

Abstract
Several investigators have studied the horizontal relationship between incisive papilla and maxillary central incisor and measured the papilla incisor distance in dentate subjects to extrapolate this distance as a guide to place maxillary central incisors in complete dentures. Based on this premise, incisive papilla is recognized as an important landmark in complete denture construction. Papilla incisor measurements were made either from the middle or posterior border of the papilla and certain ethnic and national norms have been recommended to set the central incisors in complete dentures. This study was done on Dravidian dentate subjects to relate incisive papilla to central incisors and canines and also to ascertain its shape. During its transition to the edentulous state, incisive papilla changes its shape consequent to remodeling of the alveolar bone, palatal mucosa and interdental papilla following extraction of central incisor teeth. It was found that the papilla in dentate is not always round but seen in several forms. In some it was a double papilla and in a few it was rudimentary. The center of the papilla also changes from its dentulous to edentulous state. The posterior border is a relatively stable landmark since it undergoes least change after extraction of anterior teeth.
Keywords: Classification of incisive papilla, Shape of incisive papilla, Papilla incisor distance, Canine–papilla–canine line (C–P–C line), Dentulous incisive papilla, Arrangement of upper anterior teeth
Introduction
The labial fullness of maxillary anterior edentulous ridge is dependant on alveolar resorption and bone remodeling after the extraction of upper anterior teeth [1, 2]. Alveolar resorption and atrophy causes the lip to move inward and there is loss of facial contour. The labial contour of upper occlusal rim which restores facial contour, lip support and appearance is usually determined by the visual judgement of the Prosthodontist and the esthetic preference of the denture wearer during jaw relation stage (Fig. 1). To a certain extent pre-extraction record is a reliable guide to establish the labial contour of the denture wearer to his original facial contour if natural anterior teeth are present. Though the neutral zone theory of setting anterior teeth in a physiological location appears rational, it may not always produce the desired esthetic result.
Fig. 1.

Labial contour of upper occlusal rim is a guide for anteroposterior position of central incisor and canine teeth
The horizontal relationship between the incisive papilla and the maxillary central incisors in the dentulous is a guide to position the central incisor teeth as nearly as possible in their original location to restore labial contour in edentulous subjects [3–15] (Fig. 2). This is based on studies in Caucasians, besides a few in French, Jordanian, Chinese, Korean, and Thai [16–23]. The norms recommended for the Caucasians and others may not be applicable to Indian subjects and there is a need to obtain a national guideline for the various ethnic groups. The BPS recommendation (Ivoclar Vivadent AG Schaan, Liechtenstein) based on Caucasians may not be applicable to our population. This study was designed to ascertain the relationship of maxillary central incisor teeth to incisive papilla and the location of incisive papilla to the inter-canine line in the Dravidian population of Indian subcontinent [24]. The shape of the incisive papilla in dentulous was also investigated since it can influence the center of the edentulous papilla from the dentulous state.
Fig. 2.
Incisive papilla—central incisor relation in the horizontal and vertical planes in the dentulous. Edentulous papilla is a guide to set central incisors in complete dentures
Reference Landmark—Anterior Border, Center or Base of Dentulous Papilla
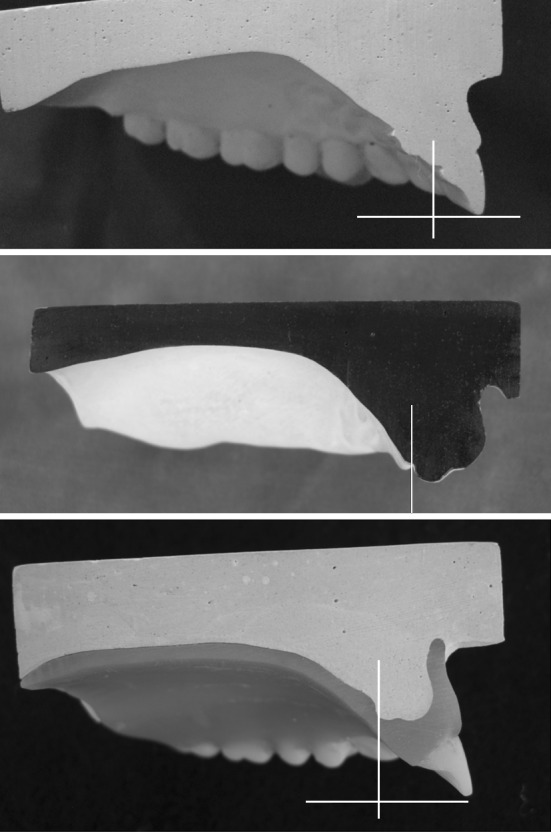
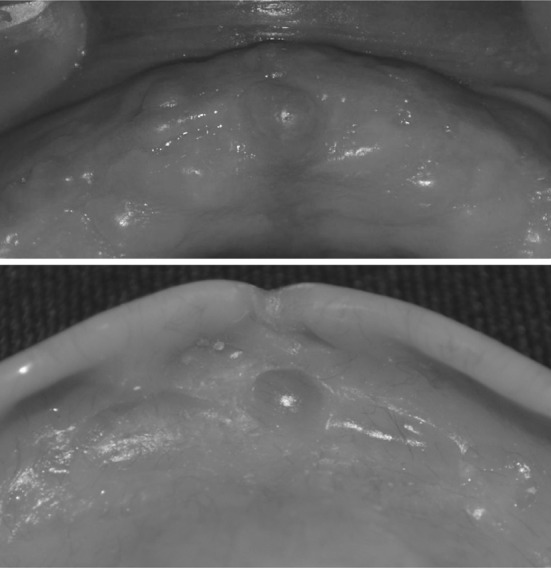
The center/middle or the base/posterior border of the papilla are mostly used as reference (Fig. 3) for papilla-incisor measurements (Table 1). Anterior border and center of incisive papilla are likely to change after extraction of incisor teeth, while the posterior border is relatively stable (Fig. 4). Papilla becomes round after extraction of incisor teeth due to changes in the anterior border. During edentulous transformation as the papilla changes to round form, its center also changes. There is a shift in the center of the papilla from the dentulous to edentulous state. In dentulous subjects incisive papilla is seen in various shapes and this change will be more in a long papilla compared to a short papilla (Fig. 5). The anterior border of the papilla is not a reliable landmark particularly when the papilla is continuous with the interdental papilla, since post extraction changes occur at the anterior border. The base/posterior border is a reliable landmark as it is definable and subject to least change in the edentulous state.
Fig. 3.
The center and base of the papilla used as reference
Table 1.
