

Abstract
Background: Although fluoride may cause neurotoxicity in animal models and acute fluoride poisoning causes neurotoxicity in adults, very little is known of its effects on children’s neurodevelopment.
Objective: We performed a systematic review and meta-analysis of published studies to investigate the effects of increased fluoride exposure and delayed neurobehavioral development.
Methods: We searched the MEDLINE, EMBASE, Water Resources Abstracts, and TOXNET databases through 2011 for eligible studies. We also searched the China National Knowledge Infrastructure (CNKI) database, because many studies on fluoride neurotoxicity have been published in Chinese journals only. In total, we identified 27 eligible epidemiological studies with high and reference exposures, end points of IQ scores, or related cognitive function measures with means and variances for the two exposure groups. Using random-effects models, we estimated the standardized mean difference between exposed and reference groups across all studies. We conducted sensitivity analyses restricted to studies using the same outcome assessment and having drinking-water fluoride as the only exposure. We performed the Cochran test for heterogeneity between studies, Begg’s funnel plot, and Egger test to assess publication bias, and conducted meta-regressions to explore sources of variation in mean differences among the studies.
Results: The standardized weighted mean difference in IQ score between exposed and reference populations was –0.45 (95% confidence interval: –0.56, –0.35) using a random-effects model. Thus, children in high-fluoride areas had significantly lower IQ scores than those who lived in low-fluoride areas. Subgroup and sensitivity analyses also indicated inverse associations, although the substantial heterogeneity did not appear to decrease.
Conclusions: The results support the possibility of an adverse effect of high fluoride exposure on children’s neurodevelopment. Future research should include detailed individual-level information on prenatal exposure, neurobehavioral performance, and covariates for adjustment.
Keywords: fluoride, intelligence, neurotoxicity
A recent report from the National Research Council (NRC 2006) concluded that adverse effects of high fluoride concentrations in drinking water may be of concern and that additional research is warranted. Fluoride may cause neurotoxicity in laboratory animals, including effects on learning and memory (Chioca et al. 2008; Mullenix et al. 1995). A recent experimental study where the rat hippocampal neurons were incubated with various concentrations (20 mg/L, 40 mg/L, and 80 mg/L) of sodium fluoride in vitro showed that fluoride neurotoxicity may target hippocampal neurons (Zhang M et al. 2008). Although acute fluoride poisoning may be neurotoxic to adults, most of the epidemiological information available on associations with children’s neurodevelopment is from China, where fluoride generally occurs in drinking water as a natural contaminant, and the concentration depends on local geological conditions. In many rural communities in China, populations with high exposure to fluoride in local drinking-water sources may reside in close proximity to populations without high exposure (NRC 2006).
Opportunities for epidemiological studies depend on the existence of comparable population groups exposed to different levels of fluoride from drinking water. Such circumstances are difficult to find in many industrialized countries, because fluoride concentrations in community water are usually no higher than 1 mg/L, even when fluoride is added to water supplies as a public health measure to reduce tooth decay. Multiple epidemiological studies of developmental fluoride neurotoxicity were conducted in China because of the high fluoride concentrations that are substantially above 1 mg/L in well water in many rural communities, although microbiologically safe water has been accessible to many rural households as a result of the recent 5-year plan (2001–2005) by the Chinese government. It is projected that all rural residents will have access to safe public drinking water by 2020 (World Bank 2006). However, results of the published studies have not been widely disseminated. Four studies published in English (Li XS et al. 1995; Lu et al. 2000; Xiang et al. 2003; Zhao et al. 1996) were cited in a recent report from the NRC (2006), whereas the World Health Organization (2002) has considered only two (Li XS et al. 1995; Zhao et al. 1996) in its most recent monograph on fluoride.
Fluoride readily crosses the placenta (Agency for Toxic Substances and Disease Registry 2003). Fluoride exposure to the developing brain, which is much more susceptible to injury caused by toxicants than is the mature brain, may possibly lead to permanent damage (Grandjean and Landrigan 2006). In response to the recommendation of the NRC (2006), the U.S. Department of Health and Human Services (DHHS) and the U.S. EPA recently announced that DHHS is proposing to change the recommended level of fluoride in drinking water to 0.7 mg/L from the currently recommended range of 0.7–1.2 mg/L, and the U.S. EPA is reviewing the maximum amount of fluoride allowed in drinking water, which currently is set at 4.0 mg/L (U.S. EPA 2011).
To summarize the available literature, we performed a systematic review and meta-analysis of published studies on increased fluoride exposure in drinking water associated with neurodevelopmental delays. We specifically targeted studies carried out in rural China that have not been widely disseminated, thus complementing the studies that have been included in previous reviews and risk assessment reports.
Methods
Search strategy. We searched MEDLINE (National Library of Medicine, Bethesda, MD, USA; http://www.ncbi.nlm.nih.gov/pubmed), Embase (Elsevier B.V., Amsterdam, the Netherlands; http://www.embase.com), Water Resources Abstracts (Proquest, Ann Arbor, MI, USA; http://www.csa.com/factsheets/water-resources-set-c.php), and TOXNET (Toxicology Data Network; National Library of Medicine, Bethesda, MD, USA; http://toxnet.nlm.nih.gov) databases to identify studies of drinking-water fluoride and neurodevelopmental outcomes in children. In addition, we searched the China National Knowledge Infrastructure (CNKI; Beijing, China; http://www.cnki.net) database to identify studies published in Chinese journals only. Key words included combinations of “fluoride” or “drinking water fluoride,” “children,” “neurodevelopment” or “neurologic” or “intelligence” or “IQ.” We also used references cited in the articles identified. We searched records for 1980–2011. Our literature search identified 39 studies, among which 36 (92.3%) were studies with high and reference exposure groups, and 3 (7.7%) studies were based on individual-level measure of exposures. The latter showed that dose-related deficits were found, but the studies were excluded because our meta-analysis focused on studies with the high- and low-exposure groups only. In addition, two studies were published twice, and the duplicates were excluded.
Inclusion criteria and data extraction. The criteria for inclusion of studies included studies with high and reference fluoride exposures, end points of IQ scores or other related cognitive function measures, presentation of a mean outcome measure, and associated measure of variance [95% confidence intervals (CIs) or SEs and numbers of participants]. Interpretations of statistical significance are based on an alpha level of 0.05. Information included for each study also included the first author, location of the study, year of publication, and numbers of participants in high-fluoride and low-fluoride areas. We noted and recorded the information on age and sex of children, and parental education and income if available.
