

Abstract
Nevus lipomatosus cutaneous superficialis (NLCS) is an uncommon benign hamartomatous condition characterized by the presence of mature ectopic adiopocytes in the dermis. It was first reported by Hoffman and Zurhelle in 1921. Clinically they areit is classified into two forms. The classical form is characterized by groups of multiple, non-tender, soft, pedunculated, cerebriform, yellowish or skin-colored papules, nodules, or plaques. The other form of NLCS clinically manifests as a solitary dome-shaped or sessile papule. The classical NLCS is mostly reported to involve the pelvic or gluteal region. We report here a case of adult-onset classical NLCS on perianal area because of its rarity and unusual location. In addition, our patient also had some rare features of NLCS, such as recurrent in nature, presence of foul-smelling discharge, and comedo-like plugs on the lesions.
Keywords: Nevus lipomatosus cutaneous superficialis, adipocytes, comedo like lesions
INTRODUCTION
Nevus lipomatosus cutaneous superficialis (NLCS) is an uncommon benign hamartomatous condition characterized by the presence of mature ectopic adiopocytes in the dermis. It was first reported by Hoffman and Zurhelle in 1921.[1] Clinically it is classified into two forms.[2,3] The classical form is characterized by groups of multiple, non-tender, soft, pedunculated, cerebriform, yellowish or skin-colored papules, nodules, or plaques. The other form of NLCS clinically manifests as a solitary dome-shaped or sessile papule. The classical NLCS is mostly reported to involve the pelvic or gluteal region. We report here a case of adult-onset classical NLCS on perianal area because of its rarity and unusual location. In addition, our patient also had some rare features of NLCS, such as recurrent in nature, presence of foul-smelling discharge, and comedo-like plugs on the lesions.
CASE REPORT
A 26-year-old man presented to the dermatology outpatient department with a well-defined multiple smooth, soft, and non-tender nodular growths over his perianal area for the preceding 2 years. He gave a history of occasional foul-smelling discharge from the lesion. Similar kind of lesions also occurred 5 years ago for which he was operated. He reported that his sister also suffered similar complaints.
Examination revealed multiple oblong-shaped, yellowish to skin-colored, cerebriform nodular lesions measuring 1.5 cm × 1.2 cm over the perianal area [Figure 1]. Surface of the lesions was studded with multiple open comedones [Figure 2]. A few discrete, soft, yellowish papules were also scattered around the lesions. There was no associated hypertrichosis, café-au-lait or hypopigmented macules. There was no tenderness, ulceration, or induration. There was no regional lymphadenopathy. Systemic examination normal. Routine laboratory examination of blood, urine and stool was within normal limits. Histopathologic examination [Figure 3] of the incisional biopsy specimen showed aggregates of mature adipocytes around the dermal blood vessels, eccrine glands, and between the collagen bundles. Based on the clinical and histopathologic features, a diagnosis of the classical variety of NLCS was made. The patient was referred to the plastic surgery department for surgical excision.
Figure 1.

Clinical photograph showing well-defined multiple smooth, nodular growths over perianal area of the case reported
Figure 2.

