

Abstract
Objective
Dental caries is a significant public health problem especially amongst children from low-income backgrounds. This longitudinal study examined the development of new occlusal caries in 227 Newark, NJ children ages 10–18. The role of previous caries experience and the presence of occlusal white and dark lesions in predicting the development of new lesions were examined.
Design
At each visit, the patient’s teeth were given a visual-tactile examination and the subject’s decayed; missing and filled (DMFS) score was determined. Next, molars lacking probeable caries or restorations were examined using transillumination for occlusal white and dark spots. This examination was repeated periodically. A Cox proportional hazard was used to analyze data concerning the development of new occusal caries in molars.
Results
The longitudinal data indicates that patients who were caries free at visit-1 developed significantly fewer occlusal caries during the longitudinal study. The hazard ratio for subjects who had first-visit caries was 2.27 compared to caries free subjects. Intact molars with occlusal white or dark lesions had caries hazard ratios of 0.78 and 1.49 respectively, compared to molars lacking initial color changes.
Conclusion
Having a prior caries history places the subject at increased risk of developing future caries. Teeth with dark lesions but not white lesions are at significantly increased risk for developing decay. White lesions may represent remineralizing or slowly progressing lesions. The results of this study can help identify patients and tooth surfaces at risk for future occlusal decay.
Keywords: caries, risk, longitudinal study, proportional hazard
1. Introduction
Dental caries remains one of the most common and costly infectious diseases to afflict humanity. Although considerable progress has been made in the prevention and treatment of dental caries, not all segments of the population have benefited equally. A recent US Surgeon’s General Report has delineated the magnitude of childhood caries in the United States. Amongst children age 5–17, 43.6% of poor children were found to need at least one dental restoration.1 In contrast the same study reported that only 23.4% of non-poor children in the same age group required dental restorations. The continued high incidence of caries in segments of the population indicate that better methods need to be developed to identify individuals and tooth sites at risk for caries development.
Recognition of the complex nature of caries causation has lead to the development of methods used to evaluate individual patients risk.2 In many studies, prior caries experience was shown to be a predictor of future caries occurrence.3,4 Adults with retained third molars who had caries on their first or second molars had an increased likelihood of developing caries on the third molars than subjects whose molars were caries free.5,6 Combining the contribution of past caries experience, as evidenced by dental restorations, to present caries improves the accuracy of caries prediction.7 Past caries indicates that the individual must have been infected by caries inducing microorganisms, had tooth surfaces that were exposed to conditions where demineralization exceeded remineralization and where clinically evident caries was diagnosed.8
Early carious lesions are marked by subsurface mineral loss resulting in white spots that are most readily visible on smooth surfaces when the tooth is dried.9 When white lesions are subjected to conditions that favor a cessation of demineralization they can remineralize. When white spots continue to demineralize, loss of surface integrity occurs resulting in a cavitated lesions. Latter in the progression of the lesion, the superficial dentin underlying the enamel lesion develops a dark gray or brown discoloration that is due to the penetration of bacterial pigments into dentin.10 Although areas of demineralization effecting both enamel and dentin can remineralize,11 demineralized dentin retains its dark appearance following remineralization since the pigments are trapped in the dentin structure.12
Few clinical studies have examined the progression of non-cavitated lesions involving the occlusal surface of posterior teeth. Using a visual caries scoring system and a device that analyzes fluorescent changes in tooth structure caused by mineral loss, it was observed that approximately one third of the occlusal lesions visually scored as having enamel demineralization but lacking surface breakdown, progressed to more severe caries scores following 12 months. In contrast, only half as many teeth with occlusal demineralizations showed clinical signs of improvement. In this same study, smooth surface lesions scored as intact demineralizations were observed to be more likely to improve and less likely to progress.13 Although the population of children followed had high caries prevalence and high rates of lesion progression, there was equivocal evidence linking the subject’s over-all caries experience to the tendency for non-cavitated lesions to progress.14 This study also had the limitations of not differentiating between white and dark non-cavitated lesions. This distinction may be helpful in indicating risk since dark lesions represent a later stage in the caries process.
This longitudinal study focused on occlusal caries development in the erupted permanent molars of inner-city children ages 10–18. We examined the relationship between a number of clinical parameters assessed at the subject’s first visit with the development of pit and fissure caries at subsequent visits. Two hypotheses will be examined:
Subjects with higher numbers of decayed missing and filled surfaces at the first visit will develop more occlusal decay during the longitudinal study.
If the presence of white and dark spots on the occlusal surface of permanent molars represent the early precavitated stages of decay, than teeth with these lesions should develop probeable caries more often than teeth that lack these lesions.
In addition, the data will be examined in order to determine if a subject’s past caries experience and the presence of white or dark lesions on individual molars act together to influence the risk of cavitated lesion formation in individual teeth. The results of this study should help identify high-risk occlusal surfaces in at risk individuals.