The distance between the incisive papilla and labial surface of upper central incisors according to various authors
| Author | Midpoint of incisive papilla in mm | Posterior border of incisive papilla in mm |
|---|---|---|
| Lau and Clark McGee |
9.17 8.00 |
12.71 |
| Mavroskoufis, Richie Ehrlich and Gazit |
10.2 12.31 |
|
| Ortman, Tsao, Harper | 5–8 | 12.45 |
| Grave and Becker | 13.17 | |
| Watts and Likeman | 10.00 | |
| Hickey, Boucher, Woelfel | 8–10 | |
| Martone | 8–10 | |
| Murray | 8–10 | |
| Young Seok et al. | 11.96 | |
| Sawiris | 8.5 | |
| Klang SH | 9.4 | |
| BPS Ivoclar | 7 |
Fig. 4.

Papilla changes its shape after extraction of central incisor teeth
Fig. 5.

Long papilla
Lip Support in Complete Dentures
In complete denture, maxillary anterior teeth play an important role in providing lip support and labial contour. When placed too far posterior, then the upper lip is unsupported and there is loss of muscle tone. Contrarily, the lip is stretched when the anterior teeth are placed too far forward. The loss of muscle and tissue tone and stretching of lip affect facial expression and appearance. Positioning anterior teeth in the neutral zone in complete denture permits a balance of muscular forces between the upper lip and the tongue. However, this is more beneficial for the stability of the denture than providing a pleasing labial contour.
The labial contour of a denture wearer as seen from front and in profile is initially achieved by the clinician while he builds and shapes the labial surface of upper occlusal rim at the time of jaw relation record (Fig. 1). The incisive papilla central incisor distance based on the dentulous biometric norm is a guide to form labial contour of occlusal rim in laboratory, which is later confirmed chairside by the clinician and subsequently to set upper central incisors in the dental arch (Fig. 6). As early as 1948 Harper stated “When artificial are set in proper position, which may be determined by the incisive papilla, the foundation is correctly laid for natural speech, pleasing appearance and normal function [3]”. The position of papilla in the articulated upper cast also helps to verify labial contour of occlusal rim obtained by the clinical method. Besides, canine–papilla line is a useful guide to orient the upper canine teeth in complete dentures.
Fig. 6.

Incisive papilla seen through palatal window is a guide to form labial contour of upper occlusal rim and to set the central incisors and canines
Incisive Papilla
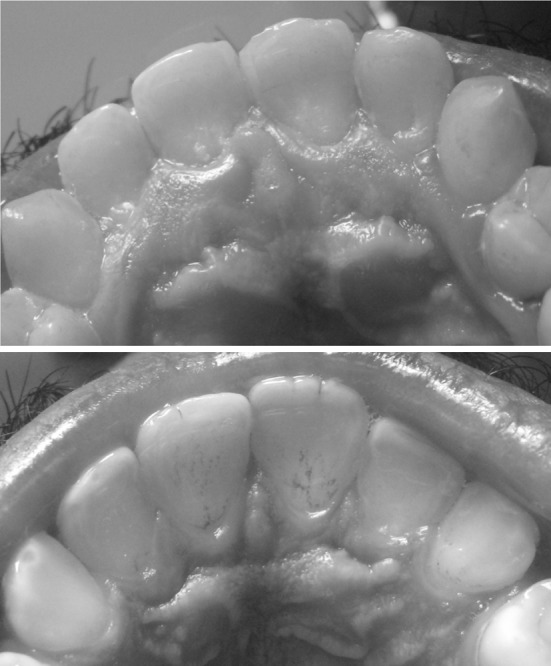
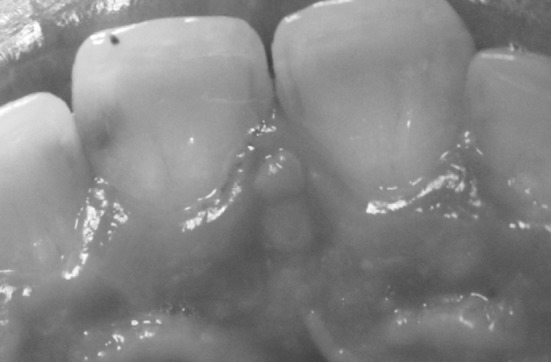
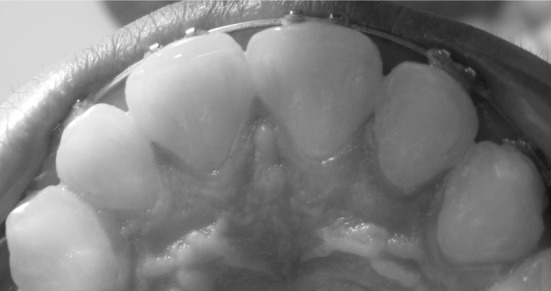
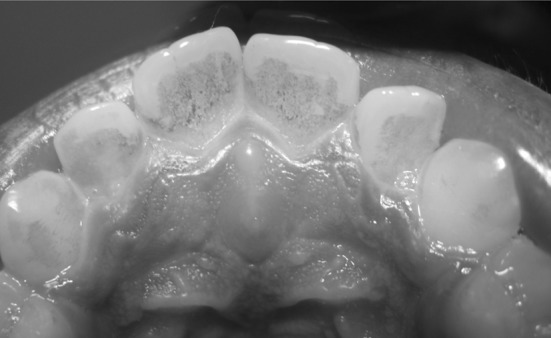
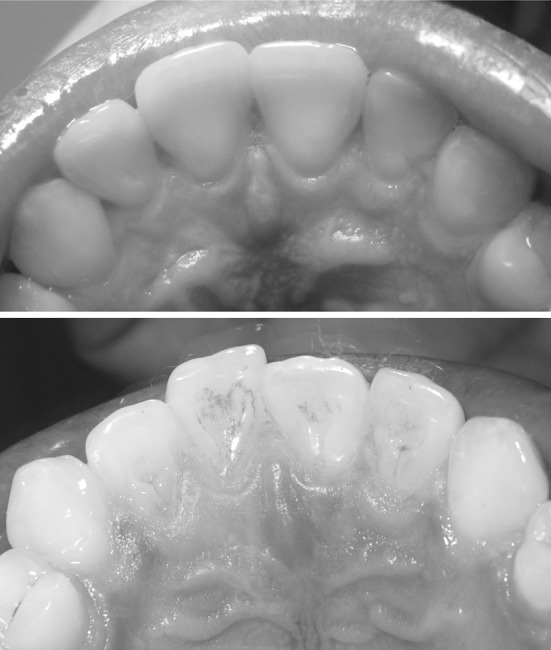
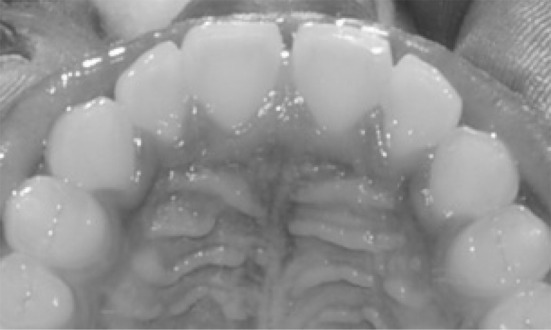
The incisive papilla otherwise known as palatine papilla is a small pear or oval shaped mucosal prominence situated at the midline of the palate, posterior to the palatal surface of the central incisors. In dentulous subjects, it is seen in various forms either discrete or continuous with the interdental papilla of the upper central incisors (Fig. 7). In the edentulous maxilla it becomes round, present behind the crest of the residual ridge or on the tip of the ridge (Fig. 8). Harper [3] found the position of the incisive papilla in the edentulous remained fairly constant since resorption took place in an anteroposterior direction. Progressive bone loss of the labial alveolar bone gives an illusion that the papilla has moved forward (Fig. 8).
