

Abstract
Background:
There is no doubt that micronutrient deficiency is common in our environment. Replacements have thus been instituted without adequate information on specific and peculiar micronutrient needs of our people. Zinc is an essential micronutrient which is prone to maternal depletion during pregnancy and lactation. Unfortunately, studies in that regard in Nigeria has received diminutive interest.
Objectives:
To determine zinc concentration during pregnancy and lactation.
Methods:
This is a cohort study involving one hundred and twenty (120) pregnant women attending the antenatal clinic of one tertiary and two secondary health care institutions in Enugu. Thirty-five (35) apparently healthy, non pregnant women were used as control subjects. Atomic Absorption Spectrophotometer (AAS) was used to determine the zinc levels in the serum of the mothers during pregnancy, postpartum and in the breast milk.
Results:
Results showed that mean serum zinc levels were significantly decreased (P <0.0001) in pregnancy when compared with non-pregnant control subjects. The levels decreased as gestation progressed, with the lowest concentration of serum zinc obtained during the third trimester. It was also observed that serum zinc levels which decreased in pregnancy, increased non- significantly (P =0.12) in mothers postpartum. In the breast milk, zinc concentration decreased significantly (P <0.0001) as lactation progressed with the highest content evident in colostrum.
Conclusion:
The observed significant decreases in the levels of zinc during pregnancy and in breast milk places the mothers and their neonates at risk and thus, necessitate maternal supplementation. Dietary interventions such as food diversification and biofortification are recommended to improve dietary zinc intakes in pregnant and lactating mothers, and infants in this region.
Keywords: Zinc, pregnancy, lactation: Enugu: Nigeria
Introduction
Several epidemiological and prospective investigators and practitioners have accepted that micronutrients have a major function in many periods of a woman's life, particularly during pregnancy and lactation.1 Understandably, nutrient needs increase during pregnancy and lactation to support foetal growth and milk production respectively.2 Indeed, micronutrient deficiencies during pregnancy are associated with low birth weight, poor growth and development and sometimes neonatal and infant mortality. During lactation, a major reduction in the concentration of some of these nutrients in breast milk could occur and subsequently leads to infant depletion.3 Recent estimates indicate that globally, over two billion people are at risk for micronutrient deficiencies, despite recent efforts at prevention and management.4 These deficiencies are more pronounced during pregnancy and lactation, and in young children of Southeast Asia and sub-Saharan Africa.4
Zinc is an essential trace element in human and animal nutrition, with protective properties against endogenous or exogenous aggression, necessitated by the hyperproduction of highly reactive oxygen derivatives. It is an antioxidant, and also an effective ‘scavenger’, mopping up free radicals and reactive oxygen species.5 It is fundamental for growth, development, reproduction and immune response.6 Variations in plasma zinc concentration occasioned by disease, pregnancy, or stress and fluctuations in dietary intake are common.7 Zinc deficiency is estimated to be one of the commonest nutritional problems in the world.8 Indeed zinc deficiency in the female can lead to impaired synthesis/secretion of follicle stimulating and luteinising hormone, abnormal ovarian development, recurrent abortion, prolonged pregnancy and labour, teratogenicity, still births, pre-eclampsia, and low birth weight of infants.9
Human breast milk is a complex fluid, rich in nutrients and non-nutritional bioactive components.10 It is not only a source of nourishment but also a powerful antimicrobial agent.11 The quality of a mother's breast milk is very crucial for the optimal survival of the new born baby. In our environment, maternal malnutrition is common, and this has led to wild spread suggestions that routine micronutrient supplementation should be the rule. This supposition has led to the haphazard importation, into the Nigerian market, of numerous multivitamin and trace element compositions, with each drug company asserting superiority of its products over the others. Regrettably, there is paucity of information on maternal zinc status during pregnancy and lactation in our environment. Invariably, this has led to the production of supplements based on information that is completely extraterrestrial to our peculiar environment. In this regard, we decided to establish the baseline zinc status of our pregnant and lactating mothers to assist health care providers determine the actual amount of zinc required during pregnancy and lactation.
Subjects and Methods
Study Area
Created in 1991 from the old Anambra state, Enugu State is one of the 36 states of the Federal Republic of Nigeria. It has an approximate land mass of 8727.1km2 . It shares borders with Abia state to the south, Ebonyi state to the East, Benue state to the North East, Kogi state to the North West and Anambra state to the West. It has a mixed rural and urban population with majority being Igbo's, with a projected population of 3.3 million out of which about 50% are females. Enugu State has a crude birth rate of 45 per 1000, crude death rate of 18 per 1000 of the population and a life expectancy of 51years.12 The maternal mortality rate ranges between 750 and 850 per 100,000 life births.13,14 Enugu city is located in the hilly tropical environment about 230 m above sea level. The average annual temperature is between 23.1°C and 31°C with a rainfall of 1520 to 2030mm. There are two major seasons, rainy season (April to October) and dry season (November to February). The city has a population of about 464,514 inhabitants.
