

Abstract
Objectives:
(1) To attain a quantitative estimate of patient satisfaction with physiotherapy care for musculoskeletal conditions in Australia; (2) to compare the observed level of patient satisfaction with care in Australia with those from other countries; and (3) to compare factors contributing to patient satisfaction between Australia and the United States (US).
Methods:
We conducted a prospective study of 274 patients presenting for physiotherapy treatment of a musculoskeletal disorder in Australian clinics. Patient satisfaction was measured using the 20-item MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care (MRPS) and satisfaction scores were compared with those from Northern Europe, North America, the United Kingdom, and Ireland. To investigate factors contributing to patient satisfaction between Australia and the US, we compared 20-item MRPS data from Australian and Spanish-speaking US cohorts.
Results:
Mean Australian MRPS satisfaction score was 4.55 (95% confidence interval: 4.51–4.59) on a scale of 1 to 5, where 1 indicates high dissatisfaction and 5 indicates high satisfaction. This high level of patient satisfaction is consistent with international data. Australian respondents specifically valued interpersonal aspects of care, including advice and information about their condition and an explanation about self-management. The correlation between treatment outcomes and global patient satisfaction was low (r = −0.22). A comparison of data collected from Australia and the US showed that MRPS items regarding interpersonal aspects of care, such as the therapists’ communication skills, correlated strongly with global satisfaction in both countries. However, there were other questionnaire items for which the correlation with global satisfaction was significantly different between Australia and the US.
Conclusions:
Patient satisfaction with musculoskeletal physiotherapy care in Australia is high and comparable with Northern Europe, North America, the United Kingdom and Ireland. Comparison of data between Australia and the US indicates that while some determinants of patient satisfaction are common, country-specific differences also exist.
Keywords: Patient satisfaction, Physiotherapy, Physical therapy, Musculoskeletal, Australia, United States
Introduction
As health care provision has become more patient-centred, patient satisfaction has emerged as a critical outcome of care.1,2 Patients’ views about their health care are intrinsically important to clinicians,3 and are one of the three key elements of evidence-based physiotherapy practice.4 Evaluation of patient satisfaction with physiotherapy care provides specific and objective feedback to clinicians about the services they provide. Physiotherapists can use this evidence to optimize the quality and outcomes of patient care. There is evidence that patients who are satisfied with the delivery of their health care are more compliant with treatment and attain a higher health-related quality of life.5–7 Patient satisfaction data can also be valuable for quality assurance and accreditation of health care clinics.8
Physiotherapists are leading providers of care for patients with musculoskeletal conditions such as back or neck pain, osteoarthritis, and sporting injuries. Patient satisfaction with musculoskeletal physiotherapy care has been investigated in many countries, as synthesized in a recent systematic review.9 However, there has been no previous quantitative evaluation of patient satisfaction with physiotherapy services for adults in Australia. The level and determinants of patient satisfaction with musculoskeletal physiotherapy care in Australia are therefore currently unknown. Therefore, the primary aims of this study were: to attain a quantitative estimate of patient satisfaction with physiotherapy care for musculoskeletal conditions in Australia; and to compare the observed level of patient satisfaction with care in Australia with those from other countries. A secondary aim was to compare factors contributing to patient satisfaction between Australia and the United States (US), using data collected in both countries with the same patient satisfaction instrument, the MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care.
Methods
Design
We conducted a prospective study of patients attending physiotherapy clinics in Australia for treatment of a musculoskeletal condition. Data were collected between September 2008 and November 2009.
Participants and clinics
Patients were eligible to be invited into the study if they presented for treatment of a musculoskeletal disorder, were aged 18 years and over, could read English and were able to complete the study questionnaire. Patients were recruited from seven physiotherapy clinics in two states of Australia: four from New South Wales (NSW) and three from Western Australia (WA). The NSW clinics were sampled to represent the majority of the state’s area health services: one rural area health service (Greater Southern) and three Sydney metropolitan area health services (Northern Sydney, South Eastern Sydney, Sydney South West). The three WA clinics were all located in the North Metropolitan Area Health Service in Perth and were a convenience sample.
