

Abstract
Despite the clinical success of anti-tumor necrosis factor (TNF) therapies in the treatment of inflammatory conditions such as rheumatoid arthritis, Crohn disease and psoriasis, full control of the diseases only occurs in a subset of patients and there is a need for new therapeutics with improved efficacy against broader patient populations. One possible approach is to combine biological therapeutics, but both the cost of the therapeutics and the potential for additional toxicities needs to be considered. In addition to the various mediators of immune and inflammatory pathways, angiogenesis is reported to contribute substantially to the overall pathogenesis of inflammatory diseases. The combination of an anti-angiogenic agent with anti-TNF into one molecule could be more efficacious without the risk of severe immunosuppression. To evaluate this approach with our Zybody technology, we generated bispecific antibodies that contain an Ang2 targeting peptide genetically fused to the anti-TNF antibody adalimumab (Humira®). The bispecific molecules retain the binding and functional characteristics of the anti-TNF antibody, but with additional activity that neutralizes Ang2. In a TNF transgenic mouse model of arthritis, the bispecific anti-TNF-Ang2 molecules showed a dose-dependent reduction in both clinical symptoms and histological scores that were significantly better than that achieved by adalimumab alone.
Keywords: Adalimumab, Ang2, TNF, Zybody, arthritis, bispecific antibody, inflammation
Introduction
Monoclonal antibodies (mAbs) that target specific proteins with high affinity and selectivity have become very important in the treatment of diseases. However, these mAbs recognize only a single target whereas multiple lesions or perturbations in different pathways commonly contribute to the overall pathology of a disease. It is therefore likely that therapeutics that are able to simultaneously target more than one mediator of a disease would be more efficacious or treat a broader spectrum of patients.
In various inflammatory conditions such as rheumatoid arthritis (RA), Crohn disease and psoriasis, antibodies against TNF, including adalimumab (Humira®) and infliximab (Remicade®), are extensively used,1-4 but the degree to which patients respond varies considerably. About 20–30% of RA patients are refractory to anti-TNF therapy, and even in patients who do respond, many of the responses can be considered partial.5,6 This has lead to the evaluation of inhibitors of other immune pathways that may also be involved in the initiation and progression of the inflammatory diseases. However, the individual targeting of pathways for interleukin (IL)-1, IL-6, CD20, IL-12/IL-23, CD86, CD80, and the integrins has shown varying degrees of clinical efficacy.1 Because of the pleiotropic nature of these diseases, it is likely that the concomitant disruption of two or more targets in the disease pathways would be more efficacious than the current monotherapy, provided that this could be done without further increasing the toxicity in patients.
In a TNF transgenic model of arthritis, the combination of infliximab (anti-TNF) with the IL-1 receptor antagonist anakinra lead to complete remission of the disease,7 however, a high incidence of opportunistic infections was observed in patients who had been treated with biologics that modulated these two targets.8 Similarly, the combination of TNF antagonists with the co-stimulation blocker cytotoxic T-lymphocyte antigen 4 (CTLA4)-Ig, which targets CD80 and CD86, was found to be too immunosuppressive and did not markedly further influence disease.9 Thus, when considering the disruption of more than one pathway in inflammation, it is desirable to disrupt an appropriate pathway that may contribute to the inflammatory response, but to do this without further exacerbation of the immunosuppressive effect of TNF antagonists.
Angiogenesis is a physiological process in which new blood vessels are formed from the existing blood vessels and it is essential for tissue growth and maintenance. In cancer, inhibitors of angiogenesis have been demonstrated to have therapeutic benefits both in various preclinical animal models and in patients. The inhibitors of vascular endothelial growth factor (VEGF) and its receptors are the most extensively studied.10-14 More recently, the role of the angiopoietins in cancer has been evaluated both preclinically and in patients.15-20
Angiopoietin (Ang) 1 and Ang2 are ligands of a tyrosine kinase receptor, Tie2, and play an important role in controlling angiogenesis and vascular stability.21 Both Ang1 and Ang2 bind with similar affinity to Tie2, a tyrosine kinase receptor that is expressed mostly on endothelial cells, but also on some hematopoietic cells.22,23 Ang1 is a Tie2 agonist that promotes stabilization of blood vessels.22,24,25 In contrast, Ang2 acts as an antagonist of Tie2 by blocking Ang1 mediated activation.22,26 At high concentrations, Ang2 has been shown to promote endothelial cell survival through activation of the PI-3 kinase/Akt pathway.27,28 Unlike Ang1, Ang2 causes destabilization of the endothelium and promotes angiogenesis by sensitizing the endothelium to other angiogenic factors, particularly VEGF.29 Direct evidence for the involvement of Ang2 in angiogenesis came from preclinical studies in which treatment of tumor bearing mice with either an Ang2 specific antibody or peptibody inhibited angiogenesis and tumor growth.15-18 Perhaps not surprisingly, the therapeutic targeting of Ang1 or Ang2 appears to be different compared with that of antagonism of the VEGF pathway. AMG-386, a peptibody that targets both Ang1 and Ang2, was well-tolerated in cancer patients, and while still showing anti-tumor activity, the therapeutic had different and less severe side effects from those seen with the VEGF inhibitors.19,20
It has recently been recognized that one or more components of the angiogenesis pathways may initiate or exacerbate chronic inflammation.30-34 In preclinical studies in various animal models of inflammation, an anti-VEGF antibody was shown to be effective in reducing the onset of clinical symptoms.35,36 Furthermore, the bispecific molecule ‘Valpha’ that targets TNF and VEGF, showed superior efficacy over the single agent in animal models of retinopathy and psoriasis.37
In addition to the role of the VEGF family of proteins in inflammation, the role of the angiopoetin/Tie2 pathway has recently gained much attention. Ang1 exhibits anti-inflammatory properties and stabilizes the endothelium.38-41 In contrast, recent data suggest that Ang2 is pro-inflammatory and may play a very significant role in inflammation.34,42 Ang2 is stored in endothelial Weibel-Palade bodies and is released rapidly upon stimulation by proinflammatory mediators.43 Ang2 also sensitizes endothelial cells to TNF which in turn induces integrin expression and increased adhesion to monocytic cells.30,44 Administration of recombinant Ang2 to mice induces edema formation.45 In Ang2 transgenic mice, the endothelial-specific overexpression of Ang2 leads to the accumulation of Tie2-positive myeloid cells (TEM) in various organs and to an increased inflammatory response in animal models of delayed type hypersensitivity and peritonitis.42 Furthermore, studies with Ang2-deficient mice demonstrated that the animals had a defective inflammatory response to thioglycollate-induced peritonitis and reduced severity in some clinical features of experimental colitis.30,44,46 In humans, serum levels of Ang2 are elevated in patients with SLE,47 sepsis,48,49 systemic sclerosis,50 COPD,51 psoriasis,52 and arthritis.53,54 In most cases, the elevated levels of Ang2 are associated with increased disease severity. Taken together, these studies demonstrate that Ang2 is likely both an inducer of angiogenesis and also plays a very important role in the pathology of inflammatory diseases.
These data suggest that a combination of anti-TNF with an anti-angiogenic agent might control inflammatory disease more effectively. In patients in the oncology setting, disruption of either the VEGF or angiopoetin pathways does not appear to markedly influence the innate or acquired immune responses,19,20,55 thus suggesting that these might be appropriately safe targets to combine with an anti-TNF approach. However, some other serious safety issues have been reported for VEGF blockers in cancer patients.56 It is thus uncertain whether targeting VEGF pathways is a viable clinical option for treatment of inflammatory conditions. Likely a more appropriate option is to target Ang2 together with an anti-TNF antibody. This combination may have enhanced efficacy in the treatment of inflammatory diseases without having the severe toxicity that may be associated with the other drug combinations. We therefore chose to evaluate the effectiveness of simultaneous blocking of TNF and the angiogenic/proinflammatory molecule Ang2 in the treatment of inflammatory diseases using a bispecific antibody generated with our Zybody technology.
The objective of this study was to determine if there is a beneficial effect in neutralizing Ang2 activity in combination with anti-TNF therapy in inflammatory diseases using a novel class of multi-specific therapeutics. We report the generation of bispecific molecules (Zybodies) by the genetic fusion of Ang2-targeting peptides to the C-terminus of the heavy chain of an anti-TNF antibody; these bispecific molecules exhibit properties similar to those seen with conventional mAbs. The anti-TNF and Ang2 bispecific Zybodies retained both anti-TNF and effector functions of the parental antibody, but also effectively neutralized Ang2. Furthermore, in the Tg197 TNF transgenic mouse model of RA, the Zybodies showed efficacy that was significantly superior to adalimumab in attenuating the clinical symptoms and histological changes in the joints.
Results
Generation and characterization of anti-TNF and Ang2 bispecific Zybody
The anti-TNF antibody adalimumab was used as a scaffold to construct the anti-TNF and Ang2 bispecific Zybodies. The Ang2 specific peptides, a2, a3 and a4 (Table S1) were generated using peptide phage display as to be described elsewhere (unpublished data). The peptides were genetically fused to the C-terminus of the heavy chain of adalimumab (Fig. 1A) to generate three bispecific Zybodies, ADA-a2H, ADA-a3H and ADA-a4H. For use as a control Zybody, an Ang2 peptide, a2 was fused to the trastuzumab (Herceptin®) scaffold in an identical manner. The Zybodies were cloned as independent heavy or light chain expression constructs into pCEP4 vector and HEK293F cells were then transiently transfected with light and heavy chain constructs at equimolar ratios. The proteins were purified using Protein A affinity chromatography following the general procedures used for conventional mAbs. The analytical and stability properties of the Zybody ADA-a2H are shown in Figure 1. The purity of ADA-a2H, as measured by size-exclusion chromatography (SEC), was ~95%; and 99% for clinical grade adalimumab (Fig. 1B). Upon storage at 30°C for seven weeks, the rate of degradation (indicated by a decrease of the monomer fraction in SEC) for the Zybody was similar to that of adalimumab despite the slightly lower monomer level at the start of the study (Fig. 1C). ADA-a2H and adalimumab were also analyzed by SDS-PAGE under reducing (lanes 1 and 2) and non-reducing conditions (lanes 3 and 4). There was no difference in the apparent molecular weight of the light chains of the adalimumab molecules, whereas the heavy chain of the Zybody that was fused with the Ang2-binding peptide migrated at a position corresponding to a higher molecular weight (Fig. 1D) due to the presence of the Ang2 binding peptide on the C-terminus of the heavy chain.

