

Abstract
Objective. To determine the prevalence and impact of autoimmune thyroid disease (AITD) in patients with rheumatoid arthritis (RA). Methods. Eight-hundred patients were included. The association between AITD and RA was analyzed was analyzed by bivariate and multivariate analysis. In addition, a literature review was done focusing on geographical variations. Results. In our cohort the prevalence of AITD was 9.8% while the presence of antibodies was 37.8% for antithyroperoxidase enzyme (TPOAb) and 20.8% for antithyroglobulin protein (TgAb). The presence of type 2 diabetes, thrombosis, abnormal body mass index, and a high educational level was positively associated with AITD. The literature review disclosed a geographical variation of AITD in RA ranging from 0.5% to 27%. Autoantibody prevalence ranges from 6% to 31% for TgAb, 5% to 37% for TPOAb, and from 11.4% to 32% for the presence of either of the two. Conclusion. AITD is not uncommon in RA and should be systematically assessed since it is a risk factor for developing diabetes and cardiovascular disease. These results may help to further study the common mechanisms of autoimmune diseases, to improve patients' outcome, and to define public health policies. An international consensus to accurately diagnose AITD is warranted.
1. Introduction
Autoimmune thyroid disease (AITD) is a term used to bring together a group of pathologies that has thyroid dysfunction and an autoimmune response against this endocrine organ as its hallmark [1, 2]. However, being a group of autoimmune diseases (ADs) clustered together, the clinical presentation varies among these diseases; it can be divided into those that cause hypothyroidism, hyperthyroidism, or both [3].
As organ specific ADs, this group of pathologies exhibits an autoantibody profile that may be composed of (1) antibodies directed against the thyroperoxidase enzyme (TPOAb), (2) antibodies directed against thyroglobulin protein (TgAb), and (3) antibodies directed against thyrotropin receptor (TSHrAb). In this last case, the antibodies can either block or enhance the receptor's activity. Furthermore, there is a T or B lymphocytic response that prevails and, ultimately, this will define the pathology that becomes manifest. Generally, T lymphocytes are the main cell type infiltrating the gland in Hashimoto's thyroiditis while a B response predominates and determines the presence of Grave's disease [3].
In general terms, those diseases where the clinical presentation is mainly a hypothyroid state include Hashimoto's thyroiditis. As originally described by Akaru Hashimoto in 1912 goiter was associated with this disease though today it may or may not be. The other disease is atrophic thyroiditis which is found with hypothyroidism in the absence of goiter. Conversely, Grave's disease, described by Robert Graves in 1835, is manifested by a hyperthyroid state that can be associated with diffuse goiter and sometimes with exophthalmos. Postpartum thyroiditis occurs in the first postpartum year and it may start with a hyperthyroid state and end with a hypothyroid state that can be transient or permanent [4].
The prevalence of AITD in the general population varies between countries. A prevalence has been described of 5 to 15% in women and 1–5% in men [5]. The prevalence of thyroid autoantibodies has also been described. Hollowell et al. [6] described a prevalence of 13% for TPOAb and 11.5% for TgAb among the general population. This prevalence rises in spontaneously hypothyroid patients [7]. In other words, AITD can be regarded as the most common autoimmune endocrine disease.
Rheumatoid arthritis (RA), in turn, is a chronic, complex, and heterogeneous AD, in which there is a response directed towards the diarthrodial joints producing symmetric polyarthritis with progressive damage to the joints, bone destruction, and extra-articular manifestations (EAMs) such as cutaneous nodules, lung involvement, cardiovascular disease (CVD), episcleritis, and so forth. All of these lead to disability [8, 9], an increase in comorbidities [10], and premature mortality. Thus, the autoimmune compromise is systemic as opposed to AITD which is organ specific [11].
RA is the most common inflammatory arthropathy worldwide. The disease is three times more frequent in women than men with a prevalence of 0.5–1.0% in industrializedcountries [12, 13] and less than 0.5% in Latin America [12, 14]. This region has a high admixture of cultures and ethnicities and thus RA genotypes and phenotypes differ between and within countries [15]. However, the prevalence rises with age and is highest in women older than 65 years [11]. The annual incidence is highly variable (12 to 1,200 per 100,000 population) [16] and is dependent on a variety of factors including gender, environmental (e.g., smoking [17], infectious diseases [18, 19]), ethnicity, and age [16]. With the exception of certain native populations, RA affects all populations worldwide. These variations are indicative of different genetic risks and hormonal exposures [20].
For several decades an increased occurrence of thyroid disorders in patients suffering from RA has been documented—both autoimmune and nonautoimmune in nature [21–24]. In addition, [25] rheumatologic and nonrheumatologic manifestations of AITD have been described. Within these manifestations, it is noteworthy that the most common symptoms are polyarthralgia and unclassified arthritis, which are the main features of RA.
ADs share similar mechanisms [12, 26–28]. In clinical practice some conditions support these commonalities. One of these corresponds to polyautoimmunity, which is defined as the presence of more than one AD in a single patient [29]. The multiple autoimmune syndrome (MAS), a form of polyautoimmunity, corresponds to the coexistence of three or more well-defined ADs [30]. The importance of these terms is due to the fact that patients with polyautoimmunity or MAS may have a modified disease course (with a worse prognosis or a better one) and a modified clinical presentation. Moreover, first degree relatives (FDR) of these patients are at increased risk of developing an AD [31]. Several studies have consistently mentioned association and clustering between ADs [32, 33].
Genetic background is, therefore, an important aspect in autoimmunity. Genetic risk factors shared among diseases have been described and AITD and RA are no exception [25, 34, 35]. Nevertheless, the etiology of ADs is complex in nature, which means that genetic, epigenetic, and environmental factors are responsible for the occurrence of these diseases. For certain ADs, genetic factors have been consistently found to be more important than environmental factors and vice versa [1, 2, 36, 37].
In AITD, numerous genes have been found to confer risk for the disease including HLA gene complex, CD40, CTLA4, PTPN22, TSH receptor gene, and thyroglobulin gene [2, 38–40]. While the term AITD lumps Graves' disease and Hashimoto's thyroiditis together, in the case of the former, genetic factors appear to be more important whereas the reverse is true in the latter [1, 2, 36, 37]. CD40, CTLA4, and PTPN22 genes as well as the HLA gene complex have also been implicated in the pathogenesis of RA [41]. In addition, shared environmental factors such as smoking [17] have been implicated in numerous studies as risk factors for AITD and for RA [2, 36].
Although AITD and RA share common physiopathological mechanisms, the connection between AITD and RA is a topic with no definite results so far. In Latin America and other regions, this association has not been thoroughly explored. It is important to establish if the presence of AITD in RA is linked with EAMs including CVD and the presence of a worse prognosis for RA (e.g., presenting erosions) [42, 43]. As a center for autoimmune research established in Latin America, we are mainly interested in unraveling the association between these diseases, to look for information from our region and to establish a solid base on which future research in this area may hold its ground.
The purposes of the study are (1) to determine the prevalence of AITD within an RA cohort of Colombian patients and determine the differences between these two groups regarding the prognostic features of RA as well as (2) to analyze the current information concerning the prevalence of AITD in RA patients and to evaluate any deviations on RA course due to AITD presence.
2. Patients and Methods
2.1. Study Population
This was a cross-sectional, analytical study in which 800 consecutive Colombian patients with RA were included. The subjects were being seen at the Center for Autoimmune Diseases Research (CREA) at the Universidad del Rosario in Bogota and Medellin between February 1996 and April 2012. All of them fulfilled the 1987 American College of Rheumatology classification criteria [44] and had AITD status investigated. The study was conducted in compliance with Act 008430/1993 by the Ministry of Health of the Republic of Colombia. The institutional review board of the Universidad del Rosario approved the study design.
Each patient was evaluated by a rheumatologist. The information on patient sociodemographic and cumulative clinical and laboratory data was obtained by interview, physical examination, and chart review. A household description was obtained by questionnaire and a clinical evaluation of the affected family members was done using the same methodology as above. All data were collected in an electronic and secure database.
The sociodemographic variables included current age, age at RA onset, disease duration, educational status, socioeconomic status (SES), current occupational status, smoking habits, coffee consumption, and physical activity. The following are the definitions of these variables: age at onset: age at which patients began to suffer from pain, typical morning stiffness (more than 1 hour), and symmetrical inflammation of hand and/or foot joints; disease duration: difference between age at onset and the date of first participation in the study. It was dichotomized as having either more or less than 10 years of disease as our group had previously reported this to be a risk factor for CVD [45]. Educational level was recorded as years of education; the cohort was split into two groups with one group including those with less than 9 years of education (including preschool, primary, and the first 2-3 years of high school) and the other more than 9 years of education. This breakdown was based on the General Law of Education in Colombia [46, 47]. SES was categorized on the basis of national legislation and was divided into high status (3 to 6) and low status (1 and 2). For occupational status we focused on establishing if the patient worked on household duties exclusively.
Regarding clinical variables, we evaluated polyautoimmunity, MAS, familial autoimmunity, erosions, comorbidities, EAMs, systolic and diastolic blood pressure, body mass index (BMI), and waist circumference. The following are the definitions of these variables: polyautoimmunity and MAS as stated above. However, we evaluated polyautoimmunity as a variable without taking into account the presence of AITD. Familial autoimmunity was defined as the presence of any diagnosed AD in another FDR of the proband. We evaluated 6 ADs on the basis of international criteria namely: systemic lupus erythematosus (SLE), AITD, Sjögren's syndrome (SS), antiphospholipid syndrome (APS), psoriasis (PSO), and vitiligo (VIT) [48]. It is important to note that there are no international criteria for the diagnosis of AITD. These cases were classified on the basis of an abnormal thyrotropin (TSH) test, or history of thyroid hormone therapy, and the presence of either TPOAb or TgAb.
Erosions were defined as having at least one point on the Sharp/van der Heijde classification [49]. EAMs was defined as the presence of at least one of the following: skin ulcerations, nodules, episcleritis, vasculitis, neuropathy, pleural effusion, pulmonary hypertension or embolism, and CVD. The latter was categorized as positive if any of the following variables were present: hypertension (defined as having blood pressure >140/90 mm Hg or using antihypertensive medication) [50], coronary artery disease, occlusive arterial disease, carotid disease, or thrombosis.
