

Abstract
Objective:
As the acquired immunodeficiency syndrome (AIDS) epidemic shows no signs of abating, the impact of AIDS is felt more in the developing countries due to socioeconomic reasons. The possibility of drug-induced ototoxicity also adds to the risk of audio vestibular dysfunction. We sought to determine if there was a difference between the audio-vestibular function in the asymptomatic human immunodeficiency virus (HIV) infected patients and patients with AIDS.
Study Design:
A prospective, cross-sectional study
Setting:
A tertiary care center in South India
Materials and Methods:
The audio-vestibular system of 30 asymptomatic HIV positive subjects (group 1) and 30 subjects with AIDS (group 2), and age-matched 30 healthy controls (group 3) were assessed using pure tone audiometry and cold caloric test.
Results:
Sixteen patients each, in group 1 and group 2 and four subjects in the control group were detected to have a hearing loss indicating significantly more HIV infected individuals (group 1 and 2) were having hearing loss (P=0.001). Kobrak's (modified) test showed 27% of patients in group 1 and 33% of patients in group 2 and none in the group 3 had a hypofunctioning labyrinth (P=0.001).
Conclusion:
It seems that the human immunodeficiency virus does affect the audio-vestibular pathway. There was a significant incidence of audio-vestibular dysfunction among the HIV infected patients, as compared to the control population (P=0.001) and no significant difference between the asymptomatic HIV seropositive patients and AIDS patients. Majority of the patients had no otological symptoms.
Keywords: AIDS, audio-vestibular function, hearing loss, HIV
INTRODUCTION
The first case of HIV infection in India was reported in 1986.[1] The 2009 estimates suggest national adult HIV prevalence in India is approximately 0.31%, amounting to about 2.4 million people. With a population of about a billion, an increase in 0.1% of HIV prevalence would result in over half a million HIV infected patients.
The human immunodeficiency virus(HIV) being neurotropic and lymphotropic, it does not spare the domain of the otolaryngologist. The HIV virus may affect the neuraxis at any level.[2] Heterosexual transmission of HIV infection continues to be the principal mode of infection in many developing countries. Also advances in anti-retroviral therapy have resulted in a dramatic decline in mortality for individuals infected with human immunodeficiency virus. There appears to be a particular geographic distribution pattern of the HIV subtypes possibly depending on the different modes of transmission of the infection.[3] Various observations from the west regarding the hearing and vestibular dysfunction have been reported in HIV infected patients, but very few reports from the developing countries.[4–8] In this study, we proposed to examine the status of the auditory and vestibular system in HIV infected patients and determine if there was a difference between the asymptomatic HIV infected patients and patients with AIDS.
MATERIALS AND METHODS
Study design
A prospective, cross-sectional study.
HIV infected patients attending a south Indian tertiary care hospital either as in-patients or outpatients of the ENT, General Medicine, Dermatology and Infectious disease clinics during a six-month period was enrolled in the study. Patients willing to participate in the study were enrolled consecutively after the study was approved by the institutional review board.
Patients were divided into 2 groups: group 1 included asymptomatic HIV seropositive individuals and group 2 patients with AIDS. Also included in the study was an age-matched control group of HIV sero-negative individuals who constituted group 3 from the general population, who were not on any medications. Each group had 30 subjects in the age group 15-45 years and they were evaluated for audio-vestibular dysfunction. None of the patients were on anti-retroviral therapy (ART). Excluded from the study were subjects(both patients and controls) in whom there was a possibility of audio-vestibular dysfunction due to other causes such as past history of any ear disease or surgeries, family history of otological problems, previous history of ototoxic drug intake, noise exposure and presence of diabetes mellitus or hypertension.
The study subjects underwent an initial otoscopy to ensure that the external canal was free of wax or any discharge. Pure tone audiometry using Beltone 2000 audiometer was performed to establish the hearing threshold using modified Hughson-Westlake procedure. Normal hearing was defined at 20 dB or better at frequencies 500 Hz to 8 kHz. The severity of hearing loss was divided as follows: 20-40 dB mild, 40-55 dB moderate, 55-70 dB moderately severe, 70-90 dB severe and > 90 dB profound.[9] Vestibular function was assessed by modified Kobrak's test. Here the external canal is irrigated for 60 s with ice cold water in increasing quantity (5, 10, 20 and 40 ml) till nystagmus is noticed. Nystagmus noticed with 5ml is a normal labyrinth. While in a hypoactive labyrinth irrigation with 10,20, or 40 ml may be required. A dead labyrinth is one where no nystagmus is elicited with even 40 ml of ice cold water.
Statistical analysis
The data was analyzed using SPSS 17software. Chi-square test was used to test the significance between the categorical variables. Analysis of variance (ANOVA) was used to compare the means of continuous variables of 3 groups. The criterion for statistical significance was P ≤0.05.