Figure 1. Generation of ADA-a2H bispecific Zybody. (A) Schematic diagram to illustrate ADA-a2H generated by fusion of Ang2 specific peptide to C-terminus H-chains of the adalimumab scaffold; (B) Size exclusion chromatography (SEC) profiles of adalimumab; solid line-ADA-a2H, dotted line- adalimumab; (C) Effect of storage at 30°C on the monomer purity of adalimumab and ADA-a2H as measured by SEC; (D) SDS PAGE analysis of purified ADA-a2H (lane 2 and 4) and adalimumab (lane 1 and 3); (E) DSC analysis of ADA-a2H and adalimumab.
Since addition of certain peptides and scFvs has in some cases given rise to the destabilization of the core mAb,57,58 we evaluated the thermal stability of ADA-a2H and adalimumab using differential scanning calorimetry (DSC). The domains of both adalimumab and ADA-a2H unfolded similarly with the lowest transition temperature (Tm) for ADA-a2H and adalimumab being 67.1°C and 67.5°C respectively and the most prominent transition temperature being 70.7°C for ADA-a2H and 71.9°C for adalimumab, respectively (Fig. 1E). These results indicate that the thermodynamic stability of ADA-a2H is very similar to that of adalimumab.
Simultaneous binding of the bispecific Zybody to TNF and Ang2
To be effective in neutralizing the two target proteins in a disease setting, the bispecific antibody should bind to both proteins simultaneously with high affinity. The binding of ADA-a2H to TNF and Ang2 was demonstrated by ELISA and Surface Plasmon Resonance (SPR). In ELISA assays, ADA-a2H binding to plate-coated Ang2 was detected with biotinylated TNF. As shown in Figure 2A, ADA-a2H binds to both plate-coated Ang2 and biotinylated TNF whereas no binding of adalimumab to Ang2 was observed. In a similar way, the binding of ADA-a2H to plate-bound TNF was also detected with biotin labeled Ang2 (data not shown). Simultaneous binding of ADA-a2H to both proteins could also be detected by SPR, using a Biacore 3000 analyzer. ADA-a2H was captured with an anti-human Fc antibody immobilized on a CM5 chip and the binding to target proteins was observed by sequential injection of Ang2 and TNF at saturating concentrations. As expected for simultaneous binding, sequential injections of Ang2 and TNF led to respective sequential increases in the SPR signal (Fig. 2B).
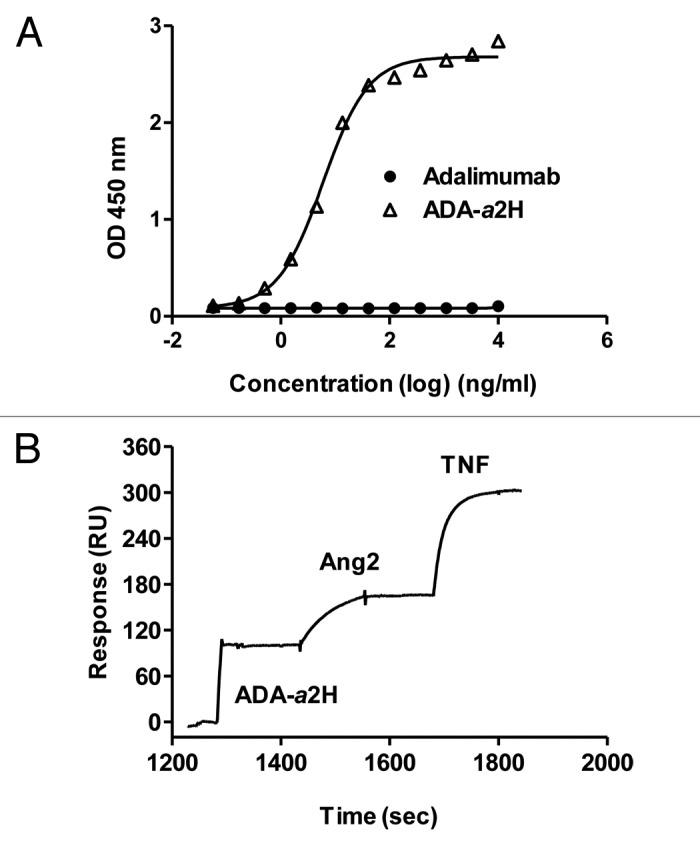
Figure 2. Simultaneous binding of ADA-a2H to TNF and Ang2. (A) ADA-a2H binding to plate bound Ang2 was detected by ELISA using biotinylated TNF. Error bars represent mean ± SEM; (B) SPR analysis of dual binding. ADA-a2H was captured by anti-human Fc antibody on to a CM5 chip. Ang2 and TNF were sequentially injected and the binding was indicated by increase in RU. Data are representatives of two independent experiments.
Binding kinetics of the bispecific Zybody, ADA-a2H to TNF and Ang2
To measure the binding kinetics of the molecule to TNF, soluble TNF was flowed over adalimumab or ADA-a2H that was captured on a CM5 chip via an anti-human Fc antibody. Individual SPR sensorgrams are presented in Figures 3A and B. The calculated association rate constant (ka: 4.0 ± 0.6 X 105 M−1 s−1) and the dissociation rate constant (kd: 8.2 ± 0.74 X 10−5s−1) of ADA-a2H binding to TNF were similar to that of adalimumab (ka: 3.79 ± 0.63 X 105M−1 s−1; kd: 7.24 ± 0.47 X 10−5 s−1). Likewise, the deduced binding affinity of ADA-a2H to TNF (KD: 0.22 ± 0.06 nM) was comparable to adalimumab (KD: 0.21 ± 0.05 nM). The binding characteristics of ADA-a2H to Ang2 were assessed using His-tagged Ang2 (R&D). Ang2 material obtained from the commercial source is a heterogeneous mixture with predominantly higher order multimers (data not shown) and its binding kinetics could not be determined due to negligible off rate when injected on to immobilized ADA-a2H. Since it has been studied that avidity can be negligible at low antigen density (Pol et al., Biacore™ T200 presentation), we captured Ang2 at low RU (resonance units) levels onto CM5 chip and ADA-a2H was flowed over to determine its apparent binding affinity to Ang2 (Fig. 3C). ADA-a2H bound to immobilized Ang2 with a high affinity (KD: 0.59 ± 0.03 nM) and with a dissociation rate, kd, of 1.19 ± 0.15 X 10−3 s−1 and an association rate, ka, of 2.06 ± 0.36 X106 M−1 s−1).

Figure 3. Kinetic measurement of binding to TNF and Ang2 by SPR. (A) ADA-a2H or (B) Adalimumab was captured by anti-human Fc antibody on to a CM5 chip. A range of concentrations of TNF (0.4 nM to 100 nM) were injected over the antibodies. Data was fitted to a 1:1 Langmuir binding model to determine binding parameters; (C) Binding of ADA-a2H to immobilized Ang2. His-tagged Ang2 (R&D) was captured by anti-His antibody on to a CM5 chip. Various concentrations (0.25 nM to 66 nM) of ADA-a2H were injected and flowed over immobilized Ang2. (D) Binding of Ang2 to immobilized ADA-a2H. ADA-a2H was captured using goat anti-human kappa chain (Fab'2) on to a CM5 chip. Various concentrations (1.2 to 100 nM) of Ang2 (Zyngenia) were injected over immobilized ADA-a2H. Binding data were analyzed using a 1:1 Langmuir model. The residual plots of curve fittings are shown. The figures and kinetics parameters values shown are representatives of three independent experiments.
Biacore experiments were also performed with His-tagged Ang2 material prepared in-house (Zyngenia) which is predominantly a dimer (data not shown). In this experiment, ADA-a2H was captured on to a CM5 chip using goat anti-human kappa chain (Fab'2). Various concentrations of Ang2 (1.2 to 100 nM) were injected over the immobilized Zybody. As shown in Figure 3 D Ang2 also bound to immobilized ADA-a2H with a high affinity (KD: 0.97 ± 0.03 nM) and with a dissociation rate (kd) of 1.75 ± 0.39 X 10−4 s−1 and an association rate (ka) of 1.81 ± 0.41 X 105 M−1 s−1). The reported binding affinity (KD) measurements for Ang2 are apparent values as the binding of ADA-a2H to Ang2 may not be strictly 1:1 due to heterogeneity of Ang2 proteins. The closeness of curve fitting (chi2) of binding data for all SPR experiments was determined to be less than 2 RU indicating a good fit. The summary of binding kinetics with chi2 values is included with supplemental data (Table S2).
Characterization of the TNF and Ang2 inhibitory activity of the bispecific Zybody
To examine whether ADA-a2H prevents the binding of Ang2 to its receptor (Tie2), we immobilized Ang2 on a 96-well plate and the inhibition of binding of soluble Tie2 to the plate-bound Ang2 was determined by ELISA. As shown in Figure 4A, ADA-a2H inhibits Tie2 binding to Ang2 in a dose-dependent fashion, whereas adalimumab had no effect. ADA-a2H also inhibits Tie2 binding to mouse Ang2 (Fig. S3).