Patient satisfaction instrument
Patient satisfaction with care was measured using an established instrument with acceptable clinimetric properties: the MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care (MRPS).10–12 We used the largest version (20-item) to maximize capture of culturally relevant factors. The questionnaire contains 18 items about specific aspects of physiotherapy care and two items about overall satisfaction. Each item is scored on a scale of 1 (strongly disagree) to 5 (strongly agree). The mean score of items 1 to 18 provides a measure of patient satisfaction, where 1 indicates high dissatisfaction and 5 indicates high satisfaction. The MRPS has been validated for use in outpatient physiotherapy populations.10–12 While shorter versions of the MRPS have been developed, we chose to use the 20-item instrument to thoroughly explore multiple domains of patient satisfaction in this cultural context. The instrument is reliable, easy to administer and can discriminate between different factors influencing patient satisfaction.11,12
In order to explore the relationship between patient satisfaction and the improvement in their condition with treatment, a single item measure of global rating of change in the patients’ condition was also used, consisting of the following question: How does your current condition compare to how it was before you started physiotherapy treatment? The response is measured on a 9-point Likert scale, where 1 indicates very much better and 9 very much worse.
Procedure
Consecutive patients were given a patient information sheet about the study when presenting for a new course of treatment and were invited to participate in the study. On completion of treatment (or after six sessions, whichever came first), each participant was invited by office staff to voluntarily complete the MRPS questionnaire in the waiting room of the clinic. After filling out the questionnaire, participants placed it in a sealed envelope and returned it for collection to the receptionist, prior to collection by a study researcher. Patients’ names were not recorded on the questionnaire or envelope, to ensure anonymity. Recruitment ceased when at least 30 patients in each clinic had completed the questionnaire. This study was approved by the University of Sydney Human Research Ethics Committee (approval no.10929).
Data analysis
Description of the sample and patient satisfaction in Australia
Quantitative variables including satisfaction score, age, and travel time, were described as means and standard deviations (SD) and qualitative variables such as sex and body area treated were described as percentages. Satisfaction scores for individual questionnaire items were calculated as means and standard deviations for all respondents. Assumptions of normality were confirmed for continuous variables. The level of overall patient satisfaction was calculated as the mean and 95% confidence interval (CI) of items 1 to 18 for all clinics.
Comparison of patient satisfaction scores in Australia with international data
We compared Australian satisfaction levels with mean satisfaction scores from other countries we have previously published in a systematic review.9 Because we did not have access to raw data from countries other than Australia, it was not possible to use inferential statistics to investigate the significance of differences between mean satisfaction scores for each country. Therefore, we calculated the 95% CIs of the mean for each country and identified significant differences where 95% CIs did not overlap.
Comparison of factors contributing to patient satisfaction in Australia and the US
To compare factors contributing to patient satisfaction with musculoskeletal physiotherapy care between two countries, we compared the means and 95%CIs of each MRPS item from the Australia cohort with those published from a US study12 that used the same 20-item MRPS instrument. The US data were collected from 203 Spanish-speaking patients in New York City, using a Spanish-language version of the 20-item MRPS, which has an identical factor-structure to the English-language version.12 Ninety-five per cent CIs were calculated for the mean of each item and significant differences were identified where 95% CIs did not overlap. We also conducted a bivariate correlation analysis of the relationship between individual items to the global satisfaction item (MRPS item 19). Significant differences between the US and Australia were identified for items where the 95% CIs of the Pearson r values did not overlap.
Statistical analyses
Criterion-referenced validity was investigated by exploring the Pearson correlation coefficient r between individual item scores (items 1 to 18) and the global measure of satisfaction (item 19) in bivariate correlation analyses. One-way ANOVA analyses were performed to explore statistical differences between questionnaire items, clinics and demographic variables. The level of statistical significance was set at P<0.05, or no overlap of 95% CIs.
SPSS version 17.0 (SPSS, Chicago, IL, USA) was used for all data analysis.
Results
Description of the sample
Patient satisfaction data were collected from 274 participants in seven clinics in two states of Australia (New South Wales and Western Australia), representing five different area health regions, both urban and rural (Table 1). Physiotherapists in all clinics had similar university entry-level physiotherapy qualifications from Australia. Caseloads per physical therapist in each clinic were comparable, typically two patients per hour. Of the respondents to the satisfaction questionnaire, 57% were female and mean (SD) age was 40 (13) (Table 1). Two of the seven clinics that predominantly treated sporting injuries (AUS02, AUS03) had significantly younger patient samples [mean (SD): 34 (11); 34 (14) respectively] than the remainder of the clinical sites (Table 1). Participants were treated for conditions of the low back (20%), neck (15%), leg (12%), foot and ankle (9%), upper limb (4%), multiple diagnoses (28%) or other areas (13%).
