

Abstract
Background:
Intestinal helminthiasis is common in our environment and antihelminthic drugs are specie specific. Thus, need to identify and characterize the species cannot be overemphasized.
Objective:
To determine the prevalence of Ascaris Lumbricoides in Enugu Metropolis.
Methods:
A cross-sectional survey of 361 subjects in Enugu metropolis was carried out in this study. A single stool sample was collected for examination from the subjects, using appropriately labelled clean specimen containers. The prevalence of Ascaris Lumbricodes was determined using the kato-katz method. Data was obtained using questionnaires which were administered by the researchers to mothers and extended family members living in the same household.
Results:
Out of the 361 single stool samples collected, from the subjects (made up of 154 samples from mothers, 156 samples from children, and 51 samples from extended family members), 69 subjects (made up of 30 mothers, 27 children and 12 extended family members) were infected with Ascaris lumbricoides, giving an overall prevalence of 19.1%. Prevalence among the mothers, children and extended family members were 19.5%, 17.3% and 23.5% respectively.
Conclusion:
There is a high prevalence of intestinal Ascaris lumbricoides among subjects living in Enugu metropolis. Attention should be given by the government to periodically carry out mass deworming exercise among households involving mothers, children and extended family members and indeed the whole members of each household.
Keywords: Ascaris lumbricoides, prevalence, Nigeria
Introduction
Ascaris lumbricoides is probably the best known nematode parasite of man and is one of the 134 species of helminths claimed to infect the human alimentary tract.[1] One of the best scientific descriptions of Ascaris lumbricoides was given by Tyson in 1683. He referred to the parasite as Lumbricus teres; the superficial resemblance of dead roundworm with their pinkish color and cuticular annulations to earthworms may have influenced this choice of name although Tyson clearly demonstrated the difference between the two types of worm. Linnaeus in 1758 provided the present name while the name and description of the closely related Ascaris suum is attributed to Goeze in 1782. Ascaris lumbricoides is the type species of the genus Ascaris.
One billion people or 25 percent of the world's population harbor Ascaris lumbricoides, making it the most prevalent helminthiasis of humans. It is usually a mild disease with relatively low morbidity and mortality rates. The high global prevalence of ascariasis ultimately results in 20,000 deaths per year, mainly due to intestinal obstruction.
Studies have shown that Intestinal Ascariasis is quite common in Enugu.[2,3,4] In Calabar, it was found to be the commonest worm infestation among pre-school children with prevalence as high as 64.4%, followed by hookworm (10.4%) and Trichuris trichuria (1.1%).[5] Low socio-economic standards tend to affect the burden of ascariasis as the prevailing conditions favor the transmission of Ascaris lumbricoides as well as other geo-helminths. Akogun, 1998[6] stated that transmission of helminths is sometimes influenced by differences in environment, local population and socio-cultural habits, such that prevalence and intensity in two or more adjacent and ecologically similar communities differ especially among school-aged population. Also Tshikuka,1995[7] found out in his study in Democratic Republic of Congo (former Zaire) that the socio-cultural habit of bringing in extended family members into their nuclear households is a significant predictor of high intensity of ascariasis in the high socio–economic subdivisions. Though few studies have been carried out in Enugu in the past, most of them were either school or hospital-based study.[4,8]
This community based study was embarked upon to determine the burden of this common prevalent helminth at the family level. This we believe will give a better picture of its prevalence in Enugu when compared to the previous studies.[4,8]
Patients and Methods
This work was carried out in Enugu metropolis, the capital city of Enugu state in South East Nigeria. Enugu is located in the tropical rainforest zone of Nigeria. It has a maximum temperature of 29 – 34.5°C and minimum between 20 – 32°C with an annual rainfall of 1500mm. The climate oscillates between a dry season (November to April) and a wet season (May to October). The people of Enugu state live in an area of approximately 12,727.1 square kilometer of land. The population density per square kilometer is quite high (248 persons per sq. km).[9] Enugu metropolis covers an area of 85 square kilometers and has an estimated population of about 464,514 individuals. It lies within three local government areas namely: Enugu North, Enugu South, and Enugu East. These local governments consist of the urban, semi-urban, the rural areas and urban slums. Enugu south and Enugu East are mainly rural areas and farmlands. Enugu North is an urban centre. Some are high density while others are medium and low density areas.
This work was carried out in four different communities in Enugu North Local Government area namely: Ngwo camp, Agu-owa, Iva-valley and New-Haven. Ngwo camp, Agu-owa, and Iva-valley are high density areas (urban slums), while New Haven is a medium density area. The four communities worked on were purposefully selected by convenience sampling technique because of their peculiar features.
