: 10.1056/NEJM200409233511324. [DOI] [PubMed] [Google Scholar]
- DiBaise JK. Tegaserod-associated ischemic colitis. Pharmacotherapy. 2005;25:620–5. doi: 10.1592/phco.25.4.620.61032. [DOI] [PubMed] [Google Scholar]
- Wooltorton E. Tegaserod (Zelnorm) for irritable bowel syndrome: reports of serious diarrhea and intestinal ischemia. CMAJ. 2004;170:1908. doi: 10.1503/cmaj.1040882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins PD, Davis KJ, Laine L. Systematic review: the epidemiology of ischaemic colitis. Aliment Pharmacol Ther. 2004;19:729–38. doi: 10.1111/j.1365-2036.2004.01903.x. [DOI] [PubMed] [Google Scholar]
- Morganroth J, Ruegg PC, Dunger-Baldauf C, Appel-Dingemanse S, Bliesath H, Lefkowitz M. Tegaserod, a 5-hydroxytryptamine type 4 receptor partial agonist, is devoid of electrocardiographic effects. Am J Gastroenterol. 2002;97:2321–7. doi: 10.1111/j.1572-0241.2002.05986.x. [DOI] [PubMed] [Google Scholar]
- Anderson JL, May HT, Bair TL, Muhlestein JB, Horne BD, Carlquist JF. Lack of association of tegaserod with adverse cardiovascular outcomes in a matched case-control study. J Cardiovasc Pharmacol Ther. 2009;14:170–5. doi: 10.1177/1074248409340158. [DOI] [PubMed] [Google Scholar]
- Busti AJ, Murillo JR, Jr, Cryer B. Tegaserod-induced myocardial infarction: case report and hypothesis. Pharmacotherapy. 2004;24:526–31. doi: 10.1592/phco.24.5.526.33351. [DOI] [PubMed] [Google Scholar]
- Chan KY, de Vries R, Leijten FP, et al. Functional characterization of contractions to tegaserod in human isolated proximal and distal coronary arteries. Eur J Pharmacol. 2009;619:61–7. doi: 10.1016/j.ejphar.2009.07.010. [DOI] [PubMed] [Google Scholar]
- Scarpellini E, Tack J. Renzapride: a new drug for the treatment of constipation in the irritable bowel syndrome. Expert Opin Investig Drugs. 2008;17:1663–70. doi: 10.1517/13543784.17.11.1663. [DOI] [PubMed] [Google Scholar]
- Alizyme. Press release: Results from Renzapride. April 2008. Available at: http://www.alizyme.com/alizyme/media/press/show.jsp?ref=128. Accessed December 14, 2010.
- Camilleri M, McKinzie S, Fox J, et al. Effect of renzapride on transit in constipation-predominant irritable bowel syndrome. Clin Gastroenterol Hepatol. 2004;2:895–904. doi: 10.1016/s1542-3565(04)00391-x. [DOI] [PubMed] [Google Scholar]
- George AM, Meyers NL, Hickling RI. Clinical trial: renzapride therapy for constipation-predominant irritable bowel syndrome–multicentre, randomized, placebo-controlled, double-blind study in primary healthcare setting. Aliment Pharmacol Ther. 2008;27:830–7. doi: 10.1111/j.1365-2036.2008.03649.x. [DOI] [PubMed] [Google Scholar]
- Spiller RC, Meyers NL, Hickling RI. Identification of patients with non-d, non-C irritable bowel syndrome and treatment with renzapride: an exploratory, multicenter, randomized, double-blind, placebo-controlled clinical trial. Dig Dis Sci. 2008;53:3191–200. doi: 10.1007/s10620-008-0295-x. [DOI] [PubMed] [Google Scholar]
- Tack J, Middleton SJ, Horne MC, et al. Pilot study of the efficacy of renzapride on gastrointestinal motility and symptoms in patients with constipation-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2006;23:1655–65. doi: 10.1111/j.1365-2036.2006.02940.x. [DOI] [PubMed] [Google Scholar]
- Meyers NL, Hickling RI. The cardiovascular safety profile of renzapride, a novel treatment for irritable bowel syndrome. J Int Med Res. 2007;35:848–66. doi: 10.1177/147323000703500613. [DOI] [PubMed] [Google Scholar]
- Mackie AD, Ferrington C, Cowan S, Merrick MV, Baird JD, Palmer KR. The effects of renzapride, a novel prokinetic agent, in diabetic gastroparesis. Aliment Pharmacol Ther. 1991;5:135–42. doi: 10.1111/j.1365-2036.1991.tb00014.x. [DOI] [PubMed] [Google Scholar]
- Motilex Summary of Product Characteristics. Draft, November 2007.