Table 1. Description of study participants and clinics [mean (SD)].
| Clinic code | State (Area Health Service) | n | Age | Gender % F | Patient satisfaction* | Global rating of change† | SES score‡ |
| AUS01 | NSW (Sydney South West) | 37 | 41 (12), range: 20–70 | 65 | 4.52 (0.36) | 2.25 (0.98) | 1124 |
| AUS02 | NSW (Northern Sydney) | 40 | 34 (11), range: 17–55 | 62 | 4.57 (0.35) | 1.85 (0.93) | 1183 |
| AUS03 | NSW (South Eastern Sydney) | 41 | 34 (14), range: 17–69 | 62 | 4.57 (0.34) | 1.85 (0.78) | 1111 |
| AUS04 | NSW (Greater Southern, rural) | 32 | 41 (16), range: 17–87 | 37 | 4.55 (0.42) | 2.43 (1.59) | 944 |
| AUS05 | WA (North Metropolitan) | 41 | 42 (12), range: 20–70 | 61 | 4.52 (0.34) | 2.18 (0.91) | 1065 |
| AUS06 | WA (North Metropolitan) | 40 | 42 (16), range: 17–79 | 55 | 4.62 (0.40) | 2.42 (1.36) | 1065 |
| AUS07 | WA (North Metropolitan) | 41 | 44 (11), range: 20–66 | 68 | 4.54 (0.35) | 2.62 (1.20) | 1065 |
Note: *Mean score of the 20-item MRPS questionnaire, where 1 indicates high dissatisfaction and 5 indicates high satisfaction.
†Global rating of change in condition, where 1 indicates very much better and 9 indicates very much worse.
‡SES: socioeconomic status score of the clinic suburb. Index scores have been standardized to have a mean of 1000 and a standard deviation of 100 across Australia (Australian Bureau of Statistics).
Patient satisfaction in Australia
The mean satisfaction score for all Australian respondents was 4.55 (95% CI: 4.51–4.59) on a scale where 1 indicates high dissatisfaction and 5 indicates high satisfaction. Mean (SD) satisfaction for individual MRPS items ranged from 4.84 (0.37) for The office receptionist was courteous, to 4.25 (0.92) for This office provided convenient parking (Table 2). There were no significant differences in mean satisfaction scores between Australian clinics (F6273 = 0.38, P = 0.89). Satisfaction scores also did not vary significantly depending on the body area treated (F6253 = 1.71, P = 0.12). Female respondents were slightly but significantly more satisfied (mean: 4.66, SD: 0.32) than their male counterparts (mean: 4.41, SD: 0.37) (t239 = 5.59, P<0.001). Global satisfaction for item 19 (Overall I am completely satisfied with the services I received from my therapist) was consistently high across clinics, with a mean score of 4.73 (SD: 0.45). There was no significant relationship between global satisfaction and travel duration (r = 0.01, P = 0.91), age (r = −0.04, P = 0.51) or socioeconomic status of the clinic location (r = 0.07, P = 0.25).
Table 2. Patient satisfaction scores for each MRPS item, listed from highest to lowest satisfaction for Australian (n = 274) and US12 (n = 203) data, and bivariate correlations between each item and global satisfaction score, with lower and upper bounds of the corresponding 95% CIs.