Study Design and Setting
This is a cohort survey, undertaken between March and December 2009. After obtaining ethical clearance and informed verbal consent, 120 pregnant women, 40 in each trimester; first (0-13 weeks), second (14-27 weeks) and third (28 weeks and above) were randomly recruited. They were attending the ante-natal clinic of one tertiary and two secondary health care institutions in Enugu. The selection was based on lucky dip of “YES” or “NO”. Women who had multiple pregnancies, obstetric haemorrhage, anaemia, fever, HIV positive, sickle cell disease, diabetes mellitus, malignancy, chronic alcoholics, tuberculosis, hypertension and any diagnosed inflammatory disorder in pregnancy were excluded. Also excluded were smokers and women on zinc supplements. The control group was made up of age and socioeconomic status matched 35 non-pregnant, non-lactating, apparently healthy mothers. They were recruited from the staff of UNTH and University of Nigeria, Enugu Campus (UNEC). The age range of the pregnant women was 19-42 years. Among those recruited, only 80 completed the study; twenty two (22) from the 1st trimester, 31 from the second trimester and 27 from the 3rd trimester.
Approval for the study was granted by the Ethics committee of the Hospital (ref: UNTH/CSA.329/Vol.6).
Methods
Socio-Economic Status of Subjects
Information on the socio-economic status was obtained by the administration of semi-structured, self-administered questionnaire. The socio-economic class was determined by the method of Szreter.15
Dietary Evaluation of Subjects
A 24-hour dietary recall interview was conducted for all the subjects to estimate their dietary zinc and calorie intake. In this method, the subjects were required to recall the individual's exact food intake during the previous twenty-four-hour period or preceding day. Detailed descriptions of all foods and beverages consumed, including cooking methods and brand names (where possible) were recorded. The amounts of nutrient intakes were calculated based on the nutrient composition of commonly eaten foods in Nigeria and other parts of the world.16,17
Anthropometric/Socio-Demographic Characteristics
The anthropometric/socio-demographic characteristics were obtained from the medical history, and physical examination. The weights were measured to the nearest 0.5 kilogram using a standard weighing scale (STADIOMETER, SECA, MODEL 220, GERMANY). The heights were measured in meters, with the same equipment without shoes, with the feet together, standing as tall as possible with the eyes level and looking straight ahead. Obstetric examinations, routine laboratory tests and ultra-sonography were performed.
Blood Sample Collection
About 5ml venous blood from the antecubital vein was collected from subjects at each period (pregnancy, and postpartum), using sterile, disposable syringes. The samples were transferred into sterile, anti-coagulant-free glass sample containers (plain tubes). Samples for the non pregnant group were collected on the 5th day of their menstrual cycle. The blood samples were allowed to stand for about thirty (30) minutes to clot and then centrifuged at 3,500 rpm for 15 minutes. The serum was collected and kept frozen at -20°C until analysed.
Breast Milk Sample Collection
Breast milk sample collection was carried out on the 3rd, 6th, 9th, 12th and 15th day after delivery since lactation did not commence on the day of delivery for most of the mothers. Breast milk samples (10ml) were collected from the lactating mothers by manual expression of the milk directly from the breast into sterile, plastic sample containers. After collecting the first 5ml, the baby was breastfed for 15 minutes and thereafter, an equal volume of hind-milk from the same breast was collected. After mixing thoroughly, the samples were immediately stored and frozen at -20°C prior to analysis. All milk samples were collected within the same period of the day (9.00 – 11.00 am) to avoid any possible diurnal changes.
Analysis of Zinc Concentration
Analyses (serum and milk) were done within two weeks of sample collection using Atomic Absorption Spectrophotometer (AAS), (Buck Scientific AAS/AES Model 205, United States of America).
Statistical Analysis
Analysis of data was done using SPSS version 11. Values were recorded as mean and standard deviation. D’Agostino & Pearson omnibus normality test was performed and data assumed Gaussian distribution. Consequently, a one way analysis of variance (ANOVA) followed by Scheffe's post hoc tests. P values < 0.05 were considered significant.