The patients were asked about the presence of diabetes mellitus, defined as having a fasting plasma glucose level >7 mmol/L (126 mg/dL) or taking antidiabetic medication at the time of the assessment [51]. Diagnosis of dyslipidemia was given if patient had hypercholesterolemia, defined as taking lipid-lowering medication or having a fasting plasma total cholesterol >200 mg/dL, HDL <40 mg/dL, hypertriglyceridemia >150 mg/dL, or LDL cholesterol >100 mg/dL [52, 53]. Anemia was diagnosed if current hemoglobin was <12 g/dL, gastritis only if evidenced by esophagogastroduodenoscopy, periodontal disease was self-reported, and renal disease if serum creatinine measurement had values above 1.2 mg/dL.
Systolic and diastolic blood pressures were measured twice with at least 15 minutes between measurements and the average was recorded. A BMI ≥25 kg/m2 (overweight and obesity) was considered abnormal [54]. Abnormal values of waist circumference (>102 cm for men, >88 cm for women) and waist-to-hip ratio (WHR > 0.9 for men, >0.85 for women) were considered indicators of abdominal obesity. Waist circumference was measured around the narrowest point between ribs and hips after exhaling and viewed from the front. Hip circumference was measured at the point of maximum extension of the buttocks when viewed from the side [55]. Abnormal WHR values are consistent with National Cholesterol Education Program Adult Treatment Panel III and World Health Organization definitions [56].
Medical treatment included the current or past use of methotrexate and other disease modifying antirheumatic drugs (DMARDs) such as sulfasalazine, D-penicillamine, azathioprine, cyclosporine, gold salts and leflunomide, steroid therapy, antimalarials (cloroquine, hydroxychloroquine), and biologic therapy (rituximab, infliximab, etanercept, abatacept, adalimumab, tocilizumab). Patients and their past medical records were evaluated for the current or past use of aspirin or hormone replacement therapy as well.
Relevant laboratory variables were also registered including erythrocyte sedimentation rate (ESR), hemoglobin levels, white blood cell count, platelet count, and serum high sensitive C-reactive protein (CRP) levels. Autoantibodies such as rheumatoid factor (RF) and anticyclic citrullinated peptide (anti-CCP), TPOAb, and TgAb antibodies were taken from the patient's clinical record. They were measured with enzyme-linked immunosorbent assay (QUANTA-Lite, INOVA, San Diego, CA, USA) following the manufacturer's protocol. Antibodies directed against either TSH receptor or thyroid hormones (THAb) were not assessed in the current study.
2.2. Statistical Analysis
First, univariate analysis was done on all members of this new cohort. Categorical variables were analyzed by frequencies. Kolmogorov-Smirnov normality test was done to evaluate normality for quantitative, continuous variables. Parametric data are expressed as mean and standard deviation (SD), and nonparametric data are described as median and interquartile range (IQR).
Second, bivariate analyses done in search of the association between different characteristics of RA and AITD were verified using chi-square test or Fisher's exact test when the factors were dichotomous. Parametric values were analyzed by Student's t-test. Nonparametric values were analyzed by Mann-Whitney U-test. A P value of less than 0.05 was considered significant.
A multivariate binomial logistic regression model was fit with AITD as the dependent variable. As independent variables, the model included those that were significantly associated in the bivariate analyses and those that were biologically and clinically plausible for this relationship. The adequacy of logistic models was assessed using the Hosmer-Lemeshow goodness-of-fit test. The Nagelkerke R 2 (i.e., pseudo-R 2) was used to estimate the percentage of variance explained by the model. Adjusted odds ratios (AORs) were calculated with 95% confidence intervals (CIs). Statistical analyses were done by using the Statistical Package for the Social Sciences (SPSS, v.20, Chicago, IL).
2.3. Literature Search
We did a literature review with reference to polyautoimmunity between RA and AITD. The search was done using the following databases: PubMed, SciELO, EMBASE, Virtual Health Library (BIREME and LILACS), and Google Scholar.
Limits regarding language, age (all adults), and humans were taken into account. No limits regarding publication date was used. The following Medical Subject Headings (MeSH terms) were used: “Thyroiditis, Autoimmune” OR “Graves Disease” AND “Arthritis, Rheumatoid”. In addition, each MeSH term was translated into DeCS (Health Sciences Descriptors), a tool that makes it possible to navigate between records and sources of information through controlled concepts organized in Spanish and English. This was done in order to search SciELO, BIREME, and Virtual Health Library databses. The DeCs terms and key words used were “artritis reumatoide” AND (“tiroiditis autoinmune” OR “enfermedad de graves”).
The inclusion criteria were the following: only articles that used accepted classification criteria for RA had a definite diagnosis of AITD (presence of antithyroid antibodies and thyroid dysfunction), and that included RA as well as AITD. They were divided based on prevalence of AITD, prevalence of antithyroid antibodies, radiographic progression, and extra-articular manifestations. Articles were excluded if they were animal models, dealt with juvenile rheumatoid arthritis, or with other autoimmune diseases other than RA or AITD.
Those references from the articles that seemed to be relevant for our review were hand searched. Titles and abstracts were reviewed by two independent reviewers in search of eligible studies.
3. Results
3.1. Colombian Cohort
There were 81.3% women and we found that the prevalence of AITD was 9.8%. The presence of antibodies was 37.8% for TPOAb and 20.8% for TgAb. Characteristics of the cohort are illustrated in Table 1. Due to the nature of this study (i.e., cross-sectional) and the cohort beginning date (i.e., 1996) there is a proportion of patients in whom not all the data were assessed. Health assessment questionnaire (HAQ) and disease activity score (DAS28) were calculated on study entry date, but were not taken into account in the analyses due to their variability over time.
Table 1.
Characteristics of 800 patients with RA.
| Characteristic | |
|---|---|
| Age (years) | 51.92 (12.19)a |
| Age at onset (years) | 39.58 (12.35)a |
| RA duration (years) | 10 (14)b |
| Educational level (years) | 11 (9)b |
| Body mass index | 24 (5.8)b |
| DAS28 | 3.63 (2.12)b |
| HAQ | 1.05 (1.31)b |
|
| |
| Sociodemographic | n/N (%) |
|
| |
| Female | 650/800 (81.3) |
| Low educational level | 264/692 (38.2) |
| Low socioeconomic status | 234/780 (30.0) |
| Current smoking | 85/768 (11.1) |
| Household duties | 254/684 (37.1) |
|
| |
| Clinical aspects | |
|
| |
| Type 2 diabetes | 32/737 (4.3) |
| Dyslipidemia | 184/752 (24.5) |
| Hypertension | 208/752 (27.7) |
| Thrombosis | 39/738 (5.3) |
| Cardiovascular disease | 173/781 (22.2) |
| Body mass index > 25 | 394/681 (57.9) |
| Abdominal obesity | 460/683 (67.4) |
| Aspirin use | 105/653 (16.1) |
| Abnormal cholesterol | 179/333 (53.8) |
|
| |
| RA characteristics | |
|
| |
| Disease duration > 10 years | 393/703 (55.9) |
| Erosions | 349/451 (77.4) |
| EAMs with CVD | 402/793 (50.7) |
| Rheumatoid factor+ | 573/717 (79.9) |
| Anti CCP+ | 312/384 (81.3) |
| Methotrexate | 702/794 (88.4) |
| DMARD (any) | 783/794 (98.6) |
| Antimalarials | 633/793 (79.8) |
| Steroids | 705/793 (88.9) |
| Biological Agents | 276/794 (34.8) |
|
| |
| Autoimmunity | |
|
| |
| Autoimmune thyroid disease | 78/800 (9.8) |
| Systemic lupus erythematosus | 11/709 (1.6) |
| Sjögren's syndrome | 24/800 (3.0) |
| Polyautoimmunity | 113/800 (14.1) |
| Polyautoimmunityc | 35/800 (4.8) |
| MAS | 17/714 (2.4) |
| Familial autoimmunity FDR | 104/800 (13.0) |
| ANAs+ | 310/448 (69.2) |
| Anti Ro+ | 43/287 (15.0) |
| Anti La+ | 20/285 (7.0) |
| TPOAb+ | 51/135 (37.8) |
| TgAb+ | 26/125 (20.8) |
ANAs: antinuclear antibodies; CCP: cyclic citrullinated peptide; CRP: C-reactive protein; CVD: cardiovascular disease; DAS28: disease activity score; DMARD: disease modifying antirheumatic drugs; EAM: extra-articular manifestations; ESR: erythrocyte sedimentation rate; FDR: first degree relatives; HAQ: health assessment questionnaire; MAS: multiple autoimmune syndrome; RA: rheumatoid arthritis; TgAb: anti-thyroglobulin; TPOAb: anti-thyroperoxidase enzyme.
a Mean (standard deviation).
b Median (interquartile range).
c Without taking AITD into account.
In the bivariate analysis, significant differences among women, educational level, abnormal BMI, diabetes, thrombosis, hypercholesterolemia, presence of RF, and use of methotrexate were observed. Tables 2 and 3 show the relationships explored in the study population.
Table 2.
Bivariate analysis of categorical variables.
| Characteristic | RA with AITD | RA without AITD | OR | 95% CI | P |
|---|---|---|---|---|---|
| MAS | 10/61 (16.39) | 7/650 (1.08) | 18.01 | 6.57–49.30 | <0.0001 |
| Type 2 Diabetes | 12/72 (16.67) | 20/665 (3.01) | 6.45 | 3.00–13.83 | 0.008 |
| Methotrexate | 75/78 (96.15) | 627/716 (87.57) | 3.54 | 1.09–11.49 | 0.024 |
| Female | 72/78 (92.31) | 575/719 (79.97) | 3.01 | 1.2–7.05 | 0.008 |
| Thrombosis | 9/71 (12.68) | 30/667 (4.50) | 3.01 | 1.4–6.78 | 0.003 |
| Anti La+ | 6/39 (15.38) | 14/246 (5.69) | 3.01 | 1.08–8.3 | 0.04* |
| Anti Ro+ | 11/39 (28.21) | 32/248 (12.90) | 2.65 | 1.20–5.84 | 0.013 |
| Abnormal BMI | 37/69 (53.60) | 250/612 (40.8) | 1.67 | 1.01–2.76 | 0.042 |
| Low educational level | 15/59 (25.4) | 249/633 (39.3) | 0.52 | 0.28–0.96 | 0.035 |
| Abnormal cholesterol | 17/43 (39.53) | 162/290 (55.86) | 0.51 | 0.26–0.99 | 0.045 |
| RF+ | 50/73 (68.49) | 523/644 (81.21) | 0.50 | 0.29–0.85 | 0.01 |
| Polyautoimmunity | 78/78 (100) | 35/722 (4.8) | N/A | N/A | N/A |
| TPOAb+ | 51/54 (94.44) | 0/81 (0.00) | N/A | N/A | N/A |
| TgAb+ | 26/50 (52.00) | 0/75 (0.00) | N/A | N/A | N/A |
*Fisher's exact test.