Statistical analysis. We used STATA (version 11.0; StataCorp, College Station, TX, USA) and available commands (Stern 2009) for the meta-analyses. A standardized weighted mean difference (SMD) was computed using both fixed-effects and random-effects models. The fixed-effects model uses the Mantel–Haenszel method assuming homogeneity among the studies, whereas the random-effects model uses the DerSimonian and Laird method, incorporating both a within-study and an additive between-studies component of variance when there is between-study heterogeneity (Egger et al. 2001). The estimate of the between-study variation is incorporated into both the SE of the estimate of the common effect and the weight of individual studies, which was calculated as the inverse sum of the within and between study variance. We evaluated heterogeneity among studies using the I2 statistic, which represents the percentage of total variation across all studies due to between-study heterogeneity (Higgins and Thompson 2002). We evaluated the potential for publication bias using Begg and Egger tests and visual inspection of a Begg funnel plot (Begg and Mazumdar 1994; Egger et al. 1997). We also conducted independent meta-regressions to estimate the contribution of study characteristics (mean age in years from the age range and year of publication in each study) to heterogeneity among the studies. The scoring standard for the Combined Raven’s Test–The Rural edition in China (CRT-RC) test classifies scores of ≤ 69 and 70–79 as low and marginal intelligence, respectively (Wang D et al. 1989). We also used the random-effects models to estimate risk ratios for the association between fluoride exposure and a low/marginal versus normal Raven’s test score among children in studies that used the CRT-RC test (Wang D et al. 1989). Scores indicating low and marginal intelligence (≤ 69 and 70–79, respectively) were combined as a single outcome due to small numbers of children in each outcome subgroup.
Results
Six of the 34 studies identified were excluded because of missing information on the number of subjects or the mean and variance of the outcome [see Figure 1 for a study selection flow chart and Supplemental Material, Table S1 (http://dx.doi.org/10.1289/ehp.1104912) for additional information on studies that were excluded from the analysis]. Another study (Trivedi et al. 2007) was excluded because SDs reported for the outcome parameter were questionably small (1.13 for the high-fluoride group, and 1.23 for the low-fluoride group) and the SMD (–10.8; 95% CI: –11.9, –9.6) was > 10 times lower than the second smallest SMD (–0.95; 95% CI: –1.16, –0.75) and 150 times lower than the largest SMD (0.07; 95% CI: –0.083, 0.22) reported for the other studies, which had relatively consistent SMD estimates. Inclusion of this study in the meta-analysis resulted with a much smaller pooled random-effects SMD estimate and a much larger I2 (–0.63; 95% CI: –0.83, –0.44, I2 94.1%) compared with the estimates that excluded this study (–0.45; 95% CI: –0.56, –0.34, I2 80%) (see Supplemental Material, Figure S1). Characteristics of the 27 studies included are shown in Table 1 (An et al. 1992; Chen et al. 1991; Fan et al. 2007; Guo et al. 1991; Hong et al. 2001; Li FH et al. 2009; Li XH et al. 2010; Li XS 1995; Li Y et al. 1994; Li Y et al. 2003; Lin et al. 1991; Lu et al. 2000; Poureslami et al. 2011; Ren et al. 1989; Seraj et al. 2006; Sun et al. 1991; Wang G et al. 1996; Wang SH et al. 2001; Wang SX et al. 2007; Wang ZH et al. 2006; Xiang et al. 2003; Xu et al. 1994; Yang et al. 1994; Yao et al. 1996, 1997; Zhang JW et al. 1998; Zhao et al. 1996). Two of the studies included in the analysis were conducted in Iran (Poureslami et al. 2011; Seraj et al. 2006); the other study cohorts were populations from China. Two cohorts were exposed to fluoride from coal burning (Guo et al. 1991; Li XH et al. 2010); otherwise populations were exposed to fluoride through drinking water. The CRT-RC was used to measure the children’s intelligence in 16 studies. Other intelligence measures included the Wechsler Intelligence tests (3 studies; An et al. 1992; Ren et al. 1989; Wang ZH et al. 1996), Binet IQ test (2 studies; Guo et al. 1991; Xu et al. 1994), Raven’s test (2 studies; Poureslami et al. 2011; Seraj et al. 2006), Japan IQ test (2 studies; Sun et al. 1991; Zhang JW et al. 1998), Chinese comparative intelligence test (1 study; Yang et al. 1994), and the mental work capacity index (1 study; Li Y et al. 1994). Because each of the intelligence tests used is designed to measure general intelligence, we used data from all eligible studies to estimate the possible effects of fluoride exposure on general intelligence.
Figure 1.