Results
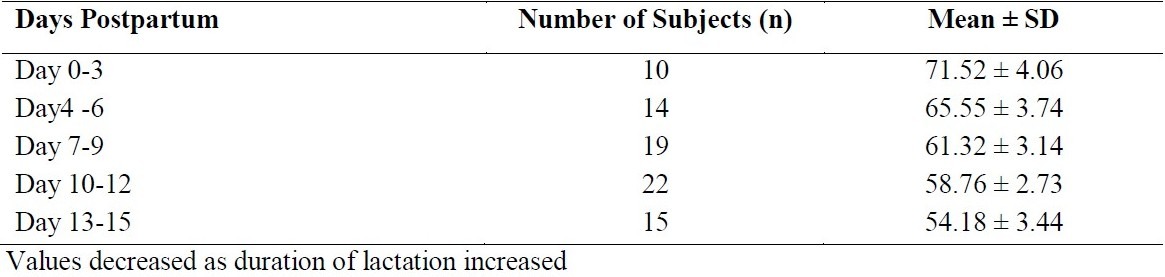
Table 1 represents the mean values of some anthropometric/sociodemographic characteristics of the subjects. The estimated daily zinc and caloric intake of the subjects did not vary significantly (P =0.54 and 0.62 respectively). The mean zinc level (μg/dl) in the control subjects was 109.75 ± 17.69. This decreased to 106.82 ± 19.76 in the 1st trimester, 101.65 ± 14.47 in the 2nd trimester and 85.57 ± 15.50 in the 3rd trimester. However immediately after delivery, the value rose to 90.66 ± 12.94. These values are statistically significant. (P <0.0001). However, after post hoc analysis, it was shown that the observed significant change is due to differences between controls versus 2nd trimester, control versus 3rd trimester and control versus postpartum. The level of zinc (μg/dl) in the breast milk (table 2) decreased significantly from 71.52 ± 4.06 on 0-3 days, 65.55 ± 3.74 4-6 days, 61.32 ± 3.14 7-9 days, 58.76 ± 2.73 10-12 days and 54.18 ± 3.44 13-15 days. (P <0.0001). Again, after post hoc analysis, it was observed that the differences between 7-9days and 10 -12days did not contribute to the statistically significant change.
Table 1.
Some Anthropometric, Socio-Demographic Characteristics and Estimated Daily Nutrient Intake
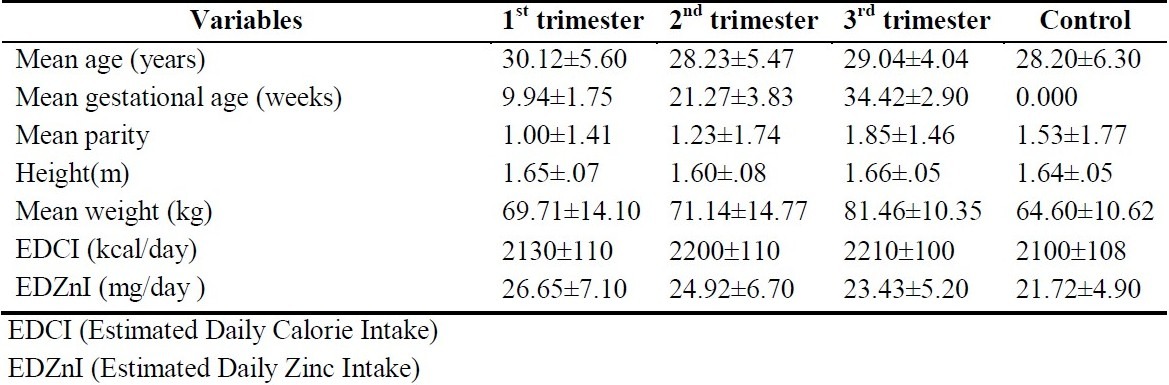
Table 2.
Mean Breast Milk Zinc Concentrations (μg/dl) at Different Days of Postpartum/Lactation Period
Discussion
There is no doubt that zinc status is an imperative nutritional parameter during pregnancy and lactation.18 Accordingly, the determination of its levels has become a valuable tool in the management of pregnancy and its complications. The results of this study revealed that there was a statistically significant decrease in mean serum zinc concentration in pregnancy when compared with non-pregnant subjects. The decrease was progressive with the lowest mean serum zinc levels obtained in the third trimester. Significantly lower serum zinc levels in pregnancy have been reported in earlier studies in different parts of the world.18,19,20
There is no doubt that the body's need for zinc is greatest during pregnancy, lactation, infancy and adolescence.9 Consequently, the need to increase zinc intake during pregnancy in this population through supplementation cannot be overemphasised. Several studies have continued to associate zinc deficiency with obstetric complications and hence continued to advocate increase in zinc intake during pregnancy and lactation.21,22 Indeed it has been reported that oxidative stress can result from deficiency of trace elements such as zinc, copper and selenium.23 Invariably, zinc supplementation reduces pregnancy complications, improves pregnancy outcome, foetal development, lactation and neonatal growth.21
In this study, it was established that serum zinc concentration which decreased in pregnancy, increased slightly, though non-significantly in mothers after the baby was delivered. The slight increase could result from the expulsion of the placenta which transports maternal zinc to the foetus. Furthermore, it has been shown that zinc absorption efficiency increases markedly in early lactation compared with preconception levels.2 Serum zinc homeostasis during pregnancy has been linked to placental hormones. As lactation commences, zinc is transferred from the mother to the breast milk.
