

Abstract
Introduction. Ten cases of dome-type adenocarcinoma of the colon have been reported so far. Most of them were presented as early lesions, with endoscopic and microscopic distinguishing features. Methods and Results. A raised plaque was removed from the right colon during colonoscopy in a 56-year-old man. Histopathological examination showed a cancerized adenoma invading the submucosa with several typical features of dome-type adenocarcinoma, in particular the associated prominent lymphoid tissue. Immunohistochemistry showed retention of the mismatch repair proteins MLH-1, MSH-2, MLH-6, and PMS-2. Conclusion. We report an additional case of dome-type adenocarcinoma of the colon as an early, low-risk, and microsatellite stable tumor, indicating that this particular histotype may deserve specific consideration for both classification and management.
1. Introduction
Since the initial reports back in late 90's & 2000's by De Petris et al. [1] and Jass et al. [2] 10 cases of dome-type (DC) adenocarcinoma of the colon have been reported [1–7]. DC is considered a rare variant of carcinoma of the colon presenting as a nonpolypoid plaque lesion, it is thought to derive from the specialized columnar M-cells of dome epithelium, which makes up in association with the gut-associated lymphoid tissue the domelike masses that bulge into the gut lumen [2].
Originating from this specific microenvironment, the most important morphological feature of DC is the association with a prominent lymphoid stroma.
We would like to add an additional case of this particular histotype that was recently diagnosed in our institute.
2. Case Presentation
A 56-years male with amyotrophic lateral sclerosis was colonoscoped because of painful constipation. There was no case of colorectal cancer in his family history.
An 8-mm raised plaque was seen in the right flexure (Figure 1) and removed.
Figure 1.
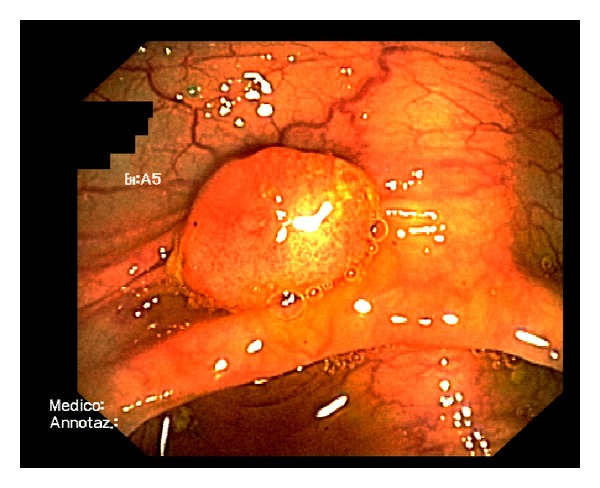
Conventional endoscopic image showing the dome-like lesion. A reddish rough mucosa can be seen in the top surface.
Routine histopathological examination showed a cancerized adenoma invading the submucosa associated with expanded lymphoid tissue encompassing several reactive germinal centres (Figures 2(a), 2(b), and 2(c)).
Figure 2.