- Karamanolis G, Tack J. Promotility medications – now and in the future. Dig Dis. 2006;24:297–307. doi: 10.1159/000092883. [DOI] [PubMed] [Google Scholar]
- Moayyedi P, Soo S, Deeks J, Delaney B, Innes M, Forman D. Pharmacological interventions for non-ulcer dyspepsia. Cochrane Database Syst Rev. 2011:CD001960. doi: 10.1002/14651858.CD001960. [DOI] [PubMed] [Google Scholar]
- Tonini M, Cipollina L, Poluzzi E, Crema F, Corazza GR, De Ponti F. Review article: clinical implications of enteric and central D2 receptor blockade by antidopaminergic gastrointestinal prokinetics. Aliment Pharmacol Ther. 2004;19:379–90. doi: 10.1111/j.1365-2036.2004.01867.x. [DOI] [PubMed] [Google Scholar]
- Corinaldesi R, Stanghellini V, Raiti C, Zarabini E, Rea E, Paparo GF. Effects of chronic oral administration of clebopride and metoclopramide on gastric emptying of solids in patients with functional dyspepsia. Curr Ther Res. 1985;38:790–7. [Google Scholar]
- Sabbatini F, Minieri M, Manzi G, Piai G, D'Angelo V, Mazzacca G. Clinical efficacy and safety of cisapride and clebopride in the management of chronic functional dyspepsia: a double-blind, randomized study. Ital J Gastroenterol. 1991;23:1–4. [PubMed] [Google Scholar]
- Martinez-Martin P. Transient dyskinesia induced by clebopride. Mov Disord. 1993;8:125–6. doi: 10.1002/mds.870080127. [DOI] [PubMed] [Google Scholar]
- Indo T, Ando K. Metoclopramide-induced Parkinsonism. Clinical characteristics of ten cases. Arch Neurol. 1982;39:494–6. doi: 10.1001/archneur.1982.00510200036006. [DOI] [PubMed] [Google Scholar]
- Sempere AP, Duarte J, Garcia F, Cabezas C, Coria F, Claveria LE. An estimate of the risk of movement disorders associated with the chronic use of clebopride. Mov Disord. 1996;11:582–3. doi: 10.1002/mds.870110518. [DOI] [PubMed] [Google Scholar]
- Kim KS, Shin WH, Park SJ, Kim EJ. Effect of clebopride, antidopaminergic gastrointestinal prokinetics, on cardiac repolarization. Int J Toxicol. 2007;26:25–31. doi: 10.1080/10915810601117992. [DOI] [PubMed] [Google Scholar]
- Yoshida N, Omoya H, Oka M, Furukawa K, Ito T, Karasawa T. AS-4370, a novel gastrokinetic agent free of dopamine D2 receptor antagonist properties. Arch Int Pharmacodyn Ther. 1989;300:51–67. [PubMed] [Google Scholar]
- Yoshida N, Ito T, Karasawa T, Itoh Z. AS-4370, a new gastrokinetic agent, enhances upper gastrointestinal motor activity in conscious dogs. J Pharmacol Exp Ther. 1991;257:781–7. [PubMed] [Google Scholar]
- Yoshida N, Ito T. Mosapride citrate (AS-4370), a new gastroprokinetic agent, is a partial 5-HT4 receptor agonist in the gut. Neurogastroenterol Motil. 1994;6:197–204. [Google Scholar]
- Yoshida N, Omoya H, Kato S, Ito T. Pharmacological effects of the new gastroprokinetic agent mosapride citrate and its metabolites in experimental animals. Arzneimittelforschung. 1993;43:1078–83. [PubMed] [Google Scholar]
- Hallerback BI, Bommelaer G, Bredberg E, et al. Dose finding study of mosapride in functional dyspepsia: a placebo-controlled, randomized study. Aliment Pharmacol Ther. 2002;16:959–67. doi: 10.1046/j.1365-2036.2002.01236.x. [DOI] [PubMed] [Google Scholar]
- Carlsson L, Amos GJ, Andersson B, Drews L, Duker G, Wadstedt G. Electrophysiological characterization of the prokinetic agents cisapride and mosapride in vivo and in vitro: implications for proarrhythmic potential? J Pharmacol Exp Ther. 1997;282:220–7. [PubMed] [Google Scholar]
- Toga T, Kohmura Y, Kawatsu R. The 5-HT(4) agonists cisapride, mosapride, and CJ-033466, a Novel potent compound, exhibit different human ether-a-go-go-related gene (hERG)-blocking activities. J Pharmacol Sci. 2007;105:207–10. doi: 10.1254/jphs.sc0070243. [DOI] [PubMed] [Google Scholar]
- Mushiroda T, Douya R, Takahara E, Nagata O. The involvement of flavin-containing monooxygenase but not CYP3A4 in metabolism of itopride hydrochloride, a gastroprokinetic agent: comparison with cisapride and mosapride citrate. Drug Metab Dispos. 2000;28:1231–7. [PubMed] [Google Scholar]
- Katoh T, Saitoh H, Ohno N, et al. Drug interaction between mosapride and erythromycin without electrocardiographic changes. Jpn Heart J. 2003;44:225–34. doi: 10.1536/jhj.44.225. [DOI] [PubMed] [Google Scholar]
- Endo J, Nomura M, Morishita S, et al. Influence of mosapride citrate on gastric motility and autonomic nervous function: evaluation by spectral analyses of heart rate and blood pressure variabilities, and by electrogastrography. J Gastroenterol. 2002;37:888–95. doi: 10.1007/s005350200150. [DOI] [PubMed] [Google Scholar]
- Horri S, Takeda T, Yasuyuki F, et al. Clinical study on safety of mosapride in combination therapy with psychiatric drugs. Rinsho Iyaku. 2000;16:153. [Google Scholar]
- Ohki R, Takahashi M, Mizuno O, et al. Torsades de pointes ventricular tachycardia induced by mosapride and flecainide in the presence of hypokalemia. Pacing Clin Electrophysiol. 2001;24:119–21. doi: 10.1046/j.1460-9592.2001.00119.x. [DOI] [PubMed] [Google Scholar]