RESULTS
The HIV sero-positive patients were divided into 2 groups: asymptomatic group and patients with AIDS. Heterosexual transmission of HIV infection was the principal mode of infection. The baseline data is presented in Table 1 and the associated medical problems in Table 2. The mean(SD)ages of the subjects of the group 1, 2 and 3 were 29(5.6), 32(6.1) and 30(6.2)years respectively and were not different across the 3 groups (P=0.237). In group 1, there were 24(80%) males and six (20%) females. In group 2, there were 29(97%) males and one (3%) female. Group 3 comprised of 26(87%) males and four (13%) females.
Table 1.
Baseline patient data
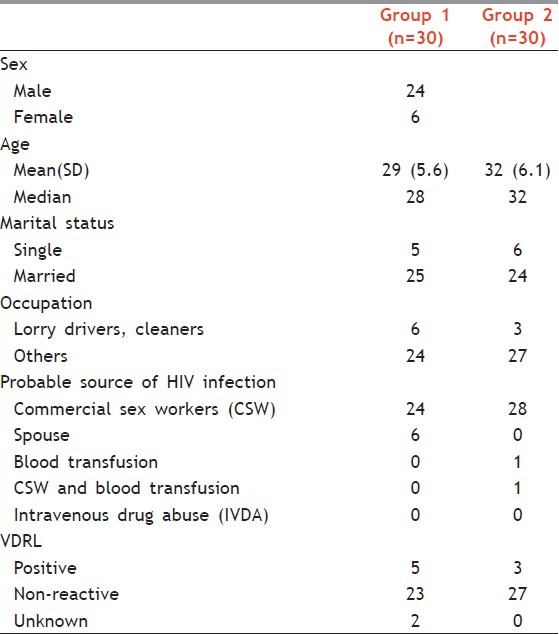
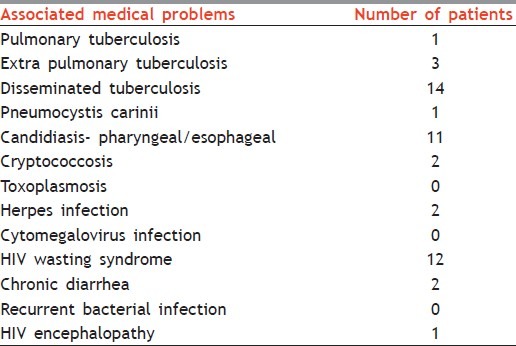
Table 2.
Associated medical problems in patients with aids
PURE TONE AUDIOMETRY: Significantly, more people in group 1 and 2 (n==16 in each group) when compared to the control group were detected to have a hearing loss (P=0.001).
Of the 16 patients(54%) in group 1 detected to have a hearing loss, 13 had sensorineural hearing loss (SNHL), two had conductive hearing loss (CHL) and in one patient, one ear showed a sensorineural loss at 4 and 8 kHz while the other had a mild conductive loss at 500 Hz and sensorineural loss at 4 kHz. In patients with only SNHL, five patients had a mild 4 kHz dip; three had a 8 kHz loss, and five showed a mild-to-moderate loss at 4 and 8 kHz.
In group 2, the audiograms of 16(54%) patients were abnormal. Hearing loss was unilateral in five and bilateral in 11 patients. Eleven patients (37%) had mild-to-moderate sensorineural hearing loss mostly in 4 and 8 kHz. Changes were noted in five others too; two had mild COHL in the lower frequencies and mild-to-moderate SNHL in the higher frequencies. In three patients, it was asymmetrical, with one ear showing a SN loss in all the frequencies and in the other COHL in the lower frequencies and SN loss in the higher frequencies.
In the control group, four audiograms showed mild SNHL (unilateral in three and bilateral in one). Here too, the hearing losses were noted at 4 or 8 kHz or at 4 and 8 kHz.
MODIFIED KOBRAK'S TEST
Kobrak's (modified) test showed 27% (n=8) of patients in group 1 and 33% (n=10) of patients in group 2 had a hypofunctioning labyrinth. It was unilateral in five and bilateral in three patients in group 1. In group 2, it was unilateral in five and bilateral in five. Groups 1 and 2 were comparable (P value = 0.95). The test was normal in all the subjects in the control group. When all 3 groups were compared, it was found that HIV infected patients (group 1 and group 2) had a greater risk of developing vestibular dysfunction (P=0.001).
DISCUSSION
In this study which was undertaken to determine the auditory and vestibular status in HIV infected patients, we sought to determine if there was any difference in the findings between HIV seropositive asymptomatic patients and HIV seropositive patients with AIDS. Also, the significance of the audio-vestibular dysfunction noted in HIV infected patients was determined by including a control group.