| MRPS item | Australia | United States | Australia | United States |
| Item satisfaction rated from | Patient satisfaction | Patient satisfaction | Correlation with global satisfaction | Correlation with global satisfaction |
| 1 (strongly disagree) to 5 (strongly agree) | Mean (95% CI) | Mean (95% CI) | Pearson r, (95% CI) | Pearson r, (95% CI) |
| The office receptionist was courteous | 4.84 (4.80–4.88) | 4.70 (4.57–4.83) | 0.37 (0.26–0.47) | 0.56 (0.46–0.65) |
| My therapist treated me respectfully | 4.80 (4.74–4.86) | 4.80 (4.71–4.89) | 0.41 (0.31–0.50) | 0.61 (0.52–0.69) |
| The office staff were respectful | 4.76 (4.70–4.82) | 4.73 (4.64–4.82) | 0.42 (0.32–0.51) | 0.64 (0.55–0.71) |
| My therapist listened to my concerns* | 4.68 (4.62–4.74) | 4.78 (4.69–4.87) | 0.35 (0.24–0.45) | 0.76 (0.70–0.81) |
| My therapist thoroughly explained my treatment | 4.66 (4.58–4.74) | 4.73 (4.65–4.81) | 0.51 (0.42–0.59) | 0.63 (0.54–0.71) |
| My therapist answered all my questions | 4.64 (4.57–4.71) | 4.77 (4.68–4.86) | 0.55 (0.46–0.63) | 0.75 (0.68–0.80) |
| The registration process was appropriate | 4.61 (4.58–4.70) | 4.60 (4.51–4.69) | 0.39 (0.28–0.49) | 0.53 (0.42–0.62) |
| The therapist's assistant was respectful | 4.61 (4.55–4.67) | 4.61 (4.51–4.71) | 0.35 (0.24–0.45) | 0.54 (0.44–0.63) |
| My therapist gave me detailed home program instructions | 4.57 (4.50–4.64) | 4.78 (4.67–4.89) | 0.61 (0.53–0.68) | 0.73 (0.66–0.79) |
| The office hours were convenient for me | 4.57 (4.49–4.65) | 4.65 (4.57–4.73) | 0.26 (0.15–0.37) | 0.63 (0.54–0.71) |
| My therapist advised how to avoid future problems | 4.55 (4.48–4.62) | 4.57 (4.47–4.67) | 0.53 (0.44–0.61) | 0.51 (0.40–0.61) |
| The office and its facilities were clean | 4.53 (4.46–4.60) | 4.74 (4.63–4.85) | 0.45 (0.35–0.54) | 0.70 (0.62–0.76) |
| My therapist spent enough time with me* | 4.47 (4.41–4.53) | 4.79 (4.71–4.87) | 0.50 (0.41–0.58) | 0.70 (0.62–0.76) |
| The office location was convenient* | 4.14 (4.05–4.23) | 3.60 (3.52–3.68) | 0.27 (0.16–0.38) | 0.11 (−0.03–0.24) |
| I didn’t wait too long to see my therapist* | 4.36 (4.23–4.49) | 3.22 (3.01–3.43) | 0.26 (0.15–0.37) | 0.11 (−0.03–0.24) |
| The office used up-to-date equipment | 4.33 (4.23–4.43) | 4.59 (4.35–4.83) | 0.56 (0.47–0.64) | 0.52 (0.41–0.61) |
| The waiting area was comfortable | 4.31 (4.23–4.39) | 4.63 (4.53–4.73) | 0.25 (0.14–0.36) | 0.58 (0.48–0.66) |
| This office provided convenient parking | 4.25 (4.17–4.33) | 4.14 (4.05–4.23) | 0.11 (−0.01–0.23) | 0.37 (0.25–0.48) |
Note: Figures in bold indicate differences in correlations that are significant at P<0.01; the rest indicate non-significant differences between US and Australian data.
*Item converted to positively worded format.
The relationships between individual item scores and global satisfaction (item 19) were explored with bivariate correlation analyses. The inter-item correlation matrix (Table 2) shows that for the Australian data, a cluster of items about interpersonal aspects of the physiotherapy consultation, particularly communication, correlate most strongly with global satisfaction. These items include: My therapist gave me detailed instructions regarding my home program (r = 0.61, P<0.001), My therapist answered all my questions (r = 0.55, P<0.001), My therapist thoroughly explained the treatment(s) I received (r = 0.51, P<0.001) and My therapist advised me on ways to avoid future problems (r = 0.53, P<0.001). Organization-related variables such as clinic location, hours, parking, and comfort had the lowest correlations with global satisfaction (Table 2).