2. Methods
2.1. Subjects
This study was conducted on subjects participating in a longitudinal study of microbial risk factors for localized periodontal disease15 and clinical risk factors for dental caries. Data was collected from all subjects for use in both studies. The Newark NJ Board of Education, the Archdiocese of Newark NJ and various autonomous charter schools agreed to allow us to visit their school’s in a mobile dental facility (provided by the Colgate Palmolive Company) and conduct the examinations. Thirty-four Individual schools agreed to participate. The goal of the study was to collect longitudinal data from as many children as possible in the Newark, New Jersey area; consequently we visited all schools that allowed us access. Approval of the university’s institutional review board (IRB protocol # 0120020236), permission of the school authorities, parental consent and subject assent was obtained prior to conducting the examinations. Within each school an IRB-approved information package, medical history question sheet, parental consent and subject assent was distributed to families of children within the target age group. Examinations were scheduled for all assenting children for whom we received parental consent and who did not have one of the exclusionary conditions listed below. Other than these criteria there was no selection process used to determine which students participated in the study.
2.2. Examination procedures and caries classification
Parents (or guardians) provided information concerning the subject’s medical history and ethnic self-classification. Exclusion criteria included incomplete medical history information, pregnancy or lactation, diabetes, and tumors of the oral hard or soft tissue. In order to participate subjects must in addition to meeting age and health qualifications, have at least 20 teeth and at least one permanent molar.
Prior to examination, teeth were cleaned with a circular bristle brush held on an electrically driven disposable prophylaxis angle, care being taken to remove plaque from the occlusal fissures. Examination and charting of decayed, missing and filled surfaces (DMFS) was performed on all teeth. Teeth with occlusal pit and fissure sealants were classified as filled. Designating a tooth as missing was restricted to teeth lost to decay. Permanent second molars were examined if the entire occlusal surface was erupted to the extent that it could be examined; otherwise they were classified as unerupted. Visual examination and the dental explorer was used to detect caries. The explorer tip was gently moved over the pits and fissures on the occlusal and buccal surfaces of the posterior teeth. The tip of the explorer was kept at a slight angle to the tooth surface to avoid pressing the explorer tip onto the enamel surface at any time in the examination. The explorer was used to remove plaque that was not removed by the brush and to detect defects on these surfaces as an adjunct to visual inspection. Once detected, the presence of an occlusal lesion was confirmed by immediately repeating the examination (by the same examiner). The object of these examinations was to reproduce the type of clinical examination performed in the dental office using contemporary examination guidelines. Teeth with visibly apparent cavitations or probeable lesions were classified as carious and included as D surfaces on the DMFS count. Since radiographs were not taken during the initial examination the incidence of proximal surface caries are assumed to be under-assessed.
In the next part of the examination, the occlusal surfaces of molars that were observed to lack probeable caries or restorations based on the mirror-explorer examination were examined for subtitle white and dark occlusal lesions. Following DMFS charting, the permanent molar teeth were dried with gauze and an air-stream then examined with a hand-held transilluminator (Microlux® AdDent Inc., Danbury, CT). Occlusal white and dark (gray or brown) discolorations, visible when the tooth was transilluminated from the buccal or lingual surfaces, were recorded. Although caries related changes in tooth tissue color could not always be identified with certainty; faint white patches that were restricted to the pits and fissures, particularly those that were accentuated by drying, were classified as white lesions. Diffuse white patches involving the cusp tips were not classified as white lesions since these enamel changes frequently have developmental origins. By varying the angle of illumination superficial dark staining of the occlusal fissures was differentiated from subsurface pigmentation. Only these deep discolorations were classified as potentially precarious dark lesions. Non-probeable white or dark areas were not included on the DMFS count.
Based on the transilluminator examination, individual permanent molars were scored as follows:
0- No probeable lesion or color change suggestive of a precarious lesion.
1- Subtle white lesion in the occlusal pit and fissure system.
2- Dark gray or brown non-removable discoloration of the occlusal surface.
Recall visits employing the same examination procedures were conducted. Our intention was to examine subjects biannually for as long as they participated. Due to scheduling considerations however, the average inter-visit interval was longer.
Since the goals of this study was to examine the transition of occlusal color changes to probeable caries, the term “carious” or “decayed” will be reserved for probeable lesions only. Based on the results of these examinations, the sequence of which is seen in Fig. 1, the overall caries activity of the subject was classified as to the types of lesions present and the total number of decayed missing and filled surfaces (DMFS). By performing repeated examinations of initially caries free occlusal surfaces we can determine what proportion of these intact teeth develop occlusal caries and determine if teeth with white or dark lesions are more likely to develop probeable lesions than teeth that lack these findings.
Figure 1.