Hausler et al.[4] noted normal hearing threshold in the asymptomatic HIV positive patients, the criteria for abnormality being thresholds > 20 dB (500 - 200 Hz). In this study among the asymptomatic HIV seropositive, as many as 16 patients (50%) were detected to have a hearing loss (thresholds > 20 dB at 500-8000 Hz). In another study among 128 serologically positive active army recruits, Bell et al.[6] detected hearing loss in 20.9% recruits (threshold > 15 dB). Among the patients with AIDS, we found hearing loss in about 50% cases which was in agreement with the findings of a prospective study of 53 patients with AIDS at the San Francisco general hospital.[6] Evaluating otologic disease in patients with AIDS in a five-year retrospective study at the New York University Medical Center, Bellevue hospital center, 26 patients with documented otologic symptoms (hearing loss 62%, otalgia 50%, otorrhea 31%, vertigo 15% and tinnitus 15%) were found.[5] In our study, only two patients were symptomatic. One patient complained of blocked sensation in the ears and the other complained of vertigo. Chandresekar et al.[10] reported that a third of HIV infected patients have significant otologic complaints or findings. Sensorineural hearing loss in patients with AIDS has been attributed to iatrogenic causes (ototoxic medications), opportunistic infections of nervous system (cryptococcal meningitis, tuberculous meningitis, viral pathogens like cytomegalovirus, herpes virus,), otosyphilis, malignancy and progressive multifocal leukoencephalopathy (PML) or AIDS encephalopathy or AIDS dementia complex.[6,11–13] In our study despite the fact that we had only two patients with cryptococcosis, one patient with HIV encephalopathy and one patient with TB meningitis, and the fact that we excluded those patients with a previous history of ototoxic drug intake, as many as 37% of cases in group 2 had a sensorineural hearing loss with two patients having a conductive hearing loss in lower frequencies and sensorineural hearing in higher frequencies, three patients had asymmetrical hearing loss. Teggi et al,[14] reported that the incidence of peripheral vestibular disorders remained almost same among the various classes of HIV infected patients, and this was in agreement with our study.
Pappas et al.,[15] investigating the presence of pathogens in the cochlea of AIDS cases, found extracellular viral-like particles with morphologic characteristics of HIV-1 on the tectorial membrane in three cases. Numerous viral-like particles appearing essentially similar to identified HIV-1 particles in infected lymphocyte cultures were found within the cytoplasm of the connective tissue cells. This demonstration of viral-like particles and cochlear pathology might explain the auditory manifestations associated with HIV infection. In another study by Pappas et al.,[16] pathological changes were identified in the labyrinth wall, the epithelial lining and the maculae and cristae. Cytological changes in hair cells included inclusion bodies, viral-like particles and hair bundle malformations. Epithelial lining cells, supporting cells and connective tissue cells had inclusions and viral-like particles. These findings together with that of the cochlear study provides an insight into the likely pathogenesis of viral-induced hearing loss and vestibular impairment in HIV infected patients.
The otopathology could be at multiple sites along the auditory and vestibular pathway and the prime cause of the otopathology could be due to the HIV virus itself as there was no statistically significant difference in the hearing loss and vestibular dysfunction between HIV seropositive asymptomatic patients and those with AIDS.
With increasing number of patients with HIV infection, otolaryngologists need to be aware that the HIV virus could result in audio-vestibular dysfunction. Initiating anti retroviral therapy (ART) in HIV positive individuals may also compound the audio-vestibular dysfunction as some of the agents like nucleoside analog reverse transcriptase inhibitors (NRTIs)may have ototoxic side effects example:.[17,18,19] So these individuals need to be screened before starting the ART treatment.
CONCLUSION
The human immunodeficiency virus being neurotropic affects the auditory and vestibular pathway, although majority of the patients did not complain of hearing loss, giddiness or tinnitus. The audio-vestibular dysfunction could be unilateral or bilateral, symmetrical or asymmetrical and the hearing loss could be conductive, sensorineural or mixed. Statistically no significant difference in the audio-vestibular dysfunction was noted between the HIV seropositive asymptomatic patients and patients with AIDS. However, long-term studies are needed to look at these aspects in a larger group of patients.
Footnotes
Source of Support: The study was supported in part by the FLUID research funds, Christian Medical College, Vellore.
Conflict of Interest: None declared.