In the present study, a progressive decline in the zinc concentrations of breast milk as the duration of lactation increased was demonstrated, with the highest concentration in colostrum (day 0-3 postpartum) and the least in mature milk (day 13-15 postpartum). The result is consistent with other reports which affirmed that concentrations of zinc in breast milk decreased significantly at successive stages of lactation.24,25 Indeed it has been demonstrated that the macronutrient, mineral and trace element composition of breast milk fluctuates to a great extent as the duration of lactation increased.24 Furthermore, breastfeeding routine/pattern; parity, age, and other maternal characteristics; regional differences, and in some situations, season of the year and maternal diet have been known to influence the concentration of breast milk constituents.26
This study forms a hinge in the establishment of serum zinc reference levels in pregnancy, postpartum and breast milk of mothers in this region. As a result, it should constitute the foundation for the formulation of sufficien micronutrient replacement policy for our pregnan and lactating mothers. Conversely, it would hav been more appropriate if we had recruited all th women in the first trimester and followed them u until delivery. Also there may have been some bia in the assessment of zinc intake from the dietar recall. Moreover, one month dietary recall wherever practicable gives superior dietar synopsis than a 24 hour recall. These will b addressed in further studies.
Our priority in developing countries shoul therefore be institution of a suitable strategy for th prevention and management of maternal undernutrition. This may require multipl interventions supported and promoted by differen delivery strategies. Food supplements should b fortified and micronutrients formulated to suit ou peculiar geographic and socioeconomic circumstances. This will go a long way to reduc the burden of maternal and infant morbidity an mortality. Furthermore, women should be educate on the importance of adequate and optimal macr and micronutrient intake during pregnancy an lactation.
References
- 1.Kontic-Vucinic O, Sulovic N, Radunovic N. Micronutrients in women's reproductive health: II. Minerals and trace elements. Int J Ferti Women's Med. 2006;51(3):116–124. [PubMed] [Google Scholar]
- 2.King JC. Effect of reproduction on the bioavailability of calcium, zinc and selenium. J Nutr. 2001;131:1355S–1358S. doi: 10.1093/jn/131.4.1355S. [DOI] [PubMed] [Google Scholar]
- 3.Allen LH, Graham JM. Assuring micronutrient adequacy in the diets of young infants. In: Delange FM, West KPJ, editors. Micronutrient deficiencies in the first six months of life. Basel: Vevey/S.Karger AG; 2003. [Google Scholar]
- 4.Ramakrishnan U. Prevalence of Micronutrient malnutrition worldwide. Nutr Rev. 2002;60:46–52. doi: 10.1301/00296640260130731. [DOI] [PubMed] [Google Scholar]
- 5.Gutteridge JMC. Antioxidants, nutritional supplements and life-threatening diseases. Br J Biomed Sci. 1994;51:288–295. [PubMed] [Google Scholar]
- 6.Kornberg A. Supplement to DNA Replication. San Francisco: W.H. Freeman Co; 1982. Origin of DNA on Earth; p. S224. [Google Scholar]
- 7.Hambidge KM, Casey CE, Krebs NF. Zinc. In: Mertz W, editor. Trace elements in human and animal nutrition. 5th ed. Vol. 2. New York: Academic Press; 1986. p. 246. [Google Scholar]
- 8.Prasad AS. Why a New Trace Element Journal? J Trace Elem Exp Med. 1988;1:1–2. [Google Scholar]
- 9.Bedwal RS, Bahuguna A. Zinc, copper and selenium in reproduction. Cell Mol Life Sci. 1994;50(7):626–640. doi: 10.1007/BF01952862. [DOI] [PubMed] [Google Scholar]