- Briejer MR, Meulemans AL, Bosmans JP. In vitro pharmacology of the novel enterokinetic R093877. Gastroenterology. 1997;112:A705. [Google Scholar]
- Camilleri M, Kerstens R, Rykx A, Vandeplassche L. A placebo-controlled trial of prucalopride for severe chronic constipation. N Engl J Med. 2008;358:2344–54. doi: 10.1056/NEJMoa0800670. [DOI] [PubMed] [Google Scholar]
- Emmanuel AV, Roy AJ, Nicholls TJ, Kamm MA. Prucalopride, a systemic enterokinetic, for the treatment of constipation. Aliment Pharmacol Ther. 2002;16:1347–56. doi: 10.1046/j.1365-2036.2002.01272.x. [DOI] [PubMed] [Google Scholar]
- Quigley EM, Vandeplassche L, Kerstens R, Ausma J. Clinical trial: the efficacy, impact on quality of life, and safety and tolerability of prucalopride in severe chronic constipation–a 12-week, randomized, double-blind, placebo-controlled study. Aliment Pharmacol Ther. 2009;29:315–28. doi: 10.1111/j.1365-2036.2008.03884.x. [DOI] [PubMed] [Google Scholar]
- Tack J, van Outryve M, Beyens G, Kerstens R, Vandeplassche L. Prucalopride (Resolor) in the treatment of severe chronic constipation in patients dissatisfied with laxatives. Gut. 2009;58:357–65. doi: 10.1136/gut.2008.162404. [DOI] [PubMed] [Google Scholar]
- Tack J, Ausma J, Kerstens R, Vandeplassche L. Safety and tolerability of prucalopride (Resolor®) in patients with chronic constipation: Pooled data from three pivotal phase III studies [Abstract T1322] Gastroenterology. 2008;134:A530–1. [Google Scholar]
- Camilleri M, Beyens G, Kerstens R, Vandeplassche L. Long-term follow-up of safety and satisfaction with bowel function in response to oral prucalopride in patients with chronic constipation [Abstract] Gastroenterology. 2009;136(Suppl. 1):160. [Google Scholar]
- Boyce M, Kerstens R, Beyens G, Ausma J, Vandeplassche L. Cardiovascular safety of prucalopride in healthy subjects: results from two randomized, double-blind, placebo-controlled, cross-over trials [Abstract] Gastroenterology. 2009;136(Suppl. 1):T1265. [Google Scholar]
- Camilleri M, Kerstens R, Beyens G, Robinson P, Vandeplassche L. A double-blind, placebo-controlled trial to evaluate the safety and tolerability of prucalopride oral solution in constipated elderly patients living in a nursing facility [Abstract] Gastroenterology. 2009;136(Suppl. 1):240. [Google Scholar]
- Goldberg MR, Li YP, Pitzer K, Johanson JF, Mangel A, Kitt MM. TD-5108 a selective 5-HT4 agonist, is consistently better than placebo regardless of response definition in patients with chronic constipation. Gastroenterology. 2008;134:A547. [Google Scholar]
- Manini ML, Camilleri M, Goldberg M, et al. Effects of velusetrag (TD-5108) on gastrointestinal transit and bowel function in health and pharmacokinetics in health and constipation. Neurogastroenterol Motil. 2010;22:42–9. doi: 10.1111/j.1365-2982.2009.01378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Theravance. Data on file.
- Dennis D, Palme M, Irwin I, Druzgala P, Teichman S. ATI-7505 is a novel, selective 5HT(4) receptor agonist that causes gastrointestinal prokinetic activity in dogs. Gastroenterology. 2004;126:A641. [Google Scholar]
- Palme M, Milner PG, Ellis DJ, Marmon T, Canafax DM. A Novel Gastrointestinal Prokinetic, ATI-7505, Increased Spontaneous Bowel Movements (Sbms) in a Phase II, Randomized, Placebo-Controlled Study of Patients With Chronic Idiopathic Constipation (CIC) Gastroenterology. 2010;138:S128–9. [Google Scholar]
- Aryx Therapeutics. ATI-7505 product fact sheet.
- Aryx Therapeutics. ATI-7505 - Gastrointestinal Disorders. Addressing safety issues of first generation drugs. Available at: http://www.aryx.com/wt/page/ati7505. Accessed December 14, 2010.
- European Agency for the Evaluation of Medicinal Products. Cisapride: Summary of product characteristics, 2002. Available at: www.ema.europa.eu/pdfs/human/referral/cisapride/2484402en.pdf.
- Zhou H, Herron J, Clyde C, Lee P, Mechlinski W, Pesco-Koplowitz L. Pharmacokinetic profile of cisapride 20 mg after once- and twice-daily dosing. Clin Ther. 1998;20:292–8. doi: 10.1016/s0149-2918(98)80092-1. [DOI] [PubMed] [Google Scholar]
- Yamamoto T, Takano K, Sanaka M, et al. Pharmacokinetic characteristics of cisapride in elderly patients. Int J Clin Pharmacol Ther. 1998;36:432–4. [PubMed] [Google Scholar]
- Appel-Dingemanse S, Lemarechal MO, Kumle A, Hubert M, Legangneux E. Integrated modelling of the clinical pharmacokinetics of SDZ HTF 919, a novel selective 5-HT4 receptor agonist, following oral and intravenous administration. Br J Clin Pharmacol. 1999;47:483–91. doi: 10.1046/j.1365-2125.1999.00936.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mims USA. Zelnorm - Detailed Prescribing Information. Available at: http://www.mims.com/USA/drug/info/Zelnorm/Zelnorm%20Tablet?q=tegaserod&type=full. Accessed November 9, 2011.
