

Abstract
OBJECTIVE
To evaluate the association between self-reported diabetes and the risk of breast cancer (BC) and its interaction with moderate-intensity physical activity in pre- and postmenopausal Mexican women.
RESEARCH DESIGN AND METHODS
A population-based case-control study was conducted using 1,000 incident case subjects and 1,074 control subjects. Blood samples and information on health, diet, physical activity, and anthropometric measurements were obtained.
RESULTS
The association between diabetes and BC risk decreased with increasing tertiles of moderate-intensity physical activity (odds ratio [OR] = 4.9 [95% CI 2.3–10.8]; 3.0 [1.3–6.9]; and 1.0 [0.1–9.2], respectively, for each tertile) (test for interaction = 0.04). Compared with the women in the lowest tertiles, increased risk was observed in those premenopausal women with the highest serum C-peptide, IGF-1, and IGF-1 binding protein 3 levels.
CONCLUSIONS
Moderate-intensity physical activity can substantially ameliorate the increased BC risk in diabetic women.
In Mexico, the prevalence of type 2 diabetes has shown a gradual rise in recent decades (from 6.7% of adults ≥20 years of age in 1993 to 14.4% in 2006). According to the 2006 National Health and Nutrition Survey (Encuesta Nacional de Salud y Nutrición 2006), its prevalence in women increases with age: 14.2% in women aged 50–59 years and 21.3% in those aged 60–69 years (1).
It has been suggested that diabetes increases the risk of breast cancer (BC) (2); however, physical activity appears to reduce the risk of BC (3) by increasing insulin sensitivity (4). Therefore, the aim of this study was to evaluate the effect of diabetes on the risk of BC in pre- and postmenopausal Mexican women, the interaction with moderate-intensity physical activity, and the association of several biomarkers, including IGF-1, its binding protein 3 (IGFBP3), and C-peptide with the risk of BC in a subsample of premenopausal women.
RESEARCH DESIGN AND METHODS
A multicenter, population-based, case-control study was conducted by the National Institute of Public Health in Mexico City, Monterrey, and Veracruz (including their metropolitan areas) from January 2004 through December 2007. Detailed methods and inclusion and exclusion criteria have been described elsewhere (3). In brief, 1,000 incident BC case subjects and 1,074 control subjects aged 35–69 years were selected. The case subjects were enrolled in the study soon after being informed about of their diagnoses (median = 3 days), were histologically confirmed, and had not been previously treated with chemotherapy or antihormonal therapy.
The control subjects were frequency matched to the case subjects by 5-year age categories, membership in a participating health care institution, and place of residence. They were enrolled at approximately the same time as the BC diagnoses. The control group was selected using a multistage probabilistic design.
After informed consent was reviewed and signed by all of the participants, information on health status, reproductive history, dietary intake, and physical activity was obtained through a questionnaire administered by trained nurses; fasting blood samples were obtained from all of the case and control subjects at recruitment. Information on diet and physical activity was obtained during a typical week prior to the first BC symptoms in order to reduce the possibility of reverse causation bias. Physical activity was estimated using a 7-day recall questionnaire that estimated an individual’s time spent performing physical activities (sleep and light-, moderate-, and vigorous-intensity physical activity) (5).
A history of diabetes was self-reported using the following question: Have you ever been diagnosed by a qualified physician as having diabetes (yes/no)? Self-reported diabetes has been used as an accurate disease measure (6,7).
Diet during the year prior to the onset of symptoms was assessed using a 104-item semiquantitative food frequency questionnaire by Willet (8) that had been adapted to the Mexican population and validated in Mexico City (9). Further details have been provided in a previous publication (3).
A random subsample of premenopausal women (244 case subjects and 320 control subjects) was selected for measuring: C-peptide, IGF-1, and IGFBP3. The blood samples were frozen at temperatures between −20 and −70°C and processed no later than 4 weeks after the blood was collected. The C-peptide, IGF-1, and IGFBP3 levels were determined using radioimmunoanalysis at Laboratorios Clínicos de Puebla, México (ISO 9001:2008).
This study was approved by the Ethics Committee of the National Institute of Public Health and the local committees from participating hospitals.
Statistical analyses
To evaluate the effect of moderate-intensity physical activity on BC risk, conditional logistic multiple-regression models were used to estimate odds ratios (ORs) and 95% CI (10). An interaction term (diabetes and moderate-intensity physical activity) was added to the model in postmenopausal women, and the effect of biomarkers on BC risk was assessed in premenopausal women. We exclude anyone diagnosed before 25 years of age to reduce the probability of including type 1 diabetes women (one pre- and four postmenopausal women). The models were a priori adjusted for 5-year age categories, health institution, site, well-known potential confounders, and European ancestry. Statistical analysis was performed using STATA version 10 (Stata Corp.).
