

Abstract
Background:
The purpose of this research is to establish the ability of employees by work ability index (WAI), physical work capacity (PWC), and finding the correlation between them. Establishing the PWC index with attention to WAI values for the purpose of saving in costs and time of PWC measurements is another aim of this project.
Methods:
The present research is an analytic cross-sectional and one-trail study. The study population consists of 228 randomly selected registered nurses from hospitals in Isfahan (Iran). The WAI and PWC were established through WAI questionnaire and Fax equation and by using ergometer bicycle, respectively. The resulting data were analyzed using SPSS 16 software.
Results:
Average WAI and PWC among the study population were 38.25±4.4 and 4.45±0.7, respectively. Pearson test results showed no significant correlation between PWC and WAI in different age groups (r=0.3 and P>0.05). Multiple linear regression analysis showed that the variables of age and diagnosed diseases were the most effective factors of WAI (β=0.18 and P>0.05). Pearson test revealed a significant correlation between the number of diagnosed diseases and PWC index in age groups of 40-49 years.
Conclusion:
Average WAI in this research, like other studies on similar jobs is in the acceptable level of >36. Work ability index and PWC index in different age groups did not show a significant correlation and this suggests that there are essential discrepancies in work ability evaluations made by each index and it is not possible to predict PWC index using WAI values. Given the PWC results and the level of nursing staff's activity (low, medium) the WAI is a suitable instrument to establish the professionals’ abilities. This study revealed that 27.6% of individuals were subject to medium-low work ability risk (WAI<37), which was 1.8 times that of Finland's professional health Institute, which could be caused by shift working and increased working hours.
Keywords: Fax equation, hospital nurses, physical work capacity, work ability index
INTRODUCTION
The correct appraisal of the employees’ work ability is important for employers in economic viewpoint and improving it is one of the ways for increasing the human resources productivity in industries and organization.[1] The concept of work ability is the base for designing work stations and proper choose of staffs for various jobs[2,3] in the other hand, if employee's physical and psychological abilities is not according to their job's requirements, it would led to detect safety and health issues, decreasing production and increasing costs related to dismissal of employees.[4] In entities, where there is no conformity between employee's ability and job requirements, it would represent musculoskeletal disorder and more common digestive difficulties.[5] Researches show that the most of the occupation stresses is caused by non conformity between individual's ability and his job.[6] Some researches introduce the occupation stresses as one of the most important risk factors related to the individuals’ workability.[6] Yet, different quantitative and qualitative models have been presented for measuring the work abilities of employees. Some of them using physiological parameters such as changes of heart rating (HR), maximum consuming oxygen (VO2 max) and in terms of mechanism are measured directly and indirectly,[7,8] including physical work capacity (PWC) which shows the ability and propriety of individuals in concerned job based on maximum consuming energy and by using the parameter of maximum consuming oxygen (VO2 max). Some of the ways for establishing the quantitative and qualitative workability are based on individual's capabilities and physical and psychological work requirements. Workability index is one of them.[9] The index is an application for establishing individual's work ability in professional health care systems, presented by researchers of Finland Institute of Health, and based on a theoretical model of the Work ability house.[10,11] This equation by showing multilateral form of workability including health condition of employees, individual's capability and factors related to work, measures the individual's workability. This model after wide clinical measurements, presented in the case of a seven part questionnaire as the “questionnaire of work capacity index”[11] [Table 1]. The best possible assessment from the WAI index was the score of 49, and the worth of it was the score of 7. Finally, based on the obtained score, the workability categorized for 4 category, including; low 7-27, average 28-36, good 37-44 and high 45-49. Also, in this study, WAI < 37 and WAI > 36 were categorized as the low ability and acceptable ability, respectively.[11] In this study, by using two indexes, WAI, PWC and rate of their correlation will be measured. If there is a proper correlation, it is easy to evaluate PWC index by using WAI values, and then plan its equation. Hence, it is possible to prevent indirect measuring mechanism with high costs.
Table 1.