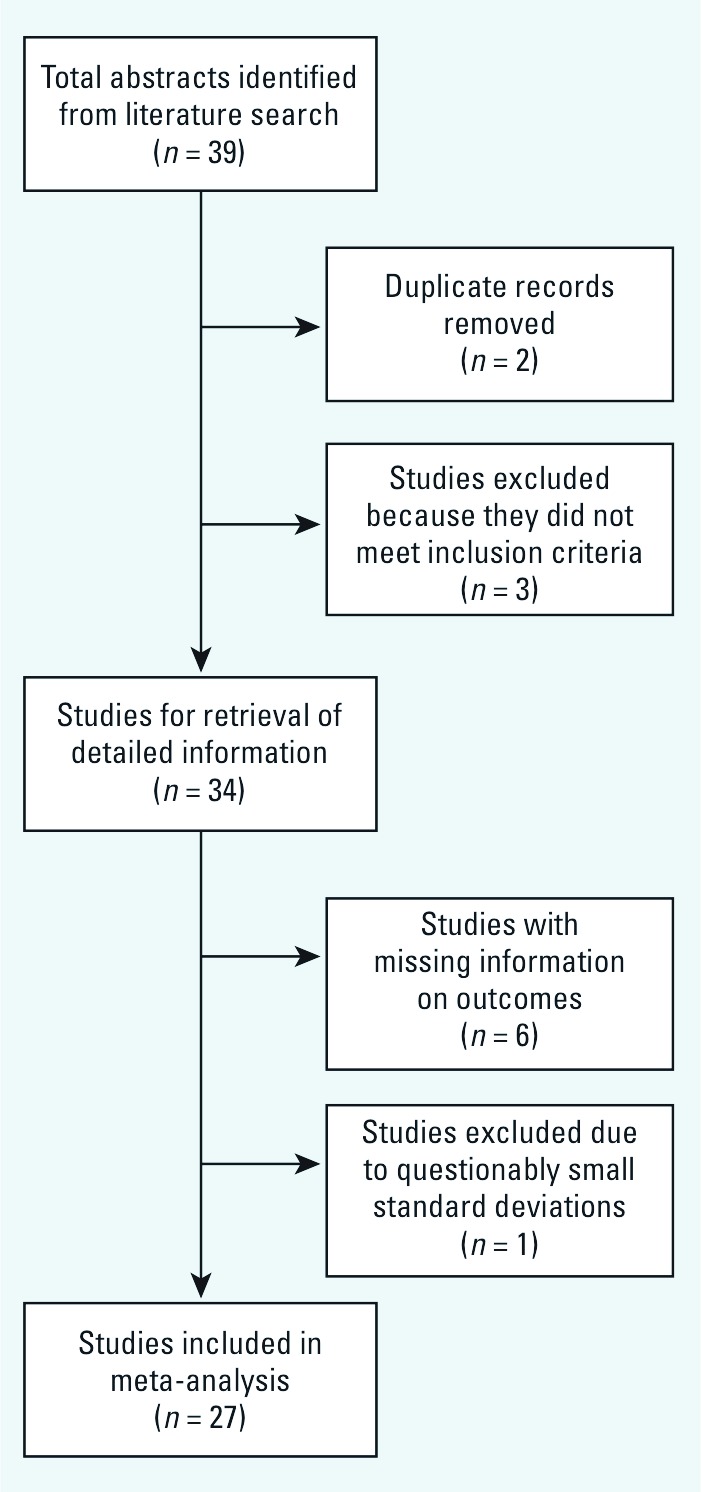
Flow diagram of the meta-analysis.
Table 1.
Characteristics of epidemiological studies of fluoride exposure and children’s cognitive outcomes.
| Reference | Study location | No. in high- exposure group | No. in reference group | Age range (years) | Fluoride exposure | Outcome measure | Results | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Assessment | Range | |||||||||||||
| Ren et al. 1989 | Shandong, China | 160 | 169 | 8–14 | High-/low-fluoride villages | Not specified | Wechsler Intelligence testa | Children in high-fluoride region had lower IQ scores | ||||||
| Chen et al. 1991 | Shanxi, China | 320 | 320 | 7–14 | Drinking water | 4.55 mg/L (high); 0.89 mg/L (reference) | CRT-RCb | The average IQ of children from high-fluoride area were lower than that of the reference area | ||||||
| Guo et al. 1991 | Hunan, China | 60 | 61 | 7–13 | Fluoride in coal burning | 118.1–1361.7 mg/kg (coal burning area); Control area used wood | Chinese Binetc | Average IQ in fluoride coal-burning area was lower than that in the reference area | ||||||
| Lin et al. 1991 | Xinjiang, China | 33 | 86 | 7–14 | Drinking water | 0.88 mg/L (high); 0.34 mg/L (reference) | CRT-RCb | Children in the high-fluoride (low-iodine) area had lower IQ scores compared with the children from the reference fluoride (low-iodine) areas | ||||||
| Sun et al. 1991 | Guiyang, China | 196 | 224 | 6.5–12 | Rate of fluorosis | Fluorosis: 98.36% (high); not specified (reference) | Japan IQ testd | Mean IQ was lower in all age groups except ≤ 7 years in the area with high fluoride and aluminum (limited to high-fluoride population only) | ||||||
| An et al. 1992 | Inner Mongolia, China | 121 | 121 | 7–16 | Drinking water | 2.1–7.6 mg/L (high); 0.6–1.0 mg/L (reference) | Wechsler Intelligence testa | IQ scores of children in high-fluoride areas were significantly lower than those of children living in reference fluoride area | ||||||
| Li Y et al. 1994 | Sichuan, China | 106 | 49 | 12–13 | Burning of high-fluoride coal to cook grain in high-fluoride area | 4.7–31.6 mg/kg (high); 0.5 mg/kg (reference) | Child mental work capacity | Early, prolonged high fluoride intake causes a decrease in the child’s mental work capacity | ||||||
| Xu et al. 1994 | Shandong, China | 97 | 32 | 8–14 | Drinking water | 1.8 mg/L (high); 0.8 mg/L (reference) | Binet-Simone | Children had lower IQ scores in high-fluoride area than those who lived in the reference area. | ||||||
| Yang et al. 1994 | Shandong, China | 30 | 30 | 8–14 | Well water | 2.97 mg/L (high); 0.5 mg/L (reference) | Chinese comparative intelligence testf | The average IQ scores was lower in children from high-fluoride and -iodine area than those from the reference area, but the results were not significant | ||||||
| Li XS et al. 1995 | Guizhou, China | 681 | 226 | 8–13 | Urine, Dental Fluorosis Index | 1.81–2.69 mg/L (high); 1.02 mg/L (reference); DFI 0.8–3.2 (high); DFI < 0.4 (reference) | CRT-RCb | Children living in fluorosis areas had lower IQ scores than children living in nonfluorosis areas | ||||||
| Wang G et al. 1996 | Xinjiang, China | 147 | 83 | 4–7 | Drinking water | > 1.0–8.6 mg/L (high); 0.58–1.0 mg/L (reference) | Wechsler Intelligence testa | Average IQ score was lower in children in the high-fluoride group than those in the reference group | ||||||
| Yao et al. 1996 | Liaoning, China | 266 | 270 | 8–12 | Drinking water | 2–11mg/L (high); 1 mg/L (reference) | CRT-RCb | Average IQ scores of children residing in exposed fluoride areas were lower than those in the reference area | ||||||
| Zhao et al. 1996 | Shanxi, China | 160 | 160 | 7–14 | Drinking water | 4.12 mg/L (high); 0.91 mg/L (reference) | CRT-RCb | Children living in high-fluoride and -arsenic area had significantly lower IQ scores than those living in the reference fluoride (and no arsenic) area | ||||||
| Yao et al. 1997 | Liaoning, China | 188 | 314 | 7–14 | Drinking water | 2 mg/L (exposed); 0.4 mg/L (reference) | CRT-RCb | IQ scores of children in the high-fluoride area were lower than those of children in the reference area | ||||||
| Assessment | Range | |||||||||||||
| Zhang JW et al. 1998 | Xinjiang, China | 51 | 52 | 4–10 | Drinking water | Not specified | Japan IQ Testd | Average IQ scores of children residing in high-fluoride and -arsenic area were lower than those who resided in the reference area | ||||||
| Lu et al. 2000 | Tianjin, China | 60 | 58 | 10–12 | Drinking water | 3.15 mg/L (high); 0.37 mg/L (reference) | CRT-RCb | Children in the high-fluoride area scored significantly lower IQ scores than those in the reference area | ||||||
| Hong et al. 2001 | Shandong, China | 85 | 32 | 8–14 | Drinking water | 2.90 mg/L (high); 0.75 mg/L (reference) | CRT-RCb | Average IQ scores were significantly lower in high-fluoride group (and -iodine) than the reference group | ||||||
