

Abstract
Objectives
The purpose of this study is to find out associations between positional dependency and obstructive levels based on sleep videofluoroscopy (SVF) in patients with obstructive sleep apnea syndrome (OSAS).
Methods
Retrospective review was made of 91 OSAS patients who underwent polysomnography and SVF from August 2009 through June 2010. Polysomnography variables including apnea-hypopnea index (AHI), supine AHI, non-supine AHI, time spent in supine sleep position of the total sleep time and positional dependency (PD) were analyzed. Obstruction sites were evaluated as SVF variables.
Results
Of 91 patients, 65 (71.4%) were positional patients (PP) and 26 (28.6%) were non-positional patients (NPP). An analysis of polysomnography variables according to PD revealed that overall AHI, non-supine AHI and supine AHI in PP was significantly lower than that in NPP. The patients with soft palate obstruction (SP type) were more likely to have PD than the patients with tongue base obstruction (TB type; P=0.046). PD was inversely related to OSAS severity significantly (P=0.001).
Conclusion
These results provide evidence that positional dependent patients may have higher success rate of soft palate OSA surgery alone than non-positional dependent patients. Although PD may be associated with obstruction site, PD only itself may not be useful in planning surgical treatment for OSAS.
Keywords: Obstructive sleep apnea, Polysomnography, Fluoroscopy, Airway obstruction, Tongue, Soft palate, Supine position
INTRODUCTION
Sleep physician & surgeons generally focus their attention on the diagnosis and treatment of obstructive sleep apnea syndrome (OSAS). Overnight polysomnography (PSG) in a sleep laboratory is the gold standard method for diagnosing OSA. Because full PSG may be difficult to obtain, expensive, or inconvenient, screening methods to diagnose OSAS have been investigated. In addition, PSG do not find out the major obstruction sites of sleep event.
Sleep videofluoroscopy (SVF) can be performed easily for a short period of time and is more economical than the use of either CT or MRI scans and also show the entire upper airway at one time and provides dynamic findings while patients are breathing during awake and asleep states. SVF is a good modality to visualize these dynamic airway changes, and the efficacy of SVF for airway evaluation in patients with OSAS has been demonstrated in our previous studies [1-5]. Those studies suggested that SVF may have role in differentiation OSAS from simple snoring, the selection of candidates for uvulopalatopharyngoplasty (UPPP) and the demonstration of mechanism of action of the mandible advancement device (MAD) [1-5]. Both PSG and SVF can be supportive each other to decide treatment methods such as surgery, MAD and positive airway pressure (PAP).
In 1984, Cartwright [6] defined positional patients as those OSAS patients in whom the apnea-hypopnea index (AHI) was at least twice as high in the supine position as in the lateral position. Positional therapy (the avoidance of the supine posture during sleep) appears to be an adequate form of therapy for positional patients [7]. However, little information exists as to whether avoiding the supine posture during sleep is a valuable form of therapy for these patients. Recent studies also showed clinical correlations between positional dependency and surgical outcomes [8,9]. But there are no data or research regarding correlation between positional dependency and SVF variables. If positional dependency has significant correlation with the obstruction site based on SVF, it should be considered more in clinical decision making for treatment of OSAS patients.
The purpose of this study is to find out associations between positional dependency and obstructive levels based on SVF in patients with OSAS.
MATERIALS AND METHODS
Patients
This study has conducted retrospectively to evaluate 91 patients (77 male, 14 female; mean age, 47.9 years; range, 19 to 71 years) who visited the Sleep Center at Seoul National University Hospital, Seoul, Korea, from August 2009 through June 2010. All patients underwent full-night nocturnal PSG and SVF. They were diagnosed as having OSAS with an AHI of greater than 5. Patients who spent less than 5% of total sleep time in either the supine or lateral position were excluded, as the goal of this study was focused on positional dependency. Patients who underwent previous oropharyngeal surgery were excluded from this study. This study was approved by the Institutional Review Board of Seoul National University Hospital (H-1110-061-381).