Figure 4. Inhibition of Ang2 and TNF activity by ADA-a2H. (A) The binding of soluble Tie2 to Ang2 coated on to a microtiter plate was determined by ELISA in presence of various concentrations of ADA-a2H or adalimumab; (B) The binding of TNF to TNFRI and TNFRII coated on to a microtiter plate in the presence of various concentration of adalimumab or ADA-a2H was determined by ELISA; (C) L929 cells were incubated with 1 ng/ml of TNF plus 1 µg/ml of actinomycin D in the presence of various concentrations of antibodies. After 24 h, the cell viability was determined using Cell Titer Glo. The error bars represent mean ± SEM. Data shown are representatives of at least two independent experiments
To determine the ability of ADA-a2H to bind to and neutralize TNF, we employed assays to assess both the inhibition of ligand binding to its receptor and the ability to prevent TNF-induced cytotoxicity in L929 cells. The ability of ADA-a2H and adalimumab to block binding of biotinylated TNF to the immobilized TNFRI or TNFRII receptor was determined using a competition ELISA. ADA-a2H inhibited TNF binding to both of its receptors in a dose-dependent manner with IC50 values similar to that found for adalimumab (Fig. 4B). In the presence of actinomycin D, L929 cells are very sensitive to TNF induced cytotoxicity. ADA-a2H inhibited TNF-induced L929 cell killing in a dose-dependent fashion and again the anti-TNF activity of the Zybody was comparable to that of adalimumab (Fig. 4C, left panel). To determine if Ang2 binding alters the anti-TNF activity of the Zybody, the cytotoxicity assay on L929 cells was repeated in the presence of Ang2. As shown in Figure 4C (right panel), addition of Ang2 had no inhibitory effect on the TNF neutralizing activity of ADA-a2H.
The bispecific Zybody, ADA-a2H simultaneously inhibits both Ang2 and TNF induced signaling in endothelial cells
Ang2 is reported to act mainly as an antagonist by blocking Ang1-induced Tie2 activation and signaling; however, at high concentrations (800 ng/ml) it can also function as an agonist.27,28 In our experiments, treatment of HUVEC with 1–4 μg/ml Ang2 induced Akt activation as measured by an increase in the levels of phosphorylated Akt, whereas at concentrations below 500 ng/ml only very minor increases in the level of phosphorylated Akt were observed (Fig. 5A). Under the experimental conditions we used, the addition of TNF did not increase the level of phosphorylated Akt (Fig. 5A, lane 9). The effect of the bispecific Zybody and control antibodies on the Ang2-mediated activation of Akt was assessed and we found that ADA-a2H (lanes 6 and 9) or the control mAb with anti-Ang2 activity alone (TRA-a2H) (lane 8), but not adalimumab (lane 7), inhibited the Ang2 -induced Akt activation (Fig. 5B).
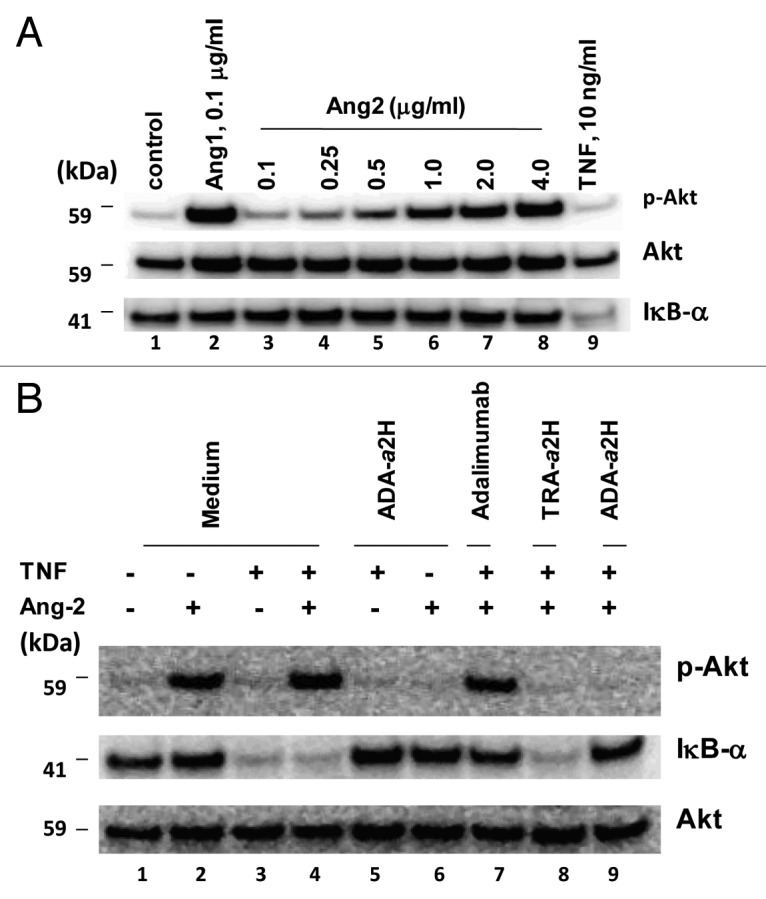
Figure 5. ADA-a2H inhibits TNF and Ang2 –induced signaling in HUVEC. (A) Serum starved HUVEC cells were stimulated with the indicated concentrations of Ang2 for 40 min at 37°C. After lysis and SDS-PAGE, the levels of Akt, phosho-Akt and IκB-α in the cells were determined by western blotting using specific antibodies; (B) HUVEC cells were treated with Ang2 (2 µg/ml) or TNF (10 ng/ml) in the presence of ADA-a2H, adalimumab or TRA-a2H. Western blot analysis was performed using specific antibodies to the indicated proteins. Results shown are representatives of two independent experiments.
TNF is a potent activator of endothelial cells through the induction of multiple signaling pathways including NF-κB, the caspases and MAP kinase.59 We followed the TNF-induced activation of the NF-κB pathway in HUVEC by measuring the loss of the protein IκB-α (Fig. 5B). Treatment of cells with adalimumab (lane 7) or ADA-a2H (lanes 5 and 9), but not with the control Zybody TRA-a2H (lane 8), inhibited TNF-induced downregulation of IκB-α. In HUVEC that were stimulated with the combination of Ang2 and TNF, ADA-a2H inhibited activation of both NF-κB and Akt pathways (Fig. 5B, lane 9), whereas adalimumab only inhibited the activation of the NF-κB pathway (Fig. 5B, lane 7).
Fc effector functions of the bispecific Zybody
TNF exists both as a mature soluble protein and in a membrane-associated precursor form; the anti-TNF antibodies infliximab and adalimumab bind to both forms with high affinity.60 It has been reported that these TNF-targeting antibodies, in addition to binding to and neutralizing the cytokine, may also mediate antibody-dependent cell-mediated cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC) on cells that express membrane TNF.61-63 To confirm that ADA-a2H also bound to membrane TNF, 293F cells were transfected with a full length TNF construct (Fig. S4) and the binding affinities of the various antibodies were measured with a saturation binding assay that used Eu-labeled goat anti-human Fc antibody for detection. Both ADA-a2H and adalimumab bind to membrane TNF transfected cells in a dose-dependent fashion and with comparable affinity (Fig. 6A).

Figure 6. ADA-a2H retains the effector functions of adalimumab. (A) Binding to membrane TNF. 293F cells that expressed TNF on the cell surface were incubated with various concentrations of adalimumab or ADA-a2H for 60 min at 4°C. The binding of the antibodies to membrane TNF was determined by a saturation binding assay using Eu-labeled goat anti-human Fc; (B) Binding to FcγRIIIA. Microtiter plates were coated with various concentrations of adalimumab or ADA-a2H at 4°C overnight. Biotin labeled FcγRIIIA (2 μg/ml) was added and incubated in the absence or presence of 1 µg/ml Ang2 at RT for 1 h. Binding of FcγRIIIA-biotin to plate bound antibodies was determined by ELISA; (C) Binding to C1q. Microtiter plates were coated with various concentrations of ADA-a2H or adalimumab overnight at 4°C. The binding of human C1q in absence or presence of 1 µg/ml Ang2 to plate bound antibodies was determined by ELISA using an HRP conjugated sheep anti-human C1q antibody. Error bars represent mean ± SEM. Results shown are representatives of two independent experiments.
To determine if ADA-a2H was likely to retain the effector functions of adalimumab, the ability of the Zybody to bind to soluble FcγRIIIA (CD16A) was determined. Various concentrations of ADA-a2H or adalimumab were captured on to a 96-well plate and the binding of biotin labeled FcγRIIIA was determined by ELISA using an HRP-labeled streptavidin. Both ADA-a2H and adalimumab showed concentration-dependent and saturable binding; furthermore, the binding affinity of ADA-a2H to FcγRIIIA was comparable to that of adalimumab (Fig. 6B). To assess the potential CDC activity of ADA-a2H, we characterized the ability of the Zybody to bind to the complement protein C1q. The binding of ADA-a2H to C1q was concentration-dependent and the EC50 and extent of binding was comparable to that of adalimumab (Fig. 6C). The assay was also performed in presence of Ang2 to determine if binding of Ang2 to ADA-a2H has any effect on its ability to bind FcγRIIIA and C1q. The data indicate that Ang2 has no effect on binding of ADA-a2H to FcγRIIIA and C1q (Fig. 6B and C). Taken together, the results suggest that ADA-a2H is likely to retain all of the effector functions of the parent scaffold antibody.
The bispecific Zybodies show superior efficacy to adalimumab in the Tg197 transgenic model of RA
Both inflammatory and angiogenic pathways are involved in the pathophysiology of rheumatoid arthritis.64 We thus evaluated whether simultaneous targeting of TNF and Ang2 showed any additional benefit over anti-TNF alone in attenuating the disease symptoms in the Tg197 human TNF transgenic mouse model of rheumatoid arthritis.65 Animals were injected intraperitoneally with the Zybodies or adalimumab starting from 3 weeks of age, immediately before the appearance of significant clinical symptoms. The mean histopathological score of the joints from the 3 week untreated control group is 1.5, ranging from 1 to 2, with 1/3 of the analyzed joints scoring at 2 (data not shown). This data suggest that, at 3 weeks of age, Tg197 mice already have an active disease. Animals treated with 3 mg/kg TRA-a2H antibody (the control Zybody that blocks Ang2 alone) showed a weak, but statistically significant, inhibition of the disease score, although less pronounced than that seen with adalimumab alone (Fig. 7A). Treatment of the animals with ADA-a2H at 1, 3 or 10 mg/kg showed a dose-dependent effect on inhibition of in-life arthritic scores (Fig. 7A). ADA-a2H, at the same dose as adalimumab (3mg/kg dose), was significantly more effective in reducing disease symptoms and score (Fig. 7A).