We were interested to investigate the relationship between patient satisfaction and treatment outcomes, measured by the global rating of change item. The mean global rating of change, as a response to the question: How does your current condition compare to how it was before you started physiotherapy treatment? was 2.2 (SD: 1.1), where 1 indicates very much better and 9 very much worse. The global rating of change score was significantly but only weakly correlated with the mean global satisfaction (item 19) score (r = −0.22, P<0.001), even though most respondents (92%) indicated their condition was better after physiotherapy treatment (25.9% very much better, 42.3% much better, and 17.2% somewhat better). Only 1.1% of participants rated their condition as worse (1.1% somewhat worse, 0% much worse, and 0% very much worse.) The two clinics that treated younger patients (AUS02, AUS03) had significantly higher (F1259 = 28.51, P<0.001) global rating of change scores than the other five clinics (Table 1). This result is interpreted as an age effect, whereby the younger cohorts presenting for sports injuries may perceive greater change in their condition with treatment and is supported by the high correlation between mean scores of global rating of change with respondent age (r = 0.95, P = 0.001).
Comparison of patient satisfaction scores in Australia with international data
The high degree of satisfaction with musculoskeletal physiotherapy care in Australia is comparable with that found from other countries (Fig. 1). The 95% CIs of mean scores for Australia overlap or differ by less than 0.05 of a point (on the scale from 1 to 5) with 95% CIs of means from Canada,13 United States,11,14 Sweden,15 and Ireland.16 However, the patient satisfaction scores obtained here were significantly higher than those in England,17 and a smaller Canadian study.18
Figure 1.
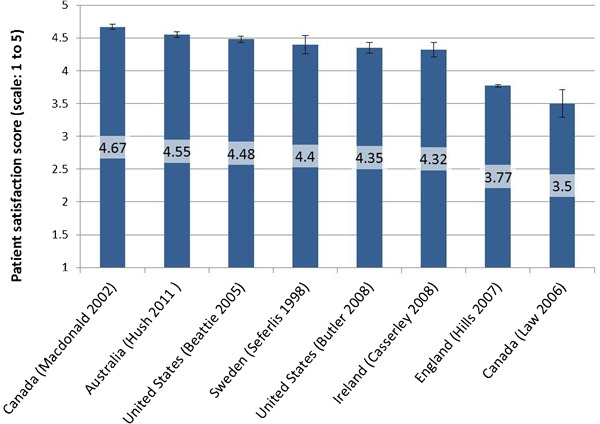
Comparison of Australian patient satisfaction scores with those from other countries. Bars represent mean scores (where 1 indicates high dissatisfaction and 5 indicates high satisfaction) with 95% CIs. Patient satisfaction data from countries other than Australia, were extracted from Ref. 9.
A comparison of patient satisfaction in Australia and the US
We compared data collected in Australia with those from a US study12 that used the same 20-item MRPS instrument (Table 2). Inspection of 95% CIs of the means for individual items showed no significant differences in satisfaction scores for most (13) items; however, scores were significantly different for the following five items: My therapist gave me detailed home program instructions; The office and its facilities were clean; My therapist spent enough time with me; The office location was convenient and The waiting area was comfortable. On all items except convenience of office location, US respondents were more satisfied than their Australian counterparts.
We also explored similarities and differences in satisfaction determinants between the Australian US cohorts, by inspecting the bivariate correlations of MRPS items with global satisfaction (Table 2). For half of the items, the correlation with global satisfaction was not significantly different between the two cohorts. These included interpersonal features of care (e.g. My therapist thoroughly explained my treatment; My therapist gave me detailed home program instructions; My therapist advised how to avoid future problems;) as well as process of care variables (e.g. The registration process was appropriate; The office location was convenient; The office used up-to-date equipment). There were nine items with significantly different correlations with global satisfaction between Australia and the US. The correlations were all higher for the US data and included professional and service aspects of care (e.g. My therapist listened to my concerns; My therapist answered all my questions; My therapist spent enough time with me; The office and its facilities were clean; The waiting area was comfortable; This office provided convenient parking; The office hours were convenient).
Respondents’ perceptions
The respondents’ perceptions about the dimensions of satisfaction with physiotherapy care were also determined by analysis of free comments made in designated space at the end of the questionnaire. Respondents frequently (20%) identified therapist attributes as a key dimension of satisfaction. The therapist and clinic staff attributes that were considered important included professionalism, competence, effectiveness, friendliness, respectfulness, and caring. Effective communication skills were highly valued, particularly with regards to explaining the condition and educating about self-management strategies. Organization of care issues such as clinic location, facilities, and equipment were less frequently commented on (3%). The importance of individualized care and patient involvement in the decision-making process was also mentioned as a desirable component of care. These comments align with the objective data summarized above.