RESULTS
Characteristics of study population have been described elsewhere (3). Overall, the women who reported a diabetes diagnosis had an increased risk of BC (OR = 2.1 [95% CI 1.5–2.8]). This association was statistically significant for the postmenopausal women (2.7 [1.7–4.1]) but not for the premenopausal women (1.4 [0.7–2.6]) (Table 1). Additionally, the effect of diabetes on BC risk in the postmenopausal women decreased with increasing tertiles of moderate-intensity physical activity: 4.9 (2.3–10.8) for the lowest tertile (≤5 h/week); 3.0 (1.3–6.9) for the second tertile (5.1 to <19 h/week); and 1.0 (0.1–9.2) for the highest tertile (>19 h/week). The P value for the interaction term comparing the lowest two tertiles combined and the highest (≤19 vs. >19 h/week) was 0.04.
Table 1.
Diabetes and BC risk in Mexican women residing in Mexico City, Monterrey, and Veracruz. Risk Factors for Breast Cancer in Mexico: Mammographic Patterns, Peptide C, and Growth Factors, a Multi-Center Study, 2004–2007
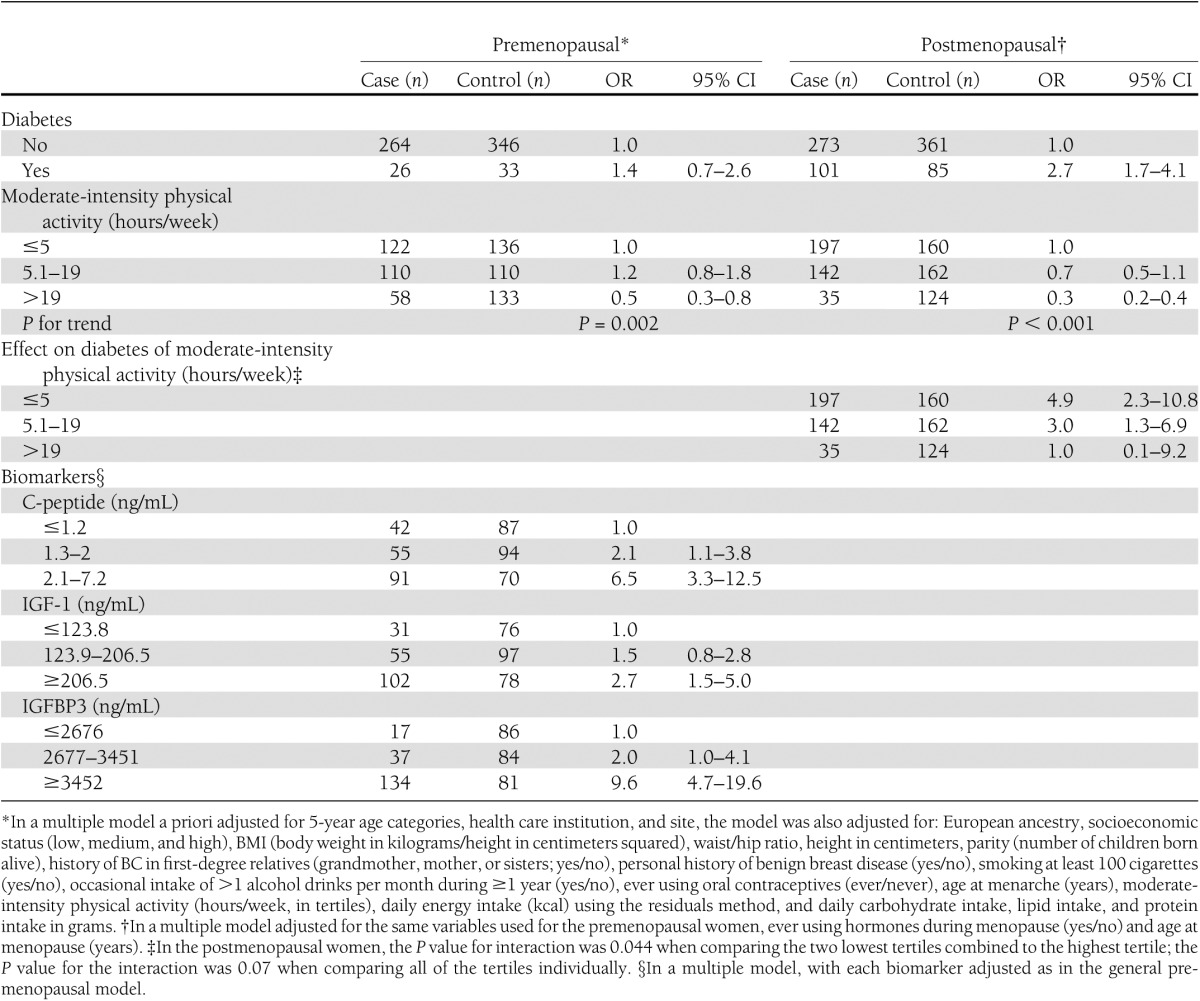
In the premenopausal subsample, a statistically significant association with BC risk was observed when comparing the highest C-peptide tertile versus the lowest (OR = 6.5 [95% CI 3.3–12.5]) and the highest IGF-1 and IGFBP3 tertiles versus the lowest tertiles (Table 1).