Figure 7. The bispecific anti-TNF-Ang2 Zybodies exhibits superior efficacy in an in vivo model of RA. (A) Mice (n = 8 per group) were treated intraperitoneally twice weekly for seven weeks starting from the third week of age with various doses of ADA-a2H (1, 3 and 10 mg/kg), vehicle control, 3 mg/kg adalimumab or 3 mg/kg control Zybody, TRA-a2H, as indicated. Animals were evaluated for arthritic scores at the indicated times; (B) Mice (n = 8 per group) were treated with 3 mg/kg of ADA-a4H, adalimumab or trastuzumab. Animals were evaluated for arthritic scores at the indicated times; (C) Effect of ADA-a4H on histology scores. After completion of the treatment (week 10) with trastuzumab (n = 5), ADA-a4H (n = 8) and adalimumab (n = 6), the ankle joints were processed and paraffin sections were stained with hematoxylin/eosin. Histopathological scores were evaluated in a blinded fashion; D) Effect of ADA-a3H and adalimumab on arthritic and histological scores. Mice were treated with vehicle control (n = 6), 5 mg/kg ADA-a3H (n = 7) and 5 mg/kg adalimumab (n = 8) as indicated. Histology and arthritic scores were measured after completion of the treatment. Data are presented as mean ± SEM and three independent experiments were performed with Zybodies with the three similar Ang2 peptides shown. *-p < 0.05, **-p < 0.01, ***p < 0.001.
Additional in vivo experiments were performed with Zybodies containing other Ang2 binding peptides (a4 and a3), that, in vitro, had similar human Ang2 binding and inhibitory activity to that of a2 (Figs. S1 and S2). As the amino acid sequence of human and mouse Ang2 are 85% identical,22 we tested the cross-reactivity of our Ang2 binding peptides. While a2 and a3 are equally effective in inhibiting mouse Ang2 activity, the a4 peptide showed relatively lower activity on mouse Ang2 (Fig. S3). At an equivalent dose of 3 mg/kg, ADA- a4H produced significantly greater reduction (p < 0.001) in the arthritic disease scores than did adalimumab (81% vs 55%, respectively; reduction at the end of treatment; Figure 7B). ADA-a3H at a dose of 5 mg/kg was also significantly superior (p < 0.01) to adalimumab in reducing the arthritic scores in treated animals (91% vs 73%, respectively; reduction in arthritic score at the end of treatment; Fig. 7D). In addition, the combined histopathological scores, that were based on a blinded assessment of PMN infiltration, pannus formation, extent of cartilage destruction and bone erosion,66 were determined in these animals. This revealed that the animals treated with ADA-a4H (Fig. 7C) and ADA-a3H (Fig. 7D), had a significantly lower histopathological score (p < 0.05) than did the animals treated with the equivalent dose of adalimumab.
Discussion
There is a considerable interest in the development of more effective treatments for diseases by simultaneously targeting multiple components of the disease pathways. For biological therapeutics, in spite of the promising preclinical data with simultaneous targeting of multiple mediators in the disease pathways,67-69 many of the current approaches to generate multi-specific antibody-like targeting agents58,70 encounter limitations that include poor expression, high levels of aggregation, shorter stabilities, more rapid clearance in vivo, and lack of Fc-effector functions.71,72 We have recently developed a technology that is based on the genetic fusion of target-specific binding peptides to the C or N termini of the heavy or light chains of a conventional antibody, and have found that this technology allows the concomitant engagement of multiple targets while also overcoming many of these described limitations (unpublished results).
In this study, we demonstrated that fusing Ang2-binding peptides to the heavy chain of the anti-TNF adalimumab results in bispecific antibodies that can be easily produced and purified, and that have stability properties, (DCS profile and accelerated long-term storage) that are similar to the parental antibody. We further demonstrate that the bispecific Zybodies retain the full functionality of the parental anti-TNF antibody, but with the added capacity to neutralize Ang2 that is conferred by the fused Ang2-binding peptide. Furthermore, at the same dose, the bispecific antibody exhibits superior efficacy in an in vivo model of RA compared with that of adalimumab.
Several lines of evidence presented in this study demonstrate that the fusion of the Ang2 binding peptides to the adalimumab scaffold has not compromised either the anti-TNF activity or the effector functions of the parental mAb. ADA-a2H exhibited both very similar binding affinity for TNF and ability to neutralize soluble TNF to that of adalimumab. The parameters of the binding kinetics of the Zybody to TNF, were determined by SPR, and are consistent with previous reports for the anti-TNF mAb.73 Since anti-TNF antibodies are reported to bind also to membrane TNF and potentially mediate ADCC and CDC on cells that express surface TNF,61,74 we assessed the ability of ADA-a2H to bind to TNF expressed on the surface of transfected 293F cells, and determined its ability to bind to FcγRIIIA and C1q proteins. The data presented here demonstrate that fusion of an anti-Ang2 peptide to the adalimumab scaffold has no significant effect on the ability of the mAb to bind cell surface TNF and to bind to the effector molecules that mediate these functions. In addition to retaining all the anti-TNF and antibody scaffold functions of adalimumab, ADA-a2H also neutralizes Ang2 as evidenced by the ability to directly bind Ang2 and inhibit Ang2 binding to its cognate receptor Tie-2. We also demonstrated by ELISA and SPR that the anti-TNF and Ang2 bispecific Zybody can bind simultaneously to both targets, TNF and Ang2, and thus is expected to be effective in inhibiting the activity of both pathways.
To confirm further the ability of ADA-a2H to simultaneously antagonize both TNF and Ang2 and to better understand the consequences of dual TNF/Ang2 targeting, we investigated the ability of the Zybody to modulate endothelial cell activation. TNF is a major inflammatory cytokine that also induces angiogenesis indirectly through secondary mediators such as VEGF, fibroblast growth factor and the angiopoietins.75,76 Depending on the dose, TNF is able to induce either proliferation or apoptosis of endothelial cells. At low concentrations, TNF stimulates endothelial cell proliferation and angiogenesis, whereas at high concentrations, it causes apoptosis.77 Ang1 and Ang2 prevent TNF induced endothelial cell apoptosis through activation of the Akt pathway in vitro and enhance TNF mediated angiogenesis in vivo.75 Ang2 also regulates TNF-induced expression of adhesion molecules and the adhesion of leukocytes to the endothelium.30,44 To study the effect of ADA-a2H on the activation of endothelial cells, we followed both the TNF and Ang2-induced signaling pathways in HUVEC. TNF activates both NF-κB and caspase signaling pathways in endothelial cells. NF-κB is a transcription factor present in the cytoplasm in a complex with the inhibitory protein IκB-α. Stimulation of the cells with TNF induces a cascade of signaling events that leads to phosphorylation and degradation of IκB-α, thus releasing NF-κB to translocate to the nucleus; thus measurement of the degradation of IκB-α can be used to assess NF-κB activation.78 We observed that at concentrations above 500 ng/ml, Ang2 is a potent inducer of Akt activation (phosphorylation of Akt) in endothelial cells, but does not activate NF-κB. Stimulation of cells for 40 min with TNF activated the NF-κB pathway with no detectable activation of Akt or ERK. Treatment of endothelial cells with a combination of TNF and Ang2 activated both NF-κB and Akt pathways. The bispecific Zybody, but not adalimumab, inhibited activation of both NF-κB and Akt pathways by the combined treatment with TNF and Ang2. In vivo, it is likely that the combined actions of TNF and Ang2 would stimulate pro-survival pathways and also inhibit apoptotic pathways, which may lead to increased expression of adhesion molecules on the endothelial cells. This, in turn, would contribute to an increased trafficking of pro-inflammatory leukocytes, particularly Tie2 positive myeloid cells, to the sites of inflammation; this then further promotes inflammatory angiogenesis. Thus, simultaneous inhibition of both TNF and Ang2 by bispecific Zybodies may result in enhanced efficacy in inflammatory diseases.
To determine whether there is an increased efficacy in targeting both TNF and Ang2 rather than TNF alone, we evaluated the effect of simultaneous inhibition of TNF and Ang2 with bispecific Zybodies in the Tg197 human TNF transgenic mouse model of arthritis. Rheumatoid arthritis is a complex disease that is mediated by multiple factors. Although it has been demonstrated in patients that inhibition of a single target such as TNF, IL-1 or IL-6 can be effective in attenuating the disease progression and pathology, complete remission is not often achieved.5,6 Because of this, combinations of anti-TNF with other inhibitors such as IL-1Rα, VEGF and RANKL have been evaluated in preclinical models.7,37 The combination of anti-TNF with IL-1Rα was more effective than anti-TNF alone in preventing cartilage damage in a TNF transgenic model of RA.7
Tg197 TNF transgenic mice develop chronic arthritis with clinical symptoms and histological features, such as bone erosion and cartilage destruction that are similar to those observed in human rheumatoid arthritis.65 In our studies, Tg197 animals were treated with the Zybodies or adalimumab beginning at the third week of age, just before development of overt clinical symptoms. As previously reported, the anti-TNF antibody adalimumab alone attenuates the clinical symptoms, weight loss and joint histology score. However, the anti-TNF and Ang2 bispecific Zybodies were significantly more effective in controlling all of these disease symptoms.
Even though combinations have worked well in animal models, one of the critical issues to consider in selecting targets to combine for therapy is the possibility of increased toxicity. Previously the combination of an anti-TNF antibody with inhibitors of other pathways such as IL-1 or CD80 and CD86, showed unacceptable toxicities due to increased susceptibility to infections.1,8 Although it remains to be seen whether simultaneous targeting of TNF and Ang-2 will exhibits similar toxicities, the angiogenic pathways appear to be on a different axis to the immunosuppressive pathways, but still play a role in inflammation. In animals, the Ang2 function appears to be restricted to endothelial cells and a small percentage of Tie2 expressing myeloid cells (TEM) unlike other inflammatory mediators. Only TEM and not other lymphocytes accumulate in mice that overexpress Ang2. In clinical trials in cancer patients, AMG-386, a specific inhibitor of Ang2/Ang1 appeared to be well tolerated with no overt immunosuppression. In addition, the toxicity profile is reported to be different and less severe than that of VEGF inhibitors.19,79,80 Thus, our data suggests that a bispecific Zybody that targets TNF and Ang2 may be a promising approach to improve the treatment of inflammatory diseases without an additional exacerbation of toxicities.