| Wang SH et al. 2001 | Shandong, China | 30 | 30 | 8–12 | Drinking water | 2.97 mg/L (high); 0.5 mg/L (reference) | CRT-RCb | No significant difference in IQ scores of children in the high-fluoride/high-iodine and reference fluoride/low-iodine areas | ||||||
| Li Y et al. 2003 | Inner Mongolia, China | 720 | 236 | 6–13 | Fluorosis | Endemic vs. control regions defined by the Chinese Geological Office | CRT-RCb | Average IQ of children in high-fluorosis area was lower than that in the reference area | ||||||
| Xiang et al. 2003 | Jiangsu, China | 222 | 290 | 8–13 | Drinking water | 0.57–4.5 mg/L (high); 0.18–0.76 mg/L (reference) | CRT-RCb | Mean IQ score was significantly lower in children who lived in the high-fluoride area than that of children in the reference exposure area (both areas also had arsenic exposure) | ||||||
| Seraj et al. 2006 | Tehran, Iran | 41 | 85 | Not specified | Drinking water | 2.5 mg/L (high); 0.4 mg/L (reference) | Raveng | The mean IQ of children in the high-fluoride area was significantly lower than that from the reference fluoride area | ||||||
| Wang ZH et al. 2006 | Shanxi, China | 202 | 166 | 8–12 | Drinking water | 5.54 ± 3.88 mg/L (high); 0.73 ± 0.28 mg/L (reference) | CRT-RCb | The IQ scores of children in the high-fluoride group were significantly lower than those in the reference group | ||||||
| Fan et al 2007 | Shaanxi, China | 42 | 37 | 7–14 | Drinking water | 1.14–6.09 mg/L (high); 1.33–2.35 mg/L (reference) | CRT-RCb | The average IQ scores of children residing in the high-fluoride area were lower than those of children residing in the reference area | ||||||
| Wang SX et al. 2007 | Shanxi, China | 253 | 196 | 8–12 | Drinking water and urine | 3.8–11.5 mg/L (water, high); 1.6–11 mg/L (urine, high); 0.2–1.1 mg/L (water, reference); 0.4–3.9 mg/L (urine, reference) | CRT-RCb | Mean IQ scores were significantly lower in the high-fluoride group than from the reference group in the fluoride/arsenic areas | ||||||
| Li et al. 2009 | Hunan, China | 60 | 20 | 8–12 | Coal burning | 1.24–2.34 mg/L (high); 0.962 mg/L (reference) | CRT-RCb | Mean IQ was lower in children in coal-burning areas compared to those in the reference group | ||||||
| Li FH et al. 2010 | Henan, China | 347 | 329 | 7–10 | Drinking water | 2.47 ± 0.75 mg/L (high) | CRT-RCb | No significant difference in IQ scores between children in the exposed and reference groups | ||||||
| Poureslami et al. 2011 | Iran | 59 | 60 | 6–9 | Drinking Water | 2.38 mg/L (high); 0.41 mg/L (reference) | Raveng | Children in the high-fluoride group scored significantly lower than those in reference group | ||||||
| aWechsler Intelligence Scale (Lin and Zhang 1986). bCRT-RC, Chinese Standardized Raven Test, rural version (Wang G et al. 1989). cChinese Binet Test (Wu 1936). dJapan test (Zhang J et al. 1985). eBinet-Simon Test (Binet and Simon 1922). fChinese comparative intelligence test (Wu 1983). gRaven test (Raven et al. 2003). | ||||||||||||||
In addition, we conducted a sensitivity analysis restricted to studies that used similar tests to measure the outcome (specifically, the CRT-RC, Wechsler Intelligence test, Binet IQ test, or Raven’s test), and an analysis restricted to studies that used the CRT-RC. We also performed an analysis that excluded studies with co-exposures including iodine and arsenic, or with non-drinking-water fluoride exposure from coal burning.
Pooled SMD estimates. Among the 27 studies, all but one study showed random-effect SMD estimates that indicated an inverse association, ranging from –0.95 (95% CI: –1.16, –0.75) to –0.10 (95% CI: –0.25, 0.04) (Figure 2). The study with a positive association reported an SMD estimate of 0.07 (95% CI: –0.8, 0.22). Similar results were found with the fixed-effects SMD estimates. The fixed-effects pooled SMD estimate was –0.40 (95% CI: –0.44, –0.35), with a p-value < 0.001 for the test for homogeneity. The random-effects SMD estimate was –0.45 (95% CI: –0.56, –0.34) with an I2 of 80% and homogeneity test p-value < 0.001 (Figure 2). Because of heterogeneity (excess variability) between study results, we used primarily the random-effects model for subsequent sensitivity analyses, which is generally considered to be the more conservative method (Egger et al. 2001). Among the restricted sets of intelligence tests, the SMD for the model with only CRT-RC tests and drinking-water exposure (and to a lesser extent the model with only CRT-RC tests) was lower than that for all studies combined, although the difference did not appear to be significant. Heterogeneity, however, remained at a similar magnitude when the analyses were restricted (Table 2).
Figure 2.

Random-effect standardized weighted mean difference (SMD) estimates and 95% CIs of child’s intelligence score associated with high exposure to fluoride. SMs for individual studies are shown as solid diamonds (♦), and the pooled SMD is shown as an open diamond (◊). Horizontal lines represent 95% CIs for the study-specific SMDs.
Table 2.