Discussion
This paper reports on the first comprehensive evaluation of patient satisfaction with musculoskeletal physiotherapy care in Australia. The results indicate that patient satisfaction in Australia is high (4.55, 95%CI: 4.51 to 4.59) and that it is comparable with the pooled score of patient satisfaction with musculoskeletal care from England, North America, Ireland and Northern Europe (4.44, 95% CI: 4.41–4.46) reported in a recent systematic review and meta-analysis.9 One feature that is most striking about these results is the consistency of high satisfaction across different populations, even though different patient satisfaction instruments were used between studies.
However, significantly lower mean satisfaction scores have been noted in two studies. The first of these was conducted in England,17 where participants were recruited from the National Health Service. It is possible that the lower patient satisfaction levels reported in this study were influenced by the widely recognized organizational problems in this public health system,17 as patients may incorporate their experiences and feelings about the health system into their satisfaction rating. In the second study that reported lower patient satisfaction, Law et al.18 investigated the efficacy of imagery techniques for athletes with lower limb injuries, at a single sports medicine clinic in Canada. Lower satisfaction scores from this small (n = 83) and specific patient group may be influenced by the patients’ feelings about the imagery treatment technique, and are also likely to be less representative than results from another Canadian study 13 in which a larger (n = 422) and wider sampling frame was employed and higher satisfaction scores were obtained (4.67, 95% CI: 4.63–4.71).
Features of care that underpin patient satisfaction were investigated by examining correlations between questionnaire items and the global measure of satisfaction. Our findings are consistent with research from Europe, North America, and the United Kingdom that showed effective therapist–patient communication to be a key determinant of high satisfaction,9 and a recent systematic review demonstrating the importance of a good working relationship between therapist and patient for satisfaction with physiotherapy treatment.19
Our results reveal some specific aspects of therapist communication that Australian respondents valued: the ability to provide helpful information about their condition, to give a thorough explanation about the treatment plan and to explain the patient’s role in the management of their condition. These aspects of professional physiotherapy care are important in empowering patients with a clear understanding of their condition, enabling involvement in treatment planning and educating patients about self-management. Interestingly, the degree of change in patients’ condition following treatment did not correlate strongly with global patient satisfaction, which supports previous research findings.9 Indeed, it has been shown that patients can feel satisfied with learning effective self-management strategies even when pain reduction is minimal.13,20,21
We also investigated whether particular respondent characteristics were associated with higher satisfaction with physiotherapy care. We found no significant correlation with age, in contrast to evidence from Ireland16 and Canada22 that older patients tend to be more satisfied with aspects of physiotherapy care such as access to services and good communication skills of the therapist. Perhaps because of the private practice setting of this Australian study where these features of care were highly rated, age-related differences were not detected. However, the two clinics that treated younger patients did have significantly higher global ratings of change, likely due to the greater physical and motivational capacity in this younger, predominantly athletic cohort for recovery from musculoskeletal injury. Our results did show small gender differences in satisfaction, with female respondents reporting higher satisfaction with physiotherapy care than males. This finding aligns with previous research into gender differences in patient satisfaction,9,17,23 and that expectations of care are significantly higher in males.17
Comparison of Australian and US data revealed both commonalities and country-specific differences, although it is unknown how representative the US cohort is of the general US population. Satisfaction levels for most aspects of physiotherapy care were comparable, as indicated by mean scores and confidence intervals. However, while interpersonal and professional aspects of care were rated highly for both cohorts, the US respondents reported greater satisfaction than their Australian counterparts for process factors such as convenience of clinic location, clinic cleanliness and waiting room comfort, perhaps because these features are considered more important for patients in the US. There were many common contributors of physiotherapy care to overall satisfaction, as shown by the correlation analysis of items with global satisfaction. These included therapist–patient communication features, such as explaining treatment and giving advice about self-care, as well as some process of care variables such as convenience of the clinic location and having up-to-date equipment. However, the fact that the correlations were significantly different between Australia and the US for half of the items suggests there may also be features of care that are unique to each country. Interestingly, items with significantly different correlations were consistently higher in the US cohort. These aspects of care included convenient hours and parking, clean and comfortable facilities, and adequate time with the therapist, suggesting that US patients have higher expectations of the professional service component of care.