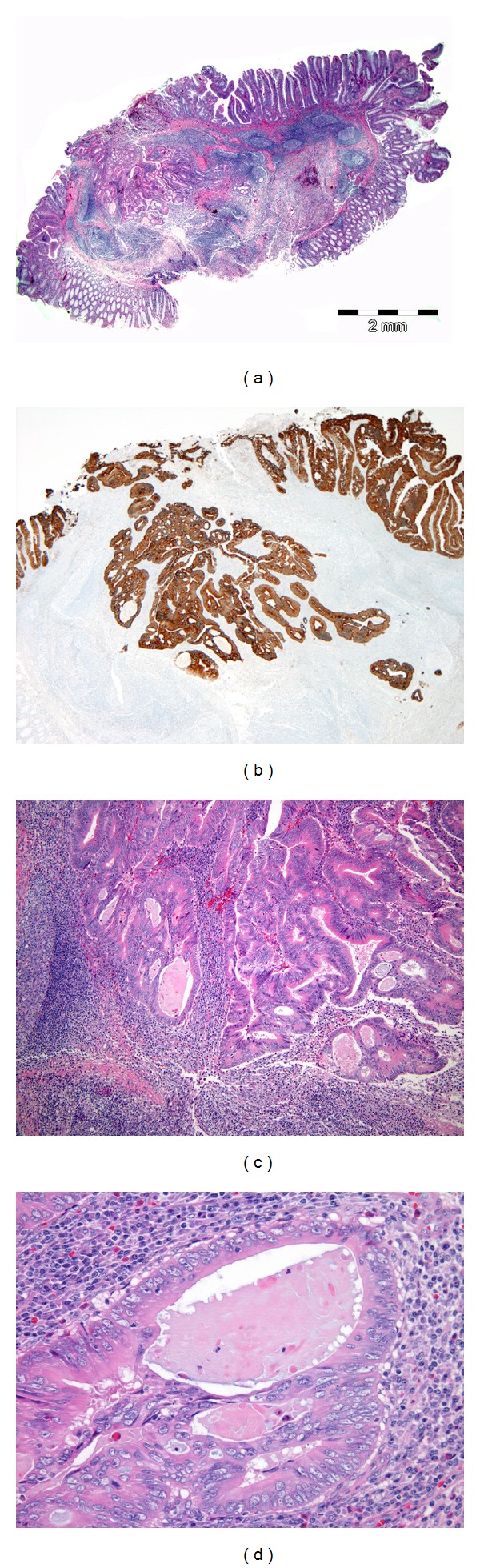
(a) Panoramic view of the tumor described. A well-demarcated tumor grows into the submucosa (hematoxylin-eosin, ×10). Overlying mucosa shows adenoma with high-grade dysplasia. Invasive adenocarcinoma associated with prominent lymphoid tissue encompassing several reactive germinal centres is observed in the submucosal layer. (b) Pan-Cytokeratin highlight tumor invasion. From the advancing edge few scattered foci of tumor budding arise (Cytocheratin AE1-3 ×20). (c) Histological architecture encompassing cystically dilated glands, in part cribriform arranged (hematoxylin-eosin, ×50). (d) The pink eosinophilic material filling the more dilated glands; a clear space separates the glandular epithelium from the intraglandular material (hematoxylin-eosin, ×200).
The cancer, arisen in a flat adenoma with high-grade dysplasia, was ulcerated superficially and the advancing edge appeared quite well circumscribed except for a more submucosa-invading tongue of neoplastic glands where some low-grade budding was observed (Figures 2(a), 2(b) and 2(c)).
The glands were in part cystically dilated containing a pink eosinophilic material, in part cribriform arranged (Figures 2(c) and 2(d)).
A clear space often separates the glandular epithelium from the intraglandular material.
Neoplastic cells lining the glands were columnar, single-layered, well-differentiated, eosinophilic (Figure 2(d)).
No tumor infiltrating lymphocytes nor goblet cells were observed. Necrosis and desmoplasia also were absent.
The T1 adenocarcinoma was considered a low-risk lesion because of the absence of lymphovascular invasion, the low-differentiation grade, and the negative resection margin, therefore no hemicolectomy was performed.
Immunohistochemistry showed retained expression of the mismatch repair proteins MLH-1, MSH-2 MSH-6, and PMS-2 in the neoplastic cells as well in the internal control (Figures 3(a), 3(b), 3(c), and 3(d), resp.).
Figure 3.
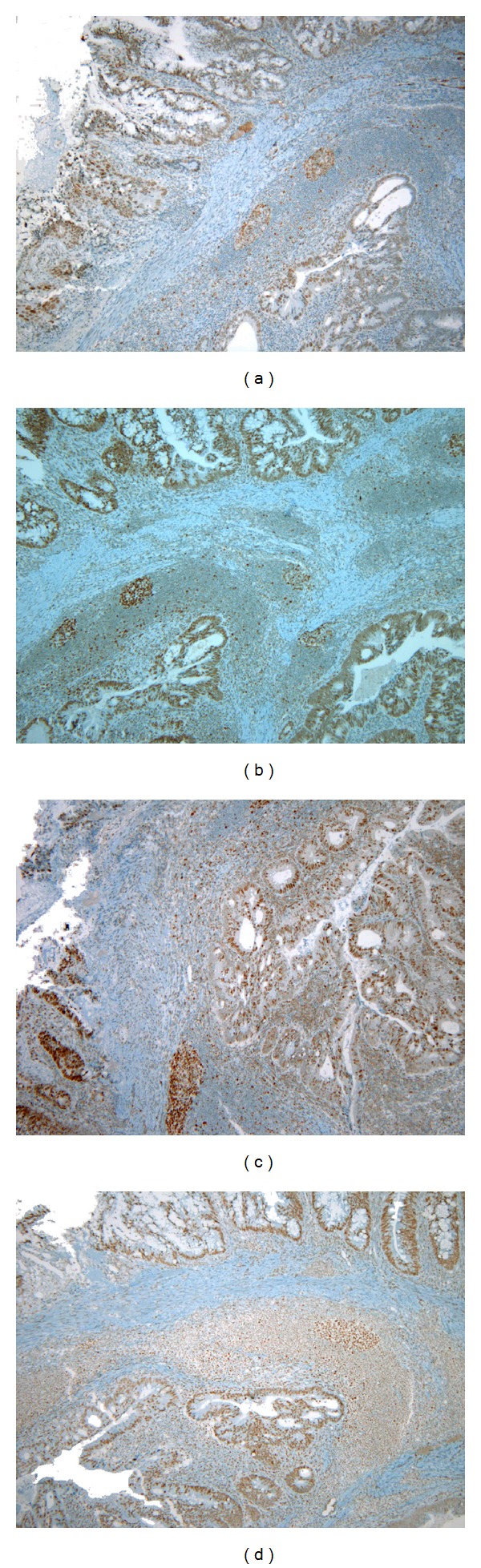
Immunohistochemical analysis of MLH-1, MSH-2, MSH-6, and PMS-2 protein expression in the DC. The neoplastic cells and the internal control (lymphocytes) are positive (a) for MLH-1 (×40), (b) for MSH-2 (×40), (c) for MSH-6 (×40), and (d) for PMS-2 (×40).