Clinical photograph showing the surface of the lesions studded with multiple open comedones
Figure 3.
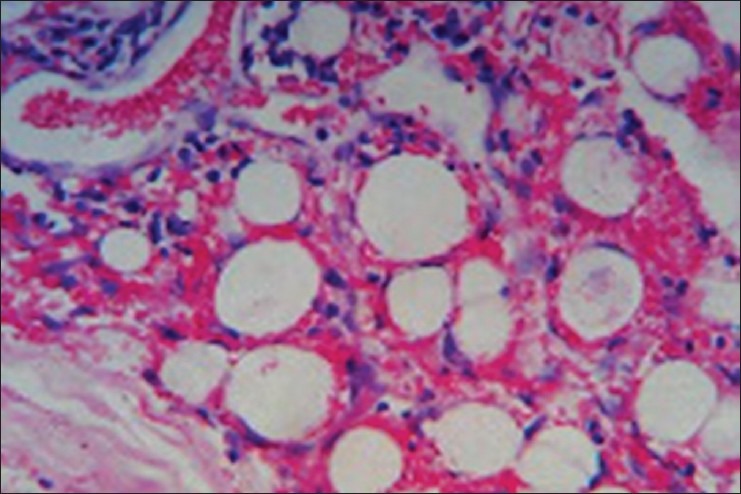
Histopathologic slide showing aggregates of mature adipocytes around the dermal blood vessels
DISCUSSION
The classical form of NLCS is usually unilateral (rarely bilateral as seen in our case) and may be band-like, linear, or zosteriform in distribution.[2,3] When there are multiple papules, they usually appear simultaneously and vary in size. Although some lesions continue to progress for many years, once formed, they usually remain static. Occasionally, they may ulcerate, probably owing to external trauma or ischemia.[4] Foul-smelling discharge, as seen in our patient, has been rarely reported.[2]
There are sporadic case reports of coexistent anomalies in the form of café-au-lait macules and scattered leucoderma.[5] Increased hairiness and comedo-like lesions[4] on the surface of the NLCS have also been reported, though rarely. Our patient had comedo-like lesions. The classic variety of NLCS is either present at birth or can arise at any other time within the first two decades of life.[6,7] Recurrence, as seen in our patient, has rarely been reported. This lesion rarely ulcerates. Thus, our case reflects some rare features of classical NLCS such as recurrence, presence of ulceration (foul-smelling discharge), and comedo-like plugs on the surface.
The histopathology of NLCS usually shows a normal or slightly attenuated epidermis associated with a dermal proliferation of mature adipocytes in the reticular dermis that may extend to the papillary dermis. The adipocytes most commonly form small aggregates around blood vessels or eccrine glands, but may also be present as solitary adipocytes between collagen bundles. The proportion of the dermal fat is variable, ranging from less than 10% of the dermis to over 50%.[8] The adipocytes may show connections to the underlying subcutaneous fat or be separated from the subcutis by collagen. Less commonly, spindle cells representing immature fat cells may also be present.
NLCS should be differentiated from nevus sebaceous, skin tags, neurofibroma, lymphangioma, hemangioma, and focal dermal hypoplasia (Goltz syndrome). Histopathologic evaluation usually helps in the differentiation. No fat cells are present in the dermis in the case of skin tags. Similar dermal collections of adipocytes on histopathologic examination are also present in some melanocytic nevi, pedunculated lipofibromas, and in Goltz syndrome. Lipofibromas contain fat cells, but no skin appendages, in the dermis. In the case of Goltz syndrome, there is an absence of collagen in the atrophic dermis and skin appendages are absent.
The precise etiopathogenesis of NLCS is not understood. There is no specific explanation behind the predilection of the lesions for the pelvic area.[9,10] Deposition of adipose tissue may be caused by the degenerative changes in dermal collagen and elastic tissue.[3,10] The proposed pathogenesis of NLCS includes adipose metaplasia in dermal connective tissue, developmental displacement of adipose tissue; alternatively, the lesions could be explained by the possible origin of adipocytes from the pericytes of dermal vessels.[11]
Treatment is not necessary other than for cosmetic reasons.[7] Systemic abnormalities and malignant changes have not been associated with NLCS. Excision is curative and recurrence after surgery is rare.[2]
ACKNOWLEDGMENT
The authors are grateful to Dr. Parasnuwal, Professor, Department of Pathology, JLN Medical College, Ajmer, for her support.
Footnotes
Source of Support: Nil
Conflict of Interest: No.
REFERENCES
- 1.Hoffmann E, Zurhelle E. Ubereinen nevus lipomatodes cutaneous superficialis der linkenglutaalgegend. Arch Dermatol Syph. 1921;130:327–33. [Google Scholar]
- 2.Yap FB. Nevus lipomatosus superficialis. Singapore Med J. 2009;50:e161–2. [PubMed] [Google Scholar]
- 3.Buch AC, Panicker NK, Karve PP. Solitary nevus lipomatosus cutaneous superficialis. J Postgrad Med. 2005;51:47–8. [PubMed] [Google Scholar]
- 4.Dhar S, Kumar B, Kaur I. Naevus lipomatosus superficialis of Hoffman and Zurhelle. Indian J Dermatol Venereol Leprol. 1994;60:39–40. [Google Scholar]
- 5.Khandpur S, Nagpal SA, Chandra S, Sharma VK, Kaushal S, Safaya R. Giant nevus lipomatosus cutaneous superficialis. Indian J Dermatol Venereol Leprol. 2009;75:407–8. doi: 10.4103/0378-6323.53149. [DOI] [PubMed] [Google Scholar]
- 6.Brenn T. Neoplasms of subcutaneous fat. In: Wolf K, Goldsmith LA, Katz SI, Gilcrest BA, Paller AS, Leffel DJ, editors. Fitzpatrick's dermatology in general medicine. 7th ed. New York: Mcgraw-Hill; 2008. pp. 1190–8. [Google Scholar]
- 7.Takashima H, Toyoda M, Ikeda Y, Kagoura M, Morohashi M. Nevus lipomatosus cutaneous superficialis with perifollicular fibrosis. Eur J Dermatol. 2003;13:584–6. [PubMed] [Google Scholar]
- 8.Ragsdale BD. Tumors with fatty, muscular, osseous, and/ or cartilaginous differentiation. In: Elder DE, Elenitsas R, Jhonson BL, Murphy GF, Xu X, editors. Lever's histopathology of the skin. 10th ed. New Delhi: Wolters Kluwer- Lippincott Williams and Wilkins; 2009. pp. 1057–106. [Google Scholar]
- 9.Atherton DJ, Moss C. Naevi and other developmental defects. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. 7th ed. Oxford: Blackwell Sciences; 2004. pp. 15.1–15.114. [Google Scholar]
- 10.Metin A, Calka O, Akpolat N. Nevus lipomatosus cutaneous superficialis (Hoffmann-Zurhelle) Eastern J Med. 2001;6:26–8. [Google Scholar]
- 11.Thappa DM, Sharma RC, Lal S, Logani KB. Naevus lipomatosus cutaneous superficialis : Report of 2 cases. Indian J Dermatol Venereol Leprol. 1992;58:27–9. [Google Scholar]