This was a cross-sectional study which involved interviewing mothers and extended family members from selected households using semi-structured questionnaire. Stool samples were collected from occupants of each household particularly the mother, children ≤ 5 years old and extended family member(s) where available. Analysis for the presence and intensity of Ascaris lumbricoides, in egg per gram (epg) stool was carried out using the standard kato-katz technique.[10]
Each selected household had at least a child under the age of 5 years. In a cluster of households, the first household that has < 5 years old child and also that gave an oral consent to participate in the research was selected. In a household where there was more than one child < 5 years of age, the eldest child who is <5 years child was selected as the index child. One household was randomly selected from each area because they have a common surrounding environment.
The houses in the communities were selected by systematic random sampling. In Ngwo camp, each line was considered as a house and a household selected from it. Household selection started from the community's major entrance and continued uphill. Only odd numbered houses were selected from each street of Agu-owa. For the streets with uncoordinated numbering, only the houses on the left were selected. One household was selected from each block in Iva-valley. A household in every other house in New-Haven was selected.
Data collection was done using a semi-structured questionnaire. The mothers and extended family members were interviewed face-to-face. On the day of interview, small, wide mouthed plastic bowls with tight fitting covers were taken and labelled thus: Community Code, Serial Number (as on questionnaire) and Name of Participant. The numbers of bowls given were according to the number of samples required. In each household, samples were collected from the mother/care giver, child between 6 months – 5 years old, and extended family members if present. Thus, per household, at least two bowls were given for sample collection.
The participants were asked to put a matchbox sized fresh morning stool into the corresponding containers. They were strictly instructed that the samples were to be collected according to the labelling on the container. That is, each participant should use the container with his/her name written on it. They were told the dangers that could arise if the labelling is not adhered to, which is, treating the uninfected and leaving the infected untreated if infection is present.
In the morning, the stool samples from each household were collected. In situations where they were not at home at the time of collection, the containers were kept at the doorpost, or on an agreed place, out of the reach of children, and away from sunlight, for collection. Those that could not produce fresh morning stools after the first day were visited the next day and samples collected. Some participants do not have morning stooling habit and so were asked to put in any stool produced between evening and morning. This was stored in a cool place for future collection.
The samples were taken immediately to the laboratory for examination. Stool samples were examined using the kato-katz technique.[10] This was used to obtain an estimate of intensity of infection with A. lumbricoides, reported as egg per gram (epg) stool. Reagent preparation and procedure for Kato-katz technique was according to that set by World Health Organization (WHO).
Prevalence and intensity of infection of all participants were compared amongst communities using binomial confidence intervals for percentages, chi square analysis and one-way analysis of variance (ANOVA) on log transformed data respectively. Level of significance was set at p < 0.05.
Results
A total of 361 single stool samples were collected from all the subjects made up as follows: 154 samples from the mothers, 156 from children and 51 from extended family members.
Out of the 361 single stool samples examined, samples from 69 persons (made up of 30 mothers, 27 children and 12 extended family members) from 61 households were infected with Ascaris lumbricoides giving an overall prevalence of 19.1%. This study also showed that A. lumbricoides was common in both high and medium density areas with prevalence ranging from 5.6% in medium density area to 24.9% in high density area. Highest prevalence in the communities was recorded in Iva-valley (29.2%), followed by Ngwo camp (27.7%), Agu-owa (14.5%) which were high density areas/urban slum and least in New-Haven (5.6%) which was a medium density area of the metropolis.
The prevalence of ascariasis among the subjects distributed according to their place of residence is shown in Table 1.
Table 1.
Prevalence of Ascariasis by place of residence
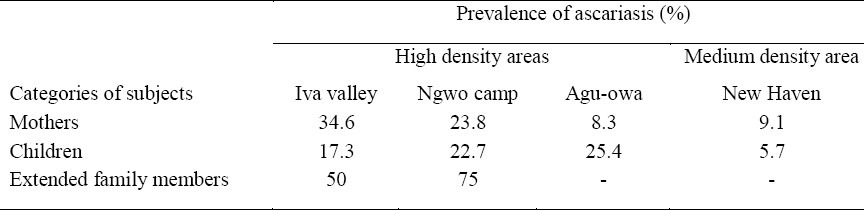
Within the subjects, extended family members had the highest prevalence (23.5%) followed by the mothers (19.5%) and then, the children (17.3%). Extended family members in Ngwo camp and Iva-valley (high-density areas) had the highest prevalence and there was no case of Ascariasis among those living in New-Haven, the medium density area. Mothers in Iva-valley had highest prevalence followed by those living in Ngwo camp, New-Haven and Agu-owa in decreasing order. Among the children, prevalence was high and similar in Ngwo camp and Agu-owa followed by Iva-valley and New-Haven.