Polysomnography
PSG over a whole night was conducted without first night adaptation. Fifteen channels of data were collected following the standard PSG routine: electroencephalograms (EEG) at the C3-A2 and O2-A1 positions, bilateral electrooculograms (EOG), three electromyograms (EMG) for the chin and anterior tibialis muscles, an electrocardiogram (ECG) at lead II, oro-nasal airflow with a thermocouple, abdominal and thoracic volume changes with piezoelectric-type belts, snoring with a microphone and blood oxygen saturation (SpO2). The sleep position was identified by placing a sensor on the chest, which distinguishes between the supine and lateral position of the trunk, and confirmed by a sleep technician. All channels were recorded with a Grass model 15 and 78 (Grass-Telefactor, West Warwick, RI, USA) and collected using a digital computer system equipped with an analog-to-digital converter (NI PCI-6014; National Instruments, Austin, TX, USA) and self-developed software (Xomnia 2005). PSG data were scored by experts at Seoul National University Hospital according to the criteria developed by Kales and Rechtschaffen [10]. Apnea was defined as the complete cessation of airflow for at least 10 seconds. Hypopnea was defined as a substantial reduction in airflow (>50%) for at least 10 seconds or a moderate reduction in airflow for at least 10 seconds associated with electroencephalographic arousals or oxygen desaturation (≥4%). Six AHI was defined as the total number of apneas and hypopneas per hour of sleep [11].
Sleep videofluoroscopy
All patients underwent SVF as described in previous study [1,2]. In brief, patients were in the supine position on a C-arm table with their head on a pillow. They were instructed to breathe in and out naturally. Oxygen saturation was monitored throughout the examination. During normal respiration before sedation, an awake event was recorded for 15 seconds. Thereafter, sleep was induced by intravenous administration with midazolam (2 mg). After the patient fell asleep, the sleep event examinations started. Although oxygen saturation does not decrease, a 15-second respiratory state was recorded as a normoxygenation sleep event. When oxygen saturation dropped by 4% or more, two 15-second desaturation sleep events were recorded.
Evaluation of polysomnography variables
The PSG recordings were carried out using polygraphs and included the following parameters: AHI, supine AHI, non-supine AHI, longest apnea time and lowest oxygen saturation, time spent in supine sleep position of the total sleep time (%), positional dependency (PD). If the AHI in the supine position was more than twice as high as that in the lateral position, the patient was considered to have PD, according to the definition of Cartwright [6]. The patients were divided into two groups according to PD as positional dependent patients (PP) and non-positional dependent patients (NPP).
Evaluation of sleep videofluoroscopy variables
Upper airway obstruction was analyzed during two different states (normoxygenation sleep and desaturation sleep) using the recorded data. The obstruction types were classified as soft palate (SP) only type and tongue base (TB) only or mixed type by the presence of SP lengthening or TB obstruction during the desaturation sleep events.
Statistical analysis
The t-test was used to compare demographic findings and base line data between PP and NPP, but the Pearson's chi-square test was used to compare sex between the 2 groups. The t-test was also used to compare PSG variables according to PD. The Pearson's chi-square test was used to compare obstruction sites between PP and NPP. Finally, the linear-by-linear association was used to compare obstruction severity between the 2 groups. All results were expressed as the mean±SD. Statistical significance was assumed at P<0.05 for all variables. All statistical analyses were performed with SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic findings and baseline data according to PD
Of 91 patients, 65 (71.4%) were PP and 26 (28.6%) were NPP. NPP was, on average, 6 years younger than PP (P=0.035). No differences in sex were observed but BMI were significantly higher in NPP than those in PP. The mean BMI in NPP was 26.1 and that in PP was 28.1 (P=0.009). No significant differences between each of the groups were seen in other baseline data including tonsil size, palate-tongue position and Epworth sleepiness scale (ESS) score (Table 1).
Table 1.