- Vickers AE, Zollinger M, Dannecker R, Tynes R, Heitz F, Fischer V. In vitro metabolism of tegaserod in human liver and intestine: assessment of drug interactions. Drug Metab Dispos. 2001;29:1269–76. [PubMed] [Google Scholar]
- European Medicines Agency. Refusal Assessment Report for Zelnorm. Doc.Ref.: EMEA/229387/2007. 2006. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/000621/WC500058849.pdf. Accessed November 9, 2011.
- Meyers NL, Hickling RI. Pharmacology and metabolism of renzapride: a novel therapeutic agent for the potential treatment of irritable bowel syndrome. Drugs R D. 2008;9:37–63. doi: 10.2165/00126839-200809010-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson PR, Jones MD, Maddock J, Rees LW. Simultaneous determination of clebopride and a major metabolite N-desbenzylclebopride in plasma by capillary gas chromatography-negative-ion chemical ionization mass spectrometry. J Chromatogr. 1991;564:147–61. doi: 10.1016/0378-4347(91)80077-p. [DOI] [PubMed] [Google Scholar]
- Mims Indonesia. Clast - Detailed Prescribing Information. Available at: http://www.mims.com/Indonesia/drug/info/Clast/Clast%20coated%20tab?type=full#Actions ≤ http://www.mims.com/Indonesia/drug/info/Clast/Clast%20coated%20tab?type=full≥. Accessed December 8, 2011.
- Sun H, Scott DO. Metabolism of 4-aminopiperidine drugs by cytochrome P450s: molecular and quantum mechanical insights into drug design. ACS Med Chem Lett. 2011;2:638–43. doi: 10.1021/ml200117z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Achtert G, Borchers F, Finner E, Hausleiter HJ. Poster presented at the 12th European Workshop on Drug Metabolism. Basel, Switzerland: 1990. Metabolism of clebopride in animals and man. [Google Scholar]
- Sakashita M, Mizuki Y, Yamaguchi T, Miyazaki H, Sekine Y. Pharmacokinetics of the gastrokinetic agent mosapride citrate after intravenous and oral administrations in dogs and monkeys. Arzneimittelforschung. 1993;43:864–6. [PubMed] [Google Scholar]
- Sakashita M, Yamaguchi T, Miyazaki H, et al. Pharmacokinetics of the gastrokinetic agent mosapride citrate after single and multiple oral administrations in healthy subjects. Arzneimittelforschung. 1993;43:867–72. [PubMed] [Google Scholar]
- Dianippon Pharma. Mosapride package insert.
- Bhan CS, Saraswat R. Short review of mosapride: a prokinetic agent. Journal of Global Pharma Technology. 2011;3:1–4. [Google Scholar]
- Shire-Movetis Resolor (prucalopride) Summary of product characteristics. October 2009. Available at: http://www.medicines.org.uk/EMC/history/23206/SPC/Resolor+2mg+film-coated+tablets#03/02/2012 to Current.
- Bowersox SS, Lightning LK, Rao S, et al. Metabolism and pharmacokinetics of naronapride (ATI-7505), a serotonin 5-HT(4) receptor agonist for gastrointestinal motility disorders. Drug Metab Dispos. 2011;39:1170–80. doi: 10.1124/dmd.110.037564. [DOI] [PubMed] [Google Scholar]
- Chen SD, Kao CH, Chang CS, Chen GH. Salivary function in patients with reflux esophagitis: effect of cisapride. J Nucl Med. 1998;39:1449–52. [PubMed] [Google Scholar]
- Orr WC, Chen CL, Sloan S. The role of age and salivation in acid clearance in symptomatic patients with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2001;15:1385–8. doi: 10.1046/j.1365-2036.2001.01080.x. [DOI] [PubMed] [Google Scholar]
- Ceccatelli P, Janssens J, Vantrappen G, Cucchiara S. Cisapride restores the decreased lower oesophageal sphincter pressure in reflux patients. Gut. 1988;29:631–5. doi: 10.1136/gut.29.5.631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corazziari E, Bontempo I, Anzini F. Effects of cisapride on distal esophageal motility in humans. Dig Dis Sci. 1989;34:1600–5. doi: 10.1007/BF01537117. [DOI] [PubMed] [Google Scholar]
- Cucchiara S, Staiano A, Boccieri A, et al. Effects of cisapride on parameters of oesophageal motility and on the prolonged intraoesophageal pH test in infants with gastro-oesophageal reflux disease. Gut. 1990;31:21–5. doi: 10.1136/gut.31.1.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paterson WG, Wang H, Beck IT. The effect of cisapride in patients with reflux esophagitis: an ambulatory esophageal manometry/pH-metry study. Am J Gastroenterol. 1997;92:226–30. [PubMed] [Google Scholar]
- Horowitz M, Maddox A, Harding PE, et al. Effect of cisapride on gastric and esophageal emptying in insulin-dependent diabetes mellitus. Gastroenterology. 1987;92:1899–907. doi: 10.1016/0016-5085(87)90622-6. [DOI] [PubMed] [Google Scholar]