Materials and Methods
Materials
Recombinant human Ang2, soluble Tie2, soluble FcγRIIIA and TNF receptors I and II were purchased from R&D Systems. Recombinant human TNF was from Peprotech. Adalimumab was obtained from Blue Door Pharmacies (Rockville, MD). L929 cells were purchased from ATCC. The peptides targeting Ang2 were identified and affinity matured by phage display methods (unpublished results). In this study, three anti-Ang2-specific peptides, a2, a3 and a4 (sequences shown in Table S1) fused to C-terminus of the heavy chain of adalimumab were used.
Construction and expression of ADA-a2H Zybody
Adalimumab sequences were used as a scaffold to which the Ang2 peptides were genetically fused to the C-termini of the heavy chain through a 6 residue Gly-Ser linker. The sequence of the Zybody heavy chain fusion construct was confirmed and the DNA constructs transiently transfected into HEK293-F cells (Invitrogen) as per manufacturer’s instructions and cultured in shake flasks. After 6 d, the Zybody containing cell culture supernatants were harvested by centrifugation at 2000 × g for 30 min and filtered though a sterile filter (0.22 μm).
Antibodies were purified from filtered cell culture supernatants by chromatography on Protein A SepharoseTM (GE Healthcare). Briefly, the cell culture supernatants were applied to a Protein A SepharoseTM column and bound antibodies were subsequently eluted with 0.1 M glycine pH 3.0 followed by immediate neutralization to pH 7.5. In the event of any protein aggregation, the aggregates were removed by SEC (Superdex 200; GE Healthcare) in 20 mM histidine, 140 mM NaCl, pH 6.0. Monomeric antibody fractions were pooled, concentrated, if required, using an Amicon Ultra (30 molecular weight cutoff) (Millipore) and the concentration was determined by measuring the UV absorbance at 280 nm. Endotoxin levels were measured by the Limulus Amebocyte Lysate (LAL) method (Charles River).
SDS-PAGE
Antibodies (2 µg) were mixed with 20 µl sample buffer alone (non-reducing condition) or in the presence of 20% DTT (reducing) and boiled at 95°C for 5 min. The samples were resolved on a 4–12% SDS Bis-Tris gel (Invitrogen). Following electrophoresis, the bands on the gel were visualized by staining with Coomassie brilliant blue.
Size-exclusion chromatography
Samples were applied to a Sepax SRT SEC-500 column (Sepax Technologies Inc.,) utilizing a mobile phase consisting of 150 mM sodium phosphate at a pH of 7.2. The flow rate was 1.0 ml/min and the eluate was monitored at 280 nm.
Differential scanning calorimetry
The analysis was performed by the Biopharmacy Core facility at the University of Washington, Seattle. A capDSC (GE Healthcare) was utilized for the analysis. For each sample, four buffer vs buffer calorimetric scans were performed prior to running the buffer vs antibody scan. The temperature range scanned was 30–130°C using a scan rate of 60°C/hour. The instrument was operated in “Passive Feedback” mode with a filtering period of 16 sec, a 15 min pre-scan equilibration, and a refill temperature of 35°C.
In vitro stability measurement
The stabilities of the Zybody and adalimumab were assessed at an accelerated temperature of 30°C. Adalimumab (1 mg/ml in PBS) was dialyzed against PBS. The proteins were formulated in PBS at 1 mg/ml. Both proteins were stored in 2 ml polypropylene tubes and their stability was assessed by visual inspection and size-exclusion chromatography after 0, 1, 8 and 18 d of storage at 30°C.
Binding kinetics measurements by surface plasmon resonance
The binding kinetics of antibodies to TNF and Ang2 was measured on a BIAcore 3000 instrument (GE) using HBS-EP running buffer (10 mM HEPES, pH 7.4, 150 mM NaCl, 3 mM EDTA and 0.15% surfactant P20). Goat anti-human IgG Fc-specific antibody (Thermo Fisher) was immobilized to the surface of a CM5 sensor chip using standard amine-coupling chemistry. Adalimumab or ADA-a2H at 10 μg/ml in running buffer was injected over an anti-Fc surface at a flow rate of 30 μl/min. After capturing approximately 50 RU of antibodies, various concentrations of TNF (0.4 nM to 100 nM at 3-fold serial dilutions) were injected at a flow rate of 30 μl/min for 3 min with 10 min dissociation per cycle. After each cycle, surfaces were regenerated with 10 mM glycine, pH 2.0. The data was reference subtracted and fitted to 1:1 Langmuir binding model to obtain the association rate constant (ka), dissociation rate constant (kd) and the equilibrium dissociation rate constant (KD).
The kinetics of Zybody binding to Ang2 was determined as follows. Anti-His IgG (Abcam) was immobilized to the CM5 sensor chip using standard amine coupling procedure as recommended by the manufacturer. Ang2 (R&D Systems) at 1 μg/ml concentration was captured onto the anti-His surface at low levels (~20–40 RU). A range of concentrations (0.25 nM to 66 nM) of ADA-a2H were injected at 30 μl/min for 3 min with 10 min dissociation per cycle. Binding kinetics was also determined with Ang2 prepared at Zyngenia using ADA-a2H captured on to a CM5 chip via goat anti-human kappa chain (Fab'2) (InvivoGen). Various concentrations of Ang2 (1.2 nM to 100 nM) were injected at 30 μl/min for 4 min with 10 min dissociation per cycle. The surface was regenerated with 10 mM glycine, pH 1.5 after each cycle. Binding data were analyzed using a 1:1 Langmuir model.
Determination of simultaneous binding to TNF and Ang2
The simultaneous binding of ADA-a2H to two target proteins, TNF and Ang2 was determined by ELISA. Ang2 (0.5 μg/ml) was coated onto a 96-well ELISA plate (Thermo Electron) overnight at 4°C and then incubated with various concentrations of adalimumab or ADA-a2H for 1 h at RT. The plate was washed four times with washing buffer (PBS, 0.1% Tween 20) and incubated with TNF biotin (100 ng/ml) for 1 h at RT. After washing, the plate was incubated with streptavidin-HRP for 1 h at RT. After the final wash step, 3, 3′, 5, 5′-tetramethylbenzidine (TMB) was added and absorbance was measured at 450 nm using a plate reader (SpectraMax, Sunnyvale, CA).
The simultaneous binding of the Zybody to the target proteins was also determined by SPR. ADA-a2H was captured using goat anti-human Fc antibody immobilized onto a CM5 sensor chip as described above followed by sequential addition of 1 μg/ml Ang2 and 1 µg/ml TNF at a flow rate of 30 μl/min for 2 min.
ELISA to determine Ang2 neutralization activity
Ang2 (R&D Systems) at 0.1 μg/ml was coated onto a 96-well ELISA plates (Thermo Electron) at 4°C overnight. The plate was blocked with blocking buffer (Thermo Electron) at RT for 2 h. The soluble human Tie2-Fc (R&D Systems) at 0.5 μg/ml was added and incubated with plate bound Ang2 in the presence of various concentrations of serially diluted adalimumab or bispecific Zybodies at RT for 1 h. After washing, 100 µl of 0.5 µg/ml anti-Tie2 antibody (R&D) was added. After 1 h incubation at RT, plates were washed and 1:1000 dilution of goat anti-mouse HRP (eBioscience) added. The plates were further incubated for 1 h at RT. After the final wash step, TMB was added and absorbance was measured at 450 nm using a plate reader. Data were analyzed by Prism (GraphPad) using nonlinear regression analysis to calculate IC50 values.
Antibody binding to membrane TNF
293F cells were transiently transfected with full length human TNF pCEP4 plasmid using 293fectin tranfection reagents as suggested by the manufacturer (Invitrogen). After 24 h, the transfected cells were resuspended in complete medium (RPMI containing 10% FBS) at 4 x 106 cells/ml. The cells (50 μl cell suspension) were incubated with 50 μl of serially diluted adalimumab, ADA-a2H or TRA-a2H for 60 min at RT. Cells were washed three times and resuspended in 100 µl of Eu-labeled goat anti-human Ig (2 µg/ml) and incubated for 60 min at RT. After washing, the cells were resuspended in 100 µl complete medium. The cell suspensions (80 µl) were transferred to a 96 well plate containing 100 µl DELFIA enhancement solution. After a 15 min incubation at RT, plates were read using an Envision plate reader (Perkin Elmer).
L929 cytotoxicity assay
L929 cells were cultured in a 96 well plate at 3.5 x 104 cells/well in 100 µl of RPMI medium supplemented with 10% FBS overnight. The cells were then treated with 1 ng/ml TNF plus 1 μg/ml of Actinomycin D in the presence of various concentrations of adalimumab or bispecific Zybody for 24 h at 37°C. Cell viability was determined by adding 100 μl of Cell Titer-Glo reagent (Promega). After 15 min incubation at RT, luminescence was measured using an Envision plate reader. IC50 values were calculated by nonlinear regression analysis using Prism software.
FcγRIIIA binding assay
Binding of ADA-a2H and adalimumab to FcγRIIIA was determined by ELISA using biotin conjugated soluble FcγRIIIA. A 96-well plate was coated with various concentrations of adalimumab or ADA-a2H at 4°C overnight. The plate was blocked with ELISA blocking buffer at RT for 2 h. After washing the plate, 100 µl of biotin labeled FcγRIIIA (2 μg/ml) was added in absence or presence of 1 µg/ml Ang2 and incubated at RT for 1 h. Binding of FcγRIIIA-biotin to plate bound antibodies was determined by ELISA using HRP conjugated streptavidin.