The elements of the work ability index

METHODS
Present study is the type analytic-cross sectional and one tail. Study population, 228 male nursing staff of Isfahan hospitals, including; nurse, anesthesia technician, and surgery technician, which were selected randomly from sections emergency, men surgery, and surgery room. Used equipments for establishing work ability index of questionnaire and required tools for establishing PWC, were ergometer bike and Bruner carpal pressure indicator. At first, the reliability of WAI questionnaire would be established by test-retest method,[12] coefficient correlation. If the questionnaire has high reliability, in case the questionnaire it would be available respondents with more than 2 years foretime for completing it would be available for research and study. Next stage, by ergometer bike and based on Fax equation, physical capacity of work would be studied. This equation calculates maximum consuming oxygen in terms of under maximum heart rate values.[13] In this method, the person pedals for 5 min with 150 Watt by ergometer bike. Immediately, after 5 min, number of heartbeat in ten seconds would multiply with 6. Then, by Fax equation;
![]()
The maximum consuming oxygen would be presented.[13,14] Before starting examination, conclusions of Bruner digital pressure indicator comprises with a medical pressure indicator. At follow, maximum aerobic capacity would be recognized and using Bink equation, PWC= physical work capability would be recognized. (t is time of shift work in each min).[14,15] During ergometer examination and measuring the HR, the range of temperature should be 23-26°C.[16] For people older than 25 years, age correction factor of Astrand should be mentioned.[16] Also, smoking people and people with torrid heart disease were removed from this research. For data analyzing in WAI questionnaire and ergometer test, we use SPSS 16 software and t-test, Pearson correlation-coefficient, multivariable regression and unilateral variance analysis test.
physical work capability would be recognized. (t is time of shift work in each min).[14,15] During ergometer examination and measuring the HR, the range of temperature should be 23-26°C.[16] For people older than 25 years, age correction factor of Astrand should be mentioned.[16] Also, smoking people and people with torrid heart disease were removed from this research. For data analyzing in WAI questionnaire and ergometer test, we use SPSS 16 software and t-test, Pearson correlation-coefficient, multivariable regression and unilateral variance analysis test.
RESULTS
The respondents’ ages ranged between 21-59 years, with an average of 38.4±8.5, from whom 52.6% were nurses, 30.3% auxiliary nurses, 10.1% operating room technicians and 7% anesthetic technicians. Average working years were 13.9. Test results indicated a WAI average of 38.25±4.4 from whom 27.6% risked low and medium ability (WAI<36); 64% were in good ability conditions and 8.3% in excellent conditions. Re-test results showed a correlation between 0.74 and 0.88 for WAI questionnaire items. As this coefficient exceeds 0.6, the questionnaire has an acceptable reliability. Pearson correlation test revealed a reverse linear relation age and WAI (r=-0.84, P<0.05) such that the highest average belonged to the age group of 20-39 years, and the lowest average, to the group of 50-59 years [Figure 1]. T-test showed a significantly higher WAI average for singles (41.2±3.2) compared with married ones (P<0.050). One-trail variable analysis showed a difference between WAI averages in various work shifts (P=0.008, P<0.05), with the highest belonging to morning shifts (39.9±3.7) and the lowest, to those circulating in all three shifts (37.9±4.5). Also, this test showed different WAI averages in various wards (P=0.04), with emergency, surgery and operation room staff having the values of 37.5±4.8, 38.4±3.9 and 39.2±4, respectively. To examine the factors affecting WAI, multiple linear (multi-linear) regression was used, which through R-Adjust factor showed that 28.5% of WAI variations, could be explained by existing variables. This analysis revealed that age and diagnosed diseases (third WAI item) were the most influential factors in WAI (β=0.13 and P<0.05).
Figure 1.

Changes of indexes WAI and PWC based on age
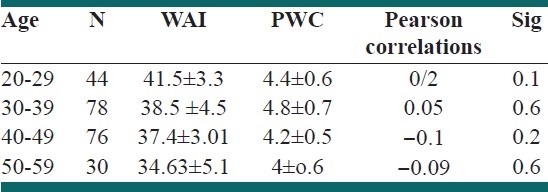
Average PWC index obtained in ergometer test and Fax model was equal to 4.45±0.7, with 55.7% of respondents had a high activity level and 44.3% in medium level. Average of physiological parameters including VO2max and sub-maximal heart rate (Rhmax) were 2.69 lit/min and 123, respectively. Pearson's correlation test results showed a reverse relationship between age and PWC index (r=- 0.26, P<0.050). The highest average in this index belonged to 30-39 years age group and the lowest, to 50-59 years group. Pearson's test showed a significant correlation between the number of diagnosed diseases and PWC index in 40-49 years age-groups. But this correlation was not significant in other age groups. One-trail variance analysis showed that work shift had no significant effect on PWC index (P=0.31). Also, the results indicated the same PWC averages for emergency, surgery and operation room wards. Pearson's correlation test indicated no significant relationship between PWC and WAI for any age group (r=0.3, P<0.13) [Table 2]. Therefore, it is impossible to reach a regressive equation for a suitable estimation of PWC index using WAI values.