95% CI: 95% confidence interval; AITD: autoimmune thyroid disease; BMI: body mass index; N/A: not assessed; OR: odds ratio; RA: rheumatoid arthritis; RF: rheumatoid factor; TgAb: anti-thyroglobulin; TPOAb: anti-thyroperoxidase enzyme.
Table 3.
Bivariate analysis of continuous variables.
| Characteristic | RA with AITD | RA without AITD | P |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age | 52.26 ± 12.39 | 51.88 ± 12.24 | 0.029 |
| Median ± IQR | Median ± IQR | ||
| Educational level (y) | 14 ± 7 | 11 ± 9 | 0.006 |
| Body mass index | 25.5 ± 6.3 | 23.9 ± 5.9 | 0.006 |
AITD: autoimmune thyroid disease; IQR: interquartile range; RA: rheumatoid arthritis; SD: standard deviation.
Table 4 depicts the multiple logistic regression analysis. Adjusted for gender and RA duration, the presence of diabetes, thrombosis, and abnormal BMI were positively associated in patients with polyautoimmunity (i.e., between RA and AITD). We found that there is a lower AITD frequency in the lowest educational level than in the highest one. This is also true when antimalarials are used (Table 4).
Table 4.
Associated factors with AITD in RA (multivariate analyses).
| Characteristic | B | AOR | 95% CI | P |
|---|---|---|---|---|
| Thrombosis | 3.19 | 24.41 | 2.73–218.43 | 0.004 |
| Diabetes | 2.61 | 13.61 | 1.61–114.96 | 0.016 |
| BMI > 25 | 1.44 | 4.22 | 1.19–14.93 | 0.025 |
| Rheumatoid factor+ | 0.95 | 2.58 | 0.33–19.88 | 0.36 |
| Methotrexate use | 0.90 | 2.48 | 0.27–22.36 | 0.418 |
| Female | 0.46 | 1.58 | 0.34–7.42 | 0.56 |
| Abnormal cholesterol | −1.22 | 0.29 | 0.08–1.10 | 0.069 |
| Duration disease > 10 years | −1.32 | 0.27 | 0.07–1.05 | 0.058 |
| Low educational level | −1.82 | 0.16 | 0.03–0.88 | 0.036 |
| Antimalarials | −2.29 | 0.10 | 0.02–0.57 | 0.01 |
95% CI: 95% confidence interval; AOR: adjusted odds ratio; BMI: body mass index.
3.2. Literature Search Results
The searches in Medline, EMBASE, LILACS, and BIREME brought up 788 articles. Forty-nine were selected for further analysis based on their title and abstract. Using information from references, other studies that met the selection criteria were chosen. The articles were divided by measured outcomes that were considered relevant: radiographic progression, genetic analysis, prevalence of AITD, and prevalence of TPOAb or TgAb.
3.2.1. Prevalence of AITD (Figure 1)
Figure 1.
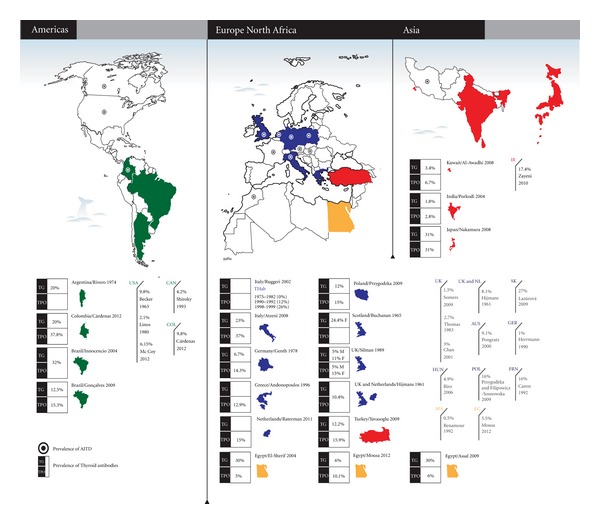
Prevalence of AITD and antibodies worldwide.
Seventeen studies identified RA as index disease and determined AITD prevalence in this group [23, 57–72]. The prevalence in RA cases ranged from 0.5% in Morocco [58] to 27% in Slovakia [71]. Within the studies analyzed, 10 studies were from Europe [23, 63–71] with prevalence ranging from 1% in Germany [65] to 27% in Slovakia [71]. Four studies were from the North American region [59–62] where prevalence ranged from 2.1% [61] to 9.8% [60]. Only two studies were from Africa were retrieved [57, 58] and one from the Middle East [72]. The search did not result in any article about Latin American or Asian populations. Table 5 gives a detailed view of the data.
Table 5.
Prevalence of AITD diagnosis in RA patients.
| Author publication date |
Location | Study population | Diagnostic criteria of RA | Diagnostic criteria of AITD | Number of Cases | Frequency | Prevalence % |
|---|---|---|---|---|---|---|---|
| Africa | |||||||
| Mousa et al. 2012 [57] | Egypt | F: 80% A: 36.3 | ACR 1987 | Lab. | 217 | 12 | 5.5 |
| Benamour et al. 1992 [58] | Morocco | F: 87.4% A: 34 | ARA | N/A | 404 | 2 | 0.5 |
| America | |||||||
| Cárdenas et al. 2012* | Colombia | F: 81.3% A: 51.92 | ACR 1987 | Lab. | 800 | 78 | 9.8 |
| Shiroky et al. 1993 [59] | Canada | F: 76. A: 58.7 | ARA | Biopsy | 119 | 7 | 4.2 |
| Becker et al. 1963 [60] | USA | N/A | ARA | Histology | 51 | 5 | 9.8 |
| Linos et al. 1980 [61] | USA | F: 74.1% A: N/A | ARA | N/A | 521 | 11 | 2.1 |
| McCoy et al. 2012 [62] | USA | F: 69% A: 55.8 ± 15.7 | ACR | Lab. | 650 | 40 | 6.1 |
| Europe | |||||||
| Hijmans et al. 1961 [23] | Europe# | N/A | ARA 1959 | N/A | 86 | 7 | 8.1 |
| Pongratz et al. 2000 [63] |
Austria | F: 88.3% A: N/A | ARA | N/A | 383 | 35 | 9.1 |
| Caron et al. 1992 [64] | France | N/A | N/A | N/A | 131 | 21 | 16 |
| Herrmann et al. 1990 [65] | Germany | F: 86% A: N/A | N/A | US, Lab. | 201 | 2 | 1 |
| Biro et al. 2006 [66] | Hungary | N/A | ARA | Lab. | 185 | 9 | 4.9 |
| Somers et al. 2009 [67] | UK | F: 92% A: N/A | GPRD | GPRD | 22888 | 337 | 1.5 |
| Thomas et al. 1983 [68] |
UK | F: N/A A: 52 | N/A | NR | 295 | 8 | 2.7 |
| Chan et al. 2001 [69] | UK | F: 90% A: N/A | ARA | Lab. | 64 | 2 | 3.0 |
| Przygodzka and Filipowicz-Sosnowska 2009 [70] |
Poland | F: 100% A: 56 ± 13 | ACR | Lab. | 100 | 16 | 16.0 |
| Lazúrová et al. 2009 [71] | Slovakia | F: N/A A: 52.2 ± 2 | N/A | US, Lab. | 68 | 19 | 27.0 |
| Middle East | |||||||
| Zayeni et al. 2010 [72] | Iran | F: 87.1% A: 49.05 | N/A | Lab. Clinical examination | 224 | 39 | 17.4 |
#Location not stated. Collaboration between the UK and The Netherlands.
*Current series.
N/A: Not available; F: Proportion of females; A: Age at time of assessment (standard deviation); ARA-ACR: RA diagnostic criteria 1987; UK: United Kingdom, US: Ultrasound, USA: United States of America, GPRD: General Practice Research Database; Lab.: Laboratory criteria.
3.2.2. Prevalence of Autoantibodies (Figure 1)
Twenty studies reported the prevalence of autoantibodies against thyroid antigens [23, 57, 70, 73–89]. The prevalence for TgAb ranged from 5% in men from the UK [88] and 6% regardless of gender in Egypt [57] to 31% in RA patients from Japan [79]; the prevalence for TPOAb was within the range of 5% in Egypt [74] to 37% in Italy [80]. This search included 2 studies from Brazil [76, 77] and one from Argentina [75] which were the only countries from Latin America that had published literature on this topic. Some studies did not discriminate the frequency of each autoantibody [23, 76]. Ruggeri et al. [81] show the assessment of THAb at three points in time. Further information can be obtained from Table 6.
Table 6.