Sensitivity analyses of pooled random-effects standardized weighted mean difference (SMD) estimates of child’s intelligence score with high exposure of fluoride.
| Model | Available studies for analysis | SMD (95% CI) | I2 | p-Value test of heterogeneity | ||
|---|---|---|---|---|---|---|
| 1. Exclude nonstandardized testsa | 23 | –0.44 (–0.54, –0.33) | 77.6% | < 0.001 | ||
| 2. Exclude non–CRT-RC Testsb | 16 | –0.36 (–0.48, –0.25) | 77.8% | < 0.001 | ||
| 3. Exclude studies with other exposures (iodine, arsenic)c or non-drinking-water fluoride exposured | 9 | –0.29 (–0.44, –0.14) | 81.8% | < 0.001 | ||
| aMental work capacity (Li Y et al. 1994); Japan IQ (Sun et al. 1991; Zhang JW et al. 1998); Chinese comparative scale of intelligence test (Yang et al. 1994). bWechsler intelligence test (An et al. 1992; Ren et al. 1989; Wang G et al. 1996); Chinese Binet IQ (Guo et al. 1991); Raven (Poureslami et al. 2011; Seraj et al. 2006); Binet-Simon (Xu et al. 1994). cIodine (Hong et al. 2001; Lin et al. 1991; Wang SH et al. 2001); arsenic [Wang SX et al. 2007; Xiang et al. 2003; Zhao et al. 1996; (Zhang JW et al. 1998 was already excluded, see note a)]. dFluoride from coal burning [Li FH et al. 2009 (Guo et al. 1991 and Li Y et al. 1994 were already excluded; see notes a and b)]. | ||||||
Sources of heterogeneity. We performed meta-regression models to assess study characteristics as potential predictors of effect. Information on the child’s sex and parental education were not reported in > 80% of the studies, and only 7% of the studies reported household income. These variables were therefore not included in the models. Among the two covariates, year of publication (0.02; 95% CI: 0.006, 0.03), but not mean age of the study children (–0.02; 95% CI: –0.094, 0.04), was a significant predictor in the model with all 27 studies included. I2 residual 68.7% represented the proportion of residual between-study variation due to heterogeneity. From the adjusted R2, 39.8% of between-study variance was explained by the two covariates. The overall test of the covariates was significant (p = 0.004).
When the model was restricted to the 16 studies that used the CRT-RC, the child’s age (but not year of publication) was a significant predictor of the SMD. The R2 of 65.6% of between-study variance was explained by the two covariates, and only 47.3% of the residual variation was attributable to heterogeneity. The overall test of both covariates in the model remained significant (p = 0.0053). On further restriction of the model to exclude the 7 studies with arsenic and iodine as co-exposures and fluoride originating from coal burning (thus including only the 9 with fluoride exposure from drinking water), neither age nor year of publication was a significant predictor, and the overall test of covariates was less important (p = 0.062), in accordance with the similarity of intelligence test outcomes and the source of exposure in the studies included. Although official reports of lead concentrations in the study villages in China were not available, some studies reported high percentage (95–100%) of low lead exposure (less than the standard of 0.01 mg/L) in drinking-water samples in villages from several study provinces (Bi et al. 2010; Peng et al. 2008; Sun 2010).
Publication bias. A Begg’s funnel plot with the SE of SMD from each study plotted against its corresponding SMD did not show clear evidence of asymmetry, although two studies with a large SE also reported relatively large effect estimates, which may be consistent with publication bias or heterogeneity (Figure 3). The plot appears symmetrical for studies with larger SE, but with substantial variation in SMD among the more precise studies, consistent with the heterogeneity observed among the studies included in the analysis. Begg (p = 0.22) and Egger (p = 0.11) tests did not indicate significant (p < 0.05) departures from symmetry.
Figure 3.
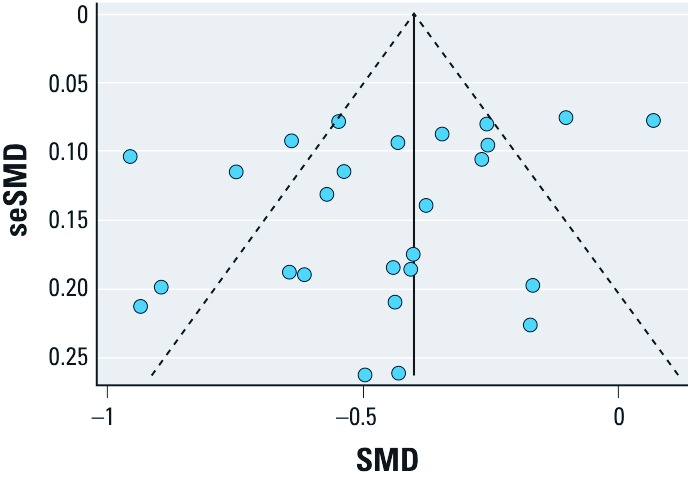
Begg’s funnel plot showing individual studies included in the analysis according to random-effect standardized weighted mean difference (SMD) estimates (x-axis) and the SE (se) of each study-specific SMD (y-axis). The solid vertical line indicates the pooled SMD estimate for all studies combined and the dashed lines indicated pseudo 95% confidence limits around the pooled SMD estimate.
Pooled risk ratios. The relative risk (RR) of a low/marginal score on the CRT-RC test (< 80) among children with high fluoride exposure compared with those with low exposure (16 studies total) was 1.93 (95% CI: 1.46, 2.55; I2 58.5%). When the model was restricted to 9 studies that used the CRT-RC and included only drinking-water fluoride exposure (Chen et al. 1991; Fan et al. 2007; Li XH et al. 2010; Li XS et al. 1995; Li Y et al. 2003; Lu et al. 2000; Wang ZH et al. 2006; Yao et al. 1996, 1997), the estimate was similar (RR = 1.75; 95% CI: 1.16, 2.65; I2 70.6%). Although fluoride exposure showed inverse associations with test scores, the available exposure information did not allow a formal dose–response analysis. However, dose-related differences in test scores occurred at a wide range of water-fluoride concentrations.
Discussion
Findings from our meta-analyses of 27 studies published over 22 years suggest an inverse association between high fluoride exposure and children’s intelligence. Children who lived in areas with high fluoride exposure had lower IQ scores than those who lived in low-exposure or control areas. Our findings are consistent with an earlier review (Tang et al. 2008), although ours more systematically addressed study selection and exclusion information, and was more comprehensive in a) including 9 additional studies, b) performing meta-regression to estimate the contribution of study characteristics as sources of heterogeneity, and c) estimating pooled risk ratios for the association between fluoride exposure and a low/marginal Raven’s test score.