REFERENCES
- 1.Simoes EA, Babu PG, John TJ, Nirmala S, Solomon S, Lakshminarayana CS, et al. Evidence for HTLV-III infection in prostitutes in Tamil Nadu (India) Indian J Med Res. 1987;85:335–8. [PubMed] [Google Scholar]
- 2.Brew BJ Medical management of AIDS patients. Med Clin North Am. 1992;76:63–81. doi: 10.1016/s0025-7125(16)30371-6. [DOI] [PubMed] [Google Scholar]
- 3.Hardy WD., Jr The human immunodeficiency virus. Med Clin North Am. 1996;80:1239–61. doi: 10.1016/s0025-7125(05)70489-2. [DOI] [PubMed] [Google Scholar]
- 4.Hausler R, Vibert D, Koralnik IJ, Hirschel B. Neuro-otological manifestations in different stages of HIV infection. Acta Otolaryngol Suppl. 1991;481:515–21. doi: 10.3109/00016489109131461. [DOI] [PubMed] [Google Scholar]
- 5.Kohan D, Rothstein SG, Cohen NL. Otologic disease in patients with acquired immunodeficiency syndrome. Ann Otol Rhino Laryngol. 1988;97:636–40. doi: 10.1177/000348948809700611. [DOI] [PubMed] [Google Scholar]
- 6.Lalwani AK, Sooy CD. Otolaryngologic Manifestations of Acquired Immunodeficiency syndrome. Otolaryngol Clin North Am. 1992;25:1183–98. [Google Scholar]
- 7.Hart CW, Cokely CG, Schupbach J, Dal Canto MC, Coppleson LW. Neurotologic findings of a patient with acquired immunodeficiency syndrome. Ear Hear. 1989;10:68–96. doi: 10.1097/00003446-198902000-00012. [DOI] [PubMed] [Google Scholar]
- 8.Fairley JW, Dhillon RS, Weller IV. HIV, Glue ear, and adenoidal hypertrophy. Lancet. 1988;2:1422. doi: 10.1016/s0140-6736(88)90610-1. [DOI] [PubMed] [Google Scholar]
- 9.Dennis JM, Neely JG. CLincal Audiology. Otolaryngol Clin North Am. 1992;25:707–28. [Google Scholar]
- 10.Chandrasekhar SS, Connelly PE, Brahmbhatt SS, Shah CS, Kloser PC, Baredes S. Otologic and audiologic evaluation of human immuno deficiency virus-infected patients. Am J Otolaryngol. 2000;21:1–9. doi: 10.1016/s0196-0709(00)80117-9. [DOI] [PubMed] [Google Scholar]
- 11.Friedman-Kein AE, Lafleur FL, Gendler E, Hennessey NP, Montagna R, Halbert S, et al. Herpes zoster: A possible early sign for development of acquired syndrome in high risk individuals. J Am Dermatol. 1986;14:1023–8. doi: 10.1016/s0190-9622(86)70127-8. [DOI] [PubMed] [Google Scholar]
- 12.Morris MS, Prasad S. Otologic disease in the acquired immunodeficiency syndrome. Ear Nose Throat J. 1990;69:451–3. [PubMed] [Google Scholar]
- 13.Smith ME, Canalis RF. Otologic manifestations of AIDS: The Otosyphilis connection. Laryngoscope. 1989;99:365–72. doi: 10.1288/00005537-198904000-00001. [DOI] [PubMed] [Google Scholar]
- 14.Teggi R, Ceserani N, Luce FL, Lazzarin A, Bussi M. Otoneurological findings in human immunodeficiency virus positive patients. J Laryngol Otol. 2008;11:1–6. doi: 10.1017/S0022215107001624. [DOI] [PubMed] [Google Scholar]
- 15.Pappas DG, Jr, Chandra Sekhar HK, Lim J, Hillman DE. Ultrastructural findings in the cochlea of AIDS cases. Am J Otol. 1994;15:456–65. [PubMed] [Google Scholar]
- 16.Pappas DG, Jr, RolandW JT, Jr, Lim J, Lai A, Hillman DE. Ultrastructural findings in the vestibular and end–organs of AIDS cases. Am J Otol. 1995;16:140–5. [PubMed] [Google Scholar]
- 17.Simdon J, Watters D, Bartlett S, Connick E. Ototoxicity associated with use of nucleoside analog reverse transcriptase inhibitors: A report of 3 possible cases and review of the literature. Clin Infect Dis. 2001;32:1623–7. doi: 10.1086/320522. [DOI] [PubMed] [Google Scholar]
- 18.Brinkman K, Kakuda TN. Mitochondrial toxicity of nucleoside analogue reverse transcriptase inhibitors: a looming obstacle for long-term antiretroviral therapy? Curr Opin Infect Dis. 2000;13:5–11. doi: 10.1097/00001432-200002000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Vogeser M, Colebunders R, Depraetere K, Van Wanzeele P, Van Gehuchten S. Deafness caused by didanosine. Eur J Clin Microbiol Infect Dis. 1998;17:214–5. doi: 10.1007/BF01691123. [DOI] [PubMed] [Google Scholar]