Prevalence of TPOAb and TgAb in RA patients.
| Author publication date |
Location | Study population | Number of Cases | Diagnostic | Frequency | Prevalence % | ||
|---|---|---|---|---|---|---|---|---|
| criteria of RA | TPOAb | TgAb | TPOAb | TgAb | ||||
| Africa | ||||||||
| Assal et al. 2009 [73] | Egypt | F: 66.6% A: 26.8 | 30 | ACR 1987 | 2 | 9 | 6.0 | 30.0 |
| El-Sherif et al. 2004 [74] | Egypt | N/A | 20 | N/A | N/A | N/A | 5.0 | 30.0 |
| Mousa et al. 2012 [57] | Egypt | F: 80% A: 36.3 | 217 | ACR 1987 | 22 | 13 | 10.1 | 6.0 |
| America | ||||||||
| Cárdenas et al. 2012* | Colombia | F: 81.3% A: 51.92 | 125–135** | ACR 1987 | 51 | 26 | 37.8 | 20.8 |
| Rivero et al. 1974 [75] | Argentina | N/A | 50 | N/A | N/A | 10 | N/A | 20.0 |
| Innocencio et al. 2004 [76] |
Brazil | N/A | 25 | ACR 1987 | 8 | 32.00 | ||
| Gonçalves et al. 2009 [77] | Brazil | F: 86% A: 50 ± 10 | 72 | ACR 1987 | 11 | 9 | 15.3 | 12.5 |
| Asia | ||||||||
| Porkodi et al. 2004 [78] | India | N/A | N/A | N/A | 21 | 13 | 2.8 | 1.8 |
| Nakamura et al. 2008 [79] | Japan | F: 82.76% A: 61 ± 14 | 29 | N/A | 9 | 9 | 31.0 | 31.0 |
| Europe | ||||||||
| Hijmans et al. 1961 [23] | Europe# | N/A | 86 | ARA 1959 | 9 | 10.4 | ||
| Atzeni et al. 2008 [80] | Italy | F: 81% A: 47 ± 16 | 70 | ACR 1987 | 26 | 16 | 37.0 | 23.0 |
| Ruggeri et al. 2002 [81]≠ | Italy | N/A | N/A | N/A | N/A | N/A | 1975–1982: 0 | |
| 1990–1992: 12 | ||||||||
| 1998-1999: 26 | ||||||||
| Genth et al. 1978 [82] | Germany | N/A | 105 | N/A | 15 | 7 | 14.3 | 6.7 |
| Andonopoulos et al. 1996 [83] | Greece | N/A | 101 | N/A | N/A | N/A | 12.9 | N/A |
| Raterman and Nurmohamed 2012 [84] |
NL | N/A | N/A | ACR 1987 | N/A | N/A | 15 | N/A |
| Magnus et al. 1995 [85] | Norway | N/A | 100 | N/A | N/A | § | ||
| Przygodzka and Filipowicz-Sosnowska 2009 [70] |
Poland | F: 100% A: 56 ± 13 | 100 | ACR 1987 | 15 | 12 | 15.0 | 12.0 |
| Buchanan 1965 [86] | Scotland | F: 100% | N/A | N/A | N/A | N/A | N/A | 24.4 |
| Yavasoglu et al. 2009 [87] | Turkey | F: 82% | 82 | ARA 1959 | 13 | 10 | 15.9 | 12.3 |
| Silman et al. 1989 [88] | UK | N/A | N/A | N/A | N/A | N/A | males: 5 females: 15 | males: 5 females: 11 |
| Middle East | ||||||||
| Al-Awadhi et al. 2008 [89] |
Kuwait | F: 79.1% A: 38.3 | 177 | ACR 1987 | 12 | 6 | 6.7 | 3.4 |
N/A: Not available; F: Proportion of females; A: Age at time of assessment (standard deviation); NL: The Netherlands; UK: United Kingdom; USA: United States of America.
*Current series.
**See text for details.
#Location not stated. Collaboration among UK and NL.
§Compared to the prevalence in the normal population, patients with rheumatoid arthritis have a higher prevalence of both antibodies.
≠Prevalence assessed in three time points. Only valid for thyroid hormone antibodies (THAb).
3.2.3. Extra-Articular Manifestations
In our search CVD was the sole EAMs found. Articles by McCoy et al. [62] and Raterman et al. [21] agreed that the presence of hypothyroidism, including Hashimoto's thyroiditis, is a risk factor for CVD in patients with RA. McCoy and colleagues found a hazard ratio of 2.7 (95% CI: 1.1–6.3) [62].
3.2.4. RA Severity
One full text article and three abstracts were located that dealt with this topic.
4. Discussion
In our cohort the prevalence of AITD was 9.8% while the presence of antibodies was 37.8% for TPOAb and 20.8% for TgAb. Type 2 diabetes (AOR: 13.61; 95% CI: 1.61–114.96; P = 0.016), thrombosis (AOR: 24.4; 95% CI: 2.72–218.42; P = 0.004), and abnormal BMI (AOR: 4.22; 95% CI: 1.19–14.93; P = 0.025) were positively associated in patients with polyautoimmunity (i.e., RA and AITD) while the lowest educational level (AOR: 0.16; 95% CI: 0.03–0.88; P = 0.036) as well as the use of antimalarials (AOR: 0.10; 95% CI: 0.18–0.57; P = 0.01) were negatively associated with this coexistence.
There is a worldwide prevalence of AITD in RA that varies considerably, ranging from 0.5 % in Morocco [58] to 27% in Slovakia [71]. Thyroid-specific antibody prevalence ranges from 6 to 31% for TgAb [57, 79], 5 to 37% for TPOAb [74, 80], and from 10.4 to 32% for the presence of either of the two [23, 76]. This high prevalence variability may be explained by certain factors. Firstly there are difficulties on diagnosing AITD because it relies on the fact that there must be a diagnosis of thyroid dysfunction a priori. However there has been much of a debate regarding how to define hypothyroidism or hyperthyroidism; the normal reference range is not universally accepted and thus authors and clinicians worldwide accept different normal ranges.
The debate is more intense when establishing the normal upper limit for TSH values; several authors have addressed this issue but there has been no consensus [90–96]. Wartofsky and Dickey [91], and the Wickham cohort propose a TSH range around 2.5 IU/mL [97] while Surks et al. [94] and the American Academy of Clinical Endocrinologists (AACE) [98] support a TSH upper limit of 5 IU/ml. Jensen et al. and Hamilton et al. [90, 95] found a normal upper TSH level of 4.1 IU/ml, which is more clinically acceptable in order for initiating therapy. Secondly, the TSH assay methods have changed with time, improving its diagnostic accuracy [96]. This may hold true for other assays. Older studies may have not detected low levels of a given laboratory value and thus report a false negative result. This could explain the results of Ruggeri et al. [81] in which the prevalence of THAb are increasing with time.
A third explanation involves iodine intake. It is well known that iodine has a particular property of inducing autoimmune response against the thyroid [99–101]. Epidemiological studies support this statement as they have found an increasing incidence of AITD, particularly Hashimoto's thyroiditis, with increasing iodine intake (0.2% for low, 1% for normal, and 1.3% for high intake) [48]. Besides, a rise in Hashimoto's thyroiditis prevalence was encountered after adjustment of iodine supplementation [102]. Given this, and accepting the fact that iodine supplementation/intake is not evenly distributed among countries [103], it is plausible to think that this may also contribute to the heterogeneous prevalence of AITD in RA found around the globe.
When polyautoimmunity was assessed without taking into account AITD, a prevalence of 5% was found, which is relatively high. This is linked to a positive association between Ro and La antibodies and AITD. Both of these findings are supported by the “Autoimmune Tautology” [27].
Surprisingly, the association between AITD and EAMs did not become apparent in the literature search nor in our cohort. Although CVD is linked to the presence of EAMs [104], an increased cardiovascular risk is observed within this subset of patients with an OR of 3.1 in the bivariate analysis and an AOR of 24 when adjusted for potential confounders and variables of clinical interest. This is the reason CVD is considered an EAM and a major predictor of poor prognosis [16] and increased RA medical costs [105].
The aforementioned relationship found is supported by other studies. McCoy et al. [62] found that Hashimoto's disease had an HR of 2.1 (95% CI: 1.2–3.8) for CVD in patients with RA in a retrospective cohort. By perpetuating an inflammatory state RA is also considered as a novel risk factor for CVD. This has been shown in a large number of reports [22, 106, 107] and was also demonstrated in our cohort previously [45, 104].
Furthermore, higher ESR, CRP, and TNF-α titers, the occurrence of RA vasculitis, and RA lung disease emerged as strong disease-specific predictors of cardiovascular mortality. This also holds even after accounting for demographics, traditional cardiovascular risk factors such as diabetes, sedentary lifestyle, obesity, smoking, and relevant comorbidities [108]. It has been proposed that an altered lipid profile is responsible for excess of CVD in patients with AITD [109]. However, Taddei et al. [110] in a case-control setting compared patients with subclinical hypothyroidism and autoimmune thyroiditis versus controls. They found that low grade systemic inflammation was responsible for endothelial dysfunction and impaired nitric oxide availability independent of lipid profile alterations [111]. Moreover, McCoy et al. [62] found that thyroxine supplementation was significantly associated with CVD, which supports the fact that the administration of this medication does not decrease the occurrence of this outcome. Autoimmunity itself may be an independent risk factor for CVD.
As both diseases increase inflammatory parameters and cytokines and cause endothelial dysfunction, a relationship between polyautoimmunity (RA and AITD) and the occurrence of CVD is not surprising.
Although antimalarial use was not significant in the bivariate analysis, we decided to keep the variable in the multivariate analysis. This is because this medication has been associated with a better cardiovascular outcome, improved glycated hemoglobin in patients with type 2 diabetes mellitus [112], enhanced glycemic control in patients with RA and SLE, and a reduced risk of developing diabetes mellitus in those patients [113, 114] in several reports. Furthermore, these medications influence cardiovascular risk by lowering total cholesterol levels [115, 116], which strengthens the hypothesis that reducing inflammation is important in reducing the risk of CVD in RA patients. This seemed to be the case with our RA patients with AITD.
It is noteworthy that most of the retrieved articles were from Europe followed by North American countries such as United States and Canada. This could be linked to the theory that Hashimoto's thyroiditis is the most frequent cause of spontaneously acquired hypothyroidism in industrialized countries. Few developing countries have data on AITD prevalence. These are Egypt, Iran, and Morocco. The latter reports the smallest prevalence of what we found in our literature search.
Considering thyroid antibodies, the prevalence is also heterogeneous. It is widely accepted that among these thyroid antibodies the most frequent is TPOAb compared to TgAb [6]. This has happened in almost all the studies that reported data on both antibodies [57, 70, 77, 80, 82, 87], and in our cohort. Nonetheless, this is not the case in the article from Japan by Nakamura et al. [79] in which they found the same prevalence for both antibodies. In addition, two studies from Egypt, one by El-Sherif et al. [74] and the other by Assal et al. [73], found an increased prevalence of TgAb, respectively. However, the study by Mousa et al. [57] found a higher prevalence for TPOAb in Egypt. A small sample size in these situations may be the best explanation for these contradictory findings. In Latin America, Rivero et al. [75], in an Argentinean setting, found a prevalence of 20% for TgAb while Gonçalves et al. [77] in Brazil found a prevalence of 15% for TPOAb and 7% for TgAb. Ruggeri et al. [81] demonstrated an increasing prevalence of THAb with time; pathologies different from AITD (RA and SS) exhibit increasing prevalences as well. It is noteworthy that this study also demonstrates that beyond an association of RA with Hashimoto's thyroiditis, antibodies to thyroid hormones (i.e., T3 and T4) may also foster the development of hypothyroidism.