One potential limitation of this study is response bias. The mean response rate of the cohort surveyed was 22% which, while not ideal, is comparable with other studies of patient satisfaction,10 particularly in a fee-for-service setting. Despite this, the distribution of demographic variables and clinic variables suggest that these data are representative of the two most common types of private outpatient physiotherapy clinics in Australia: general community clinics and sports clinics. In support of this interpretation is the evidence that mean satisfaction scores did not significantly differ between clinics, despite different geographic regions, area health services and metropolitan or rural settings. Further, the distribution of patient satisfaction scores was unimodal (Fig. 2), suggesting that respondents were not just those who were either highly dissatisfied or highly satisfied. It is important to emphasize that the response rate does not affect interpretation of the internal relationships between variables, which has provided valuable insight into possible determinants of patient satisfaction. The risk of response bias due to measurement was minimized, as items were scored using Likert scales with equal numbers of positive and negative categories. It is not possible to rule out some degree of response bias due to social desirability, as respondents may have been reluctant to admit unfavourable attitudes, particularly as surveys were administered in the clinic, although anonymously.9 Patient satisfaction in public hospital outpatient departments may differ from the data presented in this study.
Figure 2.
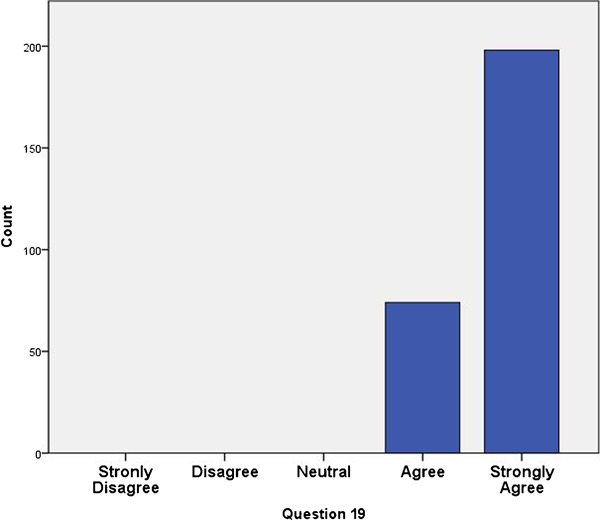
Histogram of global satisfaction scores (MRPS item 19: Overall, I am completely satisfied with the services I received from my therapist) indicating a unipolar distribution of responses.
Conclusions
This study indicates that patient satisfaction with musculoskeletal physiotherapy care in Australia is high, comparing favourably with international data. These results may be useful in providing a benchmark of patient satisfaction for clinics, professional physiotherapy associations and those who fund physiotherapy services. Of particular interest is that this study reveals commonalities as well as differences in features of patient satisfaction with care between the US and Australia, warranting further investigation of determinants of satisfaction that may be unique to specific countries or cultures.
Acknowledgments
The authors are very grateful to the physiotherapists who enabled data collection at their clinics in New South Wales and Western Australia. We would also like to acknowledge Amanda Semon (DPT) and Charles Johnson at Lebanon Valley College, Annville, PA for their excellent assistance with data entry for this study.