Table 2.
Major effective variables on WAI index based on multivariable regression analyze

DISCUSSION
The average WAI obtained in this study, as those studies performed on nurses in United States’ public hospitals, is in the acceptable level of WAI>36.[17] Most WAI studies in contexts similar to nursing have shown a good average (37- 44). For example, it was 42.2±3.4 for physicians in Helsinky hospitals,[18] or 38.7 for France's health care system employees.[19] Various studies have measured WAI in different jobs, mostly being in an acceptable level (WAI>36). For example, it was 40.9 for Dutch construction labor, 39 for Finnish police officers, and 40.9 for Belgian firefighters.[20] The distribution of work ability shows that 27.6% of professionals are at the risk of low-medium ability (WAI<37), 1.8 times the values obtained by Finland's professional health institute.[17] This risk is 13.2% for nurses in American hospitals.[21] The present results are consistent with most previous studies in terms of the relationship between age and WAI [Figure 2]. For example Bujiska et al. showed a reverse correlation between age and WAI for Polish workers (r=-0.35; P<0.05),[8] but Cameron et al., studying 416 workers of a Brazilian electric company indicated that this correlation was direct for age groups lower than 35 years (r=0.3).[21] They showed that WAI's decreasing slop in the age group of 40-49 was steeper, consistent with the findings of Soorenson on Finnish police officers.[22] A result of this study is the effect of shift type on WAI, with the highest values observed for morning shift employees and the lowest, for circulating-shift workers. A possible reason could be the higher number of personnel in morning shifts and the physiological effects of shift working. Jeivani found lowest WAI of night-shift workers, speculating psychological and physiological disorders caused by sleeplessness as its reason, and suggested that individuals older than 45 years, who are at the risk of low ability, should not be employed on night turns.[23] Findings of a WAI study on railway staff indicated that shift working schedule influences lower WAI, and Casta showed that shift workers’ health declined more than day time workers.[24,25] Various studies showed a strong relationship between reduced WAI and the individuals’ health conditions. Multivariable linear regression indicated the factors of age and diagnosed diseases as the most effective ones in WAI. Thus in this study, the WAI is most influenced by the individuals’ health conditions. Other researchers have also reported similar results[26,27] in the present study the average PWC, obtained using ergometer test and Fax model was 4.45±0.71. The experimental test results indicate no significant difference between VO2max obtained from strand anemogram and from Fax equation[27] but some studies show such a significant difference. Nowadays, the Fax equation method is used to calculate the athletes’ aerobic abilities. The findings show a reverse relationship between PWC index and the age (r=-0.26). Of course, this relationship is direct in 20-29 years age group and reverse in 40-49 years group of age, consistent with most studies.[15,21,28]
Figure 2.

Changes of WAI, PWC indexes in age groups
The results revealed a significant correlation between the number of diagnosed diseases and PWC index in the age group of 40-49 years, which could be due to the emergence of most diseases in these ages [Table 3]. Regression analysis showed higher incidences of muscular-skeletal and digestional diseases in the ages between 40 and 49 among the nurses from hospitals of Isfahan. No significant correlation was found between PWC index and WAI (r=0.01, P>0.13). Also, no significant correlation was found between these two indices in terms of various age groups. Some studies showed a direct relationship between them, such as Bujisca et al., who demonstrated a significant correlation for age groups of 20-24 and 25-30 years (r=0.3) but no significant correlation in other groups.[29,30]
Table 3.