Nevertheless, as the first study in Latin America that describes the relationship, our results do not differ from what has been reported in other latitudes. We report a prevalence of 9.8% of AITD in RA subjects, a TPOAb prevalence of 37.78%, and a TgAb prevalence of 20%. Although a prevalence of TgAb that was similar to Rivero's was found, the antibody prevalences in this study differ from those mentioned earlier by Gonçalves et al. [77]. Almost two times more of each antibody was found in our study than what they reported. In addition the AITD prevalence in RA patients is higher than in the general population from Latin America. According to Marsiglia the prevalence of AITD in the general population in Venezuela is 4.2% [117].
With respect to RA severity we only found one abstract that assessed the link between AITD and RA. Charles et al. [118] did not found a relationship between the presence of thyroid antibodies and the occurrence of anti-CCP although they did with PTPN22R620W allele. Likewise, in our cohort we did not find a correlation between AITD and proxy variables for RA severity such as erosions, biologic agent use, the presence of anti-CCP [119], and EAMs (data not shown). The reason why this association between AITD and RA severity has not been studied is not immediately apparent. One cannot but hypothesize that many of these studies are cross-sectional in nature and because the importance of DAS28 and HAQ is along a timeline, it is not relevant to include these variables in the analysis.
In nonautoimmune hypothyroidism however, Cojocaru-Gofita et al. [120] found that women with AR and clinical hypothyroidism had a higher DAS28 score compared to RA women without clinical hypothyroidism. Kang et al. [121] found that in Korean patients with AR subclinical or clinical hypothyroidism was associated to the occurrence of positive titers of anti-CCP. Also, Delamere et al. [122] found that thyroid dysfunction is associated with increased mean duration and incidence of morning stiffness. It is important to consider these reports because some of these patients may have AITD and this could be related to the severity of RA. Figure 2 illustrates the main symptoms in patients with AITD and AR.
Figure 2.
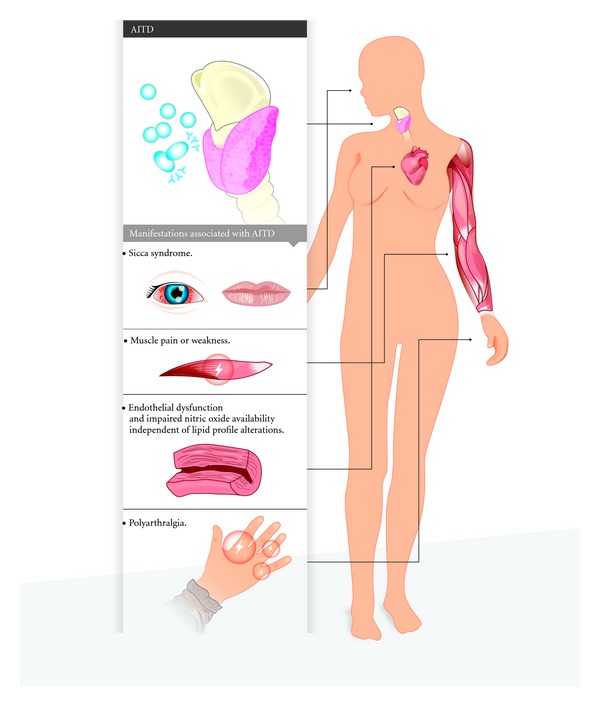
AITD manifestations in patients with RA. AITD manifestations may resemble those presented by RA. Some symptoms are exacerbated when both diseases co-occur. See text for details.
The importance of this Colombian cohort is worth considering. We attempt to add further knowledge with respect to the characteristics of RA in minorities in Latin America, a region about which literature on this topic is scarce.
We are aware of our study limitations. First of all, information bias could be present in our analysis as not all patients with RA were systematically evaluated for all the variables. This is the case for thyroid antibodies, which were only assessed in patients that had some type of thyroid disturbance. This included 135 patients for TPOAb and 125 for TgAb. Secondly, the cross-sectional nature of the study does not allow us to infer causality. Another limitation is one that is linked to all searches—some articles may have escaped our search and, thus, some regions may have been overlooked. Additionally, the articles found had small sample sizes. It is important to consider the heterogeneity in the definition of AITD as well. In contrast, our strengths are our number of participants, a well-described cohort of RA patients, and the multicenter validation of RA cases. To our knowledge, this is the first paper that addresses this particular topic from a global perspective.
There were more patients with TPOAb and TgAb than with a clinical diagnosis of AITD. Linked with the idea that autoantibodies are predictors of disease [123, 124], it is important to remain vigilant in following the clinical course of these patients; TPOAb and TgAb are known to predict AITD. This was demonstrated in the Wickham cohort [97]. Patients within accepted TSH reference range and having the aforementioned antibodies had a greater risk of developing overt hypothyroidism (i.e., AITD). Also TPOAb has been shown to predict development of AITD in pregnant women [125]. A careful assessment of those patients with a normal range of TSH but presenting specific antibodies should be done.
To conclude, we have found that AITD is not uncommon in RA patients. The range has its lower limit in 0.5% and it goes up to 27%. For TgAb, this prevalence ranges from 6% to 31% and for TPOAb, also from 5% to 37%. The prevalence of AITD and antibodies in our cohort falls within these ranges. Our literature search indicates that literature is scarce and, therefore, more research is needed on this topic, particularly in developing countries. The findings in this study justify a prospective analysis that follows RA patients diagnosed with AITD. They also support routine screening for CVD among these patients. These results may help to further study the common mechanisms of autoimmune diseases, to improve patients' outcome, and to define public health policies. An international consensus to accurately diagnose AITD is warranted.
Conflict of Interests
The authors declare no conflict of interests.
Acknowledgments
The authors thank their colleagues at the CREA for fruitful discussions and Studio SCH for their aid in infographic design. This work was supported by the Universidad del Rosario.
References
- 1.Eschler DC, Hasham A, Tomer Y. Cutting edge: the etiology of autoimmune thyroid diseases. Clinical Reviews in Allergy and Immunology. 2011;41(2):190–197. doi: 10.1007/s12016-010-8245-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tomer Y, Huber A. The etiology of autoimmune thyroid disease: a story of genes and environment. Journal of Autoimmunity. 2009;32(3-4):231–239. doi: 10.1016/j.jaut.2009.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shin JI, Kim MJ, Lee JS. Graves’ disease, rheumatoid arthritis, and anti-tumor necrosis factor-alpha therapy. The Journal of Rheumatology. 2009;36(2):449–450. doi: 10.3899/jrheum.080725. [DOI] [PubMed] [Google Scholar]
- 4.Galofre JC, Davies TF. Autoimmune thyroid disease in pregnancy: a review. Journal of Women’s Health. 2009;18(11):1847–1856. doi: 10.1089/jwh.2008.1234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dayan CM, Daniels GH. Chronic autoimmune thyroiditis. The New England Journal of Medicine. 1996;335(2):99–107. doi: 10.1056/NEJM199607113350206. [DOI] [PubMed] [Google Scholar]
- 6.Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T4, and thyroid antibodies in the United States population (1988 to 1994): national health and nutrition examination survey (NHANES III) Journal of Clinical Endocrinology and Metabolism. 2002;87(2):489–499. doi: 10.1210/jcem.87.2.8182. [DOI] [PubMed] [Google Scholar]
- 7.Carlé A, Laurberg P, Knudsen N, et al. Thyroid peroxidase and thyroglobulin auto-antibodies in patients with newly diagnosed overt hypothyroidism. Autoimmunity. 2006;39(6):497–503. doi: 10.1080/08916930600907913. [DOI] [PubMed] [Google Scholar]
- 8.Cadena J, Vinaccia S, Pérez A, Rico MI, Hinojosa R, Anaya JM. The impact of disease activity on the quality of life, mental health status, and family dysfunction in colombian patients with rheumatoid arthritis. Journal of Clinical Rheumatology. 2003;9(3):142–150. doi: 10.1097/01.RHU.0000073434.59752.f3. [DOI] [PubMed] [Google Scholar]
- 9.Rojas-Villarraga A, Bayona J, Zuluaga N, Mejia S, Hincapie ME, Anaya JM. The impact of rheumatoid foot on disability in Colombian patients with rheumatoid arthritis. BMC Musculoskeletal Disorders. 2009;10(1, article 67) doi: 10.1186/1471-2474-10-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Anaya JM. Severe rheumatoid valvular heart disease. Clinical Rheumatology. 2006;25(5):743–745. doi: 10.1007/s10067-005-0039-7. [DOI] [PubMed] [Google Scholar]
- 11.Scott DL, Wolfe F, Huizinga TWJ. Rheumatoid arthritis. The Lancet. 2010;376(9746):1094–1108. doi: 10.1016/S0140-6736(10)60826-4. [DOI] [PubMed] [Google Scholar]
- 12.Delgado-Vega AM, Anaya JM. Meta-analysis of HLA-DRB1 polymorphism in Latin American patients with rheumatoid arthritis. Autoimmunity Reviews. 2007;6(6):402–408. doi: 10.1016/j.autrev.2006.11.004. [DOI] [PubMed] [Google Scholar]