References
- 1.Donabedian A. The quality of care. How can it be assessed? J Am Med Assoc. 1988;260:1743–8 [DOI] [PubMed] [Google Scholar]
- 2.Law M, Baptiste S, Mills J. Client-centred practice: What does it mean and does it make a difference? Canadian Journal of Occupational Therapy. 1995;62:250–7 [DOI] [PubMed] [Google Scholar]
- 3.Wagner D, Bear M. Patient satisfaction with nursing care: a concept analysis within a nursing framework. J Adv Nurs. 2009;65:692–701 [DOI] [PubMed] [Google Scholar]
- 4.Hush JM, Alison JA. Evidence-based practice: lost in translation? J Physiother. 2011;57:207–8 [DOI] [PubMed] [Google Scholar]
- 5.Safran D, Taira D, Rogers W, Kosinski M, Ware JE, Tarlov AR. Linking primary care performance to outcomes of care. J Fam Pract. 1998;47:213–20 [PubMed] [Google Scholar]
- 6.Fitzpatrick R. Scope and measurement of patient satisfaction. Fitzpatrick R, Hopkins A, editors. Measurement of patients’ satisfaction with their care London: Royal College of Physicians; 1993 [Google Scholar]
- 7.Guldvog B. Can patient satisfaction improve health among patients with angina pectoris? Int J Qual Health Care. 1999;11:233–40 [DOI] [PubMed] [Google Scholar]
- 8.Draper M, Hill S. The role of patient satisfaction surveys in a national approach to hospital quality managment. Melbourne: Faculty of Social Sciences and Communications. Royal Melbourne Institute of Technology; 1995 [Google Scholar]
- 9.Hush J, Cameron K, Mackey M. Patient satisfaction with musculoskeletal physical therapy care: A systematic review. Phys Ther. 2011;91:25–36 [DOI] [PubMed] [Google Scholar]
- 10.Beattie PF, Pinto MB, Nelson MK, Nelson R. Patient satisfaction with outpatient physical therapy: instrument validation. Phys Ther. 2002;82:557–65 [PubMed] [Google Scholar]
- 11.Beattie P, Turner C, Dowda M, Michener L, Nelson R. The MedRisk instrument for measuring patient satisfaction with physical therapy care: a psychometric analysis. Journal of Orthopaedic and Sports Physical Therapy. 2005;35(1):24–32 [DOI] [PubMed] [Google Scholar]
- 12.Beattie PF, Nelson RM, Lis A. Spanish-language version of the MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care (MRPS): preliminary validation. Phys Ther. 2007;87:793–800 [DOI] [PubMed] [Google Scholar]
- 13.MacDonald CA, Cox PD, Bartlett DJ. Productivity and client satisfaction: a comparison between physical therapists and student-therapist pairs. Physiother Can. 2002;54:92–101 [Google Scholar]
- 14.Butler RJ, Johnson WG, Butler RJ, Johnson WG. Satisfaction with low back pain care. Spine J. 2008;8:510–21 [DOI] [PubMed] [Google Scholar]
- 15.Seferlis T, Nemeth G, Carlsson AM, Gillstrom P. Conservative treatment in patients sick-listed for acute low-back pain: a prospective randomised study with 12 months’ follow-up. Eur Spine J. 1998;7:461–70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Casserley-Feeney SN, Phelan M, Duffy F, Roush S, Cairns MC, Hurley DA. Patient satisfaction with private physiotherapy for musculoskeletal pain. BMC Musculoskelet Disord. 2008;9:50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hills R, Kitchen S. Satisfaction with outpatient physiotherapy: a survey comparing the views of patients with acute and chronic musculoskeletal conditions. Physiother Theory Pract. 2007;23:21–36 [DOI] [PubMed] [Google Scholar]
- 18.Law B, Driediger M, Hall C, Forwell L. Imagery use, perceived pain, limb functioning and satisfaction in athletic injury rehabilitation. N Z J Physiother. 2006;34:10–6 [Google Scholar]
- 19.Hall AM, Ferreira PH, Maher CG, Latimer J, Ferreira ML. The Influence of the Therapist-Patient Relationship on Treatment Outcome in Physical Rehabilitation: A Systematic Review. Phys Ther. 2010;90:1099–110 [DOI] [PubMed] [Google Scholar]
- 20.May SJ. Patient Satisfaction with Management of Back Pain. Physiotherapy. 2001;87:4–20 [Google Scholar]
- 21.Hills R, Kitchen S. Toward a theory of patient satisfaction with physiotherapy: exploring the concept of satisfaction. Physiother Theory Pract. 2007;23:243–54 [DOI] [PubMed] [Google Scholar]
- 22.McKinnon AL. Client Satisfaction with Physical Therapy Services: Does Age Make a Difference? Phys Occup Ther Geriatr. 2001;19:23–37 [Google Scholar]
- 23.Hsieh M, Kagle JD. Understanding patient satisfaction and dissatisfaction with health care. Health Soc Work. 1991;16:281–90 [DOI] [PubMed] [Google Scholar]