Baseline data according to positional dependency
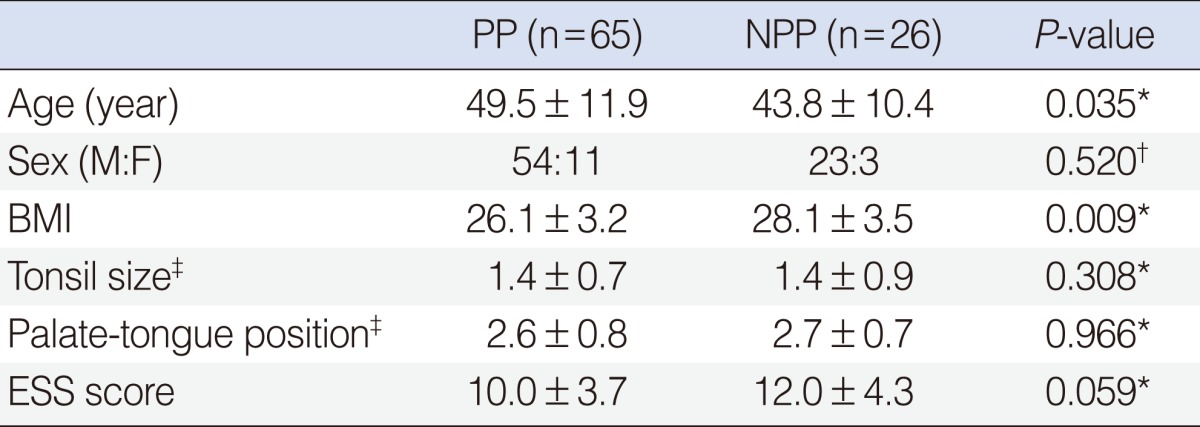
Values are presented as mean±SD.
PP, positional dependent patients; NPP, non-positional dependent patients; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); ESS, Epworth sleepiness scale.
*Student t-test was used. †Chi-square test was used. ‡Friedman clinical staging system [12].
PSG variables according to PD
Table 2 shows data on the comparison of various nocturnal sleep parameters between the two groups of PD. The mean overall AHI in NPP was 51.4 and that in PP was 25.4 (P<0.001). The mean non-supine AHI was 46.3 in NPP and 5.0 in PP (P<0.001). The mean supine AHI in NPP was 56.2 and that in PP was 40.0 (P=0.003). The proportion of supine sleep position was not significantly different between the 2 groups of positional dependency (P=0.268). No significant differences between each of the groups were seen in PSG variables including lowest saturation, longest apnea time.
Table 2.
Polysomnographic variables according to positional dependency
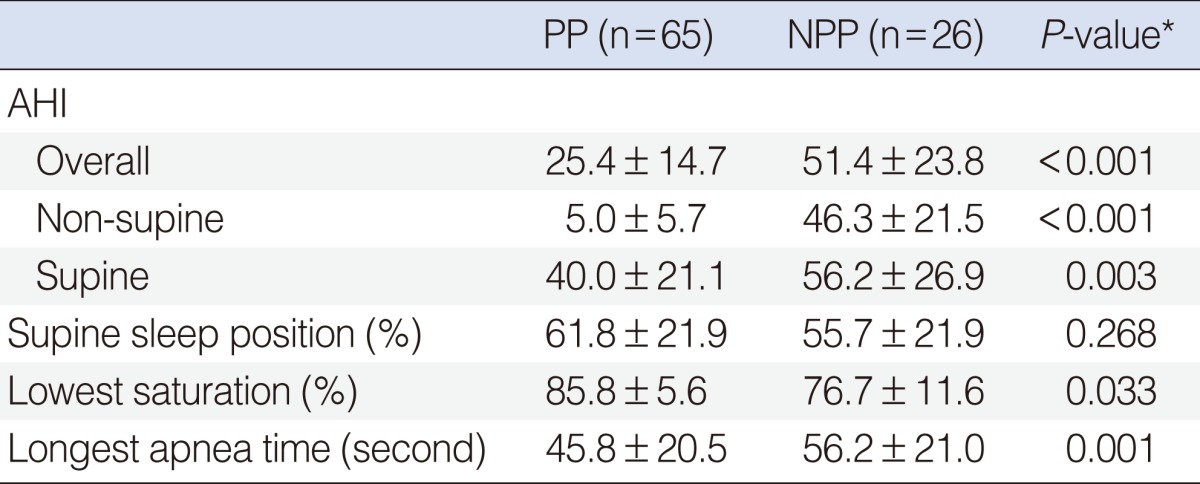
Values are presented as mean±SD.
PP, positional dependent patients; NPP, non-positional dependent patients; AHI, apnea-hypopnea index.
*Student t-test was used.