- 13.Alamanos Y, Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmunity Reviews. 2005;4(3):130–136. doi: 10.1016/j.autrev.2004.09.002. [DOI] [PubMed] [Google Scholar]
- 14.Cardiel MH, Rojas-Serrano J. Community based study to estimate prevalence, burden of illness and help seeking behavior in rheumatic diseases in Mexico City. A COPCORD study. Clinical and Experimental Rheumatology. 2002;20(5):617–624. [PubMed] [Google Scholar]
- 15.Cadena J, Anaya JM, Kvien TK, Dadoniene J. Clinical comparisons of RA between different populations: are they feasible? Annals of the Rheumatic Diseases. 2003;62(11):1124–1125. doi: 10.1136/ard.62.11.1124-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.DeMaria AN. Relative risk of cardiovascular events in patients with rheumatoid arthritis. American Journal of Cardiology. 2002;89(6):33D–38D. doi: 10.1016/s0002-9149(02)02235-x. [DOI] [PubMed] [Google Scholar]
- 17.Baka Z, Buzás E, Nagy G. Rheumatoid arthritis and smoking: putting the pieces together. Arthritis Research and Therapy. 2009;11(4, article 238) doi: 10.1186/ar2751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Meron MK, Amital H, Shepshelovich D, et al. Infectious aspects and the etiopathogenesis of rheumatoid arthritis. Clinical Reviews in Allergy and Immunology. 2010;38(2-3):287–291. doi: 10.1007/s12016-009-8158-6. [DOI] [PubMed] [Google Scholar]
- 19.Barzilai O, Sherer Y, Ram M, Izhaky D, Anaya JM, Shoenfeld Y. Epstein-Barr virus and cytomegalovirus in autoimmune diseases: are they truly notorious? A preliminary report. Annals of the New York Academy of Sciences. 2007;1108:567–577. doi: 10.1196/annals.1422.059. [DOI] [PubMed] [Google Scholar]
- 20.Quintero OL, Amador-Patarroyo MJ, Montoya-Ortiz G, Rojas-Villarraga A, Anaya JM. Autoimmune disease and gender: plausible mechanisms for the female predominance of autoimmunity. Journal of Autoimmunity. 2012;38(2-3):109–119. doi: 10.1016/j.jaut.2011.10.003. [DOI] [PubMed] [Google Scholar]
- 21.Raterman HG, van Halm VP, Voskuyl AE, Simsek S, Dijkmans BAC, Nurmohamed MT. Rheumatoid arthritis is associated with a high prevalence of hypothyroidism that amplifies its cardiovascular risk. Annals of the Rheumatic Diseases. 2008;67(2):229–232. doi: 10.1136/ard.2006.068130. [DOI] [PubMed] [Google Scholar]
- 22.Peters MJL, Nielen MMJ, Raterman HG, Verheij RA, Schellevis FG, Nurmohamed MT. Increased cardiovascular disease in patients with inflammatory arthritis in primary care: a cross-sectional observation. Journal of Rheumatology. 2009;36(9):1866–1868. doi: 10.3899/jrheum.090010. [DOI] [PubMed] [Google Scholar]
- 23.Hijmans W, Doniach D, Roitt IM, Holborow E. Serological overlap between lupus erythematosus, rheumatoid arthritis, and thyroid auto-immune disease. British Medical Journal. 1961;2(5257):909–914. doi: 10.1136/bmj.2.5257.909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Becker K, Ferguson R, McConahey W. The connective-tissue diseases and symptoms associated with Hashimoto’s thyroiditis. The New England Journal of Medicine. 1963;268:277–280. doi: 10.1056/NEJM196302072680601. [DOI] [PubMed] [Google Scholar]
- 25.Punzi L, Betterle C. Chronic autoimmune thyroiditis and rheumatic manifestations. Joint Bone Spine. 2004;71(4):275–283. doi: 10.1016/j.jbspin.2003.06.005. [DOI] [PubMed] [Google Scholar]
- 26.Deshmukh HA, Maiti AK, Kim-Howard XR, Rojas-Villarraga A, Guthridge JM, Anaya JM, et al. Evaluation of 19 autoimmune disease-associated loci with rheumatoid arthritis in a Colombian population: evidence for replication and gene-gene interaction. The Journal of Rheumatology. 2011;38(9):1866–1870. doi: 10.3899/jrheum.110199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Anaya JM, Rojas-Villarraga A, García-Carrasco M. The autoimmune tautology: from polyautoimmunity and familial autoimmunity to the autoimmune genes. Autoimmune Diseases. 2012;2012:2 pages. doi: 10.1155/2012/297193.297193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fallena Zonana M, Reyes E, Weisman AK. Coexistence of four autoimmune diseases in one patient: the kaleidoscope of autoimmunity. Journal of Clinical Rheumatology. 2002;8(6):322–325. doi: 10.1097/00124743-200212000-00008. [DOI] [PubMed] [Google Scholar]
- 29.Rojas-Villarraga A, Amaya-Amaya J, Rodriguez-Rodriguez A, Mantilla RD, Anaya JM. Introducing polyautoimmunity: secondary autoimmune diseases no longer exist. Autoimmune Diseases. 2012;2012:9 pages. doi: 10.1155/2012/254319.254319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Anaya JM, Castiblanco J, Rojas-Villarraga A, Pineda-Tamayo R, Levy RA, Gómez-Puerta J, et al. The multiple autoimmune syndromes. A clue for the autoimmune tautology. doi: 10.1007/s12016-012-8317-z. Clinical Reviews in Allergy and Immunology. In press. [DOI] [PubMed] [Google Scholar]
- 31.Anaya JM, Castiblanco J, Tobón GJ, et al. Familial clustering of autoimmune diseases in patients with type 1 diabetes mellitus. Journal of Autoimmunity. 2006;26(3):208–214. doi: 10.1016/j.jaut.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 32.Rojas-Villarraga A, Toro CE, Espinosa G, et al. Factors influencing polyautoimmunity in systemic lupus erythematosus. Autoimmunity Reviews. 2010;9(4):229–232. doi: 10.1016/j.autrev.2009.10.001. [DOI] [PubMed] [Google Scholar]
- 33.Szyper-Kravitz M, Marai I, Shoenfeld Y. Coexistence of thyroid autoimmunity with other autoimmune diseases: friend or foe? Additional aspects on the mosaic of autoimmunity. Autoimmunity. 2005;38(3):247–255. doi: 10.1080/08916930500050194. [DOI] [PubMed] [Google Scholar]
- 34.Wiebolt J, Koeleman BPC, van Haeften TW. Endocrine autoimmune disease: genetics become complex. European Journal of Clinical Investigation. 2010;40(12):1144–1155. doi: 10.1111/j.1365-2362.2010.02366.x. [DOI] [PubMed] [Google Scholar]
- 35.Chistiakov DA, Turakulov RI. CTLA-4 and its role in autoimmune thyroid disease. Journal of Molecular Endocrinology. 2003;31(1):21–36. doi: 10.1677/jme.0.0310021. [DOI] [PubMed] [Google Scholar]
- 36.Duntas LH. Environmental factors and thyroid autoimmunity. Annales d’Endocrinologie. 2011;72(2):108–113. doi: 10.1016/j.ando.2011.03.019. [DOI] [PubMed] [Google Scholar]
- 37.Stathatos N, Daniels GH. Autoimmune thyroid disease. Current Opinion in Rheumatology. 2012;24(1):70–75. doi: 10.1097/BOR.0b013e32834ddb27. [DOI] [PubMed] [Google Scholar]
- 38.Tomer Y. Genetic susceptibility to autoimmune thyroid disease: past, present, and future. Thyroid. 2010;20(7):715–725. doi: 10.1089/thy.2010.1644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Simmonds MJ, Gough SCL. The search for the genetic contribution to autoimmune thyroid disease: the never ending story? Briefings in Functional Genomics. 2011;10(2):77–90. doi: 10.1093/bfgp/elq036. [DOI] [PubMed] [Google Scholar]
- 40.Tomer Y, Davies TF. Searching for the autoimmune thyroid disease susceptibility genes: from gene mapping to gene function. Endocrine Reviews. 2003;24(5):694–717. doi: 10.1210/er.2002-0030. [DOI] [PubMed] [Google Scholar]
- 41.Barton A, Worthington J. Genetic susceptibility to rheumatoid arthritis: an emerging picture. Arthritis Care and Research. 2009;61(10):1441–1446. doi: 10.1002/art.24672. [DOI] [PubMed] [Google Scholar]
- 42.Scott DL, Smith C, Kingsley G. Joint damage and disability in rheumatoid arthritis: an updated systematic review. Clinical and Experimental Rheumatology. 2003;21(5, supplement 31):S20–S27. [PubMed] [Google Scholar]
- 43.Rojas-Villarraga A, Diaz FJ, Calvo-Páramo E, et al. Familial disease, the HLA-DRB1 shared epitope and anti-CCP antibodies influence time at appearance of substantial joint damage in rheumatoid arthritis. Journal of Autoimmunity. 2009;32(1):64–69. doi: 10.1016/j.jaut.2008.11.004. [DOI] [PubMed] [Google Scholar]
- 44.Arnett FC, Edworthy SM, Bloch DA, et al. The American rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis and Rheumatism. 1988;31(3):315–324. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- 45.Rojas-Villarraga A, Ortega-Hernandez OD, Gomez LF, et al. Risk factors associated with different stages of atherosclerosis in Colombian patients with rheumatoid arthritis. Seminars in Arthritis and Rheumatism. 2008;38(2):71–82. doi: 10.1016/j.semarthrit.2008.01.019. [DOI] [PubMed] [Google Scholar]
- 46.Law115. General on Education, p. 4, February 1994.
- 47.Law30. General on Higher Education, p. 4, December 1992.