- Gardner JD, Rodriguez-Stanley S, Robinson M, Miner PB., Jr Cisapride inhibits meal-stimulated gastric acid secretion and post-prandial gastric acidity in subjects with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2002;16:1819–29. doi: 10.1046/j.1365-2036.2002.01342.x. [DOI] [PubMed] [Google Scholar]
- Inauen W, Emde C, Weber B, et al. Effects of ranitidine and cisapride on acid reflux and oesophageal motility in patients with reflux oesophagitis: a 24 hour ambulatory combined pH and manometry study. Gut. 1993;34:1025–31. doi: 10.1136/gut.34.8.1025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katschinski M, Schirra J, Arnold R. The efficacy of a 40-mg extended-release formulation of cisapride in the treatment of patients with gastro-oesophageal reflux. Aliment Pharmacol Ther. 2000;14:113–22. doi: 10.1046/j.1365-2036.2000.00672.x. [DOI] [PubMed] [Google Scholar]
- Pouderoux P, Kahrilas PJ. A comparative study of cisapride and ranitidine at controlling oesophageal acid exposure in erosive oesophagitis. Aliment Pharmacol Ther. 1995;9:661–6. doi: 10.1111/j.1365-2036.1995.tb00436.x. [DOI] [PubMed] [Google Scholar]
- Gilbert RJ, Dodds WJ, Kahrilas PJ, Hogan WJ, Lipman S. Effect of cisapride, a new prokinetic agent, on esophageal motor function. Dig Dis Sci. 1987;32:1331–6. doi: 10.1007/BF01296657. [DOI] [PubMed] [Google Scholar]
- Smout AJ, Bogaard JW, Grade AC, ten Thije OJ, Akkermans LM, Wittebol P. Effects of cisapride, a new gastrointestinal prokinetic substance, on interdigestive and postprandial motor activity of the distal oesophagus in man. Gut. 1985;26:246–51. doi: 10.1136/gut.26.3.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Degen L, Petrig C, Studer D, Schroller S, Beglinger C. Effect of tegaserod on gut transit in male and female subjects. Neurogastroenterol Motil. 2005;17:821–6. doi: 10.1111/j.1365-2982.2005.00715.x. [DOI] [PubMed] [Google Scholar]
- Harish K, Hazeena K, Thomas V, Kumar S, Jose T, Narayanan P. Effect of tegaserod on colonic transit time in male patients with constipation-predominant irritable bowel syndrome. J Gastroenterol Hepatol. 2007;22:1183–9. doi: 10.1111/j.1440-1746.2006.04543.x. [DOI] [PubMed] [Google Scholar]
- Bovero E, Poletti M, Vigneri S. The effect of clebopride on esophageal motility: a double-blind randomized manometric study. Curr Ther Res. 1989;46:895–901. [Google Scholar]
- Ruth M, Finizia C, Cange L, Lundell L. The effect of mosapride on oesophageal motor function and acid reflux in patients with gastro-oesophageal reflux disease. Eur J Gastroenterol Hepatol. 2003;15:1115–21. doi: 10.1097/00042737-200310000-00009. [DOI] [PubMed] [Google Scholar]
- Ruth M, Hamelin B, Rohss K, Lundell L. The effect of mosapride, a novel prokinetic, on acid reflux variables in patients with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 1998;12:35–40. doi: 10.1046/j.1365-2036.1998.00268.x. [DOI] [PubMed] [Google Scholar]
- Wallin L, Kruse-Andersen S, Madsen T, Boesby S. Effect of cisapride on the gastro-oesophageal function in normal human subjects. Digestion. 1987;37:160–5. doi: 10.1159/000199494. [DOI] [PubMed] [Google Scholar]
- Finizia C, Lundell L, Cange L, Ruth M. The effect of cisapride on oesophageal motility and lower sphincter function in patients with gastro-oesophageal reflux disease. Eur J Gastroenterol Hepatol. 2002;14:9–14. doi: 10.1097/00042737-200201000-00003. [DOI] [PubMed] [Google Scholar]
- Cho YK, Choi MG, Han HW, et al. The effect of mosapride on esophageal motility and bolus transit in asymptomatic volunteers. J Clin Gastroenterol. 2006;40:286–92. doi: 10.1097/01.mcg.0000210103.82241.97. [DOI] [PubMed] [Google Scholar]
- Vantrappen G, Kortan P, Janssens J. The effect of clebopride on lower esophageal sphincter pressure in normal subjects. Curr Ther Res. 1985;37:284–94. [Google Scholar]
- Pehlivanov N, Sarosiek I, Whitman R, Olyaee M, McCallum R. Effect of cisapride on nocturnal transient lower oesophageal sphincter relaxations and nocturnal gastro-oesophageal reflux in patients with oesophagitis: a double-blind, placebo-controlled study. Aliment Pharmacol Ther. 2002;16:743–7. doi: 10.1046/j.1365-2036.2002.01225.x. [DOI] [PubMed] [Google Scholar]
- Holloway RH, Downton J, Mitchell B, Dent J. Effect of cisapride on postprandial gastro-oesophageal reflux. Gut. 1989;30:1187–93. doi: 10.1136/gut.30.9.1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smythe A, Bird NC, Troy GP, Ackroyd R, Johnson AG. Does the addition of a prokinetic to proton pump inhibitor therapy help reduce duodenogastro-oesophageal reflux in patients with Barrett's oesophagus? Eur J Gastroenterol Hepatol. 2003;15:305–12. doi: 10.1097/00042737-200303000-00014. [DOI] [PubMed] [Google Scholar]