Fig. 7.
Discrete papilla, papilla continuous with interdental papilla and papilla continuous with rugae
Fig. 8.
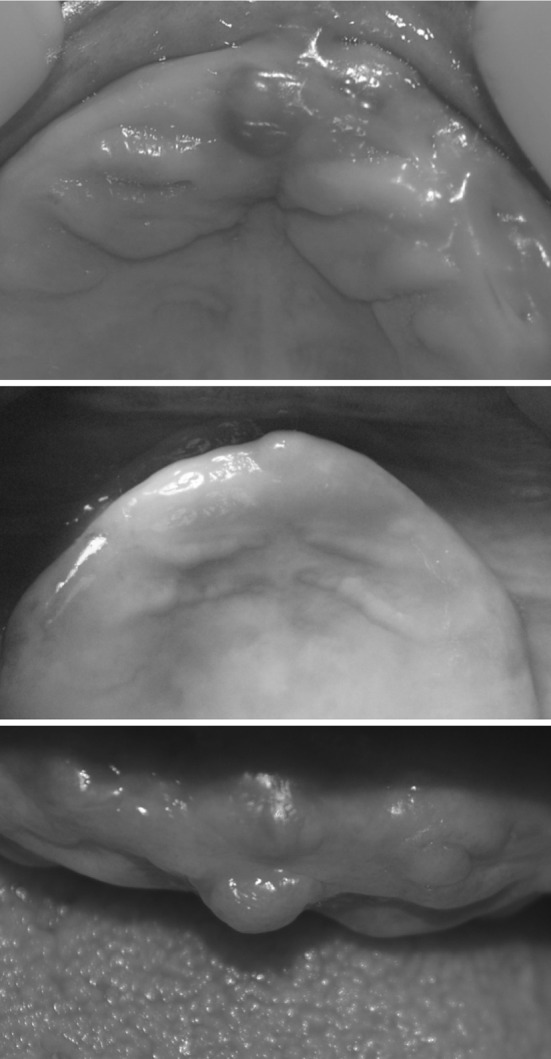
In the edentulous state IP changes its shape and lies behind the crest or tip of alveolar ridge
Histologically it consists of firmly interwoven fibers of dense connective tissue and is believed to contain the oral parts of the vestigial nasopalatine ducts, which are blind epithelial ducts of varying lengths [25, 26]. It is lined by simple or pseudostratified columnar epithelium which is frequently keratinized. The incisive papilla is generally situated over the incisive foramen through which emerge the nasopalatine nerves and palatine vessels. Watt and Likeman [27] found that the papilla moved forward about 1.6 mm as a result of maxillary alveolar bone resorption and the incisive fossa lies slightly posterior to the papilla. Pressure on papilla by the maxillary denture can result in pain or burning sensation requiring relief (Fig. 9).
Fig. 9.
Incisive papilla requires relief in denture
Studies on Papilla Incisor Distance Earlier to This Study (1982)
| Harper [3] | 5–8 mm |
| McGee [4] | 8 mm |
| Hickey, Boucher and Woelfel [6] | 8–10 mm |
| Martone [7] | 8–10 mm |
| Schiffman [8] 507 subjects | – |
| Ehrlich (1975) 430 casts | – |
| Watt (1976) | 8–10 mm |
| Ortman and Tsao [10] 38 casts | 12.45 mm |
| Mavroskoufis and Ritchie [11] 64 students | 10.2 mm |
| Grave and Becker [14] | 12–13 mm |
| Lau and Clark [16] 82 subjects | 9.17 mm (mid point), 12.71 mm (post border) |
| Sawiris [29] | 8.5 mm |
| Ehrlich and Gazit [9] 507 casts | 12.3 mm |
Papilla Incisor Relationship: A Guide to Position Upper Central Incisors
Prior to 1948 the only reference of incisive papilla in text books was about its location in edentulous mouth and the effect of denture pressure on this area. Harper in 1948, after extensive longitudinal studies on preextraction and postextraction models was the first to show that the positional relationship of incisive papilla to the natural teeth offers valuable data in the treatment of edentulous patient [3]. He recognized that the incisive papilla is a dependable landmark to position the upper central incisors in the horizontal and vertical planes in complete denture. He found the horizontal distance between the papilla and central incisor was not less than 5 mm and not more than 8 mm. After a decade, McGee [4] stated that in order to place the upper central incisors in complete denture as close as possible to their original position, the average distance between the labial surface of central incisor to the papilla in natural dentition should be determined. He recommended to set the labial surface of central incisors 8 mm anterior to the papilla.
Hickey, Boucher and Woelfel in 1962 recommended that the labial surface of central incisors in dentures should be 8–10 mm anterior to the middle of papilla [6]. Martone in 1963 emphasized that the best guide in setting anterior teeth was the papilla incisor relationship and recommended the incisors should be 10 mm in front of the incisive papilla [7]. Marxkors [28] found papilla incisal distance was 8 ± 1 mm in 77 % of Germans. Mavroskoufis and Ritchie [11] believed that the incisive papilla is a stable landmark for arranging the labial surfaces of central incisors 10 mm anterior to the incisive papilla. They also recommended the tips of the canines should be set on a horizontal line which pass through the posterior border of incisive papilla. Since then several authors have studied the papilla incisor relationship in the dentulous and have suggested various norms to place the central incisors in complete denture [10–18, 20–24].