CONCLUSIONS
Our results suggest that moderate-intensity physical activity can substantially ameliorate the increased BC risk observed in diabetic women. These results are consistent with the results of other studies involving Hispanic women residing in the U.S. These studies have observed a protective effect against BC in diabetic women who exercise regularly, possibly through a reduced insulin resistance (11). Data from Mexico, Chile, Peru, Argentina, Brazil, and the multicountry Pan American Health Organization study showed a prevalence of adult physical inactivity from 50–91% (12–14). Given that higher serum levels of C-peptide, IGF-1, and IGFBP3 have been found to increase BC risk, further studies are required to address this issue. Our results suggest that IGF-1 and C-peptide offer a potential biological mechanism that explains the increased BC risk associated with diabetes. There is an urgent need to detect and treat diabetes early and promote physical activity to control weight and improve women’s health by improving public policy. Research on chronic disease prevention is a top research priority.
Acknowledgments
This study was supported by Consejo Nacional de Ciencia y Tecnología, the Mexican Research Program (Grant Salud 2002-CO1-7462 to G.T.-M.), and the National Institutes of Health (Grant R01-CA-120120 to E.Z.).
No potential conflicts of interest relevant to this article were reported.
G.T.-M., A.A.-L., C.O.-O., E.L.-P., E.Z., J.P.-R., M.d.J.G.-S., E.M.-Z., J.V.-L., and I.R. read and approved the final version of the manuscript. A.A.-L., C.O.-O., and E.M.-Z. analyzed the data and wrote the draft of the manuscript. E.L.-P., J.P.-R., and M.d.J.G.-S. performed critical review of the manuscript. E.Z., J.V.-L., and I.R. contributed to the discussion of the data and performed critical review of the manuscript. G.T.-M. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
References
- 1.Villalpando S, de la Cruz V, Rojas R, et al. Prevalence and distribution of type 2 diabetes mellitus in Mexican adult population: a probabilistic survey. Salud Publica Mex 2010;52(Suppl. 1):S19–S26 [DOI] [PubMed] [Google Scholar]
- 2.Larsson SC, Mantzoros CS, Wolk A. Diabetes mellitus and risk of breast cancer: a meta-analysis. Int J Cancer 2007;121:856–862 [DOI] [PubMed] [Google Scholar]
- 3.Angeles-Llerenas A, Ortega-Olvera C, Pérez-Rodríguez E, et al. Moderate physical activity and breast cancer risk: the effect of menopausal status. Cancer Causes Control 2010;21:577–586 [DOI] [PubMed] [Google Scholar]
- 4.Colberg SR, Grieco CR. Exercise in the treatment and prevention of diabetes. Curr Sports Med Rep 2009;8:169–175 [DOI] [PubMed] [Google Scholar]
- 5.Sallis JF, Haskell WL, Wood PD, et al. Physical activity assessment methodology in the Five-City Project. Am J Epidemiol 1985;121:91–106 [DOI] [PubMed] [Google Scholar]
- 6.Oksanen T, Kivimäki M, Pentti J, Virtanen M, Klaukka T, Vahtera J. Self-report as an indicator of incident disease. Ann Epidemiol 2010;20:547–554 [DOI] [PubMed] [Google Scholar]
- 7.El Fakiri F, Bruijnzeels MA, Hoes AW. No evidence for marked ethnic differences in accuracy of self-reported diabetes, hypertension, and hypercholesterolemia. J Clin Epidemiol 2007;60:1271–1279 [DOI] [PubMed] [Google Scholar]
- 8.Willet W. Nutritional Epidemiology. 2nd ed New York, Oxford University Press, 1998 [Google Scholar]
- 9.Hernández-Avila M, Romieu I, Parra S, Hernández-Avila J, Madrigal H, Willett W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Publica Mex 1998;40:133–140 [DOI] [PubMed] [Google Scholar]
- 10.Hosmer DW, Lemeshow S. Model-building strategies and methods for logistic regression. In Applied Logistic Regression. 2nd ed Canada, John Wiley & Sons, 2000 [Google Scholar]
- 11.Sanderson M, Peltz G, Perez A, et al. Diabetes, physical activity and breast cancer among Hispanic women. Cancer Epidemiol 2010;34:556–561 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hernández B, de Haene J, Barquera S, et al. [Factors associated with physical activity among Mexican women of childbearing age]. Rev Panam Salud Publica 2003;14:235–245 [in Spanish] [DOI] [PubMed] [Google Scholar]
- 13.Pratt M, Jacoby ER, Neiman A. Promoting physical activity in the Americas. Food Nutr Bull 2004;25:183–193 [DOI] [PubMed] [Google Scholar]
- 14.Jacoby ER. PAHO regional consultation of the Americas on diet, physical activity and health. Food Nutr Bull 2004;25:172–174 [DOI] [PubMed] [Google Scholar]