- Chen JD, Ke MY, Lin XM, Wang Z, Zhang M. Cisapride provides symptomatic relief in functional dyspepsia associated with gastric myoelectrical abnormality. Aliment Pharmacol Ther. 2000;14:1041–7. doi: 10.1046/j.1365-2036.2000.00801.x. [DOI] [PubMed] [Google Scholar]
- Besherdas K, Leahy A, Mason I, Harbord M, Epstein O. The effect of cisapride on dyspepsia symptoms and the electrogastrogram in patients with non-ulcer dyspepsia. Aliment Pharmacol Ther. 1998;12:755–9. doi: 10.1046/j.1365-2036.1998.00369.x. [DOI] [PubMed] [Google Scholar]
- Borovicka J, Lehmann R, Kunz P, et al. Evaluation of gastric emptying and motility in diabetic gastroparesis with magnetic resonance imaging: effects of cisapride. Am J Gastroenterol. 1999;94:2866–73. doi: 10.1111/j.1572-0241.1999.01392.x. [DOI] [PubMed] [Google Scholar]
- Jones KL, Horowitz M, Carney BI, Sun WM, Chatterton BE. Effects of cisapride on gastric emptying of oil and aqueous meal components, hunger, and fullness. Gut. 1996;38:310–5. doi: 10.1136/gut.38.3.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazzaroni M, Sangaletti O, Bianchi Porro G. Effect of cisapride on gastric emptying and ileal transit time of balanced liquid meal in healthy subjects. Digestion. 1987;37:110–3. doi: 10.1159/000199476. [DOI] [PubMed] [Google Scholar]
- Fraser RJ, Horowitz M, Maddox AF, Dent J. Postprandial antropyloroduodenal motility and gastric emptying in gastroparesis – effects of cisapride. Gut. 1994;35:172–8. doi: 10.1136/gut.35.2.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stacher G, Granser GV, Bergmann H, Kugi A, Stacher-Janotta G, Hobart J. Slow gastric emptying induced by high fat content of meal accelerated by cisapride administered rectally. Dig Dis Sci. 1991;36:1259–65. doi: 10.1007/BF01307519. [DOI] [PubMed] [Google Scholar]
- Camilleri M, Malagelada JR, Abell TL, Brown ML, Hench V, Zinsmeister AR. Effect of six weeks of treatment with cisapride in gastroparesis and intestinal pseudoobstruction. Gastroenterology. 1989;96:704–12. [PubMed] [Google Scholar]
- Jian R, Ducrot F, Piedeloup C, Mary JY, Najean Y, Bernier JJ. Measurement of gastric emptying in dyspeptic patients: effect of a new gastrokinetic agent (cisapride) Gut. 1985;26:352–8. doi: 10.1136/gut.26.4.352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feldman M, Smith HJ. Effect of cisapride on gastric emptying of indigestible solids in patients with gastroparesis diabeticorum. A comparison with metoclopramide and placebo. Gastroenterology. 1987;92:171–4. doi: 10.1016/0016-5085(87)90854-7. [DOI] [PubMed] [Google Scholar]
- Kawagishi T, Nishizawa Y, Okuno Y, Sekiya K, Morii H. Effect of cisapride on gastric emptying of indigestible solids and plasma motilin concentration in diabetic autonomic neuropathy. Am J Gastroenterol. 1993;88:933–8. [PubMed] [Google Scholar]
- Richards RD, Valenzuela GA, Davenport KG, Fisher KL, McCallum RW. Objective and subjective results of a randomized, double-blind, placebo-controlled trial using cisapride to treat gastroparesis. Dig Dis Sci. 1993;38:811–6. doi: 10.1007/BF01295905. [DOI] [PubMed] [Google Scholar]
- Corinaldesi R, Stanghellini V, Raiti C, Rea E, Salgemini R, Barbara L. Effect of chronic administration of cisapride on gastric emptying of a solid meal and on dyspeptic symptoms in patients with idiopathic gastroparesis. Gut. 1987;28:300–5. doi: 10.1136/gut.28.3.300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abell TL, Camilleri M, DiMagno EP, Hench VS, Zinsmeister AR, Malagelada JR. Long-term efficacy of oral cisapride in symptomatic upper gut dysmotility. Dig Dis Sci. 1991;36:616–20. doi: 10.1007/BF01297028. [DOI] [PubMed] [Google Scholar]
- Stacher G, Bergmann H, Wiesnagrotzki S, et al. Intravenous cisapride accelerates delayed gastric emptying and increases antral contraction amplitude in patients with primary anorexia nervosa. Gastroenterology. 1987;92:1000–6. doi: 10.1016/0016-5085(87)90976-0. [DOI] [PubMed] [Google Scholar]
- Heyland DK, Tougas G, Cook DJ, Guyatt GH. Cisapride improves gastric emptying in mechanically ventilated, critically ill patients. A randomized, double-blind trial. Am J Respir Crit Care Med. 1996;154:1678–83. doi: 10.1164/ajrccm.154.6.8970354. [DOI] [PubMed] [Google Scholar]
- Maddern GJ, Jamieson GG, Myers JC, Collins PJ. Effect of cisapride on delayed gastric emptying in gastro-oesophageal reflux disease. Gut. 1991;32:470–4. doi: 10.1136/gut.32.5.470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Di Lorenzo C, Reddy SN, Villanueva-Meyer J, Mena I, Martin S, Hyman PE. Cisapride in children with chronic intestinal pseudoobstruction. An acute, double-blind, crossover, placebo-controlled trial. Gastroenterology. 1991;101:1564–70. doi: 10.1016/0016-5085(91)90393-y. [DOI] [PubMed] [Google Scholar]