Method
250 dentulous subjects of Dravidian origin consisting of 125 males and 125 females in the 20–40 age group were randomly selected for the purpose of measurement between the labial surface of the upper incisor teeth and the incisive papilla. Alginate impression of the upper arch was obtained in these subjects with class 1 occlusion having normal arch form with full compliment of teeth, with good gingival and periodontal health, who fulfilled the selection criteria such as absence of caries, diastema, anterior restorations and no orthodontic treatment. Maxillary casts were made with Type 1 dental stone and the casts were used for further measurements. In each of the cast the following landmarks were selected and the distance between them was measured with a vernier caliper to the accuracy of tenth of a millimeter.
Incisive Papilla—Central Incisor Distance
The base of the incisive papilla and the most prominent labial convexity of the central incisor were taken as references for measuring the papilla incisor distance. A horizontal line was marked at the base of the incisive papilla. A second line was marked in the midsagittal plane to bisect the papilla. The point of intersection was taken as the reference point for measurement. Papilla-incisor distance was recorded to the tenth of a millimeter by adjusting the pointed arms of the vernier caliper to contact the reference point at the base of the incisive papilla and the maximum convexity of central incisor.
Inter-Canine Line
Photograph of each cast was taken to mark the inter-canine line and to find the relationship between the incisive papilla and the inter-canine line. The tip of canine on both sides was located on the cast with pencil mark and the line connecting these two points on the photograph was designated as inter-canine line.
Incisive Papilla—Inter-Canine Line
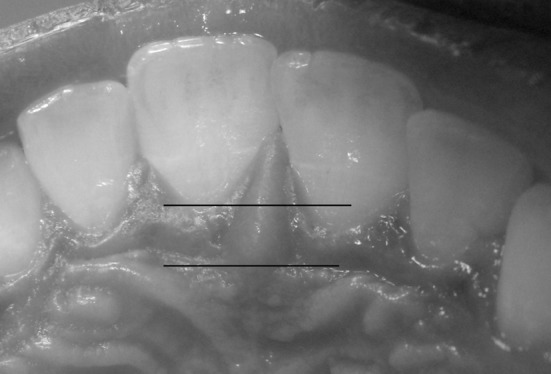
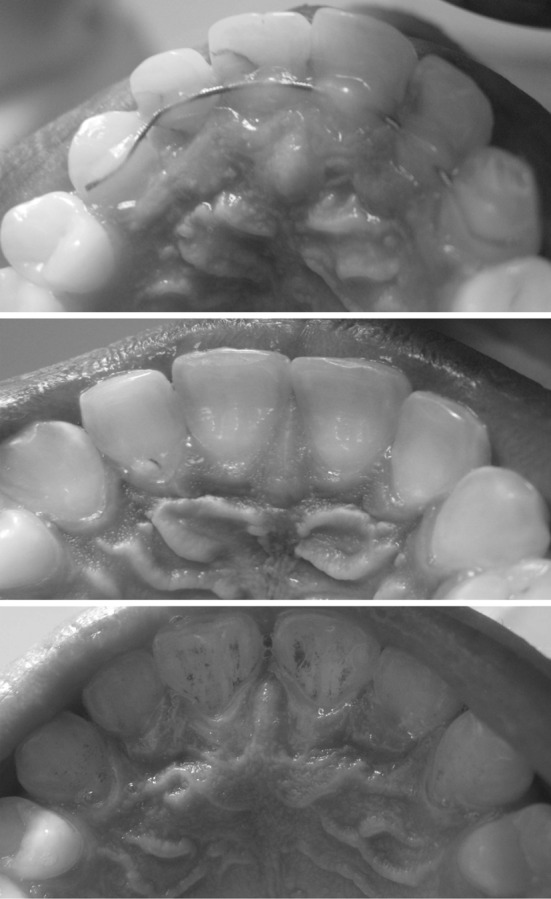
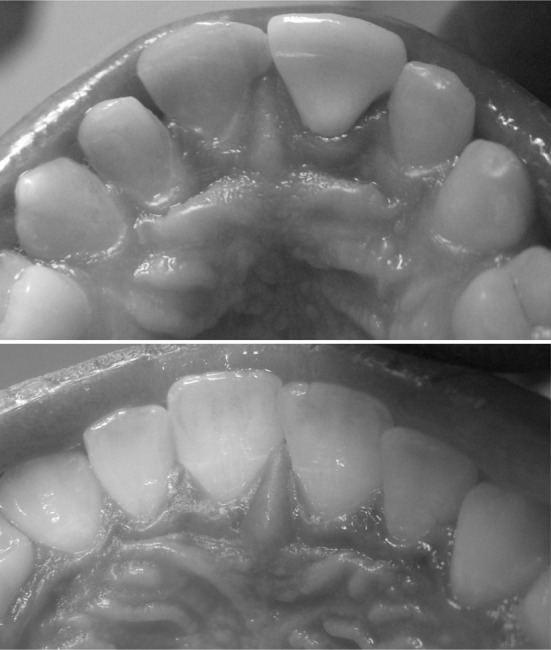
The relationship of the incisive papilla to the inter-canine line was observed in the photograph. When the position of incisive papilla coincided with the inter-canine line it was defined as Canine–Papilla–Canine (C–P–C line) (Fig. 10). When it was non coincident (Fig. 11), location of papilla and distance between the incisive papilla to inter-canine line was measured.
Fig. 10.