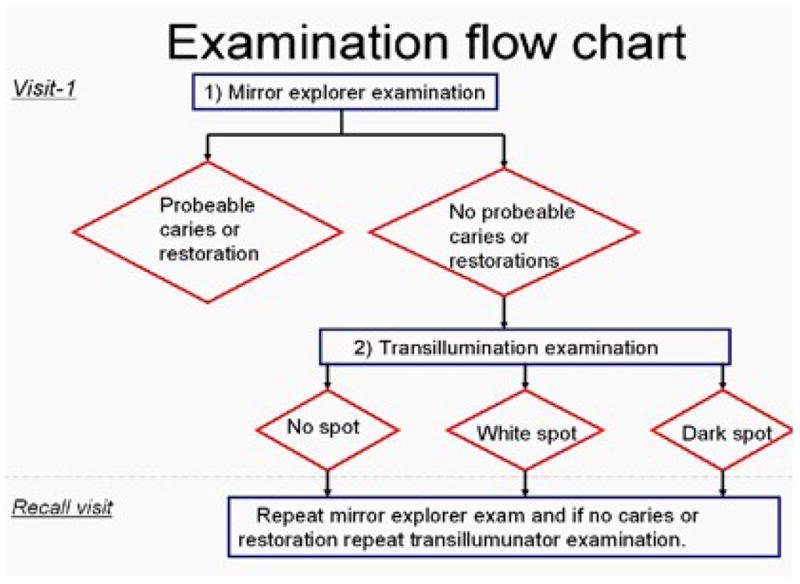
Sequence of visual/tactile and transilluminator examinations used in the longitudinal caries study. A diagnosis of occlusal caries is made when caries is detected by visual tactile examination. At each examination molars that were found to be free of occlusal caries or restorations are examined with a hand-held transilluminator for the presence of non-probeable white or dark lesions. At recall examinations it was determined if initially intact teeth developed occlusal caries and if the presence of white and dark spots at the initial visit increased the risk of occlusal caries development.
Following each examination, all subjects were given a soft toothbrush, oral hygiene instruction and dietary information. Since the dental van was used for examinations only, children found to have evidence of localized aggressive periodontal disease or caries (cavitated lesions) were referred to New Jersey Dental School’s Center for Dental and Oral health for treatment.
2.3. Examiner Calibration
The clinical examiner (KM) was trained to conduct the caries examination by DHF. A training exercise was held where both investigators examined nine subjects scheduled for examination at that time. Following each examination the full mouth DMFS and molar transilluminaton scores obtained by the two examiners were compared. The two examiners agreed on the DMFS charting of the nine subjects. Discrepancies in the white-dark lesion classification of individual occlusal surfaces were resolved by discussion of points of disagreement and then reviewed via joint examination. By the completion of the exercise the two examiners arrived at the same scores. In follow-up examinations, the clinical examiner (KM) was blinded as to the results of the previous examinations.
2.4. Data analysis
Data concerning the subject’s demographics, DMFS and transillumination results were entered into an electronic database (Microsoft Access, Microsoft Corporation, Redmond, WA, USA). An analysis of the longitudinal data was performed in order to determine the relationship between the subject’s first visit dental findings and subsequent molar occlusal caries development. A Cox proportional hazard model was used to analyze the influence of the subject’s visit-I DMFS, the presence of occlusal white and dark lesions on individual teeth and patient demographic variables such as gender or ethnic affiliation on the development of occlusal caries. This was carried out using a SAS (version 9.1) statistical software package (SAS Institute Inc., Cary, NC, USA). Hazard ratios were calculated and displayed with 95% confidence limits. Statistical significance was set at the 0.05 level.
A marginal Cox model for clustered data was used where data from each of the subject’s one-eight erupted and initially intact molars are treated as a data cluster. In this analysis, the hazard ratios associated with the various variables was calculated. The influence of gender and the subject’s ethnic affiliation was done by comparing the proportional survival (hazard rate) of one group with the other. For DMFS the caries hazard rate for DMFS=0 subjects was calculated and used as a reference value to calculate the hazard ratio for incrementally increasing DMFS values. In order to determine the role of white and dark lesions on subsequent caries development, the hazard ratio of each of these conditions was calculated using the hazard rate of teeth with no occlusal discolorations as a reference value. In addition to examining the effect of incremental DMFS increases on caries hazzard, a three-way system was used to classify the subject’s DMFS status for caries hazard ratio calculations. This classification divided the subjects into the following catergories:
Caries free (DMFS=0) subjects had no decayed, missing or filled surfaces.
Caries susceptible (D=0, DMFS>0) subjects had at least one-restored or missing surface but no unrestored caries.
Caries active (DMFS>0, D>0) subjects had at least one-unrestored carious lesion.
This classification differentiates subjects with active disease, past (as evidenced by restored teeth) but not necessarily current disease and no disease. This system has been used in studies correlating Streptococcus. mutans levels at oral sites, with caries development.16,17 The hazard ratio for caries susceptible and caries active subjects was calculated using the hazard rate of caries free subjects as a reference value. The combined effects of occlusal color change and visit-1 DMFS status on caries development was also examined using the Cox proportional hazard approach.
3. Results
3.1 Subject population
1257 patients were examined for caries as described above, of these, 227 (18.1%) were examined at least twice. Of these 227, 98 subjects were examined at least three times. The mean (±SD) inter-visit interval was 277± 113 days and the average length of the subject’s participation was 481± 253 days.
The study population (as recorded at the first visit) was 60.8% female. In terms of ethnic breakdown the subjects were identified as; 50.9% Hispanic, 40.5% African American and 8.6% who were described as Caucasian, Asian or Pacific Islander, American Indian or Alaska native, other or did not have ethnic information reported. The average age of the subjects was 12.2± 1.6 years.
As shown in Fig. 2, cross-sectional caries data collected from subjects at the first visit indicates that 68.7% of the children had at least one probeable caries lesion, 18.5% had more than five lesions, and 4.4% had more than 10 lesions. 4% of subjects were missing one or more permanent molars due to caries related causes. 48.6% of subjects had at least one restoration on a primary or permanent tooth. 76% of the subjects had at least one white or dark lesion reveled by transilluminator examination. Overall only 3% of children were free of caries, restorations, missing teeth or nonprobable white/dark lesions.