As noted by the NRC committee (NRC 2006), assessments of fluoride safety have relied on incomplete information on potential risks. In regard to developmental neurotoxicity, much information has in fact been published, although mainly as short reports in Chinese that have not been available to most expert committees. We carried out an extensive review that includes epidemiological studies carried out in China. Although most reports were fairly brief and complete information on covariates was not available, the results tended to support the potential for fluoride-mediated developmental neurotoxicity at relatively high levels of exposure in some studies. We did not find conclusive evidence of publication bias, although there was substantial heterogeneity among studies. Drinking water may contain other neurotoxicants, such as arsenic, but exclusion of studies including arsenic and iodine as co-exposures in a sensitivity analysis resulted in a lower estimate, although the difference was not significant. The exposed groups had access to drinking water with fluoride concentrations up to 11.5 mg/L (Wang SX et al. 2007); thus, in many cases concentrations were above the levels recommended (0.7–1.2 mg/L; DHHS) or allowed in public drinking water (4.0 mg/L; U.S. EPA) in the United States (U.S. EPA 2011). A recent cross-sectional study based on individual-level measure of exposures suggested that low levels of water fluoride (range, 0.24–2.84 mg/L) had significant negative associations with children’s intelligence (Ding et al. 2011). This study was not included in our meta-analysis, which focused only on studies with exposed and reference groups, thereby precluding estimation of dose-related effects.
The results suggest that fluoride may be a developmental neurotoxicant that affects brain development at exposures much below those that can cause toxicity in adults (Grandjean 1982). For neurotoxicants such as lead and methylmercury, adverse effects are associated with blood concentrations as low as 10 nmol/L. Serum fluoride concentrations associated with high intakes from drinking water may exceed 1 mg/L, or 50 µmol/L—more than 1,000 times the levels of some other neurotoxicants that cause neurodevelopmental damage. Supporting the plausibility of our findings, rats exposed to 1 ppm (50 µmol/L) of water fluoride for 1 year showed morphological alterations in the brain and increased levels of aluminum in brain tissue compared with controls (Varner et al. 1998).
The estimated decrease in average IQ associated with fluoride exposure based on our analysis may seem small and may be within the measurement error of IQ testing. However, as research on other neurotoxicants has shown, a shift to the left of IQ distributions in a population will have substantial impacts, especially among those in the high and low ranges of the IQ distribution (Bellinger 2007).
Our review cannot be used to derive an exposure limit, because the actual exposures of the individual children are not known. Misclassification of children in both high- and low-exposure groups may have occurred if the children were drinking water from other sources (e.g., at school or in the field).
The published reports clearly represent independent studies and are not the result of duplicate publication of the same studies (we removed two duplicates). Several studies (Hong et al. 2001; Lin et al. 1991; Wang SH et al. 2001; Wang SX et al. 2007; Xiang et al. 2003; Zhao et al. 1996) report other exposures, such as iodine and arsenic, a neurotoxicant, but our sensitivity analyses showed similar associations between high fluoride exposure and the outcomes even after these studies were excluded. Large tracts of China have superficial fluoride-rich minerals with little, if any, likelihood of contamination by other neurotoxicants that would be associated with fluoride concentrations in drinking water. From the geographic distribution of the studies, it seems unlikely that fluoride-attributed neurotoxicity could be attributable to other water contaminants.
Still, each of the articles reviewed had deficiencies, in some cases rather serious ones, that limit the conclusions that can be drawn. However, most deficiencies relate to the reporting of where key information was missing. The fact that some aspects of the study were not reported limits the extent to which the available reports allow a firm conclusion. Some methodological limitations were also noted. Most studies were cross-sectional, but this study design would seem appropriate in a stable population where water supplies and fluoride concentrations have remained unchanged for many years. The current water fluoride level likely also reflects past developmental exposures. In regard to the outcomes, the inverse association persisted between studies using different intelligence tests, although most studies did not report age adjustment of the cognitive test scores.
Fluoride has received much attention in China, where widespread dental fluorosis indicates the prevalence of high exposures. In 2008, the Ministry of Health reported that fluorosis was found in 28 provinces with 92 million residents (China News 2008). Although microbiologically safe, water supplies from small springs or mountain sources created pockets of increased exposures near or within areas of low exposures, thus representing exposure settings close to the ideal, because only the fluoride exposure would differ between nearby neighborhoods. Chinese researchers took advantage of this fact and published their findings, though mainly in Chinese journals and according to the standards of science at the time. This research dates back to the 1980s, but has not been widely cited at least in part because of limited access to Chinese journals.
In its review of fluoride, the NRC (2006) noted that the safety and the risks of fluoride at concentrations of 2–4 mg/L were incompletely documented. Our comprehensive review substantially extends the scope of research available for evaluation and analysis. Although the studies were generally of insufficient quality, the consistency of their findings adds support to existing evidence of fluoride-associated cognitive deficits, and suggests that potential developmental neurotoxicity of fluoride should be a high research priority. Although reports from the World Health Organization and national agencies have generally focused on beneficial effects of fluoride (Centers for Disease Control and Prevention 1999; Petersen and Lennon 2004), the NRC report examined the potential adverse effects of fluoride at 2–4 mg/L in drinking water and not the benefits or potential risks that may occur when fluoride is added to public water supplies at lower concentrations (0.7–1.2 mg/L) (NRC 2006).
In conclusion, our results support the possibility of adverse effects of fluoride exposures on children’s neurodevelopment. Future research should formally evaluate dose–response relations based on individual-level measures of exposure over time, including more precise prenatal exposure assessment and more extensive standardized measures of neurobehavioral performance, in addition to improving assessment and control of potential confounders.
Supplemental Material
Acknowledgments
We thank V. Malik, Harvard School of Public Health, for the helpful advice on the meta-analysis methods.
Footnotes
This study was supported by internal institutional funds.
The authors declare they have no actual or potential competing financial interests.