These differences in prevalence among the subjects in the different communities are statistically significant in the mothers (P = 0.01) and extended family members (P = 0.003) but not in children (P = 0.175).
Of the 27 children infected, 15 (55.6%) were male and 12 (44.4%) were females. Infection among males was slightly higher in high-density area than in the medium density area where infection between subjects was the same.
Geometric egg output was highest in extended family members in the high density area ranging from 787.20 epg stool in those in Ngwo camp, 629.73 epg stool in Iva-valley to 400.00 epg stool in Agu-owa. A lower intensity was recorded among mothers and children in the medium density area (332.11 epg and 400.00 epg respectively). The overall total showed that intensity was highest in extended family members 598.67 epg, followed by children, 432.44 epg and least in mothers (389.06 epg). Kruskal-Wallis test showed that the intensity in the different communities were not statistically significant (P=0.345).
Categorising the intensity according to WHO standards showed that there were only light and moderate infections. The moderate infections recorded were all in extended family members. The result also showed a relationship between the intensity and age. Age of highest intensity was between 12.1 to 13.0 years.
Discussion
The prevalence of ascariasis in Enugu as determined by this study is still very high. This finding suggests an increasing trend in the burden of ascariasis when compared to the findings of Ozumba et al., 2002[8] in their hospital-based study which gave a prevalence of 14.3%. This prevalence is also much similar to the high prevalence rate of ascariasis documented by Ilechukwu et al., 2008[4] in Enugu even though their study was school-based. The findings in the index study showed a high rate and a better representation of the prevalence of ascariasis in Enugu metropolis being a community-based study and having involved both adults and children in different socio-economic classes.
Ozumba et al., 2002[8] showed that the age of highest prevalence was between 6 – 11 years. The age characteristic in this index study differed from that of Ozumba et al., 2002.[8] Our study showed the age of highest prevalence to be 13.0 ± 4.2 years. This could be because of the spread in subject and study locations. Theirs was based only on subjects that came to hospital while this study involved the wider community.
In the entire subjects within the communities, subjects in the medium density area showed the least intensity. None of the extended family members in this area was infected unlike in the mothers of the households. In Enugu metropolis, the main purpose of accommodating most of the extended family members was for mutual benefits i.e. they help in domestic chores and handling of food while they are being trained in school. The mothers in our study because of their higher educational level and with the purpose of taking helps at heart said that they deworm them and also teach and insist on good sanitary practices and personal hygiene. All those were in a bid to protect their children as well as the entire family. These mothers, on the other hand, believe that they and their children are worm-free and become a bit careless and do not deworm themselves as well. Unknown to them, they harbor A. lumbricoides while the extended family members were relatively worm-free.
The picture seen in the high density area in this study is not surprising and is in line with the finding of Fashuyi,1981 and 1987[11,12] who reported that the rate and intensity of infection and subsequent post treatment re-infection is higher in urban slums. The huge population concentration in these areas, coupled with unplanned nature of the settlement and total absence of municipal services like good drainage network, pipe borne water supply/portable water, and waste disposal facilities have increased the potential of infection. Again, in agreement with Croll and Ghadiran, 1981[13] another important factor which affects the level of infection is unequal exposure. Those in the high density areas are more exposed to the predisposing factors of Ascaris infection than those in the medium density. Prevalence was however low among the mothers from one of the high density areas (Agu -owa) compared to other high density areas. This is contrary to the expected norm since socio-environmental factors are known to play crucial roles in disease transmission.[14] Abuse of or self-medication with antihelminthics by these mothers could result in low prevalence. Self-medication is a common practice among Nigerian mothers and women.[15,16] Antihelminthic drugs or antibiotics generally with simple analgesics were the most self-medicated drugs reported in a study by Tenaw and Tsige,2004.[17] The relative cheap cost of antihelminthics and analgesics encourages easy access to these drugs and hence, self-medication.[18]
Ascaris Lumbricoides is still quite common in the tropics as documented in this study. Ascaris Lumbricoides was common in both subdivisions, with prevalence ranging from 5.6% to 29.2%. Prevalence was significantly higher in the communities classified as high population density areas when compared to the medium density area. The observed prevalence of Ascaris lumbricoides is still high when compared with the prevalences obtained from older studies in Enugu. Proper intervention by the government by way of provision of clean environment, social amenities and provision of free medications for planned periodical deworming programme will go a long way in reducing the burden of Ascariasis.