Figure 2.
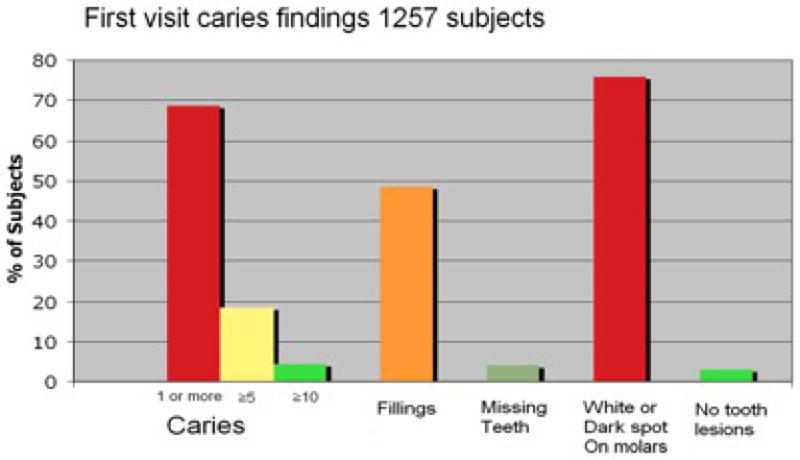
Cross-sectional caries data collected from subjects at the first visit. A majority of subjects had at least one carious lesion and at lest one molar with an occlusal white or dark spot.
3.2. Development of occlusal caries on initially caries free molars
Repeated dental examinations were performed on 227 subjects. 186 of these study participants were found to have at least one erupted, non-decayed and un-restored permanent molar at the first visit. Overall, these 186 subjects had a total of 746 teeth that were free of probeable occlusal lesions at the initial visit; these teeth were monitored for caries development during the longitudinal study. 236 (31.6%) of these teeth developed probeable decay or were given occlusal restorations by the subject’s final visit. The number and percent of teeth presenting as caries free at the beginning of the study in each of the three transillumination categories described above and developing caries by the final visit is shown in Table 1. The percentages of molars developing caries by the final visit was 29.5% for molars that were initially free of either white or dark lesions, 23.9% for molars that initially had occlusal white spots and 43.4% for molars with dark lesions at the initial visit.
Table 1.
Caries development in initially caries free erupted molars. Numbers of molars that were caries free at the initial examination are shown in the second row. Third row shows numbers (%) of molars that developed caries by the last visit.
| Transilluminator classification | ||||
|---|---|---|---|---|
| All initially caries and restoration free molars | 0- No spot (normal color) | 1- White spot | 2- Dark spot | |
| Number of teeth at visit-1. | 746 | 291 | 243 | 212 |
| Number (%) of teeth developing occlusal decay by the end of the study. | 236 (31.6%) | 86 (29.5%) | 58 (23.9%) | 92 (43.4%) |
As shown in Table 2, the Cox proportional hazard model indicated that the patient’s age and gender had no significant effect on the risk of developing molar caries with hazard ratios of 1.0 and 0.85 respectively. By comparing the hazard rates of the various ethnic categories it was determined that ethnic group did not have a significant effect.
Table 2.
Cox proportional hazard model of caries development in initially caries free permanent molars. The presence of dark spots but not white spots was associated with a higher hazard of caries development compared to teeth without dark or white spots. Patients who had carious lesions (caries active subjects) and patients who had restored (or missing) teeth but no active lesions (caries susceptible subjects) were more likely to develop caries in initially caries free molars than patients who were caries free at the first visit. None of the other demographic variables examined (gender, age and ethnic group) had a significant effect on the caries hazard.
| Variable | Hazard ratio | Hazard ratio 95% Confidence limits | ||
|---|---|---|---|---|
| Visit-1 Transilluminator Classification | No Spot | Reference | ||
| White spot | 0.78 | 0.52 | 1.17 | |
| Dark spot | 1.49* | 1.04 | 2.15 | |
| DMFS Category | Caries free | Reference | ||
| Caries active | 2.27* | 1.26 | 4.11 | |
| Caries susceptible | 2.33* | 1.05 | 5.17 | |
| Demographics | Gender | 0.85 | 0.57 | 1.27 |
| Age | 1.00 | 0.93 | 1.09 | |
| Ethnic-Hispanic verse African American | 1.41 | 0.91 | 2.16 | |
| Ethnic-Other verse African American | 1.89 | 0.91 | 3.93 | |
Increased DMFS was associated with a statically significant increase of caries risk although the hazard ratio associated with increases in DMFS score was low, for each one-unit increase in DMFS, the hazard ratio was 1.07 (95% confidence intervals 1.04–1.12). Table 2 shows the hazard ratios calculated for caries free, caries susceptible and caries active subjects. The 128 subjects who were classified as caries active (D>0) and the 19 caries susceptible subjects (D=0, DMFS>0) were found to have significantly higher hazards of developing molar caries than the 39 caries free subjects with hazard ratios of 2.27 and 2.33 respectively. Dark spots but not white spots were found to be associated with a significantly increased risk of caries development with hazard ratios of 1.49 and 0.78 respectively.