References
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Fluorides, Hydrogen Fluoride, and Fluorine (Update). 2003 Available: http://www.atsdr.cdc.gov/toxprofiles/tp11.pdf [accessed 5 April 2010] [PubMed] [Google Scholar]
- An JA, Mei SZ, Liu AP, Fu Y, Wang CF. Effect of high level of fluoride on children’s intelligence. Chin J Control Endem Dis. 1992;7(2):93–94. [in Chinese] [Google Scholar]
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. [PubMed] [Google Scholar]
- Bellinger DC. Interpretation of small effect sizes in occupational and environmental neurotoxicity: individual versus population risk. Neurotoxicology. 2007;28:245–251. doi: 10.1016/j.neuro.2006.05.009. [DOI] [PubMed] [Google Scholar]
- Bi WJ, Zheng X, Lan TX. Analysis on test results of drinking water’s quality in Janan Railway Bureau from 2005–2009. Prev Med Trib. 2010;16(6):483–485. [in Chinese] [Google Scholar]
- Binet A, Simon T. Shanghai: Commercial Press; 1922. The Measurement of the Mental Development of the Child (translated into Chinese by Jie FP) [Google Scholar]
- Centers for Disease Control and Prevention Achievements in public health, 1990–1999: fluoridation of drinking water to prevent dental caries. MMWR. 1999;48(41):933–940. [Google Scholar]
- Chen YX, Han F, Zhou Z, Zhang H, Jiao X, Zhang S, et al. Research on the intellectual development of children in high fluoride areas. Chin J Control Endem Dis. 1991;6(suppl):99–100. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- China News. Twenty-eight provinces were affected by fluorosis in China [in Chinese]. 2008 Available: http://news.qq.com/a/20081216/001707.htm [accessed 3 July 2012] [Google Scholar]
- Chioca LR, Raupp IM, Da Cunha C, Losso EM, Andreatini R. Subchronic fluoride intake induces impairment in habituation and active avoidance tasks in rats. Eur J Pharmacol. 2008;579:196–201. doi: 10.1016/j.ejphar.2007.10.019. [DOI] [PubMed] [Google Scholar]
- Ding Y, Gao Y, Sun H, Han H, Wang W, Ji X, et al. The relationships between low levels of urine fluoride on children’s intelligence, dental fluorosis in endemic fluorosis area in Hulunbuir, Inner Mongolia, China. J Hazard Mater. 2011;186:1942–1946. doi: 10.1016/j.jhazmat.2010.12.097. [DOI] [PubMed] [Google Scholar]
- Egger M, Davey Smith G, Altman DG. London: BMJ Publishing; 2001. Systematic Reviews in Health Care: Meta-Analysis in Context. [Google Scholar]
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan ZX, Dai HY, Bai AM, Li PO, Li T, LI GD, et al. Effect of high fluoride exposure in children’s intelligence. J Environ Health. 2007;24(10):802–803. [in Chinese] [Google Scholar]
- Grandjean P. Occupational fluorosis through 50 years: clinical and epidemiological experiences. Am J Ind Med. 1982;3(2):227–336. doi: 10.1002/ajim.4700030215. [DOI] [PubMed] [Google Scholar]
- Grandjean P, Landrigan P. Developmental neurotoxicity of industrial chemicals. Lancet. 2006;368(9553):2167–2178. doi: 10.1016/S0140-6736(06)69665-7. [DOI] [PubMed] [Google Scholar]
- Guo XC, Wang R, Cheng C, Wei W, Tang L, Wang Q, et al. A preliminary exploration of IQ of 7–13 year old pupils in a fluorosis area with contamination from burning coal. Chin J Endemiol. 1991;10:98–100. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- Hong F, Cao Y, Yang D, Wang H. A study of fluorine effects on children’s intelligence development under different environments. Chin Prim Health Care. 2001;15:56–57. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- Li FH, Chen X, Huang RJ, Xie YP. Intelligence impact of children with endemic fluorosis caused by fluoride from coal burning. J Environ Health. 2009;26(4):338–340. [in Chinese] [Google Scholar]
- Li XH, Hou GQ, Yu B, Yuan CS, Liu Y, Zhang L, et al. Investigation and analysis of children’s intelligence and dental fluorosis in high fluoride area. J Med Pest Control. 2010;26(3):230–231. [in Chinese] [Google Scholar]
- Li XS, Zhi JL, Gao RO. Effect of fluoride exposure on intelligence in children. Fluoride. 1995;28(4):189–192. [Google Scholar]
- Li Y, Jing X, Chen D, Lin L, Wang Z. The effects of endemic fluoride poisoning on the intellectual development of children in Baotou. Chin J Public Health Manag. 2003;19(4):337–338. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- Li Y, Li X, Wei S. Effect of excessive fluoride intake on mental work capacity of children and a preliminary study of its mechanism. J West China Univ Med Sci. 1994;25(2):188–191. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [PubMed] [Google Scholar]
- Lin C, Zhang H. Beijing: Beijing Normal University Press; 1986. Wechsler Children Intelligence Scale. Revised Edition in China. [Google Scholar]
- Lin FF, Ai HT, Zhao HX, Lin J, Jhiang JY, Maimaiti, et al. High fluoride and low iodine environment and subclinical cretinism in Xinjiang. Endem Dis Bull. 1991;6(2):62–67. [in Chinese] [Google Scholar]
- Lu Y, Sun ZR, Wu LN, Wang X, Lu W, Liu SS, et al. Effect of high-fluoride water on intelligence in children. Fluoride. 2000;33(2):74–78. [in Chinese] [Google Scholar]
- Mullenix PJ, Denbesten PK, Schunior A, Kernan WJ. Neurotoxicity of sodium fluoride in rats. Neurotoxicol Teratol. 1995;17:169–177. doi: 10.1016/0892-0362(94)00070-t. [DOI] [PubMed] [Google Scholar]
- NRC (National Research Council) Washington, DC: National Academies Press; 2006. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards. [Google Scholar]
- Peng YP, Zou J, Yang DF, Li XH, Wu K. Analysis of water quality from homemade wells in Leshan downtown during 2004–2006. J Occup Health Damage. 2008;23(4):219–221. [in Chinese] [Google Scholar]
- Petersen PE, Lennon MA. Effective use of fluorides for the prevention of dental caries in the 21st century: the WHO approach. Community Dent Oral Epidem. 2004;32(5):319–321. doi: 10.1111/j.1600-0528.2004.00175.x. [DOI] [PubMed] [Google Scholar]