C1q binding assay
Binding of ADA-a2H and adalimumab to human C1q (ProSpec-Tany Technogene, New Brunswick, NJ) was determined by ELISA. A 96-well plate was coated with various concentrations of adalimumab or ADA-a2H at 4°C overnight. The plate was blocked with ELISA blocking buffer at RT for 2 h. After washing the plate, 100 µl of human C1q (2 μg/ml) in absence or presence of 1 µg/ml Ang2 was added and incubated at RT for 1 h. Plates were washed and incubated with 100 µl of 1 µg/ml HRP conjugated sheep anti-human C1q antibody (AbD SerTec) for 1 h at RT. After washing, the binding of C1q to plate bound antibodies was determined by ELISA.
TNFRI and TNFRII binding assays
TNFRI and TNRII were coated (0.5 µg/ml) onto a 96-well plate overnight at 4°C. The plate was blocked with blocking buffer at RT for 2 h. After washing, biotinylated TNF (0.1 µg/ml) was added and incubated with various concentrations of ADA-a2H or adalimumab for 1 h at RT. TNF-biotin binding to plate bound TNF receptors was determined by ELISA using streptavidin-HRP.
Western blot analysis
HUVEC cells were plated in a 6-well plate at 0.8 x 106/well in 1 ml of EGMTM growth medium (Lonza). After 24 h, cells were starved in serum free medium overnight. The cells were then stimulated with 10 ng/ml TNF or 2 μg/ml Ang2 or the combination of both at 37°C for 40 min. Cell lysates were prepared after a wash with 1.5 ml ice cold PBS and subsequent lysis of the cells in 100 μl of cell lysis buffer containing 1% Triton-X 100 in 20 mM TRIS-HCl, pH7.5, 150 mM NaCl, 1 mM sodium vanadate, 1 mM EDTA and a protease inhibitor cocktail (Sigma-Aldrich). After centrifugation at 14000 rpm for 10 min at 4°C, the cell lysates were resolved on 4–12% SDS-PAGE gels (Invitrogen) and transferred to PVDF membranes (Invitrogen). The membranes were immunoblotted with antibodies specific to phospho-Akt (Cell Signaling, Danvers, MA) or IκB-α (Cell Signaling) and detected with horseradish peroxidase-conjugated secondary antibodies and enhanced chemiluminescence (Invitrogen). Membranes were also blotted with antibody against total Akt to determine equal loading of proteins.
Tg197 transgenic model of rheumatoid arthritis
Tg197 human TNF transgenic mice were used to the test efficacy of various anti-TNF antibodies as described.65,81 Animals were housed and maintained by Biomedcode at the facilities of the animal house unit of the Biomedical Sciences Research Center “Alexander Fleming” (Biomedcode, Greece). Animal protocols were approved by the BSRC “Alexander Fleming” Institutional Animal Care and Use Committee. Tg197 mice, homozygous or heterozygous for the human TNF-globin hybrid transgene (maintained in a CBAxC57BL/6 genetic background) were crossed with CBAxC57BL/6 F1 females. Their heterozygous offspring were identified by tail DNA genotyping. Mice (n = 8 per group, gender and age matched) were injected intraperitoneally with different doses (10 μl/g body weight) of adalimumab or Zybodies twice weekly. The treatments were started at the third week of age before the establishment of overt signs of arthritis. The effect of the test materials was monitored by weekly assessment of body weight measurements and clinical symptoms. The arthritic symptoms were evaluated macroscopically on both ankle joints based on the following scoring scales: 0.0-no arthritis, (normal appearance, mouse can support upside its weight, whole body flexibility/evasiveness normal, grip strength maximum), 0.5-onset of arthritis (mild joint swelling above paw), 1.0-mild arthritis (joint distortion by swelling, paw inflamed), 1.5-mild to moderate arthritis (joint-paw swelling, distortion + last finger inward deformation, brief support upside its weight borderline yes/no, whole body flexibility reduced, less grip strength), 2.0-moderate arthritis (severe joint, paw and finger swelling, joint–leg deformation, no support upside its weight falls off, no whole body flexibility, no grip strength, climbing/feeding affected), 2.5-moderate to heavy arthritis (as above 2 + finger deformation in paws, mouse movement impaired), 3.0-heavy arthritis (ankylosis detected on flexion and severely impaired movement, mouse moribund). Ankle joints were collected and paraffin blocks prepared. Ankle joint sections were stained with hematoxylin/eosin and a series of sections were prepared to microscopically evaluate the histopathological arthritic scores.
Statistical analysis
The results are reported as the mean ± SEM for arthritic and histological scores. Mann-Whitney (2-tail, 95%) was used to determine statistical significance between control and the Zybody treated groups and p < 0.05 was considered as statistically significant.
Supplementary Material
Disclosure of Potential Conflicts of Interest
The authors are employees of Zyngenia, Inc. and have equity interest in the company.
Supplemental Material
Supplemental material may be downloaded here:
http://www.landesbioscience.com/journals/mabs/article/21277/
Glossary
Abbreviations:
- Ang2
angiopoietin 2
- COPD
chronic obstructive pulmonary disease
- HUVEC
human umbilical vein endothelial cells
- IκB
inhibitor of κB
- RA
rheumatoid arthritis
- SPR
surface plasmon resonance
- TNF
tumor necrosis factor-α
- VEGF
vascular endothelial cell growth factor
Footnotes
Previously published online: www.landesbioscience.com/journals/mabs/article/21227
References
- 1.Chan AC, Carter PJ. Therapeutic antibodies for autoimmunity and inflammation. Nat Rev Immunol. 2010;10:301–16. doi: 10.1038/nri2761. [DOI] [PubMed] [Google Scholar]
- 2.Karampetsou MP, Liossis SN, Sfikakis PP. TNF-α antagonists beyond approved indications: stories of success and prospects for the future. QJM. 2010;103:917–28. doi: 10.1093/qjmed/hcq152. [DOI] [PubMed] [Google Scholar]
- 3.Rigby WF. Drug insight: different mechanisms of action of tumor necrosis factor antagonists-passive-aggressive behavior? Nat Clin Pract Rheumatol. 2007;3:227–33. doi: 10.1038/ncprheum0438. [DOI] [PubMed] [Google Scholar]
- 4.Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther. 2008;117:244–79. doi: 10.1016/j.pharmthera.2007.10.001. [DOI] [PubMed] [Google Scholar]
- 5.Scheinfeld N. A comprehensive review and evaluation of the side effects of the tumor necrosis factor alpha blockers etanercept, infliximab and adalimumab. J Dermatolog Treat. 2004;15:280–94. doi: 10.1080/09546630410017275. [DOI] [PubMed] [Google Scholar]
- 6.van Vollenhoven RF. Treatment of rheumatoid arthritis: state of the art 2009. Nat Rev Rheumatol. 2009;5:531–41. doi: 10.1038/nrrheum.2009.182. [DOI] [PubMed] [Google Scholar]
- 7.Zwerina J, Hayer S, Tohidast-Akrad M, Bergmeister H, Redlich K, Feige U, et al. Single and combined inhibition of tumor necrosis factor, interleukin-1, and RANKL pathways in tumor necrosis factor-induced arthritis: effects on synovial inflammation, bone erosion, and cartilage destruction. Arthritis Rheum. 2004;50:277–90. doi: 10.1002/art.11487. [DOI] [PubMed] [Google Scholar]
- 8.Genovese MC, Cohen S, Moreland L, Lium D, Robbins S, Newmark R, et al. 20000223 Study Group Combination therapy with etanercept and anakinra in the treatment of patients with rheumatoid arthritis who have been treated unsuccessfully with methotrexate. Arthritis Rheum. 2004;50:1412–9. doi: 10.1002/art.20221. [DOI] [PubMed] [Google Scholar]
- 9.Weinblatt M, Schiff M, Goldman A, Kremer J, Luggen M, Li T, et al. Selective costimulation modulation using abatacept in patients with active rheumatoid arthritis while receiving etanercept: a randomised clinical trial. Ann Rheum Dis. 2007;66:228–34. doi: 10.1136/ard.2006.055111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–42. doi: 10.1056/NEJMoa032691. [DOI] [PubMed] [Google Scholar]
- 11.Demetri GD, van Oosterom AT, Garrett CR, Blackstein ME, Shah MH, Verweij J, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368:1329–38. doi: 10.1016/S0140-6736(06)69446-4. [DOI] [PubMed] [Google Scholar]
- 12.Motzer RJ, Rini BI, Bukowski RM, Curti BD, George DJ, Hudes GR, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516–24. doi: 10.1001/jama.295.21.2516. [DOI] [PubMed] [Google Scholar]
- 13.Dixon JA, Oliver SC, Olson JL, Mandava N. VEGF Trap-Eye for the treatment of neovascular age-related macular degeneration. Expert Opin Investig Drugs. 2009;18:1573–80. doi: 10.1517/13543780903201684. [DOI] [PubMed] [Google Scholar]
- 14.Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. SHARP Investigators Study Group Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–90. doi: 10.1056/NEJMoa0708857. [DOI] [PubMed] [Google Scholar]