PD according to obstruction site and severity
Obstruction sites could be identified during desaturation sleep events of SVF. Of 91 patients, 43 (47.3%) were SP type and 48 (52.7%) were TB type. SP type was more likely to have positional dependency than TB type (P=0.046) (Table 3). In order to estimate the influence of OSAS severity, as expressed by AHI, the entire group of OSAS patients was first divided into three different AHI categories (5 to 15, mild; 15 to 30, moderate; >30, severe). Twenty-three patients had mild, 23 patients had moderate, and 45 had severe OSAS. The prevalence of PD in each category was calculated. The PD prevalence remained high and fairly steady (between 91.3% and 82.6%) in the mild-moderate categories, but showed a marked and significant reduction to 55.6% in the severe category. Thus, an OSA patient with a severe AHI is less likely to have PD than an OSA patient with a mild to moderate AHI (P=0.001).
Table 3.
Relation between positional dependency and obstruction sites

Values are presented as number of patients (%). Chi-square test was used (P=0.046).
PP, positional dependent patients; NPP, non-positional dependent patients; SP, soft palate; TB, tongue base.
DISCUSSION
The purpose of this study is to find associations between obstructive levels based on SVF and PSG variables in patients with OSAS.
This study has shown that 71.4% of the 91 adult OSAS patients whose conditions were diagnosed in our sleep clinic have at least twice as many apneas/hypopneas in the supine than in the lateral position. The percentage of PD in OSAS patients varies in different reports from 9% to 60% [13,14]. This variation is probably due to different types of OSAS patients studied. Little information exists about the relationship of positional dependency to the physical characteristics of the OSAS patients.
Present study showed that overall OSAS severity seems to be higher in TB type than that in SP type. However, there was no statistical significance. Our study showed that only non-supine AHIs in TB type were higher than those in SP type. The differences of non-supine AHI demonstrated in the present study are thought to be the obstruction effect of the tongue base in the oropharyngeal area. This result correspond well with a recent article which reported that the supine AHI was reduced significantly and the lateral AHI remained almost the same in positional patients after uvulopalatopharyngoplasty (UPPP) [9].
According to previous study [15], a severe, obese, and older OSAS patient is significantly less likely to be positional than a mild-moderate, thin, and young OSAS patient. And AHI was the most dominant factor that could predict the PD followed by BMI and age. Our study also showed that PD was inversely related to OSAS severity and BMI. And PP was older than NPP, which differ from the previous study. Because age thought to be an only minor contributing factor for PD, this inconsistency was not that controversial [15].
Many sleep physician & surgeons generally determined the treatment plan according to severity of OSAS. Our study results differ from these. Severity itself showed no relationship to obstruction sites. In addition, our study also showed that SP type was more likely to have PD than TB type. Since our results demonstrate that obstruction sites correlate better with PD than severity, we suggest that the treatment plan should be more considered by PD. Some patients with PD have succeeded in lowering their total AHI to normal by merely sleeping on their sides and it has been estimated that this type of therapy alone could be successful in treating [7,16]. Though PP are the ones in whom positional therapy (avoiding the supine posture) should play an important role in their treatment [16], long-term whole-night (during whole sleep time) positional therapy appears to be poor and alternative forms of therapy appear to be needed [17,18]. Results of the present study was consistent with the earlier study which reported that the overall success rates after UPPP were only 31.8% in NPP and 34.6% in PP and the supine success rates were somewhat higher in PP [9]. Therefore, our study implied that the OSAS patients with PD could be treated successfully after UPPP, only soft palate surgery, not multi-level surgery.