- Poureslami HR, Horri A, Atash R. High fluoride exposure in drinking water: effect on children’s IQ, one new report. Int J Pediatr Dent. 2011;21(suppl 1):47. [Google Scholar]
- Raven J, Raven JC, Court JH. San Antonio, TX:Harcourt Assessment. 2003. Manual for Raven’s Progressive Matrices and Vocabulary Scales. [Google Scholar]
- Ren DL, Li K, Lin D. An investigation of intelligence development of children aged 8–14 years in high-fluoride and low-iodine areas. Chin J Control Endem Dis. 1989;4:251. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- Seraj B, Shahrabi M, Falahzade M, Falahzade FP, Akhondi N. Effect of high fluoride concentration in drinking water on children’s intelligence. J Dental Med. 2006;19(2):80–86. [abstract in English]. Available: http://journals.tums.ac.ir/upload_files/pdf/_/2530.pdf [accessed 24 August 2012] [Google Scholar]
- Stern JAC. College Station, TX:Stata Press. 2009. Meta-analysis in Stata: An Updated Collection from the Stata Journal. [Google Scholar]
- Sun LY. Survey of drinking water quality in Jintang County. J Occup Health Damage. 2010;25(5):277–280. [in Chinese] [Google Scholar]
- Sun MM, Li SK, Wang YF, Li FS. Measurement of intelligence by drawing test among the children in the endemic area of Al-F combined toxicosis. J Guiyang Med College. 1991;16(3):204–206. [in Chinese] [Google Scholar]
- Tang QQ, Du J, Ma HH, Jiang SJ, Zhou XJ. Fluoride and children’s intelligence: a meta-analysis. Bio Trace Elem Res. 2008;126:115–120. doi: 10.1007/s12011-008-8204-x. [DOI] [PubMed] [Google Scholar]
- Trivedi MH, Verma RJ, Chinoy NJ, Patel RS, Sathawara NG. Effect of high fluoride water on intelligence of school children in India. Fluoride. 2007;40(3):178–183. [Google Scholar]
- U.S. EPA. EPA and HHS Announce New Scientific Assessments and Actions on Fluoride: Agencies Working Together to Maintain Benefits of Preventing Tooth Decay while Preventing Excessive Exposure. 2011 Available: http://yosemite.epa.gov/opa/admpress.nsf/bd4379a92ceceeac8525735900400c27/86964af577c37ab285257811005a8417!OpenDocument [accessed 7 January 2011] [Google Scholar]
- Varner JA, Jensen KF, Horvath W, Isaacson RL. Chronic administration of aluminum-fluoride or sodium-fluoride to rats in drinking water: alterations in neuronal and cerebrovascular integrity. Brain Res. 1998;784:284–298. doi: 10.1016/s0006-8993(97)01336-x. [DOI] [PubMed] [Google Scholar]
- Wang D, Di M, Qian M. Tianjin, China: Tianjin Medical University; 1989. Chinese Standardized Raven Test, Rural Version. [Google Scholar]
- Wang G, Yang D, Jia F, Wang H. Research on intelligence quotient of 4-7 year-old children in a district with a high level of fluoride. Endem Dis Bull. 1996;11:60–62. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [Google Scholar]
- Wang SH, Wang LF, Hu PY, Guo SW, Law SH. Effects of high iodine and high fluorine on children’s intelligence and thyroid function. Chin J Endemiol. 2001;20(4):288–290. [in Chinese] [Google Scholar]
- Wang SX, Wang ZH, Cheng XT, Li J, Sang ZP, Zhang XD, et al. Arsenic and fluoride exposure in drinking water: children’s IQ and growth in Shanyin County, Shanxi Province, China. Environ Health Perspect. 2007;115:643–647. doi: 10.1289/ehp.9270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang ZH, Wang SX, Zhang XD, Li J, Zheng XT, Hu CM, et al. Investigation of children’s growth and development under long-term fluoride exposure. Chin J Control Endem Dis. 2006;21(4):239–241. [in Chinese; abstract in English] [Google Scholar]
- World Bank. Water Quality Management: Policy and Institutional Considerations. 2006 Available: http://siteresources.worldbank.org/INTEAPREGTOPENVIRONMENT/Resources/China_WPM_final_lo_res.pdf [accessed 13 June 2012] [Google Scholar]
- World Health Organization. Fluorides. Geneva:World Health Organization. 2002 Available: http://whqlibdoc.who.int/ehc/WHO_EHC_227.pdf [accessed 5 September 2012] [Google Scholar]
- Wu TM. Shanghai: Commercial Press (in Chinese); 1936. Second revision of Chinese-Binet Intelligence Test. [Google Scholar]
- Wu T. Beijing: Beijing University Press; 1983. The Chinese Comparative Intelligence Test Guidebook. 3rd ed. [Google Scholar]
- Xiang Q, Liang Y, Chen L, Wang C, Chen B, Chen X, et al. Effect of fluoride in drinking water on children’s intelligence. Fluoride. 2003;36(2):84–94. [Google Scholar]
- Xu YL, Lu CS, Zhang XN. Effect of fluoride on children’s intelligence. Endem Dis Bull. 1994;2:83–84. [in Chinese] [Google Scholar]
- Yang Y, Wang X, Guo X, Hu P. Effects of high iodine and high fluorine on children’s intelligence and the metabolism of iodine and fluorine. Chin J Pathol. 1994;15(5):296–298. Available: http://www.fluoridealert.org/chinese/ [accessed 20 August 2012] [PubMed] [Google Scholar]
- Yao LM, Deng Y, Yang SY, Zhou JL, Wang SL, Cui JW. Comparison of children’s health and intelligence between the fluorosis areas with and without altering water sources. Lit Inf Prev Med. 1997;3(1):42–43. [in Chinese] [Google Scholar]
- Yao LM, Zhou JL, Wang SL, Cui KS, Lin FY. Analysis of TSH levels and intelligence of children residing in high fluorosis areas. Lit Inf Prev Med. 1996;2(1):26–27. [in Chinese] [Google Scholar]
- Zhang J, Gung Y, Guo J. Beijing: Captial Institute of Pediatrics Heatlh Research Office; 1985. Children Intelligence Scale Handbook. [Google Scholar]
- Zhang JW, Yao H, Chen Y. Effect of high level of fluoride and arsenic on children’s intelligence. Chin J Public Health. 1998;17(2):57. [in Chinese] [Google Scholar]
- Zhang M, Wang A, Xia T, He P. Effects of fluoride on DNA damage, S-phase cell-cycle arrest and the expression of NF-κB in primary cultured rat hippocampal neurons. Toxicol Lett. 2008;179:1–5. doi: 10.1016/j.toxlet.2008.03.002. [DOI] [PubMed] [Google Scholar]
- Zhao LB, Liang GH, Zhang DN, Wu XR. Effect of a high fluoride water supply on children’s intelligence. Fluoride. 1996;29(4):190–192. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.