

Abstract
This article reports a type II Salter and Harris injury at either ends of the clavicle in a 13-year-old child with postero-inferior displacement at the lateral and antero-superior displacement at the medial end of the clavicle shaft. He was treated in a shoulder immobilizer. The mechanism of injury is postulated as pivoting of the clavicle on the first rib with shearing at either ends leading to a bipolar injury. The brachial plexus and subclavian vessels are at a risk of damage at the pivot as they lie in close vicinity to the first rib. In view of the intact periosteal sleeve as well as joint articulation at both ends, the fracture healed with no functional loss.
Keywords: Shoulder girdle, clavicle, fracture, bipolar physeal injury
INTRODUCTION
Clavicle is one of the commonest bones to fracture in a child.1 Though physeal injuries of this bone are uncommon, a few reports of ipsilateral fracture or dislocation along with fracture of the medial physis of the clavicle exist.2–4 In most of the medial physeal injuries, the displacement of the fragment is posterior when the force is direct.5 Reports of anterior clavicular displacements in association with posterior acromioclavicular dislocation have been cited in children and adolescents.2
A simultaneous ipsilateral physeal fracture displacement of both ends of clavicle has not been reported yet, to the best of our knowledge. We report a case of a 13-year-old boy who sustained type II Salter and Harris physeal injury at either ends of the clavicle with anterior displacement of the medial and posterior displacement of the lateral end of the clavicular shaft. The mechanism of injury, radiology, and management of this unreported injury are discussed here.
CASE REPORT
A 13-year-old boy presented to us with pain in the left shoulder and chest, after allegedly being hit by a sport utility vehicle. The child was asleep, semi-prone with left shoulder up on a pavement when he was hit on his left shoulder by the vehicle.
He was brought awake, oriented to time, place and person to the emergency department 2 hours after injury. His blood pressure was 118/82 mm of mercury, and pulse was regular with a rate of 103 per minute. An ovoid, tender swelling was present over the left sternoclavicular joint [Figure 1]. There was tenderness over the lateral end of clavicle and difficulty in moving the ipsilateral shoulder. He complained of numbness over the medial aspect of upper forearm. There were no abrasions or tyre marks. A serendipity view radiograph of the Left side [Figure 2a] showed displacement of the medial fractured end of the clavicle with the proximal epiphyseal fragment in situ. The lateral epiphyseal end too remained in continuity with the joint while the fractured proximal fragment was displaced inferiorly and posteriorly. The serendipity view (40° cephalic tilt view) is considered the next best thing to a true cephalocaudal lateral view of the sternoclavicular joint.6 A Computed Tomography revealed a bipolar physeal injury of the left clavicle [Figure 2b]. The middle floating shaft fragment had displaced anterosuperiorly at its medial end and posteroinferiorly at its lateral end. The Thurston Holland fragment was visualized at either ends [Figure 2a].7
Figure 1.
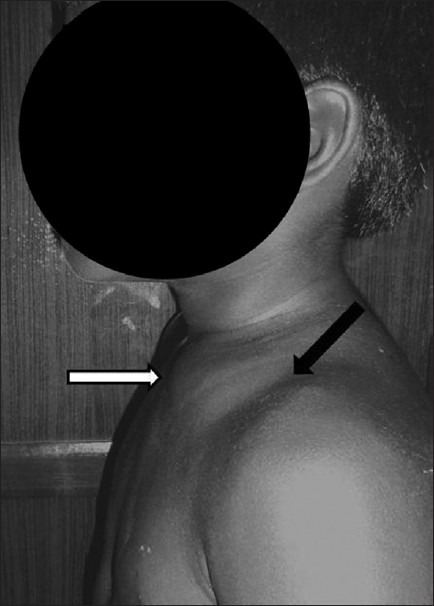
Clinical photograph showing the prominence above the medial end of clavicle represents anterosuperior displacement of the shaft (white arrow), and the depression above the lateral end of clavicle indicates the inferior displacement (black arrow)
Figure 2.