- 10.Prentice A. Breast milk calcium and phosphorus concentrations of mothers in rural Zaire. Eur J Clin Nutr. 1991;45:611–617. [PubMed] [Google Scholar]
- 11.Bamgbose O, Opeolu BO, Bamgbose JT. Levels of Zinc in Breast Milk of Selected Nigerian Women in Abeokuta Township, Ogun-State. Nig J Nutri Sci. 2008;29(1):153–160. [Google Scholar]
- 12.State Ministry of Health, Enugu Health Sector Reform: Implementing the District Health System. [Assessed on 30th August 2010];Posted. 2004 Available from: http://www.enugustate.gov.ng/ [Google Scholar]
- 13.Onah HE, Okaro JM, Umeh U, Chigbu CO. Maternal mortality in health institutions with emergency obstetric care facilities in Enugu State, Nigeria. J Obstet Gynecol. 2005;25(6):569–574. doi: 10.1080/01443610500231484. [DOI] [PubMed] [Google Scholar]
- 14.Ezugwu EC, Onah HE, Ezugwu FO, Okafor II. Maternal Mortality in a Transitional Hospital in Enugu, South East Nigeria. Afr J Reprod Health. 2009;13(4):67–72. [PubMed] [Google Scholar]
- 15.Szreter SRS. The Official representation of Social Classes in Britain, the United States and France: The Professional Model and “Les Cadres”. Comparative Studies in Society and History. 1993;35(2):285–317. [Google Scholar]
- 16.Oguntano EB, Akinyele IO. Nutrient Composition of commonly eaten foods in Nigeria; raw, processed and prepared. Ibadan, Nigeria: Food Basket foundation Publication series; 1995. [Google Scholar]
- 17.Paul AA, Southgate DAT, editors. The composition of foods. 4th ed. London: Her Majesty Stationery Office (HMSO); 1979. [Google Scholar]
- 18.Izquierdo-Alvarez S, Castanon SG, Ruata ML, Aragues EF, Terraz PB, Irazabal YG, et al. Updating of normal levels of copper, zinc and selenium in serum of pregnant women. J Trace Elem Med Biol. 2007;21(Suppl 1):49–52. doi: 10.1016/j.jtemb.2007.09.023. [DOI] [PubMed] [Google Scholar]
- 19.Martin-Lagos F, Navarro-Alarcon M, Terres-Martos C, Lopez-Garcia de la Serrana H, Perez-Valero V, Lopez-Martinez MC. Zinc and Copper concentrations in serum from Spanish Women during pregnancy. Biol Trace Elem Res. 1998;61(1):61–70. doi: 10.1007/BF02784041. [DOI] [PubMed] [Google Scholar]
- 20.Arnaud J, Preziosi P, Mashako L, Galan P, Nsibu C, Favier A et al. Serum trace elements in Zairian mothers and their newborns. Eur J Clin Nutr. 1994;48(5):341–348. [PubMed] [Google Scholar]
- 21.Tamura T, Goldenberg RL, Johnston KE, DuBard M. Maternal plasma zinc concentrations and pregnancy outcome. Am J Clin Nutr. 2000;71(1):109–113. doi: 10.1093/ajcn/71.1.109. [DOI] [PubMed] [Google Scholar]
- 22.Ashraf M, Nasrullah M, Javeed S, Salam A, Ahmad Z, Rauf R. Maternal Serum Zinc level; its associate with complications of labor. The Professional. 2001;8(3):383–386. [Google Scholar]
- 23.Al-Sayer H, Al-Bader A, Khoursheed M, Asfar S, Hussain T, Mathew A, et al. Serum values of copper, zinc and selenium in adults resident in Kuwait. Med Princ Prac. 2000;9:139–146. [Google Scholar]
- 24.Hannan MA, Dogadkin NN, Ashur IA, Markus WM. Copper, selenium, and zinc concentrations in human milk during the first three weeks of lactation. Biol Trace Elem Res. 2005;107(1):11–20. doi: 10.1385/BTER:107:1:011. [DOI] [PubMed] [Google Scholar]
- 25.Yamawaki N, Yamada M, Kan-no T, Kojima T, Kaneko T, Yonekubo A. Macronutrient, mineral and trace element composition of breast milk from Japanese women. Trace Elem Med Biol. 2005;19(2-3):171–181. doi: 10.1016/j.jtemb.2005.05.001. [DOI] [PubMed] [Google Scholar]
- 26.Domellöf M, Lönnerdal B, Dewey KG, Cohen RJ, Hernell O. Iron, zinc, and copper concentrations in breast milk are independent of maternal mineral status. Am J Clin Nutr. 2004;79:111–115. doi: 10.1093/ajcn/79.1.111. [DOI] [PubMed] [Google Scholar]