The combined effect of occlusal color change and visit-1 DMFS status on caries development was then examined (Table 3). Since, as shown in Table 2, both caries active and caries susceptible groups had higher hazard rates for caries development than caries free subjects, these two groups were combined into one group defined as DMFS>0. The caries hazard rate for teeth without occlusal color changes (no spots) in DMFS=0 subjects was used as a reference value. Against this reference value, the hazard ratios were calculated for teeth with white or dark spots in DMFS=0 subjects and for teeth with white spots, dark spots or teeth lacking color changes in DMFS>0 subjects.
Table 3.
Results of a Cox’s proportional hazard model examining caries development in permanent molars that were initially caries free. The combined effect of the subject’s visit-1 DMFS status and the presence of occlusal white and dark lesions were evaluated. Using caries development in teeth lacking visit-1 color changes in subjects with a DMFS=0 as a reference value, the hazard ratios were calculated for 5 other groups based on the presence of white or dark lesions and based on subjects having a visit-1 DMFS value of 0 or DMFS>0.
| Variable | Number of molars | Hazard ratio | 95% Confidence limits | ||
|---|---|---|---|---|---|
| DMFS- 2 category: | DMFS=0 No spots |
134 | Reference | ||
|
|
|||||
| DMFS=0 | DMFS=0 White spot |
54 | 0.98 | 0.38 | 2.50 |
|
|
|||||
| DMFS>0 | DMFS=0 Dark spot |
33 | 0.83 | 0.27 | 2.57 |
|
|
|||||
| Combined effect with Transilluminator Classification | DMFS>0 No spot |
166 | 2.61* | 1.09 | 3.91 |
|
| |||||
| DMFS>0 White spot |
178 | 1.59 | 0.83 | 3.06 | |
|
| |||||
| DMFS>0 Dark spot |
176 | 3.38* | 1.86 | 6.17 | |
Significant difference at 0.05 level.
In subjects with DMFS=0, white spots and dark spots were associated with insignificant hazard ratios of 0.98 and 0.83 respectively. In subjects with DMFS values greater than 0, significant differences in caries hazard were observed depending on the initial condition of the molar. The presence of white spots in DMFS>0 subjects was not associated with a statistically significant increased hazard ratio (1.59) of caries. In contrast, the presence of dark spots was associated with a significant hazard (3.38) of caries compared to no spot teeth in DMFS=0 subjects. In the DMFS>0 group, teeth with no detected visit-1 color change had a significantly increased hazard (2.61) of caries development compared to no spot teeth in DMFS=0 subjects.
4. Discussion
Dental caries in underserved youth continues to be a major public health issue. This study and a companion investigation of localized aggressive periodontal disease in Newark, NJ school children was designed to study the early stages and progression of periodontal disease and caries in an urban population. The goal of the study was to identify risk factors for future occlusal decay that could be readily assessed during routine dental examinations.
The diagnosis of cavitated occlusal lesions was accomplished by visual and tactile examination. Although concerns with the use of the dental explorer in the caries detection have been expressed, this is still a widely used diagnostic procedure.18–20 In this study a gentle probing procedure was used to detect areas of pathological pit and fissure enlargement. Molars that were free of probeable lesions or restorations were then examined with a transilluminator to detect non-cavitated white and dark areas. Previous studies have shown transilluminators to be a useful aid in detecting subtle caries-related color changes on the occlusal surface.21,22
We characterized the caries prevalence in over 1200 subjects between the ages of 10–18. In this population a small percentage of subjects were free of caries or precarious white or dark lesions. By the clinical criteria used, the proportion of children requiring at least one dental restoration was above the national average cited in the recent Surgeon’s General report.1 This finding documents the need for improved methods of caries diagnosis and prevention in our local community.
Longitudinal data spanning an average period of 1.3 years was collected for 227 of the 1257 subjects. This large loss of subjects occurring between the first and second visits may be due to the dynamic nature of this urban subject population and highlights the need to recruit large numbers of subjects in longitudinal studies. The difficulty retaining subjects was predicted in the initial study design, where the plan was to visit as many schools as possible and perform the initial screening on all students meeting the inclusion criteria.
Our results and the literature indicate that erupted molars in children of this age group are susceptible to occlusal decay. Overall, 31.6% of initially intact occlusal surfaces developed caries during the course of the longitudinal study. This is higher than what was reported in other studies involving this general age group. 10.5% of occlusal surfaces developed decay per-year in a study of 10–16 year-olds on Long Island, New York 23. In Scottish children, 41% of maxillary and 39% of mandibular molars, developed decay over a 3-year period.24 The higher rate of caries development observed in this study may be due to the socioeconomic status of the population, with the City of Newark having a substantially lower median household income than the State of New Jersey as a whole.25
The contribution of several independent variables, assessed at the first visit, including: patient’s demographics, patient’s DMFS, as well as the presence of occlusal white/dark spots, on the subsequent development of occlusal caries was evaluated by a Cox proportional hazard model (Table 2). Increasing DMFS values were significantly associated with increased hazard of developing occlusal caries. Subjects who at the first visit were observed to be both caries active and caries susceptible had significantly higher hazards of developing occlusal lesions, than subjects who were caries and restoration free. These observations agree with other reports that demonstrate the importance of prior caries experience in predicting the risk of future caries.9
Although the majority of molars that developed new probeable lesions had pre-existing white or dark lesions at the first visit, our results indicate that two types of lesions differ in their propensity to progress into probeable lesions. As seen in Table 2, molars with occlusal white spots did not have a significantly different hazard of caries development than molars that lacked these lesions. In contrast molars with initially non-probeable dark lesions showed a significantly higher (1.49) hazard of caries development than teeth with no-color changes or teeth with white lesions.