- 15.Brown JL, Cao ZA, Pinzon-Ortiz M, Kendrew J, Reimer C, Wen S, et al. A human monoclonal anti-ANG2 antibody leads to broad antitumor activity in combination with VEGF inhibitors and chemotherapy agents in preclinical models. Mol Cancer Ther. 2010;9:145–56. doi: 10.1158/1535-7163.MCT-09-0554. [DOI] [PubMed] [Google Scholar]
- 16.Hashizume H, Falcón BL, Kuroda T, Baluk P, Coxon A, Yu D, et al. Complementary actions of inhibitors of angiopoietin-2 and VEGF on tumor angiogenesis and growth. Cancer Res. 2010;70:2213–23. doi: 10.1158/0008-5472.CAN-09-1977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Huang H, Lai JY, Do J, Liu D, Li L, Del Rosario J, et al. Specifically targeting angiopoietin-2 inhibits angiogenesis, Tie2-expressing monocyte infiltration, and tumor growth. Clin Cancer Res. 2011;17:1001–11. doi: 10.1158/1078-0432.CCR-10-2317. [DOI] [PubMed] [Google Scholar]
- 18.Oliner J, Min H, Leal J, Yu D, Rao S, You E, et al. Suppression of angiogenesis and tumor growth by selective inhibition of angiopoietin-2. Cancer Cell. 2004;6:507–16. doi: 10.1016/j.ccr.2004.09.030. [DOI] [PubMed] [Google Scholar]
- 19.Herbst RS, Hong D, Chap L, Kurzrock R, Jackson E, Silverman JM, et al. Safety, pharmacokinetics, and antitumor activity of AMG 386, a selective angiopoietin inhibitor, in adult patients with advanced solid tumors. J Clin Oncol. 2009;27:3557–65. doi: 10.1200/JCO.2008.19.6683. [DOI] [PubMed] [Google Scholar]
- 20.Karlan BY, Oza AM, Richardson GE, Provencher DM, Hansen VL, Buck M, et al. Randomized, Double-Blind, Placebo-Controlled Phase II Study of AMG 386 Combined With Weekly Paclitaxel in Patients With Recurrent Ovarian Cancer. J Clin Oncol. 2011 doi: 10.1200/JCO.2010.34.3178. [DOI] [PubMed] [Google Scholar]
- 21.Gale NW, Yancopoulos GD. Growth factors acting via endothelial cell-specific receptor tyrosine kinases: VEGFs, angiopoietins, and ephrins in vascular development. Genes Dev. 1999;13:1055–66. doi: 10.1101/gad.13.9.1055. [DOI] [PubMed] [Google Scholar]
- 22.Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. 1997;277:55–60. doi: 10.1126/science.277.5322.55. [DOI] [PubMed] [Google Scholar]
- 23.Davis S, Aldrich TH, Jones PF, Acheson A, Compton DL, Jain V, et al. Isolation of angiopoietin-1, a ligand for the TIE2 receptor, by secretion-trap expression cloning. Cell. 1996;87:1161–9. doi: 10.1016/S0092-8674(00)81812-7. [DOI] [PubMed] [Google Scholar]
- 24.Suri C, Jones PF, Patan S, Bartunkova S, Maisonpierre PC, Davis S, et al. Requisite role of angiopoietin-1, a ligand for the TIE2 receptor, during embryonic angiogenesis. Cell. 1996;87:1171–80. doi: 10.1016/S0092-8674(00)81813-9. [DOI] [PubMed] [Google Scholar]
- 25.Huang J, Bae JO, Tsai JP, Kadenhe-Chiweshe A, Papa J, Lee A, et al. Angiopoietin-1/Tie-2 activation contributes to vascular survival and tumor growth during VEGF blockade. Int J Oncol. 2009;34:79–87. [PMC free article] [PubMed] [Google Scholar]
- 26.Davis S, Papadopoulos N, Aldrich TH, Maisonpierre PC, Huang T, Kovac L, et al. Angiopoietins have distinct modular domains essential for receptor binding, dimerization and superclustering. Nat Struct Biol. 2003;10:38–44. doi: 10.1038/nsb880. [DOI] [PubMed] [Google Scholar]
- 27.Kim I, Kim JH, Moon SO, Kwak HJ, Kim NG, Koh GY. Angiopoietin-2 at high concentration can enhance endothelial cell survival through the phosphatidylinositol 3′-kinase/Akt signal transduction pathway. Oncogene. 2000;19:4549–52. doi: 10.1038/sj.onc.1203800. [DOI] [PubMed] [Google Scholar]
- 28.Teichert-Kuliszewska K, Maisonpierre PC, Jones N, Campbell AI, Master Z, Bendeck MP, et al. Biological action of angiopoietin-2 in a fibrin matrix model of angiogenesis is associated with activation of Tie2. Cardiovasc Res. 2001;49:659–70. doi: 10.1016/S0008-6363(00)00231-5. [DOI] [PubMed] [Google Scholar]
- 29.Asahara T, Chen D, Takahashi T, Fujikawa K, Kearney M, Magner M, et al. Tie2 receptor ligands, angiopoietin-1 and angiopoietin-2, modulate VEGF-induced postnatal neovascularization. Circ Res. 1998;83:233–40. doi: 10.1161/01.RES.83.3.233. [DOI] [PubMed] [Google Scholar]
- 30.Fiedler U, Augustin HG. Angiopoietins: a link between angiogenesis and inflammation. Trends Immunol. 2006;27:552–8. doi: 10.1016/j.it.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 31.Koutroubakis IE, Tsiolakidou G, Karmiris K, Kouroumalis EA. Role of angiogenesis in inflammatory bowel disease. Inflamm Bowel Dis. 2006;12:515–23. doi: 10.1097/00054725-200606000-00012. [DOI] [PubMed] [Google Scholar]
- 32.Costa C, Incio J, Soares R. Angiogenesis and chronic inflammation: cause or consequence? Angiogenesis. 2007;10:149–66. doi: 10.1007/s10456-007-9074-0. [DOI] [PubMed] [Google Scholar]
- 33.Jackson JR, Seed MP, Kircher CH, Willoughby DA, Winkler JD. The codependence of angiogenesis and chronic inflammation. FASEB J. 1997;11:457–65. [PubMed] [Google Scholar]
- 34.Kim H, Koh GY. Ang2, the instigator of inflammation. Blood. 2011;118:4767–8. doi: 10.1182/blood-2011-09-377333. [DOI] [PubMed] [Google Scholar]
- 35.Sone H, Kawakami Y, Sakauchi M, Nakamura Y, Takahashi A, Shimano H, et al. Neutralization of vascular endothelial growth factor prevents collagen-induced arthritis and ameliorates established disease in mice. Biochem Biophys Res Commun. 2001;281:562–8. doi: 10.1006/bbrc.2001.4395. [DOI] [PubMed] [Google Scholar]
- 36.Tolstanova G, Khomenko T, Deng X, Chen L, Tarnawski A, Ahluwalia A, et al. Neutralizing anti-vascular endothelial growth factor (VEGF) antibody reduces severity of experimental ulcerative colitis in rats: direct evidence for the pathogenic role of VEGF. J Pharmacol Exp Ther. 2009;328:749–57. doi: 10.1124/jpet.108.145128. [DOI] [PubMed] [Google Scholar]
- 37.Jung K, Lee D, Lim HS, Lee SI, Kim YJ, Lee GM, et al. Double anti-angiogenic and anti-inflammatory protein Valpha targeting VEGF-A and TNF-alpha in retinopathy and psoriasis. J Biol Chem. 2011;286:14410–8. doi: 10.1074/jbc.M111.228130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gamble JR, Drew J, Trezise L, Underwood A, Parsons M, Kasminkas L, et al. Angiopoietin-1 is an antipermeability and anti-inflammatory agent in vitro and targets cell junctions. Circ Res. 2000;87:603–7. doi: 10.1161/01.RES.87.7.603. [DOI] [PubMed] [Google Scholar]
- 39.McCarter SD, Mei SH, Lai PF, Zhang QW, Parker CH, Suen RS, et al. Cell-based angiopoietin-1 gene therapy for acute lung injury. Am J Respir Crit Care Med. 2007;175:1014–26. doi: 10.1164/rccm.200609-1370OC. [DOI] [PubMed] [Google Scholar]
- 40.Mei SH, McCarter SD, Deng Y, Parker CH, Liles WC, Stewart DJ. Prevention of LPS-induced acute lung injury in mice by mesenchymal stem cells overexpressing angiopoietin 1. PLoS Med. 2007;4:e269. doi: 10.1371/journal.pmed.0040269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pizurki L, Zhou Z, Glynos K, Roussos C, Papapetropoulos A. Angiopoietin-1 inhibits endothelial permeability, neutrophil adherence and IL-8 production. Br J Pharmacol. 2003;139:329–36. doi: 10.1038/sj.bjp.0705259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Scholz A, Lang V, Henschler R, Czabanka M, Vajkoczy P, Chavakis E, et al. Angiopoietin-2 promotes myeloid cell infiltration in a β₂-integrin-dependent manner. Blood. 2011;118:5050–9. doi: 10.1182/blood-2011-03-343293. [DOI] [PubMed] [Google Scholar]
- 43.Fiedler U, Scharpfenecker M, Koidl S, Hegen A, Grunow V, Schmidt JM, et al. The Tie-2 ligand angiopoietin-2 is stored in and rapidly released upon stimulation from endothelial cell Weibel-Palade bodies. Blood. 2004;103:4150–6. doi: 10.1182/blood-2003-10-3685. [DOI] [PubMed] [Google Scholar]
- 44.Fiedler U, Reiss Y, Scharpfenecker M, Grunow V, Koidl S, Thurston G, et al. Angiopoietin-2 sensitizes endothelial cells to TNF-alpha and has a crucial role in the induction of inflammation. Nat Med. 2006;12:235–9. doi: 10.1038/nm1351. [DOI] [PubMed] [Google Scholar]
- 45.Roviezzo F, Tsigkos S, Kotanidou A, Bucci M, Brancaleone V, Cirino G, et al. Angiopoietin-2 causes inflammation in vivo by promoting vascular leakage. J Pharmacol Exp Ther. 2005;314:738–44. doi: 10.1124/jpet.105.086553. [DOI] [PubMed] [Google Scholar]
- 46.Ganta VC, Cromer W, Mills GL, Traylor J, Jennings M, Daley S, et al. Angiopoietin-2 in experimental colitis. Inflamm Bowel Dis. 2010;16:1029–39. doi: 10.1002/ibd.21150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kümpers P, David S, Haubitz M, Hellpap J, Horn R, Bröcker V, et al. The Tie2 receptor antagonist angiopoietin 2 facilitates vascular inflammation in systemic lupus erythematosus. Ann Rheum Dis. 2009;68:1638–43. doi: 10.1136/ard.2008.094664. [DOI] [PubMed] [Google Scholar]