- 48.Yehuda Shoenfeld GME, Cervera R. Diagnostic Criteria in Autoimmune Diseases. 1st edition. New Jersey, NJ, USA: Humana Press; 2008. [Google Scholar]
- 49.van der Heijde D. How to read radiographs according to the Sharp/van der Heijde method. Journal of Rheumatology. 1999;26(3):743–745. [PubMed] [Google Scholar]
- 50.Jones DW, Hall JE. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure and evidence from new hypertension trials. Hypertension. 2004;43(1):1–3. doi: 10.1161/01.HYP.0000110061.06674.ca. [DOI] [PubMed] [Google Scholar]
- 51.Statements P. Standards of medical care in diabetes—2012. Diabetes Care. 2012;35(supplement 1):S11–S63. doi: 10.2337/dc12-s011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Stone NJ, Bilek S, Rosenbaum S. Recent national cholesterol education program adult treatment panel III update: adjustments and options. American Journal of Cardiology. 2005;96(4):53E–59E. doi: 10.1016/j.amjcard.2005.06.006. [DOI] [PubMed] [Google Scholar]
- 53.Reiner Z, Catapano AL, de Backer G, Graham I, Taskinen MR, Wiklund O, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European society of cardiology (ESC) and the European atherosclerosis society (EAS) European Heart Journal. 2011;32(14):1769–1818. doi: 10.1093/eurheartj/ehr158. [DOI] [PubMed] [Google Scholar]
- 54.Liao Y, Kwon S, Shaughnessy S, et al. Critical evaluation of adult treatment panel III criteria in identifying insulin resistance with dyslipidemia. Diabetes Care. 2004;27(4):978–983. doi: 10.2337/diacare.27.4.978. [DOI] [PubMed] [Google Scholar]
- 55.Klein S, Allison DB, Heymsfield SB, et al. Waist circumference and cardiometabolic risk: a consensus statement from shaping America’s health: association for weight management and obesity prevention; NAASO, the obesity society; the American society for nutrition; and the American diabetes association. American Journal of Clinical Nutrition. 2007;85(5):1197–1202. doi: 10.1093/ajcn/85.5.1197. [DOI] [PubMed] [Google Scholar]
- 56.Day C. Metabolic syndrome, or what you will: definitions and epidemiology. Diabetes and Vascular Disease Research. 2007;4(1):32–38. doi: 10.3132/dvdr.2007.003. [DOI] [PubMed] [Google Scholar]
- 57.Mousa AA, Ghonem M, Hegazy A, El-Baiomy AA, El-Diasty A. Thyroid function and auto-antibodies in egyptian patients with systemic lupus erythematosus and rheumatoid arthritis. Trends in Medical Research. 2012;7(1):25–33. [Google Scholar]
- 58.Benamour S, Zeroual B, Fares L, El Kabli H, Bettal S. Rheumatoid arthritis in Morocco. Revue du Rhumatisme et des Maladies Ostéo-Articulaires. 1992;59(12):801–807. [PubMed] [Google Scholar]
- 59.Shiroky JB, Cohen M, Ballachey ML, Neville C. Thyroid dysfunction in rheumatoid arthritis: a controlled prospective survey. Annals of the Rheumatic Diseases. 1993;52(6):454–456. doi: 10.1136/ard.52.6.454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Becker KL, Titus JL, Woolner LB, Ferguson RH. Thyroiditis and rheumatoid arthritis. Proceedings of the Staff Meetings. Mayo Clinic. 1963;38:125–129. [PubMed] [Google Scholar]
- 61.Linos A, Worthington JW, Palumbo PJ, O’Fallon WM, Kurland LT. Occurrence of Hashimoto’s thyroiditis and diabetes mellitus in patients with rheumatoid arthritis. Journal of Chronic Diseases. 1980;33(2):73–77. doi: 10.1016/0021-9681(80)90030-2. [DOI] [PubMed] [Google Scholar]
- 62.McCoy SS, Crowson CS, Gabriel SE, Matteson EL. Hypothyroidism as a risk factor for development of cardiovascular disease in patients with rheumatoid arthritis. The Journal of Rheumatology. 2012;39(5):954–958. doi: 10.3899/jrheum.111076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pongratz R, Buchinger W, Semlitsch G, Meister E, Nadler K, Rainer F. Increased occurrence of autoimmune thyroiditis in patients with rheumatoid arthritis. Acta Medica Austriaca. 2000;27(2):58–60. [PubMed] [Google Scholar]
- 64.Caron P, Lassoued S, Dromer C, Oksman F, Fournie A. Prevalence of thyroid abnormalities in patients with rheumatoid arthritis. Thyroidology/A.P.R.I.M. 1992;4(3):99–102. [PubMed] [Google Scholar]
- 65.Herrmann F, Hambsch K, Müller P, Häntzschel H, Zugehör M. Incidence of goiter and thyroiditis in chronic inflammatory rheumatism. Zeitschrift fur die gesamte innere Medizin und ihre Grenzgebiete. 1990;45(2):52–55. [PubMed] [Google Scholar]
- 66.Biro E, Szekanecz Z, Czirjk L, et al. Association of systemic and thyroid autoimmune diseases. Clinical Rheumatology. 2006;25(2):240–245. doi: 10.1007/s10067-005-1165-y. [DOI] [PubMed] [Google Scholar]
- 67.Somers EC, Thomas SL, Smeeth L, Hall AJ. Are individuals with an autoimmune disease at higher risk of a second autoimmune disorder? American Journal of Epidemiology. 2009;169(6):749–755. doi: 10.1093/aje/kwn408. [DOI] [PubMed] [Google Scholar]
- 68.Thomas DJB, Young A, Gorsuch AN, Bottazzo GF, Cudworth AG. Evidence for an association between rheumatoid arthritis and autoimmune endocrine disease. Annals of the Rheumatic Diseases. 1983;42(3):297–300. doi: 10.1136/ard.42.3.297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Chan ATY, Al-Saffar Z, Bucknall RC. Thyroid disease in systemic lupus erythematosus and rheumatoid arthritis. Rheumatology. 2001;40(3):353–354. doi: 10.1093/rheumatology/40.3.353. [DOI] [PubMed] [Google Scholar]
- 70.Przygodzka M, Filipowicz-Sosnowska A. Prevalence of thyroid diseases and antithyroid antibodies in women with rheumatoid arthritis. Polskie Archiwum Medycyny Wewnetrznej. 2009;119(1-2):39–44. [PubMed] [Google Scholar]
- 71.Lazúrová I, Benhatchi K, Rovenský J, et al. Autoimmune thyroid disease and autoimmune rheumatic disorders: a two-sided analysis. Annals of the New York Academy of Sciences. 2009;1173:211–216. doi: 10.1111/j.1749-6632.2009.04809.x. [DOI] [PubMed] [Google Scholar]
- 72.Zayeni SH, Mohammadi F, Jafareneghad A, Amini N, Assar R. The relative frequency of thyroid disease in rheumatoid arthritis: abstract cross sectional study of 224 rheumatoid arthritis patients. International Journal of Rheumatic Diseases. 2010;13, article 68 [Google Scholar]
- 73.Assal HS, Elsherbiny A, Alsayed A, Maaboud MA, AlShabrawi H, Rasheed EA. Thyroid dysfunction in patients with systemic connective tissue disease. Macedonian Journal of Medical Sciences. 2009;2(3):223–229. [Google Scholar]
- 74.El-Sherif WT, El Gendi SS, Ashmawy MM, Ahmed HM, Salama MM. Thyroid disorders and autoantibodies in systemic lupus erythematosus and rheumatoid arthritis patients. The Egyptian Journal of Immunology/Egyptian Association of Immunologists. 2004;11(2):81–90. [PubMed] [Google Scholar]
- 75.Rivero I, Guntsche E, Abaurre R, Posse RM. Antithyroglobulin antibody in autoimmune disease. Medicina. 1974;34(4):307–312. [PubMed] [Google Scholar]
- 76.Innocencio RM, Romaldini JH, Ward LS. Thyroid autoantibodies in autoimmune diseases. Medicina. 2004;64(3):227–230. [PubMed] [Google Scholar]
- 77.Gonçalves FT, Feibelmann TCM, Ranza R, et al. Autoimmune thyroiditis and rheumatoid arthritis: is there really an association? Endocrinologist. 2009;19(1):31–34. [Google Scholar]
- 78.Porkodi R, Ramesh S, Maheshk A, Kanakarani P, Rukmangathrajan S, Rajedran C. Thyroid dysfunction in systemic lupus erythematosus and rheumatoid arthritis. Journal of Indian Rheumatology Association. 2004;12:88–97. [Google Scholar]
- 79.Nakamura H, Usa T, Motomura M, et al. Prevalence of interrelated autoantibodies in thyroid diseases and autoimmune disorders. Journal of Endocrinological Investigation. 2008;31(10):861–865. doi: 10.1007/BF03346432. [DOI] [PubMed] [Google Scholar]
- 80.Atzeni F, Doria A, Ghirardello A, et al. Anti-thyroid antibodies and thyroid dysfunction in rheumatoid arthritis: prevalence and clinical value. Autoimmunity. 2008;41(1):111–115. doi: 10.1080/08916930701620100. [DOI] [PubMed] [Google Scholar]
- 81.Ruggeri RM, Galletti M, Mandolfino MG, et al. Thyroid hormone autoantibodies in primary Sjögren syndrome and rheumatoid arthritis are more prevalent than in autoimmune thyroid disease, becoming progressively more frequent in these diseases. Journal of Endocrinological Investigation. 2002;25(5):447–454. doi: 10.1007/BF03344036. [DOI] [PubMed] [Google Scholar]
- 82.Genth E, Detering-Huebner B, Stankovic A. Disorders of the thyroid gland in rheumatoid arthritis. Medizinische Welt. 1978;29(45):1746–1753. [PubMed] [Google Scholar]
- 83.Andonopoulos AP, Siambi V, Makri M, Christofidou M, Markou C, Vagenakis AG. Thyroid function and immune profile in rheumatoid arthritis. A controlled study. Clinical Rheumatology. 1996;15(6):599–603. doi: 10.1007/BF02238551. [DOI] [PubMed] [Google Scholar]
- 84.Raterman HG, Nurmohamed MT. Hypothyroidism in rheumatoid arthritis—to screen or not to screen? Journal of Rheumatology. 2012;39(5):885–886. doi: 10.3899/jrheum.120015. [DOI] [PubMed] [Google Scholar]
- 85.Magnus JH, Birketvedt T, Haga HJ. A prospective evaluation of antithyroid antibody between prevalence in 100 patients with rheumatoid arthritis. Scandinavian Journal of Rheumatology. 1995;24(3):180–182. doi: 10.3109/03009749509099312. [DOI] [PubMed] [Google Scholar]
- 86.Buchanan WW. The relationship of Hashimoto’s thyroiditis to rheumatoid arthritis. Geriatrics. 1965;20(11):941–948. [PubMed] [Google Scholar]