The combined effect of DMFS status (DMFS=0 or DMFS>0) and occlusal white or dark spots was examined using a Cox proportional hazard model that evaluated these factors together. The group consisting of teeth with no spots in DMFS=0 subjects was designated as the reference group for the analysis since this group could be thought of as presenting no evidence of caries or color changes indicative of the early stages of caries. As seen in Table 3, in subjects with visit-1 DMFS of zero, neither white nor dark spots were associated with a hazard of decay that was significantly higher than that for teeth with no spots.
In subjects with a DMFS>0 the pattern was quite different. Teeth with dark lesions had a substantially higher (3.38) hazard ratio than no spot teeth in DMFS=0 subjects. In contrast, teeth with white spots in DMFS>0 subjects did not have a significantly higher hazard ratio than no spot teeth in DMFS=0 subjects. Teeth with no spots in the DMFS>0 group behaved in a manner akin to the teeth in those subjects having dark spots in that they had significantly higher hazard ratio (2.61) than identically appearing, no spot teeth in DMFS=0 subjects.
Our observation concerning the proportion of teeth with occlusal discoloration that progressed to probeable lesions agree with the results of a study conducted in Puerto Rico where 34% of molars with visually detected color changes progressed to more severer clinical scores in 12 months.13 In that study the ICDAS (International Caries Detection and Assessment System) was used to visually score occlusal surfaces. The ICDAS does not distinguish between white and dark lesions.26 Our results indicate that the distinction between white and dark lesions is important since these types of lesions may behave differently in terms of caries progression. Our results also show that the subject’s caries history has an important influence over caries risk.
The low frequency of progression to probeable caries, we observed in teeth with white lesions is consistent with the well-documented capacity of these lesions to remineralize.9,27 Remineralized white spots can be resistant to future demineralization due to acid induced modifications of the enamel composition.28 These finding need to be verified in longer duration longitudinal studies since the rate of progression to cavitation may be low and more probeable lesions may have become apparent over time. It would also be interesting to determine if the static nature of white lesions observed in this study, could also be observed in populations with a high rate of caries development.
Teeth with occlusal dark spots were found to have a higher hazard of developing probable lesions in subjects with a first visit DMFS>0 but not in DMFS=0 subjects. These data indicate that these dark lesions represent, in some cases at least, true nonprobeable carious lesions depending on the patient’s caries susceptibility. In primary molars with nonprobeable lesions; dark discolored dentin was observed to harbor culturable bacteria in only 33% of the teeth examined.29 Thus based on clinical examination, it is impossible to tell if occlusal dark spots represent areas where decay has arrested or is progressing. In DMFS=0 subjects dark lesions may have a very low tendency or slow progression to probeable decay, possibly representing arrested lesions.
A sizeable proportion, (36.4%) of the teeth that developed probeable lesions during the course of the study were free of visible occlusal color changes at the initial visit. In DMFS>0 subjects, teeth with no spots had a higher hazard of caries development than no spot teeth in DMFS=0 subjects indicating the importance of the subject’s caries experience in determining risk of future caries. These teeth may have developed caries rapidly, making the transition from intact to carious entirely within the inter-visit interval. Alternatively, these teeth may have had occlusal color changes at visit-1 that were undetectable due to small size or inaccessible location. It is likely that although the transillumunator assisted in the detection of these lesions, this device was not completely effective.
The results obtained in this study demonstrate that both the subject’s caries experience and the condition of the individual tooth should be taken into consideration in determining the caries risk of a particular occlusal site. Clinicians should factor together both considerations when assessing the caries risk of individual tooth sites.
The examination procedures used here were typical of those routinely performed in dental offices with the exceptions that radiographs were omitted and the molars were examined with a hand-held transilluminator. These results support the utility of transilluminators in detecting subtle occlusal color changes.
Placement of restorations was assumed to be due to the presence of caries. Sealants, not commonly encountered, were classified as restorations, thus the number of filled surfaces may have overestimated the subject’s past caries experience. The practice of scoring sealants as restorations may also have led to a higher count of filled surfaces at recall exams and exaggerated our assessment of intact teeth developing caries. In this study no information was collected concerning the subject’s diet or oral hygiene practices.
Caries requires time to develop; the main limitation of the study was the fairly short period of time over which the patients were followed. Since the data was collected from clinical examinations alone, without radiographs, it is likely that this study underestimated caries incidence. Most of our subject’s primary teeth were lost when we examined them for the first time. This may have caused us to underestimate their true previous caries experience.