Correlation between two indexes based on age in different groups
CONCLUSION
As our results indicated, there was no significant relationship between WAI and PWC and no equation can be obtained to estimate PWC based on WAI values. Results show a substantial difference between the two indices in measuring work ability. Also, the results show that WAI is a good instrument for determination of professionals’ abilities in low-medium activity levels, and in activities with low-medium work loads, it is not necessary to use PWC's measurement protocols. But for evaluation of staff's ability in heavy-work-load jobs, one has to use PWC measurement and protocols. In this study, as the values obtained for WAI indicate 64% of study population had a good ability and it is necessary to take required protective actions to elevate the work ability. Also, given the high proportion of practitioners with low-medium work ability scores, the identification and optimization of factors affecting it must become a priority in intervention and prevention programs. Given the effect of work shift nature on WAI, one has to prevent decreased WAI and emergence of many diseases by modification of working schedules, correct design of shift work schedules, and by improving the staff's sleep and rest conditions. Our results showed a high statistic relationship between WAI values and health conditions. Thus, it is highly necessary to review the health care systems within the organizations with the aim of developing a preventive attitude toward disease control, especially in upper age groups. It is suggested that WAI should be used as a complement to the workers periodic medical examination to determine their abilities to perform the intended task(s), and that future studies must take into account the effects of factors such as job stress on this index since questionnaire-related information has been gathered by interviewing the subjects, there is a possibility for errors. Therefore, the results must be used and comparisons made very carefully.
ACKNOWLEDGMENT
We appreciate the assistance and help of adjutancy of medicine science department of Isfahan University and all district superintendents of Isfahan hospitals.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ahonen G, Bjurström L, Hussi T, Räsänen K. Economic effectiveness of the maintenance and promotion of work ability. Maintenance of Work Ability-Research and Assessment: Summaries Bilbao: Ministry of Social Affairs and Health, Finnish Institute of Occupational Health. 2002:33–44. [Google Scholar]
- 2.van den Berg TI, Elders LA, Burdorf A, editors. The effects of work-related and individual factors on work ability: A systematic review. Promotion of Work Ability towards Productive Aging: Selected papers of the 3rd International Symposium on Work Ability, Hanoi, Vietnam, 22-24 October 2007. 2008 CRC. [Google Scholar]
- 3.Costa AF, Puga-Leal R, Nunes IL. An exploratory study of the Work Ability Index (WAI) and its components in a group of computer workers. Work. 2011;39:357–67. doi: 10.3233/WOR-2011-1186. [DOI] [PubMed] [Google Scholar]
- 4.Vigatto R, Alexandre NM, Correa Filho HR. Development of a Brazilian Portuguese version of the Oswestry Disability Index: cross-cultural adaptation, reliability, and validity. Spine. 2007;32:481–6. doi: 10.1097/01.brs.0000255075.11496.47. [DOI] [PubMed] [Google Scholar]
- 5.Boedeker W. Associations between workload and diseases rarely occurring in sickness absence data. J Occup Environ Med. 2001;43:1081–8. doi: 10.1097/00043764-200112000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Benavides F. Ill health, social protection, labour relations, and sickness absence. Occup Environ Med. 2006;63:228–9. doi: 10.1136/oem.2005.025817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ghaeini A, Rajabi H. The basic principles of physical fitness. Tehran: Samt Publications; 2003. [Google Scholar]
- 8.Billat VL, Demarle A, Slawinski J, Paiva M, Koralsztein JP. Physical and training characteristics of top-class marathon runners. Med Sci Sports Exerc. 2001;33:2089–97. doi: 10.1097/00005768-200112000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Tuomi K, Huuhtanen P, Nykyri E, Ilmarinen J. Promotion of work ability, the quality of work and retirement. Occup Med. 2001;51:318–24. doi: 10.1093/occmed/51.5.318. [DOI] [PubMed] [Google Scholar]