- 48.Giuliano JS, Jr., Wheeler DS. Excess circulating angiopoietin-2 levels in sepsis: harbinger of death in the intensive care unit? Crit Care. 2009;13:114. doi: 10.1186/cc7685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kümpers P, van Meurs M, David S, Molema G, Bijzet J, Lukasz A, et al. Time course of angiopoietin-2 release during experimental human endotoxemia and sepsis. Crit Care. 2009;13:R64. doi: 10.1186/cc7866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Michalska-Jakubus M, Kowal-Bielecka O, Chodorowska G, Bielecki M, Krasowska D. Angiopoietins-1 and -2 are differentially expressed in the sera of patients with systemic sclerosis: high angiopoietin-2 levels are associated with greater severity and higher activity of the disease. Rheumatology (Oxford) 2011;50:746–55. doi: 10.1093/rheumatology/keq392. [DOI] [PubMed] [Google Scholar]
- 51.Cho YJ, Ma JE, Yun EY, Kim YE, Kim HC, Lee JD, et al. Serum angiopoietin-2 levels are elevated during acute exacerbations of COPD. Respirology. 2011;16:284–90. doi: 10.1111/j.1440-1843.2010.01915.x. [DOI] [PubMed] [Google Scholar]
- 52.Kuroda K, Sapadin A, Shoji T, Fleischmajer R, Lebwohl M. Altered expression of angiopoietins and Tie2 endothelium receptor in psoriasis. J Invest Dermatol. 2001;116:713–20. doi: 10.1046/j.1523-1747.2001.01316.x. [DOI] [PubMed] [Google Scholar]
- 53.Fearon U, Griosios K, Fraser A, Reece R, Emery P, Jones PF, et al. Angiopoietins, growth factors, and vascular morphology in early arthritis. J Rheumatol. 2003;30:260–8. [PubMed] [Google Scholar]
- 54.Westra J, de Groot L, Plaxton SL, Brouwer E, Posthumus MD, Kallenberg CG, et al. Angiopoietin-2 is highly correlated with inflammation and disease activity in recent-onset rheumatoid arthritis and could be predictive for cardiovascular disease. Rheumatology (Oxford) 2011;50:665–73. doi: 10.1093/rheumatology/keq378. [DOI] [PubMed] [Google Scholar]
- 55.Kamba T, McDonald DM. Mechanisms of adverse effects of anti-VEGF therapy for cancer. Br J Cancer. 2007;96:1788–95. doi: 10.1038/sj.bjc.6603813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Chen HX, Cleck JN. Adverse effects of anticancer agents that target the VEGF pathway. Nat Rev Clin Oncol. 2009;6:465–77. doi: 10.1038/nrclinonc.2009.94. [DOI] [PubMed] [Google Scholar]
- 57.Miller BR, Demarest SJ, Lugovskoy A, Huang F, Wu X, Snyder WB, et al. Stability engineering of scFvs for the development of bispecific and multivalent antibodies. Protein Eng Des Sel. 2010;23:549–57. doi: 10.1093/protein/gzq028. [DOI] [PubMed] [Google Scholar]
- 58.Marvin JS, Zhu Z. Recombinant approaches to IgG-like bispecific antibodies. Acta Pharmacol Sin. 2005;26:649–58. doi: 10.1111/j.1745-7254.2005.00119.x. [DOI] [PubMed] [Google Scholar]
- 59.Makó V, Czúcz J, Weiszhár Z, Herczenik E, Matkó J, Prohászka Z, et al. Proinflammatory activation pattern of human umbilical vein endothelial cells induced by IL-1β, TNF-α, and LPS. Cytometry A. 2010;77:962–70. doi: 10.1002/cyto.a.20952. [DOI] [PubMed] [Google Scholar]
- 60.Kaymakcalan Z, Sakorafas P, Bose S, Scesney S, Xiong L, Hanzatian DK, et al. Comparisons of affinities, avidities, and complement activation of adalimumab, infliximab, and etanercept in binding to soluble and membrane tumor necrosis factor. Clin Immunol. 2009;131:308–16. doi: 10.1016/j.clim.2009.01.002. [DOI] [PubMed] [Google Scholar]
- 61.Mitoma H, Horiuchi T, Tsukamoto H, Tamimoto Y, Kimoto Y, Uchino A, et al. Mechanisms for cytotoxic effects of anti-tumor necrosis factor agents on transmembrane tumor necrosis factor alpha-expressing cells: comparison among infliximab, etanercept, and adalimumab. Arthritis Rheum. 2008;58:1248–57. doi: 10.1002/art.23447. [DOI] [PubMed] [Google Scholar]
- 62.Nesbitt A, Fossati G, Bergin M, Stephens P, Stephens S, Foulkes R, et al. Mechanism of action of certolizumab pegol (CDP870): in vitro comparison with other anti-tumor necrosis factor alpha agents. Inflamm Bowel Dis. 2007;13:1323–32. doi: 10.1002/ibd.20225. [DOI] [PubMed] [Google Scholar]
- 63.Scallon BJ, Moore MA, Trinh H, Knight DM, Ghrayeb J. Chimeric anti-TNF-alpha monoclonal antibody cA2 binds recombinant transmembrane TNF-alpha and activates immune effector functions. Cytokine. 1995;7:251–9. doi: 10.1006/cyto.1995.0029. [DOI] [PubMed] [Google Scholar]
- 64.Koch AE. Angiogenesis as a target in rheumatoid arthritis. Ann Rheum Dis. 2003;62(Suppl 2):ii60–7. doi: 10.1136/ard.62.suppl_2.ii60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Keffer J, Probert L, Cazlaris H, Georgopoulos S, Kaslaris E, Kioussis D, et al. Transgenic mice expressing human tumour necrosis factor: a predictive genetic model of arthritis. EMBO J. 1991;10:4025–31. doi: 10.1002/j.1460-2075.1991.tb04978.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Douni E, Sfikakis PP, Haralambous S, Fernandes P, Kollias G. Attenuation of inflammatory polyarthritis in TNF transgenic mice by diacerein: comparative analysis with dexamethasone, methotrexate and anti-TNF protocols. Arthritis Res Ther. 2004;6:R65–72. doi: 10.1186/ar1028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Dong J, Sereno A, Aivazian D, Langley E, Miller BR, Snyder WB, et al. A stable IgG-like bispecific antibody targeting the epidermal growth factor receptor and the type I insulin-like growth factor receptor demonstrates superior anti-tumor activity. MAbs. 2011;3:273–88. doi: 10.4161/mabs.3.3.15188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Doppalapudi VR, Huang J, Liu D, Jin P, Liu B, Li L, et al. Chemical generation of bispecific antibodies. Proc Natl Acad Sci U S A. 2010;107:22611–6. doi: 10.1073/pnas.1016478108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Demarest SJ, Hariharan K, Dong J. Emerging antibody combinations in oncology. MAbs. 2011;3:338–51. doi: 10.4161/mabs.3.4.16615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Thakur A, Lum LG. Cancer therapy with bispecific antibodies: Clinical experience. Curr Opin Mol Ther. 2010;12:340–9. [PMC free article] [PubMed] [Google Scholar]
- 71.Fischer N, Léger O. Bispecific antibodies: molecules that enable novel therapeutic strategies. Pathobiology. 2007;74:3–14. doi: 10.1159/000101046. [DOI] [PubMed] [Google Scholar]
- 72.Hagemeyer CE, von Zur Muhlen C, von Elverfeldt D, Peter K. Single-chain antibodies as diagnostic tools and therapeutic agents. Thromb Haemost. 2009;101:1012–9. [PubMed] [Google Scholar]
- 73.Song MY, Park SK, Kim CS, Yoo TH, Kim B, Kim MS, et al. Characterization of a novel anti-human TNF-alpha murine monoclonal antibody with high binding affinity and neutralizing activity. Exp Mol Med. 2008;40:35–42. doi: 10.3858/emm.2008.40.1.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Horiuchi T, Mitoma H, Harashima S, Tsukamoto H, Shimoda T. Transmembrane TNF-alpha: structure, function and interaction with anti-TNF agents. Rheumatology (Oxford) 2010;49:1215–28. doi: 10.1093/rheumatology/keq031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Chen JX, Chen Y, DeBusk L, Lin W, Lin PC. Dual functional roles of Tie-2/angiopoietin in TNF-alpha-mediated angiogenesis. Am J Physiol Heart Circ Physiol. 2004;287:H187–95. doi: 10.1152/ajpheart.01058.2003. [DOI] [PubMed] [Google Scholar]
- 76.Yoshida S, Ono M, Shono T, Izumi H, Ishibashi T, Suzuki H, et al. Involvement of interleukin-8, vascular endothelial growth factor, and basic fibroblast growth factor in tumor necrosis factor alpha-dependent angiogenesis. Mol Cell Biol. 1997;17:4015–23. doi: 10.1128/mcb.17.7.4015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Leibovich SJ, Polverini PJ, Shepard HM, Wiseman DM, Shively V, Nuseir N. Macrophage-induced angiogenesis is mediated by tumour necrosis factor-alpha. Nature. 1987;329:630–2. doi: 10.1038/329630a0. [DOI] [PubMed] [Google Scholar]
- 78.Kanakaraj P, Ngo K, Wu Y, Angulo A, Ghazal P, Harris CA, et al. Defective interleukin (IL)-18-mediated natural killer and T helper cell type 1 responses in IL-1 receptor-associated kinase (IRAK)-deficient mice. J Exp Med. 1999;189:1129–38. doi: 10.1084/jem.189.7.1129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Mita AC, Takimoto CH, Mita M, Tolcher A, Sankhala K, Sarantopoulos J, et al. Phase 1 study of AMG 386, a selective angiopoietin 1/2-neutralizing peptibody, in combination with chemotherapy in adults with advanced solid tumors. Clin Cancer Res. 2010;16:3044–56. doi: 10.1158/1078-0432.CCR-09-3368. [DOI] [PubMed] [Google Scholar]
- 80.Robson EJ, Ghatage P. AMG 386: profile of a novel angiopoietin antagonist in patients with ovarian cancer. Expert Opin Investig Drugs. 2011;20:297–304. doi: 10.1517/13543784.2011.549125. [DOI] [PubMed] [Google Scholar]
- 81.Shealy DJ, Wooley PH, Emmell E, Volk A, Rosenberg A, Treacy G, et al. Anti-TNF-alpha antibody allows healing of joint damage in polyarthritic transgenic mice. Arthritis Res. 2002;4:R7. doi: 10.1186/ar430. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.