In conclusion, these results provide evidence that PP may have higher success rate of soft palate OSA surgery alone than NPP. Although PD may be associated with obstruction site, PD only itself may not be useful in planning surgical treatment for OSAS.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Lee CH, Mo JH, Kim BJ, Kong IG, Yoon IY, Chung S, et al. Evaluation of soft palate changes using sleep videofluoroscopy in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2009 Feb;135(2):168–172. doi: 10.1001/archoto.2008.538. [DOI] [PubMed] [Google Scholar]
- 2.Lee CH, Mo JH, Seo BS, Kim DY, Yoon IY, Kim JW. Mouth opening during sleep may be a critical predictor of surgical outcome after uvulopalatopharyngoplasty for obstructive sleep apnea. J Clin Sleep Med. 2010 Apr;6(2):157–162. [PMC free article] [PubMed] [Google Scholar]
- 3.Rama AN, Tekwani SH, Kushida CA. Sites of obstruction in obstructive sleep apnea. Chest. 2002 Oct;122(4):1139–1147. doi: 10.1378/chest.122.4.1139. [DOI] [PubMed] [Google Scholar]
- 4.Lee CH, Kim JW, Lee HJ, Yun PY, Kim DY, Seo BS, et al. An investigation of upper airway changes associated with mandibular advancement device using sleep videofluoroscopy in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2009 Sep;135(9):910–914. doi: 10.1001/archoto.2009.112. [DOI] [PubMed] [Google Scholar]
- 5.Lee CH, Kim JW, Lee HJ, Seo BS, Yun PY, Kim DY, et al. Determinants of treatment outcome after use of the mandibular advancement device in patients with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2010 Jul;136(7):677–681. doi: 10.1001/archoto.2010.106. [DOI] [PubMed] [Google Scholar]
- 6.Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7(2):110–114. doi: 10.1093/sleep/7.2.110. [DOI] [PubMed] [Google Scholar]
- 7.Cartwright RD, Lloyd S, Lilie J, Kravitz H. Sleep position training as treatment for sleep apnea syndrome: a preliminary study. Sleep. 1985;8(2):87–94. doi: 10.1093/sleep/8.2.87. [DOI] [PubMed] [Google Scholar]
- 8.Lee CH, Shin HW, Han DH, Mo JH, Yoon IY, Chung S, et al. The implication of sleep position in the evaluation of surgical outcomes in obstructive sleep apnea. Otolaryngol Head Neck Surg. 2009 Apr;140(4):531–535. doi: 10.1016/j.otohns.2008.12.023. [DOI] [PubMed] [Google Scholar]
- 9.Lee CH, Kim SW, Han K, Shin JM, Hong SL, Lee JE, et al. Effect of uvulopalatopharyngoplasty on positional dependency in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2011 Jul;137(7):675–679. doi: 10.1001/archoto.2011.99. [DOI] [PubMed] [Google Scholar]
- 10.Kales A, Rechtschaffen A. A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. Bethesda (MD): US National Institute of Health; 1968. [DOI] [PubMed] [Google Scholar]
- 11.Gould GA, Whyte KF, Rhind GB, Airlie MA, Catterall JR, Shapiro CM, et al. The sleep hypopnea syndrome. Am Rev Respir Dis. 1988 Apr;137(4):895–898. doi: 10.1164/ajrccm/137.4.895. [DOI] [PubMed] [Google Scholar]
- 12.Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg. 2002 Jul;127(1):13–21. doi: 10.1067/mhn.2002.126477. [DOI] [PubMed] [Google Scholar]
- 13.Lloyd SR, Cartwright RD. Physiologic basis of therapy for sleep apnea. Am Rev Respir Dis. 1987 Aug;136(2):525–526. doi: 10.1164/ajrccm/136.2.525b. [DOI] [PubMed] [Google Scholar]
- 14.George CF, Millar TW, Kryger MH. Sleep apnea and body position during sleep. Sleep. 1988 Feb;11(1):90–99. doi: 10.1093/sleep/11.1.90. [DOI] [PubMed] [Google Scholar]
- 15.Oksenberg A, Silverberg DS, Arons E, Radwan H. Positional vs non-positional obstructive sleep apnea patients: anthropomorphic, nocturnal polysomnographic, and multiple sleep latency test data. Chest. 1997 Sep;112(3):629–639. doi: 10.1378/chest.112.3.629. [DOI] [PubMed] [Google Scholar]
- 16.Cartwright R, Ristanovic R, Diaz F, Caldarelli D, Alder G. A comparative study of treatments for positional sleep apnea. Sleep. 1991 Dec;14(6):546–552. doi: 10.1093/sleep/14.6.546. [DOI] [PubMed] [Google Scholar]
- 17.Oksenberg A, Silverberg D, Offenbach D, Arons E. Positional therapy for obstructive sleep apnea patients: a 6-month follow-up study. Laryngoscope. 2006 Nov;116(11):1995–2000. doi: 10.1097/01.mlg.0000237674.66716.a7. [DOI] [PubMed] [Google Scholar]
- 18.Bignold JJ, Deans-Costi G, Goldsworthy MR, Robertson CA, McEvoy D, Catcheside PG, et al. Poor long-term patient compliance with the tennis ball technique for treating positional obstructive sleep apnea. J Clin Sleep Med. 2009 Oct;5(5):428–430. [PMC free article] [PubMed] [Google Scholar]