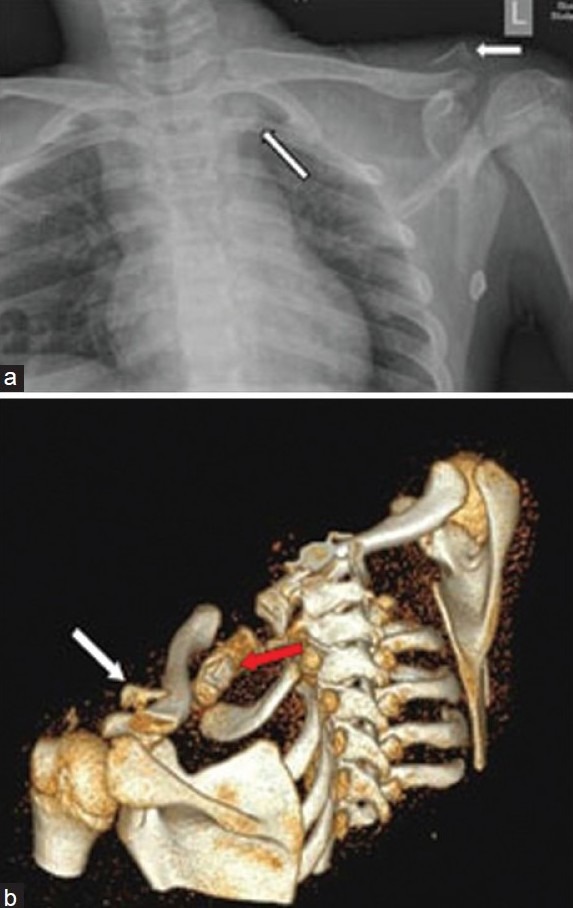
(a) X-ray serendipity view showing the triangular metaphyseal fragments (white arrows) representing the Thurston Holland fragment attached to the clavicular physes adjacent to sternoclavicular and acromioclavicular joint (b) 3-D reconstruction CT scan showing the displacements of either ends of the left clavicle (red and white arrows) in an anteroposterior plane
An initial attempt to reduce the medial physeal fracture failed, probably because of the floating intermediate segment which failed to transmit the reduction force. The position was accepted in view of the reported natural history of similar physeal injuries at either ends of the clavicle and the child was treated in a shoulder immobilizer. The parasthesia resolved over the next 2 days. The child was followed up at 2, 6, and 18 months. There was no sensory deficit at 2 months. At 18 months, the child had full range of movements at the shoulder and radiographs showed periosteal remodeling at either end with no joint incongruity [Figure 3].
Figure 3.
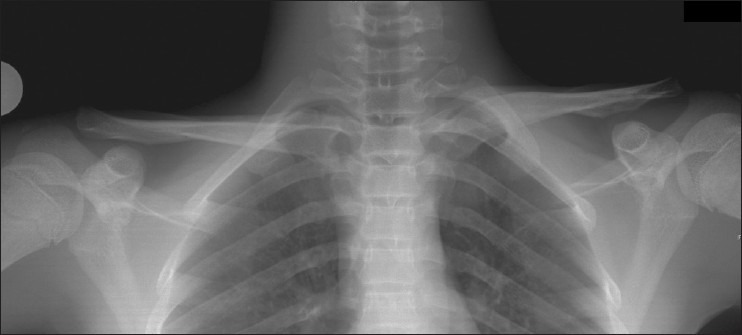
X-ray serendipity view 18 months after injury shows periosteal remodeling with normal sternoclavicular and acromioclavicular articulation
DISCUSSION
Physeal injuries of clavicle are seen in children and young adults. The physis of the clavicle closes at 22–25 years of age at the medial and until 18–19 years at the lateral end.8 Both medial and lateral physeal injuries are reported. A simultaneous physeal injury to either ends, however, has not been reported previously in the English literature to the best of our knowledge.
The mechanism of such an injury can be postulated from similar joint injuries in adults wherein a posteriorly directed force at the shoulder girdle causes anterior dislocation of the sternal end of the clavicle.9 A force applied to the lateral end of the clavicle in a posteroinferior direction, as inferred in our case, would result in the clavicle pivoting against the first rib (fulcrum), causing failure at the medial clavicular physis. With continued force, the lateral end would fail. The physis, being weaker in children, gives way [Figure 4]. An injury of such magnitude will incite damage to the adjacent neurovascular structures. The first rib being the pivot, the neurovascular structures overlying it would be amenable to serious injury. The downward and posterior displacement of the lateral end of the clavicular shaft would endanger the thoracic viscera.5 In our patient, a transient sensory loss on the medial aspect of forearm was recorded, suggestive of a neuropraxia. The surgeon should therefore be watchful for such associated injuries.
Figure 4.