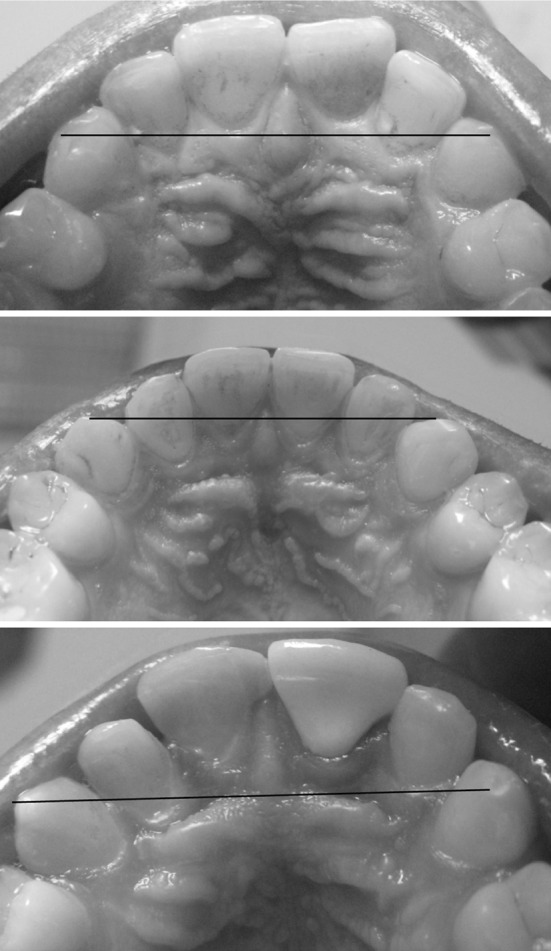
C–P–C line at the middle of papilla (above) at the anterior border (middle) and at its posterior border (bottom)
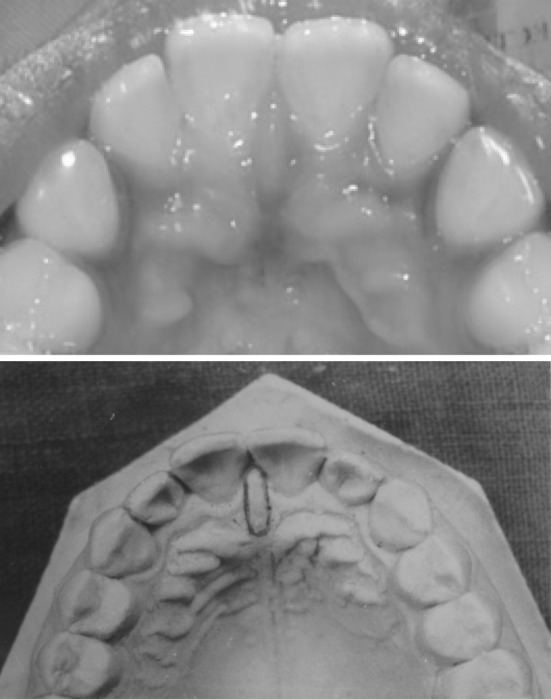
Fig. 11.
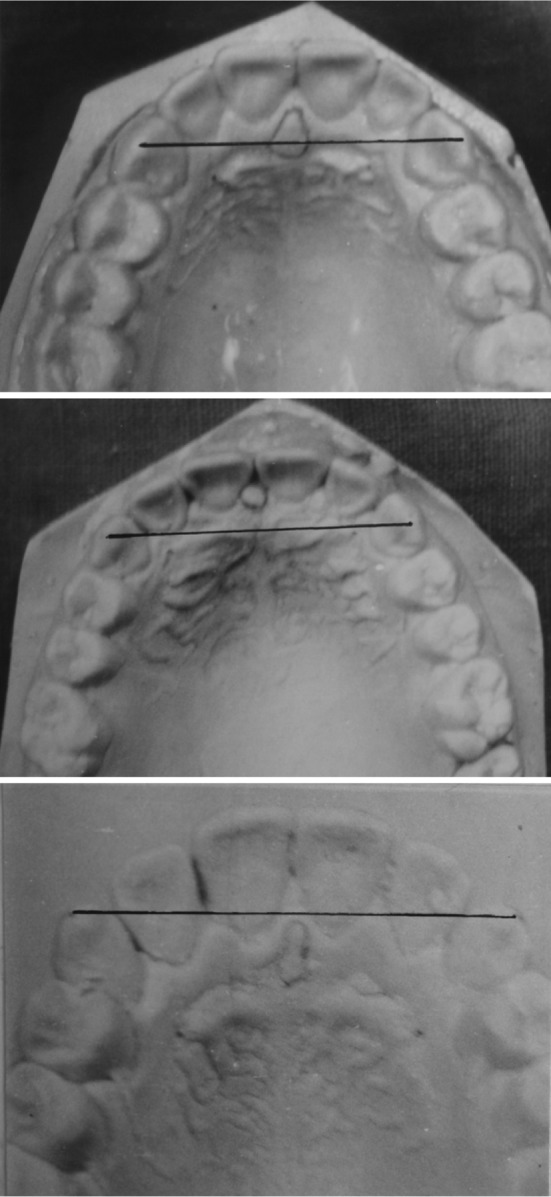
Papilla at the inter-canine line—C–P–C line (above), anterior to inter-canine line (middle), posterior to inter-canine line (bottom)
For the purpose of studying the form and shape of the incisive papilla, 500 dentate subjects of both sexes in the 20–30 age group who fulfilled the selection criteria were randomly selected. Intraoral photographs were taken for each of them to analyze the different shapes of incisive papilla.
Results
The results are shown in Tables 2–5. Papilla incisor distance and papilla canine relationship based on anthropometric measurements in dentulous samples of various races and ethnic groups are useful guides to set anterior teeth in complete dentures. In this study the distance between the incisive papilla and labial convexity of the central incisor was 11.9 mm, (mode 12.42 mm) Table 2. A difference of nearly 2 mm was seen in the western population where it ranged from 8 to 10 mm (Fig. 12). This is probably because of the prominent premaxillary arch seen in south Indian population as compared to Caucasians. The vertical distance between the incisive papilla and the incisal edge of maxillary central incisor was 7.8 mm (Fig. 13).
Table 2.
Distance between incisive papilla to the maxillary anterior teeth and occlusal plane in 125 males and 125 females in millimeters
| Landmark | Sex | Mean | Standard deviation | |
|---|---|---|---|---|
| IP to CI | Male | 12.02 | 11.92 | 2.01 |
| Female | 11.82 | |||
| IP to canine | Male | 18.60 | 18.34 | 1.93 |
| Female | 18.08 | |||
| IP to occlusal plane | Male | 7.81 | 7.79 | 1.62 |
| Female | 7.75 | |||
| Inter-canine distance | Male | 34.06 | 33.92 | 2.01 |
| Female | 33.78 | |||
Table 5.