The ability of fluoride, oral hygiene improvements and dietary modification to effect remineralization of smooth surface enamel lesions is well established. The efficacy of these measures on occlusal caries is less clear. Pit and fissure sealants hinder occlusal decay by preventing the egress of organisms and substrate into the narrow confines of fissure. Recent studies supporting the effectives of sealants30,31 taken together with the results of this study strongly argue in favor of early sealant application to molars in caries active and caries susceptible children, and especially to teeth with nonprobeable dark lesions.
The results of this study indicate that occlusal caries remains a significant health problem for Newark, NJ school children. By performing careful examinations at regular intervals, teeth and individuals at risk can be identified. The ability to diagnose molars with precavited lesions indicates that this population would benefit from intense preventive and minimally invasive caries treatment. These results also suggest that since this population experiences a relatively high increase in carious lesions over short periods of time, it may be an attractive target for caries clinical trials involving new preventive and therapeutic agents.
Acknowledgments
The authors thank Dr. Barbara Greenberg and Shuying Jiang in the NJDS Office of Research for guidance and assistance with the statistical analysis. We thank the Delta Dental Foundation of New Jersey for supporting the early stages of this research and the Colgate Palmolive Corporation for allowing us to use their mobile dental facility to conduct this study. We thank the National Institute of Dental and Craniofacial Research for providing financial support in the form of grant DE-017968 to Daniel H. Fine.
Footnotes
Conflict of interest:
The authors have no conflict of interest related to this study.
Ethics:
Approval of the university’s institutional review board (protocol # 0120020236), parental consent and subject assent was obtained prior to conducting the examinations.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Evans CA, Kleinman DV. The Surgeon General’s report on America’s oral health: opportunities for the dental profession. J Am Dent Assoc. 2000;131(12):1721–8. doi: 10.14219/jada.archive.2000.0118. [DOI] [PubMed] [Google Scholar]
- 2.Domejean-Orliaguet S, Gansky SA, Featherstone JD. Caries risk assessment in an educational environment. J Dent Educ. 2006;70(12):1346–54. [PubMed] [Google Scholar]
- 3.Disney JA, Graves RC, Stamm JW, Bohannan HM, Abernathy JR, Zack DD. The University of North Carolina Caries Risk Assessment study: further developments in caries risk prediction. Community Dent Oral Epidemiol. 1992;20(2):64–75. doi: 10.1111/j.1600-0528.1992.tb00679.x. [DOI] [PubMed] [Google Scholar]
- 4.van Palenstein Helderman WH, van’t Hof MA, van Loveren C. Prognosis of caries increment with past caries experience variables. Caries Res. 2001;35(3):186–92. doi: 10.1159/000047454. [DOI] [PubMed] [Google Scholar]
- 5.Divaris K, Fisher EL, Shugars DA, White RP., Jr Risk Factors for Third Molar Occlusal Caries: A Longitudinal Clinical Investigation. J Oral Maxillofac Surg. 2012 doi: 10.1016/j.joms.2011.12.035. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 6.Shugars DA, Elter JR, Jacks MT, White RP, Phillips C, Haug RH, et al. Incidence of occlusal dental caries in asymptomatic third molars. J Oral Maxillofac Surg. 2005;63(3):341–6. doi: 10.1016/j.joms.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 7.Bader JD, Perrin NA, Maupome G, Rush WA, Rindal BD. Exploring the contributions of components of caries risk assessment guidelines. Community Dent Oral Epidemiol. 2008;36(4):357–62. doi: 10.1111/j.1600-0528.2007.00399.x. [DOI] [PubMed] [Google Scholar]
- 8.Quaglio JM, Sousa MB, Ardenghi TM, Mendes FM, Imparato JC, Pinheiro SL. Association between clinical parameters and the presence of active caries lesions in first permanent molars. Braz Oral Res. 2006;20(4):358–63. doi: 10.1590/s1806-83242006000400014. [DOI] [PubMed] [Google Scholar]
- 9.Zandona AF, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc. 2006;137(12):1675–84. doi: 10.14219/jada.archive.2006.0113. [DOI] [PubMed] [Google Scholar]
- 10.Lussi A, Hibst R, Paulus R. DIAGNOdent: an optical method for caries detection. J Dent Res. 2004;83 (SpecC):C80–3. doi: 10.1177/154405910408301s16. [DOI] [PubMed] [Google Scholar]
- 11.ten Cate JM. Remineralization of caries lesions extending into dentin. J Dent Res. 2001;80(5):1407–11. doi: 10.1177/00220345010800050401. [DOI] [PubMed] [Google Scholar]
- 12.Silva BB, Severo NB, Maltz M. Validity of diode laser to monitor carious lesions in pits and fissures. J Dent. 2007;35(8):679–82. doi: 10.1016/j.jdent.2007.05.005. [DOI] [PubMed] [Google Scholar]