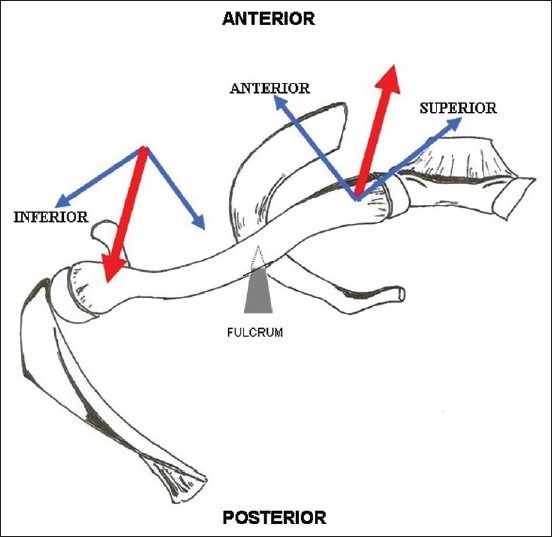
A schematic diagram showing postulated mechanism of bipolar physeal injury: F1 and F2 are the forces and the reaction creating a torque which pivots over the underlying first rib (fulcrum). The vectors, represented by blue arrows, show the resultant displacement of ends of the floating segment
A serendipity view gives a good radiological definition of the displacements. However, a duplex ultrasound and CT scan examination would be ideal for a more detailed profile when there are associated injuries.10
Physeal injuries in children are associated with an intact periosteal sleeve and no joint incongruity. Hence, excellent remodeling and function is expected. Our patient was treated with an immobilizer and it was adequate to prevent discomfort due to movement. A review of the recommendations for isolated physeal injuries for either ends of the clavicle suggests that an operative fixation is not necessary unless there is a neurovascular or soft tissue compromise or late complications.9,11 Ogden has reported duplication of the clavicle and a prominent bump which may require removal for cosmesis, but this was not necessary in our patient.12 Our patient shows duplication at both ends, which is expected to remodel with time.
We report a physeal injury at both clavicular ends with possible mechanism of pivoting of clavicle on the first rib secondary to a posteroinferiorly directed force applied to the shoulder. The articulation at both ends of the clavicle remains intact and stability is ensured by virtue of its ligamentous attachments and an intact periosteum. Hence, if uncomplicated, this injury may not require surgical intervention.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Rennie L, Court-Brown CM, Mok JY, Beattie TF. The epidemiology of fractures in children. Injury. 2007;38:913–22. doi: 10.1016/j.injury.2007.01.036. [DOI] [PubMed] [Google Scholar]
- 2.Wade AM, Barret MO, Crist BD, Rocca GJ, Kane SM. Medial clavicular epiphyseal fracture with ipsilateral acromioclavicular dislocation: A case report of panclavicular fracture dislocation. J Orthop Trauma. 2007;21:418–21. doi: 10.1097/BOT.0b013e3180dca5ad. [DOI] [PubMed] [Google Scholar]
- 3.Lampasi M, Bochicchio V, Bettuzzi C, Donzelli O. Sternoclavicular physeal fracture associated with adjacent clavicle fracture in a 14-year-old boy: A case report and literature review. Knee Surg Sports Traumatol Arthrosc. 2008;16:699–702. doi: 10.1007/s00167-008-0495-0. [DOI] [PubMed] [Google Scholar]
- 4.Allen BF, Jr, Zielinski CJ. Posterior fracture through the sternoclavicular physis associated with a clavicle fracture: a case report and literature review. Am J Orthop. 1999;28:598–600. [PubMed] [Google Scholar]
- 5.Wirth MA, Rockwood CA., Jr . Rockwood and Wilkins’ Fractures in Children. 7th Ed. Philadelphia: Lippincott Williams and Wilkins; 2009. Sternoclavicular joint injuries. [Google Scholar]
- 6.Spencer ER, Jr, Wirth MA, Rockwood CA., Jr . Disorders of the shoulder: Diagnosis and management. 2nd Ed. Vol. 2. Lippincott Williams & Wilkins; 2007. Disorders of the sternoclavicular joint: Pathology, diagnosis and management. [Google Scholar]
- 7.RB Salter, WR Harris. Injuries involving the eiphyseal plate. J Bone Joint Surg. 1963;45A:587–632. [Google Scholar]
- 8.Sarwark JF, King EC, Luhmann SJ. Rockwood and Wilkins’ Fractures in Children. 6th Edition. Philadelphia: Lippincott Williams and Wilkins; 2006. Proximal Humerus, Scapula, and Clavicle. [Google Scholar]
- 9.Bahk MS, Kuhn JE, Galatz LM, Connor PM, Williams GR., Jr Acromioclavicular and sternoclavicular injuries and clavicular, Glenoid, and scapular fractures. J Bone Joint Surg Am. 2009;91:2492–510. [PubMed] [Google Scholar]
- 10.Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am. 2009;91:447–60. doi: 10.2106/JBJS.H.00034. [DOI] [PubMed] [Google Scholar]
- 11.Kubiak R, Slongo T. Operative treatment of clavicle fractures in children: A review of 21 Years. J Pediatr Orthop. 2002;22:736–9. [PubMed] [Google Scholar]
- 12.Ogden JA. Distal clavicular physeal injury. Clin Orthop Relat Res. 1984;188:68–73. [PubMed] [Google Scholar]