References
- 1.Crompton DWT. Ascaris and its Prevention and Control. London, New York and Philadelphia: Taylor and Francis; 1989. Biology of Ascaris lumbricoides. [Google Scholar]
- 2.Agugua NEN. Intestinal Ascariasis in Nigeria Children. J Trop Paed. 1983;13:237–40. doi: 10.1093/tropej/29.4.237. [DOI] [PubMed] [Google Scholar]
- 3.Onwasigwe CN. Intestinal Parasite in Enugu School Children. Orient J Med. 1999;11(1 - 4):56–60. [Google Scholar]
- 4.Ilechukwu CGA, Ilechukwu GC. Prevalence of Intestinal Helminthiasis in Pre-school and Primary School Children in Enugu, South-East Nigeria. Ebonyi Med J. 2008;7(1&2):42–6. [Google Scholar]
- 5.Anah MU, Ikpeme OE, Etuk IS, Yong KE, Ibanga I, Asuquo BE. Worm infestation and anemia among pre-school children of peasant farmers in Calabar, Nigeria. Nig J Clin Pract. 2008;11(3):220–4. [PubMed] [Google Scholar]
- 6.Akogun OB, Badaki J. Intestinal Helminth Infection in Two Communities along the Benue River Valley Adamawa State. Nig J Parasitol. 1998;19:67–72. [Google Scholar]
- 7.Tshikuka JG, Scott ME, Gray- Donald K. Ascaris Lumbricoides Infection and Environmental Risk Factors in an Urban African Setting. Ann Trop Med Parasitol. 1995;89(5):504–14. doi: 10.1080/00034983.1995.11812983. [DOI] [PubMed] [Google Scholar]
- 8.Ozumba UC, Ozumba N. Patterns of helminth infection in the human gut at the University of Nigeria Teaching Hospital, Enugu. Nig J Health Sci. 2002;48(3):263–8. [Google Scholar]
- 9. National Population Commission (NPC, 1991): Census Report.
- 10.Manual of Basic laboratory Methods in Medical Parasitology. Geneva: World Health Organization series. No. 69; 1991. World Health Organization. Kato–Katz technique. [Google Scholar]
- 11.Fashuyi SA. A Comparison of the Morphometric Characters of Two Geographically isolated Populations of Ascaris lumbricoides. Ind. J Hel. 1981;33:87–94. [Google Scholar]
- 12.Fashuyi SA. An Observation of the Dynamics of Intestinal Helminth Infections in two Isolated Communities in South Western Nigeria. Trop Geogr Med. 1987;40:226–32. [PubMed] [Google Scholar]
- 13.Croll NA, Ghadirian EA. Wormy Persons: Contributions to the Nature and Patterns of Overdispersion with Ascaris lumbricoides, Ancylostoma duodenales, Necator americanus, and Trichuris trichiura. Trop Geogr Med. 1981;38:241–8. [PubMed] [Google Scholar]
- 14.Ugbomoiko US, Dalumo V, Ofoezie IE, Obiezue RNN. Socio-environmental factors and ascariasis infection among school-aged children in Ilobu, Osun State, Nigeria. Trans R Soc Trop Med Hyg. 2009;103:223–8. doi: 10.1016/j.trstmh.2008.12.014. [DOI] [PubMed] [Google Scholar]
- 15.Sapkota AR, Coker ME, Rosenberg Goldstein RE, Atkinson NL, Sweet SJ, et al. Self-medication with antibiotics for the treatment of menstrual symptoms in southwest Nigeria: a cross-sectional study. BMC Public Health. 2010;10:610. doi: 10.1186/1471-2458-10-610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ene-Obong HN, Iroegbu CU, Uwaegbute AC. Perceived causes and management of diarrhoea in young children by market women in Enugu State, Nigeria. J Health Popul Nutr. 2000;18(2):97–102. [PubMed] [Google Scholar]
- 17.Tenaw A, Tsige G. Self-medication practices in Addis Ababa: a prospective study. Ethiop J Health Sci. 2004;14(1):1–13. [Google Scholar]
- 18.Worku S, Abebe G. Practice of Self-medication in Jimma Town. Ethiop.J.Health Dev. 2003;17(2):111–6. [Google Scholar]