- Stacher G, Schernthaner G, Francesconi M, et al. Cisapride versus placebo for 8 weeks on glycemic control and gastric emptying in insulin-dependent diabetes: a double blind cross-over trial. J Clin Endocrinol Metab. 1999;84:2357–62. doi: 10.1210/jcem.84.7.5859. [DOI] [PubMed] [Google Scholar]
- McClure RJ, Kristensen JH, Grauaug A. Randomised controlled trial of cisapride in preterm infants. Arch Dis Child Fetal Neonatal Ed. 1999;80:F174–7. doi: 10.1136/fn.80.3.f174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wei W, Ge ZZ, Lu H, Gao YJ, Hu YB, Xiao SD. Effect of mosapride on gastrointestinal transit time and diagnostic yield of capsule endoscopy. J Gastroenterol Hepatol. 2007;22:1605–8. doi: 10.1111/j.1440-1746.2007.05064.x. [DOI] [PubMed] [Google Scholar]
- Kanaizumi T, Nakano H, Matsui Y, et al. Prokinetic effect of AS-4370 on gastric emptying in healthy adults. Eur J Clin Pharmacol. 1991;41:335–7. doi: 10.1007/BF00314963. [DOI] [PubMed] [Google Scholar]
- Yamada M, Hongo M, Okuno Y, et al. Effect of AS-4370 on gastric motility in patients with diabetic autonomic neuropathy. J Smooth Muscle Res. 1992;28:153–8. doi: 10.1540/jsmr.28.153. [DOI] [PubMed] [Google Scholar]
- Asai H, Udaka F, Hirano M, et al. Increased gastric motility during 5-HT4 agonist therapy reduces response fluctuations in Parkinson's disease. Parkinsonism Relat Disord. 2005;11:499–502. doi: 10.1016/j.parkreldis.2005.06.007. [DOI] [PubMed] [Google Scholar]
- Manini ML, Camilleri M, Goldberg M, et al. Effects of Velusetrag (TD-5108) on gastrointestinal transit and bowel function in health and pharmacokinetics in health and constipation. Neurogastroenterol Motil. 2010;22:42–9. doi: 10.1111/j.1365-2982.2009.01378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tack J, Broeckaert D, Coulie B, Janssens J. The influence of cisapride on gastric tone and the perception of gastric distension. Aliment Pharmacol Ther. 1998;12:761–6. doi: 10.1046/j.1365-2036.1998.00366.x. [DOI] [PubMed] [Google Scholar]
- Manes G, Dominguez-Munoz JE, Leodolter A, Malfertheiner P. Effect of cisapride on gastric sensitivity to distension, gastric compliance and duodeno-gastric reflexes in healthy humans. Dig Liver Dis. 2001;33:407–13. doi: 10.1016/s1590-8658(01)80012-8. [DOI] [PubMed] [Google Scholar]
- Thumshirn M, Fruehauf H, Stutz B, Tougas G, Salter J, Fried M. Clinical trial: effects of tegaserod on gastric motor and sensory function in patients with functional dyspepsia. Aliment Pharmacol Ther. 2007;26:1399–407. doi: 10.1111/j.1365-2036.2007.03521.x. [DOI] [PubMed] [Google Scholar]
- Bouras EP, Camilleri M, Burton DD, Thomforde G, McKinzie S, Zinsmeister AR. Prucalopride accelerates gastrointestinal and colonic transit in patients with constipation without a rectal evacuation disorder. Gastroenterology. 2001;120:354–60. doi: 10.1053/gast.2001.21166. [DOI] [PubMed] [Google Scholar]
- Elorza JM, Capdevila C. Double-blind parallel comparison of the gastrokinetic effects of clebopride, domperidone and placebo in human volunteers with gastric stasis induced by glucagon. Curr Ther Res. 1982;31:S58–60. [Google Scholar]
- Verhagen MA, Roelofs JM, Edelbroek MA, Smout AJ, Akkermans LM. The effect of cisapride on duodenal acid exposure in the proximal duodenum in healthy subjects. Aliment Pharmacol Ther. 1999;13:621–30. doi: 10.1046/j.1365-2036.1999.00520.x. [DOI] [PubMed] [Google Scholar]
- Rezende-Filho J, Di Lorenzo C, Dooley CP, Valenzuela JE. Cisapride stimulates antral motility and decreases biliary reflux in patients with severe dyspepsia. Dig Dis Sci. 1989;34:1057–62. doi: 10.1007/BF01536374. [DOI] [PubMed] [Google Scholar]
- Testoni PA, Bagnolo F, Fanti L, Passaretti S, Tittobello A. Longterm oral cisapride improves interdigestive antroduodenal motility in dyspeptic patients. Gut. 1990;31:286–90. doi: 10.1136/gut.31.3.286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaezi MF, Sears R, Richter JE. Placebo-controlled trial of cisapride in postgastrectomy patients with duodenogastroesophageal reflux. Dig Dis Sci. 1996;41:754–63. doi: 10.1007/BF02213132. [DOI] [PubMed] [Google Scholar]
- Marzio L, DiGiammarco AM, Capone F, et al. Effect of cisapride on human fasting gallbladder volume: a real-time ultrasonographic study. Eur J Clin Pharmacol. 1986;29:631–3. doi: 10.1007/BF00635906. [DOI] [PubMed] [Google Scholar]