Classification of incisive papilla according to its shape in 500 subjects
| Type | Shape | Sex | No. of samples | Percentage | Percentage in both sexes | |
|---|---|---|---|---|---|---|
| I | Pear | M | 36 | 14.4 | 23.6 | 33.2 |
| Large | ||||||
| F | 22 | 9.2 | ||||
| M | 9.6 | |||||
| Small | 15 | 6.0 | ||||
| F | 9 | 3.6 | ||||
| II | Spindle | M | 20 | 8.0 | 22.4 | |
| F | 36 | 14.4 | ||||
| III | Cylindrical | M | 32 | 12.8 | 21.6 | |
| F | 22 | 8.8 | ||||
| IV | Tapering/flame | M | 17 | 6.8 | 10.0 | |
| F | 8 | 3.2 | ||||
| V | Dumbbell | M | 7 | 2.8 | 9.2 | |
| F | 16 | 6.4 | ||||
| VI | Circular | M | 2 | 0.8 | 1.6 | |
| F | 2 | 0.8 | ||||
| VII | Inverted pear | M | 1 | 0.4 | 0.8 | |
| F | 1 | 0.4 | ||||
| VIII | Double papilla | M | – | – | 0.4 | |
| F | 1 | 0.4 | ||||
| IX | Rudimentary | M | – | – | 0.4 | |
| F | 1 | 0.4 | ||||
| X | Papilla absent | M | – | – | 0.4 | |
| F | 1 | 0.4 | ||||
Fig. 12.
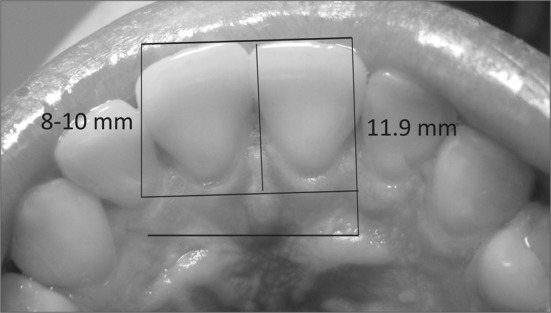
Mean incisive papilla central incisor distance in Caucasian (left) and Dravidian population (right)
Fig. 13.
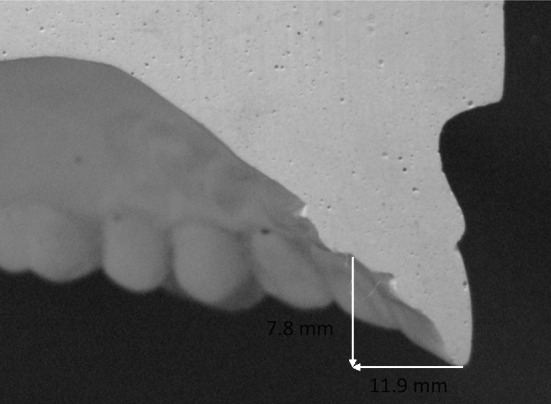
Mean horizontal and vertical papilla incisor distance
McGee [4], Hickey [6], Mavroskoufis [11], Watt and Macgregor [12] related the middle of the incisive papilla while Ortman and Tsao [10], Grave and Becker [14] used the base of incisive papilla as a reference for the measurement. Base of the incisive papilla was taken as a reference in this study since it was fairly constant to changes which occur from the dentulous to the edentulous state. It is stable after extraction of teeth. If any change occurred it was noticeable only in the anterior region.
One of the findings of this study was the location of the incisive papilla to the inter-canine line. In 93 % of the subjects the tip of the canines and incisive papilla were the same line known as C–P–C line. The inter-canine line passed through the middle of the papilla in 78 %, along the base in 14.1 % and in 0.4 % at its anterior border (Fig. 10). In 6.5 % it was anterior and posterior in 0.5 % within 1.5 mm distance to the inter-canine line (Fig. 11, Table 3).
Table 3.
Location of the incisive papilla to the inter-canine line in 250 subjects
| Location of incisive papilla | Course of C–P–C line | Percentage | |
|---|---|---|---|
| Incisive papilla and canine present in the same line C–P–C line |
Anterior border of incisive papilla | 0.4 | 93.1 |
| Body of IP | 78.6 | ||
| Base of IP | 14.1 | ||
| IP anterior to inter-canine line | – | 6.5 mm | |
| IP posterior to inter-canine | – | 0.5 mm | |
Schiffman [8] who first defined C–P–C line (canine–papilla line) found coincidence in 78.3 % of subjects, in 10.4 % it was anterior to the papilla while in 11.4 % it was posterior to the papilla. When non coincident, in 92.1 % it was located 1 mm anterior or posterior to the inter-canine line. Ehrlich and Gazit [9] found that in 57.6 % inter-canine lines passed through the center of the papilla. Sawiris [29] showed in 64 % of subjects the inter-canine line was situated 1 mm from the center of the papilla. Mavroskoufis and Ritchie [11] found the middle of the incisive papilla in Caucasians appeared to lie close to the inter-canine line. The discrepancy between the inter-canine line and the middle of the papilla in 93.4 % of the subjects was less than 2 mm. Lau and Clark [16] found that the incisive papilla was situated on the inter-canine line in 57.3 % of Chinese subjects. Grove and Christensen [15] stated that in 92 % of the 50 subjects the posterior point of the incisive papilla was approximately 3 mm anterior to a line between the distal points of the canines.
Marxkors in 1968 and later Solomon described a method of measuring papilla incisor distance by cutting a window on the palatal surface of the trial denture base to expose the papilla [28]. Incisive papilla is visualized through the window on the palatal surface of waxed trial denture (Fig. 6). The position of central incisor to incisive papilla can be measured. It is also possible to observe the C–P–C line and verify the position of upper canines to the papilla.
Laboratory and Clinical Application
In the laboratory technician should expose the papilla in the trial base and construct the labial surface of maxillary occlusal rim 8–10 mm anterior to incisive papilla rather than arbitrarily forming the labial contour. This considerably minimizes clinicians chair side time. Again during anterior set up, central incisors are positioned 8–10 mm forward to the incisive papilla (Fig. 6).
Ivoclar AG much later in the nineties advocated this method of opening a palatal window (Fig. 14) to locate the upper central incisor and canine teeth in BPS denture with the incisor papilla as a guideline. It recommends the upper central incisor kept 7 mm anterior to the midpoint of the papilla and the cervical margin of canine 2 mm lateral to main rugae. The labial surface of canine is placed 9 mm to the lateral end of main rugae [30].
Fig. 14.