- 10.Peltomäki P, Hussi T, Julin H, Launis K, Liira J, Räsänen K. Social Insurance Institution. Helsinki: Ministry of Social Affairs and Health, Finnish Institute of Occupational Health; 2002. Maintenance of work ability research and assessment: summaries. [Google Scholar]
- 11.Fischer FM. Breve histórico desta tradução. The ability to index worked. 2005:9–10. In: Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A, organizadores. EduFSCar. [Google Scholar]
- 12.De Zwart B, Frings-Dresen M, Van Duivenbooden J. Test–retest reliability of the Work Ability Index questionnaire. Occup Med. 2002;52:177–81. doi: 10.1093/occmed/52.4.177. [DOI] [PubMed] [Google Scholar]
- 13.Darby LA, Pohlman RL. Prediction of maxVO2 for women: adaptation of the Fox cycle ergometer protocol. JEPonline. 1999;2:13–9. [Google Scholar]
- 14.Fox EL. A simple, accurate technique for predicting maximal aerobic power. J Appl Physiol. 1973;35:914–6. doi: 10.1152/jappl.1973.35.6.914. [DOI] [PubMed] [Google Scholar]
- 15.Darby LA, Pohlman RL. American Society of Exercise Physiologists. J Exerc Physiol. 1999;2:4. [Google Scholar]
- 16.Ftaiti F, Kacem A, Jaidane N, Tabka Z, Dogui M. Changes in EEG activity before and after exhaustive exercise in sedentary women in neutral and hot environments. Appl Ergon. 2010;41:806–11. doi: 10.1016/j.apergo.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 17.Rotenberg L, Portela LF, Banks B, Griep RH, Fischer FM, Landsbergis P. A gender approach to work ability and its relationship to professional and domestic work hours among nursing personnel. Appl Ergon. 2008;39:646. doi: 10.1016/j.apergo.2008.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Camerino D, Conway PM, Van der Heijden BI, Estryn-Behar M, Consonni D, Gould D, et al. Low-perceived work ability, ageing and intention to leave nursing: a comparison among 10 European countries. J Adv Nurs. 2006;56:542–52. doi: 10.1111/j.1365-2648.2006.04046.x. [DOI] [PubMed] [Google Scholar]
- 19.Tuomi K, Huuhtanen P, Nykyri E, Ilmarinen J. Promotion of work ability, the quality of work and retirement. Occup Med. 2001;51:318–24. doi: 10.1093/occmed/51.5.318. [DOI] [PubMed] [Google Scholar]
- 20.Alavinia S, De Boer A, Van Duivenbooden J, Frings-Dresen M, Burdorf A. Determinants of work ability and its predictive value for disability. Occup Med. 2009;59:32–7. doi: 10.1093/occmed/kqn148. [DOI] [PubMed] [Google Scholar]
- 21.Bugajska J, Makowiec-Dąbrowska T, Jegier A, Marszałek A, editors. International Congress Series. Elsevier; 2005. Physical work capacity (VO2 max) and work ability (WAI) of active employees (men and women) in Poland. [Google Scholar]
- 22.Sörensen LE, Pekkonen MM, Männikkö KH, Louhevaara VA, Smolander J, Alén MJ. Associations between work ability, health-related quality of life, physical activity and fitness among middle-aged men. Appl Ergon. 2008;39:786–91. doi: 10.1016/j.apergo.2007.11.001. [DOI] [PubMed] [Google Scholar]
- 23.Alavinia SM, van Duivenbooden C, Burdorf A. Influence of work-related factors and individual characteristics on work ability among Dutch construction workers. Scand J Work Environ Health. 2007;33:351–7. doi: 10.5271/sjweh.1151. [DOI] [PubMed] [Google Scholar]
- 24.Costa G, Goedhard W, Ilmarinen J, editors. Assessment and promotion of work ability, health and well-being of ageing workers. International Congress Series. 2005 [Google Scholar]
- 25.Costa G. Factors influencing health of workers and tolerance to shift work. Theor Issues Ergon Sci. 2003;4:263–88. [Google Scholar]
- 26.Ilmarinen JE. Aging workers. Occup Environ Med. 2001;58:546–52. doi: 10.1136/oem.58.8.546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ilmarinen J, Tuomi K, editors. Past, present and future of work ability. Proceedings of the 1st International Symposium on Work Ability, Helsinki. 2004 [Google Scholar]
- 28.Legaz-Arrese A, Munguía-Izquierdo D, Nuviala Nuviala A, Serveto-Galindo O, Moliner Urdiales D, Reverter Masia J. Average VO2max as a function of running performances on different distances. Sci Sports. 2007;22:43–9. [Google Scholar]
- 29.Martinez MC, Latorre MR, Fischer FM. Work ability: a literature review. Science & Public Health. 2010;15:1553–61. doi: 10.1590/s1413-81232010000700067. [DOI] [PubMed] [Google Scholar]
- 30.Latorre O. Health and work ability among office workers. Rev Public Health. 2006;40:851–8. doi: 10.1590/s0034-89102006000600015. [DOI] [PubMed] [Google Scholar]