The patient underwent a follow-up colonoscopy one year later: the mucosal biopsies from the polypectomy site showed at histology mild fibroinflammatory changes.
3. Discussion
DC may develop as sporadic-type colon cancer or in association with ulcerative colitis, [6] familial adenomatous polyposis, [2] hereditary nonpolyposis colorectal cancer, [1] and other positive family history of colorectal cancer, [2, 5] in both right and left colon, therefore DC is not associated to any specific mechanisms of tumour predisposition.
Some distinguishing features both macroscopic and microscopic are constantly present: the nonpolypoid appearance, the cell architecture, the cytology, and the presence of prominent lymphoid tissue; other features such as the tumor infiltrating lymphocytes, the intra-acinar necrosis, the remnants of a preexisting adenoma and foci of usual-type adenocarcinoma of the colon may be present or absent.
Most cases are reported in the early growth phase: eight over ten case reported are T1N0, [1–6] one is T2N0 [3], and the last one is T3N0 [7]. No recurrence is documented so far and the patient presented with this report is one-year recurrence-free.
The case reported here of DC is another early and low-grade lesion, lacking features of biological aggressiveness, microsatellite stable tumor, suggesting that this particular histotype may deserve a space in the classification of tumors of the colon and rectum.
In the management of neoplastic colonic polyps DC per se may identify a low-risk malignant lesion, influencing the treatment decision-making process.
References
- 1.De Petris G, Lev R, Quirk DM, Ferbend PR, Butmarc JR, Elenitoba-Johnson K. Lymphoepithelioma-like carcinoma of the colon in a patient with hereditary nonpolyposis colorectal cancer. Archives of Pathology and Laboratory Medicine. 1999;123(8):720–724. doi: 10.5858/1999-123-0720-LLCOTC. [DOI] [PubMed] [Google Scholar]
- 2.Jass JR, Constable L, Sutherland R, et al. Adenocarcinoma of colon differentiating as dome epithelium of gut-associated lymphoid tissue. Histopathology. 2000;36(2):116–120. doi: 10.1046/j.1365-2559.2000.00864.x. [DOI] [PubMed] [Google Scholar]
- 3.Asmussen L, Pachler J, Holck S. Colorectal carcinoma with dome-like phenotype: an under-recognised subset of colorectal carcinoma? Journal of Clinical Pathology. 2008;61(4):482–486. doi: 10.1136/jcp.2007.047621. [DOI] [PubMed] [Google Scholar]
- 4.Clouston AD, Clouston DR, Jass JR. Adenocarcinoma of colon differentiating as dome epithelium of gut-associated lymphoid tissue. Histopathology. 2000;37(6):p. 567. doi: 10.1046/j.1365-2559.2000.01018-3.x. [DOI] [PubMed] [Google Scholar]
- 5.Coyne JD. Dome-type colorectal carcinoma: a case report and review of the literature. Colorectal Disease. 2012;14(6):e360–e362. doi: 10.1111/j.1463-1318.2011.02795.x. [DOI] [PubMed] [Google Scholar]
- 6.Stewart CJR, Hillery S, Newman N, Platell C, Ryan G. Dome-type carcinoma of the colon. Histopathology. 2008;53(2):231–234. doi: 10.1111/j.1365-2559.2008.03061.x. [DOI] [PubMed] [Google Scholar]
- 7.Yamada M, Sekine S, Matsuda T, et al. Dome-type carcinoma of the colon, a rare variant of adenocarcinoma resembling a submucosal tumor: a case report. BMC Gastroenterology. 2012;12(1):p. 21. doi: 10.1186/1471-230X-12-21. [DOI] [PMC free article] [PubMed] [Google Scholar]