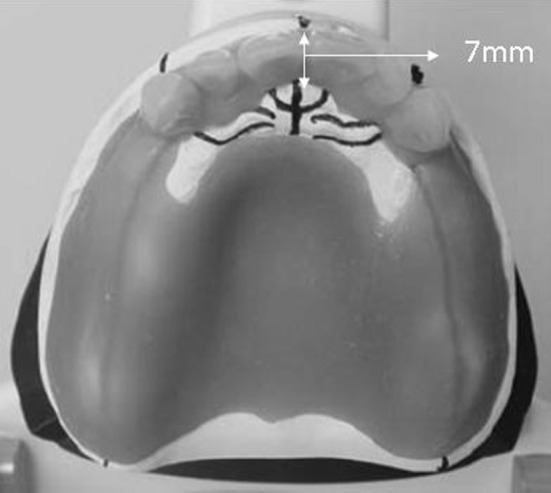
BPS method of setting anterior teeth
Shape of Incisive Papilla
The incisive papilla is generally referred as a round or oval elevation present anteriorly along the middle line on the palatal mucosa. This is not true in dentulous subjects, as the shape of incisive papilla varied from round to pear, spindle, flame, cylindrical, tapering and dumb bell forms (Figs. 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25). Ortman and Tsao [10] classified it as pear, oval, irregular, triangular, inverted pear and no papilla. Bamberadeniya [31] classified incisive papilla in Sri Lankan population as long, spindle, flame, pear oval and round. The shape of the dentulous incisive papilla is significant since it influences the center of the edentulous papilla from its earlier dentulous state.
Fig. 15.

Classical pear, long pear and inverted pear
Fig. 16.
Flame shaped pear
Fig. 17.
Cylindrical papilla
Fig. 18.
Dumbbell shaped papilla
Fig. 19.
Double papilla
Fig. 20.

Round papilla
Fig. 21.
Notched pear papilla
Fig. 22.
Football shaped papilla
Fig. 23.
Bowling pin shape papilla
Fig. 24.

Base of papilla not recognizable
Fig. 25.
Papilla absent
Classification of Incisive Papilla
Nine different types of incisive papilla were recognized and they are classified according to the order of their occurrence (Figs. 15–25).
Type I: Large pear
Type 2: Small pear
Type 3: Inverted pear
Type 4: Tapering/flame
Type 5: Cylindrical/spindle
Type 6: Round/oval/football
Type 7: Dumb-bell/bowling pin
Type 8: Double papilla
Type 9: Rudimentary and difficult to recognize.
Pear shaped papilla was most common, found in 33.2 % of the subjects investigated. Large pear papilla was seen in 23.6 % while small pear in 9.6 %. The other frequent types were spindle/flame in 22.4 %, cylindrical in 21.6 %, tapering in 10 % and dumb-bell seen in 9.2 % of the subjects. Certain rare forms like inverted pear and double papilla were also observed. However their incidence was low. In 0.8 % of the subjects incisive papilla was rudimentary, difficult to recognize or absent (Fig. 25). No significant sex differentiation was seen. Males predominantly showed pear, cylindrical and tapering forms, in females spindle and dumb-bell forms were common. The incisive papilla was discrete and isolated (Fig. 7) in 76 % of the subjects. In the remaining 24 % it was continuous with the interdental gingival papilla, located between the central incisors (Table 4).
Table 4.
Relationship between incisive papilla and interdental gingival papilla of maxillary central incisors in 250 subjects consisting of 125 males and 125 females
| Type of papilla | Sex | Samples | Percentage | Percentage in both sexes |
|---|---|---|---|---|
| Incisive papilla continuous with interdental papilla | M | 38 | 15.32 | 24.19 |
| F | 22 | 8.87 | ||
| Discrete incisive papilla | M | 87 | 35.08 | 75.81 |
| F | 101 | 40.73 |
When continuous, it was difficult to identify the anterior border of the papilla. This is significant since there are few studies where the anterior border of the incisive papilla has been used as a reference for measurements. In continuous papilla, post extraction changes in its anterior border and the subsequent change in its center will be more than in the discrete papilla. The center of the papilla in such is not a preferable landmark for biometric measurements. Very rarely it was not possible to identify the base of the papilla (Fig. 24).
Recommendation
Papilla incisor distance is a useful biometric guide to both the dentist and the dental technician. However it may not be applicable in every case; clinician should judiciously consider individual variations. Other biometric guides, phonetic tests and clinical judgement should be considered to decide the most appropriate position of central incisors in the horizontal plane. In the laboratory it is a distinct advantage for the technician to develop the labial contour of occlusal rim. Over contouring and under contouring the labial surface of occlusal rim by technician is minimized; simplifying the procedure of obtaining the labial contour of the occlusal rim in patients mouth, saving chair side time. It is also a valuable guide for the technician to set the incisor and canine teeth particularly when the labial contour of the maxillary occlusal rim is ignored by clinician or not correctly recorded by him.
Conclusion
Biometric analysis of incisive papilla in dentate subjects serves as a guide to develop facial contour in upper occlusal rim and anterior tooth position in complete dentures. Incisive papilla—central incisor distance was found to be 11.9 mm. The distance between incisive papilla and incisal plane was 7.8 mm. The labial surface of upper canine was 18.3 mm lateral to the incisive papilla. There was no significant difference in the age groups and between both the sexes.
The inter-canine distance between the tips of the cusps was in 33.9 mm. Incisive papilla was situated on the inter-canine line (C–P–C line) in 93 % of the subjects. In 7 % of the subjects incisive papilla was either anterior or posterior, within 1.5 mm distance to the inter-canine line.
Incisive papilla is classified according to its various forms as pear, inverted pear, tapering, flame, cylindrical, round, football, spindle, dumbbell and bowling pin shape. Pear shaped papilla was the most common while inverted pear and double papilla were less frequent. In a few the incisive papilla was absent or rudimentary and difficult to recognise.
Summary
The horizontal relationship of the incisive papilla to the maxillary permanent central incisor teeth was determined in 250 dentulous subjects consisting of 125 males and 125 females. The mean distance between the base of incisive papilla and labial surface of central incisor was 11.92 mm. In 93 % of the subjects the canines and incisive papilla were situated in a line (C–P–C line). In 7 % incisive papilla was within 1.5 mm anterior or posterior to the inter-canine line. There was no significant difference between males and females nor between the different age groups. The shape of incisive papilla was observed in photographs of 500 subjects. Based on this a classification of incisive papilla is suggested. The incisive papilla is an useful anatomical landmark to locate the position of central incisors and canines in upper complete dentures. A method to obtain the labial contour of maxillary occlusal rim and set the central incisors and canine teeth with incisive papilla as a reference in complete dentures is described.