- Takaoka M, Kubota Y, Fujimura K, et al. Effect of single and multiple administrations of cisapride on postprandial gallbladder emptying in healthy humans. Intern Med. 1994;33:381–6. doi: 10.2169/internalmedicine.33.381. [DOI] [PubMed] [Google Scholar]
- Coremans G, Janssens J, Vantrappen G, Chaussade S, Ceccatelli P. Cisapride stimulates propulsive motility patterns in human jejunum. Dig Dis Sci. 1988;33:1512–9. doi: 10.1007/BF01535939. [DOI] [PubMed] [Google Scholar]
- Evans PR, Bak YT, Kellow JE. Effects of oral cisapride on small bowel motility in irritable bowel syndrome. Aliment Pharmacol Ther. 1997;11:837–44. doi: 10.1046/j.1365-2036.1997.00240.x. [DOI] [PubMed] [Google Scholar]
- Stacher G, Gaupmann G, Mittelbach G, Schneider C, Steinringer H, Langer B. Effects of oral cisapride on interdigestive jejunal motor activity, psychomotor function, and side-effect profile in healthy man. Dig Dis Sci. 1987;32:1223–30. doi: 10.1007/BF01296370. [DOI] [PubMed] [Google Scholar]
- Stacher G, Steinringer H, Schneider C, Winklehner S, Mittelbach G, Gaupmann G. Effects of cisapride on jejunal motor activity in fasting healthy humans. Gastroenterology. 1986;90:1210–6. doi: 10.1016/0016-5085(86)90387-2. [DOI] [PubMed] [Google Scholar]
- Noor N, Small PK, Loudon MA, Hau C, Campbell FC. Effects of cisapride on symptoms and postcibal small-bowel motor function in patients with irritable bowel syndrome. Scand J Gastroenterol. 1998;33:605–11. doi: 10.1080/00365529850171873. [DOI] [PubMed] [Google Scholar]
- Camilleri M, Brown ML, Malagelada JR. Impaired transit of chyme in chronic intestinal pseudoobstruction. Correction by cisapride. Gastroenterology. 1986;91:619–26. doi: 10.1016/0016-5085(86)90631-1. [DOI] [PubMed] [Google Scholar]
- Krevsky B, Malmud LS, Maurer AH, Somers MB, Siegel JA, Fisher RS. The effect of oral cisapride on colonic transit. Aliment Pharmacol Ther. 1987;1:293–304. doi: 10.1111/j.1365-2036.1987.tb00629.x. [DOI] [PubMed] [Google Scholar]
- Bak YT, Kim JH, Lee CH. Cisapride in chronic idiopathic constipation: clinical response and effect on colonic transit time. Korean J Intern Med. 1996;11:151–6. doi: 10.3904/kjim.1996.11.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krevsky B, Maurer AH, Malmud LS, Fisher RS. Cisapride accelerates colonic transit in constipated patients with colonic inertia. Am J Gastroenterol. 1989;84:882–7. [PubMed] [Google Scholar]
- Jost WH, Schimrigk K. The effect of cisapride on delayed colonic transit time in patients with idiopathic Parkinson's disease. Wien Klin Wochenschr. 1994;106:673–6. [PubMed] [Google Scholar]
- Geders JM, Gaing A, Bauman WA, Korsten MA. The effect of cisapride on segmental colonic transit time in patients with spinal cord injury. Am J Gastroenterol. 1995;90:285–9. [PubMed] [Google Scholar]
- Roberts JP, Benson MJ, Rogers J, Deeks JJ, Wingate DL, Williams NS. Effect of cisapride on distal colonic motility in the early postoperative period following left colonic anastomosis. Dis Colon Rectum. 1995;38:139–45. doi: 10.1007/BF02052441. [DOI] [PubMed] [Google Scholar]
- Poen AC, Felt-Bersma RJ, Van Dongen PA, Meuwissen SG. Effect of prucalopride, a new enterokinetic agent, on gastrointestinal transit and anorectal function in healthy volunteers. Aliment Pharmacol Ther. 1999;13:1493–7. doi: 10.1046/j.1365-2036.1999.00629.x. [DOI] [PubMed] [Google Scholar]
- Sloots CE, Poen AC, Kerstens R, et al. Effects of prucalopride on colonic transit, anorectal function and bowel habits in patients with chronic constipation. Aliment Pharmacol Ther. 2002;16:759–67. doi: 10.1046/j.1365-2036.2002.01210.x. [DOI] [PubMed] [Google Scholar]
- Coffin B, Farmachidi JP, Rueegg P, Bastie A, Bouhassira D. Tegaserod, a 5-HT4 receptor partial agonist, decreases sensitivity to rectal distension in healthy subjects. Aliment Pharmacol Ther. 2003;17:577–85. doi: 10.1046/j.1365-2036.2003.01449.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional Supporting Information may be found in the online version of this article:
Table S1. Clinical trials on the efficacy of cisapride in GI conditions.
Table S2. Clinical trials on the efficacy of tegaserod in GI conditions.
Table S3. Clinical trials on the efficacy of renzapride in irritable bowel syndrome.
Table S4. Clinical trials on the efficacy of clebopride in GI conditions.
Table S5. Clinical trials on the efficacy of mosapride in GI conditions.
Table S6. Clinical trials on the efficacy of prucalopride in GI conditions.
Table S7. Clinical trials on the efficacy of velusetrag in chronic constipation.
Please note: Wiley-Blackwell are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.