- 87.Yavasoglu I, Senturk T, Coskun A, Bolaman Z. Rheumatoid arthritis and anti-thyroid antibodies. Autoimmunity. 2009;42(2):168–169. doi: 10.1080/08916930802428114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Silman AJ, Ollier WER, Bubel MA. Autoimmune thyroid disease and thyroid autoantibodies in rheumatoid arthritis patients and their families. British Journal of Rheumatology. 1989;28(1):18–21. doi: 10.1093/rheumatology/28.1.18. [DOI] [PubMed] [Google Scholar]
- 89.Al-Awadhi AM, Olusi S, Hasan EA, Abdullah A. Frequency of abnormal thyroid function tests in Kuwaiti Arabs with autoimmune diseases. Medical Principles and Practice. 2008;17(1):61–65. doi: 10.1159/000109592. [DOI] [PubMed] [Google Scholar]
- 90.Jensen E, Petersen PH, Blaabjerg O, et al. Establishment of a serum thyroid stimulating hormone (TSH) reference interval in healthy adults. The importance of environmental factors, including thyroid antibodies. Clinical Chemistry and Laboratory Medicine. 2004;42(7):824–832. doi: 10.1515/CCLM.2004.136. [DOI] [PubMed] [Google Scholar]
- 91.Wartofsky L, Dickey RA. The evidence for a narrower thyrotropin reference range is compelling. Journal of Clinical Endocrinology and Metabolism. 2005;90(9):5483–5488. doi: 10.1210/jc.2005-0455. [DOI] [PubMed] [Google Scholar]
- 92.Dickey RA, Wartofsky L, Feld S. Optimal thyrotropin level: normal ranges and reference intervals are not equivalent. Thyroid. 2005;15(9):1035–1039. doi: 10.1089/thy.2005.15.1035. [DOI] [PubMed] [Google Scholar]
- 93.Surks MI, Hollowell JG. Age-specific distribution of serum thyrotropin and antithyroid antibodies in the U.S. population: implications for the prevalence of subclinical hypothyroidism. Journal of Clinical Endocrinology and Metabolism. 2007;92(12):4575–4582. doi: 10.1210/jc.2007-1499. [DOI] [PubMed] [Google Scholar]
- 94.Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. The Journal of the American Medical Association. 2004;291(2):228–238. doi: 10.1001/jama.291.2.228. [DOI] [PubMed] [Google Scholar]
- 95.Hamilton TE, Davis S, Onstad L, Kopecky KJ. Thyrotropin levels in a population with no clinical, autoantibody, or ultrasonographic evidence of thyroid disease: implications for the diagnosis of subclinical hypothyroidism. Journal of Clinical Endocrinology and Metabolism. 2008;93(4):1224–1230. doi: 10.1210/jc.2006-2300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Baloch Z, Carayon P, Conte-Devolx B, et al. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid. 2003;13(1):3–126. doi: 10.1089/105072503321086962. [DOI] [PubMed] [Google Scholar]
- 97.Vanderpump MPJ, Tunbridge WMG, French JM, et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham survey. Clinical Endocrinology. 1995;43(1):55–68. doi: 10.1111/j.1365-2265.1995.tb01894.x. [DOI] [PubMed] [Google Scholar]
- 98.Baskin HJ, Cobin RH, Duick DS, Gharib H, Guttler RB, Kaplan MM, et al. American association of clinical endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocrine Practice. 2002;8(6):457–469. [PubMed] [Google Scholar]
- 99.Burek CL. Autoimmune thyroiditis research at Johns Hopkins University. Immunologic Research. 2010;47(1–3):207–215. doi: 10.1007/s12026-009-8151-4. [DOI] [PubMed] [Google Scholar]
- 100.Ruwhof C, Drexhage HA. Iodine and thyroid autoimmune disease in animal models. Thyroid. 2001;11(5):427–436. doi: 10.1089/105072501300176381. [DOI] [PubMed] [Google Scholar]
- 101.Saranac L, Zivanovic S, Bjelakovic B, Stamenkovic H, Novak M, Kamenov B. Why is the thyroid so prone to autoimmune disease? Hormone Research in Paediatrics. 2011;75(3):157–165. doi: 10.1159/000324442. [DOI] [PubMed] [Google Scholar]
- 102.Doufas AG, Mastorakos G, Chatziioannou S, et al. The predominant form of non-toxic goiter in Greece is now autoimmune thyroiditis. European Journal of Endocrinology. 1999;140(6):505–511. doi: 10.1530/eje.0.1400505. [DOI] [PubMed] [Google Scholar]
- 103.de Benoist B, Andersson M, editors. Iodine Status Worldwide Iodine Status Worldwide. Geneva, Switzerland: World Health Organization; 2004. [Google Scholar]
- 104.Ortega-Hernandez OD, Pineda-Tamayo R, Pardo AL, Rojas-Villarraga A, Anaya JM. Cardiovascular disease is associated with extra-articular manifestations in patients with rheumatoid arthritis. Clinical Rheumatology. 2009;28(7):767–775. doi: 10.1007/s10067-009-1145-8. [DOI] [PubMed] [Google Scholar]
- 105.Pineda-Tamayo R, Arcila G, Restrepo P, Anaya JM. Impact of cardiovascular illness on hospitalization costs in patients with rheumatoid arthritis. Biomédica. 2004;24(4):366–374. [PubMed] [Google Scholar]
- 106.Nurmohamed MT. Cardiovascular risk in rheumatoid arthritis. Autoimmunity Reviews. 2009;8(8):663–667. doi: 10.1016/j.autrev.2009.02.015. [DOI] [PubMed] [Google Scholar]
- 107.Libby P. Role of inflammation in atherosclerosis associated with rheumatoid arthritis. American Journal of Medicine. 2008;121(10, supplement 1):S21–S31. doi: 10.1016/j.amjmed.2008.06.014. [DOI] [PubMed] [Google Scholar]
- 108.Maradit-Kremers H, Nicola PJ, Crowson CS, Ballman KV, Gabriel SE. Cardiovascular death in rheumatoid arthritis: a population-based study. Arthritis and Rheumatism. 2005;52(3):722–732. doi: 10.1002/art.20878. [DOI] [PubMed] [Google Scholar]
- 109.Buchinger W, Pongratz R, Binter G, Eber O. Do increased lipoprotein(a) levels in euthyroid autoimmune thyroid diseases predict an increased risk of arteriosclerosis? Acta Medica Austriaca. 1995;22(4):78–81. [PubMed] [Google Scholar]
- 110.Taddei S, Caraccio N, Virdis A, et al. Low-grade systemic inflammation causes endothelial dysfunction in patients with Hashimoto’s thyroiditis. Journal of Clinical Endocrinology and Metabolism. 2006;91(12):5076–5082. doi: 10.1210/jc.2006-1075. [DOI] [PubMed] [Google Scholar]
- 111.Raterman HG, van Halm VP, Voskuyl AE, Simsek S, Dijkmans BA, Nurmohamed MT. Increased prevalence of antithyroid antibodies in rheumatoid arthritis (RA) patients with a low prevalence of hormonal alterations. Autoimmunity. 2008;41(5, article 337) doi: 10.1080/08916930802015549. [DOI] [PubMed] [Google Scholar]
- 112.Mercer E, Rekedal L, Garg R, Lu B, Massarotti EM, Solomon DH. Hydroxychloroquine improves insulin sensitivity in obese non-diabetic individuals. Arthritis Research and Therapy. 2012;14, article R135 doi: 10.1186/ar3868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Wasko MCM, Hubert HB, Lingala VB, et al. Hydroxychloroquine and risk of diabetes in patients with rheumatoid arthritis. The Journal of the American Medical Association. 2007;298(2):187–193. doi: 10.1001/jama.298.2.187. [DOI] [PubMed] [Google Scholar]
- 114.Solomon DH, Massarotti E, Garg R, Liu J, Canning C, Schneeweiss S. Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. The Journal of the American Medical Association. 2011;305(24):2525–2531. doi: 10.1001/jama.2011.878. [DOI] [PubMed] [Google Scholar]
- 115.Wallace DJ, Metzger AL, Stecher VJ, Turnbull BA, Kern PA. Cholesterol-lowering effect of hydroxychloroquine in patients with rheumatic disease: reversal of deleterious effects of steroids on lipids. American Journal of Medicine. 1990;89(3):322–326. doi: 10.1016/0002-9343(90)90345-e. [DOI] [PubMed] [Google Scholar]
- 116.Munro R, Morrison E, McDonald AG, Hunter JA, Madhok R, Capell HA. Effect of disease modifying agents on the lipid profiles of patients with rheumatoid arthritis. Annals of the Rheumatic Diseases. 1997;56(6):374–377. doi: 10.1136/ard.56.6.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Marsiglia I. Enfermedad tiroidea autoinmune. Estudio Clínico—Epidemiológico, Gaceta Médica De Caracas. 2008;116:23–36. [Google Scholar]
- 118.Charles PJ, Plant D, Chowdhury M, Worthington J, Venables P. Antibodies to thyroglobulin and thyroid peroxidase in rheumatoid arthritis: environmental and genetic associations. Annals of the Rheumatic Diseases. 2011;70(2):A88–A89. [Google Scholar]
- 119.Diaz FJ, Rojas-Villarraga A, Salazar JC, Iglesias-Gamarra A, Mantilla RD, Anaya JM. Anti-CCP antibodies are associated with early age at onset in patients with rheumatoid arthritis. Joint Bone Spine. 2011;78(2):175–178. doi: 10.1016/j.jbspin.2010.07.014. [DOI] [PubMed] [Google Scholar]
- 120.Cojocaru-Gofita IR, Ciurea P, Rosu A, Musetescu AE, Vreju F, Barbulescu A. Hypothyroidism—risk factor for treatment ressistent, agressive rheumatoid arthritis onset. Scandinavian Journal of Rheumatology. 2010;39, article 29 [Google Scholar]
- 121.Kang EJ, Choi ST, Park YB, Lee SK. Thyroid disease in Korean patients with rheumatoid arthritis. International Journal of Rheumatic Diseases. 2010;13:81–82. [Google Scholar]
- 122.Delamere JP, Scott DL, Felix-Davies DD. Thyroid dysfunction and rheumatic diseases. Journal of the Royal Society of Medicine. 1982;75(2):102–106. [PMC free article] [PubMed] [Google Scholar]
- 123.Bizzaro N. The predictive significance of autoantibodies in organ-specific autoimmune diseases. Clinical Reviews in Allergy and Immunology. 2008;34(3):326–331. doi: 10.1007/s12016-007-8059-5. [DOI] [PubMed] [Google Scholar]
- 124.Scofield RH. Autoantibodies as predictors of disease. The Lancet. 2004;363(9420):1544–1546. doi: 10.1016/S0140-6736(04)16154-0. [DOI] [PubMed] [Google Scholar]
- 125.Kita M, Goulis DG, Avramides A. Post-partum thyroiditis in a Mediterranean population: a prospective study of a large cohort of thyroid antibody positive women at the time of delivery. Journal of Endocrinological Investigation. 2002;25(6):513–519. doi: 10.1007/BF03345493. [DOI] [PubMed] [Google Scholar]