- 13.Ferreira Zandona A, Santiago E, Eckert G, Fontana M, Ando M, Zero DT. Use of ICDAS combined with quantitative light-induced fluorescence as a caries detection method. Caries Res. 2010;44(3):317–22. doi: 10.1159/000317294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fontana M, Santiago E, Eckert GJ, Ferreira-Zandona AG. Risk factors of caries progression in a Hispanic school-aged population. J Dent Res. 2011;90(10):1189–96. doi: 10.1177/0022034511413927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fine DH, Markowitz K, Furgang D, Fairlie K, Ferrandiz J, Nasri C, et al. Aggregatibacter actinomycetemcomitans and its relationship to initiation of Localized Aggressive Periodontitis: A longitudinal cohort study of initially healthy adolescents. J Clin Microbiol. 2007;45(12):3859–69. doi: 10.1128/JCM.00653-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Loesche WJ, Straffon LH. Longitudinal investigation of the role of Streptococcus mutans in human fissure decay. Infect Immun. 1979;26(2):498–507. doi: 10.1128/iai.26.2.498-507.1979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kopycka-Kedzierawski DT, Billings RJ. A longitudinal study of caries onset in initially caries-free children and baseline salivary mutans streptococci levels: a Kaplan-Meier survival analysis. Community Dent Oral Epidemiol. 2004;32(3):201–9. doi: 10.1111/j.1600-0528.2004.00153.x. [DOI] [PubMed] [Google Scholar]
- 18.Hamilton JC. Should a dental explorer be used to probe suspected carious lesions? Yes--an explorer is a time-tested tool for caries detection. J Am Dent Assoc. 2005;136(11):1526, 28. doi: 10.14219/jada.archive.2005.0082. 30 passim. [DOI] [PubMed] [Google Scholar]
- 19.Stookey G. Should a dental explorer be used to probe suspected carious lesions? No--use of an explorer can lead to misdiagnosis and disrupt remineralization. J Am Dent Assoc. 2005;136(11):1527, 29, 31. [PubMed] [Google Scholar]
- 20.Wagner J, Thomas G, Stanford C. Forces exerted by a conventional dental explorer during clinical examination. Caries Res. 2003;37(5):365–8. doi: 10.1159/000072169. [DOI] [PubMed] [Google Scholar]
- 21.Cortes DF, Ellwood RP, Ekstrand KR. An in vitro comparison of a combined FOTI/visual examination of occlusal caries with other caries diagnostic methods and the effect of stain on their diagnostic performance. Caries Res. 2003;37(1):8–16. doi: 10.1159/000068230. [DOI] [PubMed] [Google Scholar]
- 22.Cortes DF, Ekstrand KR, Elias-Boneta AR, Ellwood RP. An in vitro comparison of the ability of fibre-optic transillumination, visual inspection and radiographs to detect occlusal caries and evaluate lesion depth. Caries Res. 2000;34(6):443–7. doi: 10.1159/000016621. [DOI] [PubMed] [Google Scholar]
- 23.Ripa LW, Leske GS, Varma AO. Longitudinal study of the caries susceptibility of occlusal and proximal surfaces of first permanent molars. J Public Health Dent. 1988;48(1):8–13. doi: 10.1111/j.1752-7325.1988.tb03154.x. [DOI] [PubMed] [Google Scholar]
- 24.Chestnutt IG, Schafer F, Jacobson AP, Stephen KW. Incremental susceptibility of individual tooth surfaces to dental caries in Scottish adolescents. Community Dent Oral Epidemiol. 1996;24(1):11–6. doi: 10.1111/j.1600-0528.1996.tb00804.x. [DOI] [PubMed] [Google Scholar]
- 25.Newark NJ. QuickFacts from the US Census Burau. 2011 http://quickfacts.census.gov/qfd/states/34/3451000.html.
- 26.Kuhnisch J, Berger S, Goddon I, Senkel H, Pitts N, Heinrich-Weltzien R. Occlusal caries detection in permanent molars according to WHO basic methods, ICDAS II and laser fluorescence measurements. Community Dent Oral Epidemiol. 2008;36(6):475–84. doi: 10.1111/j.1600-0528.2008.00436.x. [DOI] [PubMed] [Google Scholar]
- 27.Karlsson L, Lindgren LE, Trollsas K, Angmar-Mansson B, Tranaeus S. Effect of supplementary amine fluoride gel in caries-active adolescents. A clinical QLF study. Acta Odontol Scand. 2007;65(5):284–91. doi: 10.1080/00016350701620644. [DOI] [PubMed] [Google Scholar]
- 28.Robinson C, Shore RC, Brookes SJ, Strafford S, Wood SR, Kirkham J. The chemistry of enamel caries. Crit Rev Oral Biol Med. 2000;11(4):481–95. doi: 10.1177/10454411000110040601. [DOI] [PubMed] [Google Scholar]
- 29.Arif N, Beighton D, Sheehy EC. Microbiological assessment of occlusal brown-spot lesions in primary molars. Caries Res. 2006;40(5):398–402. doi: 10.1159/000094285. [DOI] [PubMed] [Google Scholar]
- 30.Oong EM, Griffin SO, Kohn WG, Gooch BF, Caufield PW. The effect of dental sealants on bacteria levels in caries lesions: a review of the evidence. J Am Dent Assoc. 2008;139(3):271–8. doi: 10.14219/jada.archive.2008.0156. [DOI] [PubMed] [Google Scholar]
- 31.Griffin SO, Oong E, Kohn W, Vidakovic B, Gooch BF, Bader J, et al. The effectiveness of sealants in managing caries lesions. J Dent Res. 2008;87(2):169–74. doi: 10.1177/154405910808700211. [DOI] [PubMed] [Google Scholar]