References
- 1.Carlsson GE, Bergman B, Hedegard B. Changes in contour of the maxillary alveolar process under immediate dentures. A longitudinal clinical and X-ray cephalometric study covering 5 years. Acta Odontol Scand. 1967;25:45–75. doi: 10.3109/00016356709072522. [DOI] [PubMed] [Google Scholar]
- 2.Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed longitudinal study covering 25 years. J Prosthet Dent. 1972;27:120–132. doi: 10.1016/0022-3913(72)90188-6. [DOI] [PubMed] [Google Scholar]
- 3.Harper RN. The incisive papilla—basis of technic to reproduce the positions of key teeth in prosthodontia. J Dent Res. 1948;27:661–668. doi: 10.1177/00220345480270060301. [DOI] [Google Scholar]
- 4.McGee GF. Tooth placement and base contour in denture construction. J Prosthet Dent. 1960;10:651. doi: 10.1016/0022-3913(60)90245-6. [DOI] [Google Scholar]
- 5.Krajicek D. Simulation of natural appearance. J Prosthet Dent. 1962;12:30. doi: 10.1016/0022-3913(62)90004-5. [DOI] [Google Scholar]
- 6.Hickey JC, Boucher CO, Woelfel JB. Responsibility of the dentist in complete denture construction. J Prosthet Dent. 1962;12:637–653. doi: 10.1016/0022-3913(62)90092-6. [DOI] [Google Scholar]
- 7.Martone LC. Clinical application of concepts of functional anatomy and speech science to complete denture prosthodontics. J Prosthet Dent. 1963;13:204. doi: 10.1016/0022-3913(63)90165-3. [DOI] [Google Scholar]
- 8.Schiffman P. Relation of the maxillary canines to the incisive papilla. J Prosthet Dent. 1964;14:469–472. doi: 10.1016/S0022-3913(64)80013-5. [DOI] [Google Scholar]
- 9.Erlich J, Gazit E. Relationship of maxillary central incisors and canines to the incisive papilla. J Oral Rehabil. 1975;2:309–312. doi: 10.1111/j.1365-2842.1975.tb00923.x. [DOI] [PubMed] [Google Scholar]
- 10.Ortman HR, Tsao DH. Relationship of the incisive papilla to the maxillary central incisors. J Prosthet Dent. 1979;42:492–496. doi: 10.1016/0022-3913(79)90240-3. [DOI] [PubMed] [Google Scholar]
- 11.Marvroskoufis F, Ritchie GM. Nasal width and incisive papilla as guides for selection and arrangement of maxillary anterior teeth. J Prosthet Dent. 1981;45:592–597. doi: 10.1016/0022-3913(81)90417-0. [DOI] [PubMed] [Google Scholar]
- 12.Watt MD (1976) Designing complete dentures. W. B. Saunders, Philadelpia
- 13.Kharat DU, Madan RS. An investigation into the distances between incisive papilla and incisal edge of maxillary central incisors. J Indian Dent Assoc. 1984;56:426–428. [PubMed] [Google Scholar]
- 14.Grave AM, Becker PJ. Evaluation of incisive papilla as a guide to anterior tooth position. J Prosthet Dent. 1987;22:113–119. doi: 10.1016/0022-3913(87)90369-6. [DOI] [PubMed] [Google Scholar]
- 15.Grove HR, Christensen LV. Relationship of maxillary canines to the incisive papilla. J Prosthet Dent. 1989;42:492–496. doi: 10.1016/0022-3913(89)90108-x. [DOI] [PubMed] [Google Scholar]
- 16.Lau GC, Clark RF. The relationship of incisive papilla to the maxillary central incisors and canine teeth in southern Chinese. J Prosthet Dent. 1993;70:86–96. doi: 10.1016/0022-3913(93)90037-O. [DOI] [PubMed] [Google Scholar]
- 17.Abd Al-hadi L. Relationship between the incisal papilla and the anterior teeth in dentate patients. Chir Dent Fr. 1990;530:53–56. [PubMed] [Google Scholar]
- 18.Keng SB, Foong KV. Maxillary arch and central incisor dimensions on an ethnic Chinese population in relation to complete denture prosthesis. Int Dent J. 1996;46:103–107. [PubMed] [Google Scholar]
- 19.Bengakul C. Relation of maxillary canines to incisive papilla. J Dent Assoc Thail. 1983;33:178–179. [PubMed] [Google Scholar]
- 20.Young-Seok P, Seung PL, Ki-Suk P. The three dimensional relationship on a virtual model between the maxillary anterior teeth and incisive papilla. J Prosthet Dent. 2007;98:312–318. doi: 10.1016/S0022-3913(07)60104-8. [DOI] [PubMed] [Google Scholar]
- 21.Amin WM, Sandra K, Ghazawi A. The relationships of the maxillary central incisors and canines to the incisive papilla in Jordanians. J Contemp Dent Pract. 2008;9:1–18. [PubMed] [Google Scholar]
- 22.Fabiana MV, Sergio SN, Joao NA. The center of the incisive papilla for the selection of complete denture maxillary anterior teeth in 4 racial groups. Quintessence Int. 2008;39:841–845. [PubMed] [Google Scholar]
- 23.Siddharth S, Solomon EGR. Investigation of the vertical distance between the incisive papilla and incisal edge of maxillary central incisor in two ethnically diverse population. Dissertation. Chennai: Saveetha University; 2011. [Google Scholar]
- 24.Arunachalam KS, Solomon EGR. Relationship of the incisive papilla and the rugae to the maxillary permanent anterior teeth in Dravidian population. Dissertation. Chennai: University of Madras; 1982. [Google Scholar]
- 25.Lysel L, Brayton V. Plicae palatinae transversae and papilla incisiva in man: A morphologic and genetic study. Acta Odont Scandinav. 1955;13(18):135–137. [PubMed] [Google Scholar]
- 26.Salzmann JA. Review of Lysell, L.: plicae palatinae transversae and papillae incisiva in man. A morphologic and genetic study. Am J Orthodont. 1955;41:879–880. doi: 10.1016/0002-9416(55)90193-7. [DOI] [PubMed] [Google Scholar]
- 27.Watt DM, Likeman PR (1976) Morphological changes in the denture bearing area following the extraction of maxillary teeth. Br Dent J 136:225–235 [DOI] [PubMed]
- 28.Marxkors R. Zahnarzthliche tecknik. Dr.Alfred Huthig Verlag, Heidelberg. Denture. 1983;5:141–148. [Google Scholar]
- 29.Sawiris MM. The role of anthropometric measurements in the design of complete denture construction. J Dent. 1977;5:141–148. doi: 10.1016/0300-5712(77)90075-6. [DOI] [PubMed] [Google Scholar]
- 30.Hue O, Mariani P. The biofunctional prosthetic system—a new approach in removable denture prosthetics. Dent Spectr. 1999;4:5. [Google Scholar]
- 31.Bamberadeniya K. A study of the rugae pattern and the shape of the incisive papilla in Sri Lankan population. Ceyl Dent J. 1978;9:11–21. [Google Scholar]