

Abstract
Introduction:
Few studies have investigated the natural course of nicotine dependence prospectively from the earliest experiences with smoking.
Methods:
Drawing on a cohort of 9th- and 10th-grade adolescents followed over 48 months, survival analyses were conducted to evaluate the cumulative probability, following smoking initiation, for the development of nicotine dependence symptoms.
Results:
Although each nicotine dependence symptom was significantly more prevalent among adolescents who had smoked more than 100 cigarettes by the end of the follow-up assessment, 20% of adolescents smoking fewer than 100 cigarettes reported experiencing “smoking to relieve restlessness and irritability” and “smoking a lot more now to be satisfied compared to when first smoked.” Nicotine dependence symptoms were also reported before reaching 100 cigarettes for a substantial number of adolescents (between 9.4% and 58.8% for individual symptoms). Endorsement of nicotine dependence symptoms prospectively predicted past-week smoking (odds ratios [ORs] between 3.18 and 14.62 for significant symptoms) and past-month daily smoking (significant symptoms’ ORs between 3.52 and 10.68) at the 48-month assessment even when controlling for amount of previous smoking.
Conclusions:
The present study adds to the growing body of literature on the natural course of nicotine dependence from earliest experiences with smoking by showing that symptoms of nicotine dependence may develop soon after initiation and/or at low levels of smoking. Our findings suggest that novice adolescent smokers should not be neglected in smoking cessation intervention and that screening and effective intervention for early emerging symptoms among adolescent smokers may be an important target in preventing chronic smoking.
Introduction
Over the past several decades, public health interventions have been successful in reducing smoking in the United States by influencing both higher rates of quitting and decreased uptake. This has largely been achieved through approaches that have increased knowledge of deleterious effects of smoking and exposure to second hand smoke and influenced major antismoking legislation that has increased prices, reduced access, and limited smoking in both public and private areas (Biener & Siegel, 1997; Centers for Disease Control and Prevention [CDC], 2010a, 2011; Chaloupka, 1999; DiFranza & Dussault, 2005; Fichtenberg & Glantz, 2002; Garrett, Dube, Trosclair, Caraballo, & Pechacek, 2011; Levy, Nikolayev, & Mumford, 2005; Wakefield et al., 2000). Despite the success of these initiatives, national monitoring surveys have shown that decreases in smoking prevalence have slowed in recent years (Nelson et al., 2008). It is estimated that 21% of adults in the United States currently smoke and that of current smokers, 78% smoke daily (CDC, 2010b).
As the primary contributor to the establishment and maintenance of chronic smoking (Berrettini & Lerman, 2005; Hu, Davies, & Kandel, 2006), nicotine dependence has been characterized by both physiological adaptations (e.g., tolerance and withdrawal) and other accommodating behaviors (e.g., time spent in activities necessary to obtain/use nicotine and recover from its effects and the forfeiting or reduction of important social, occupational, or recreational activities). Although traditional descriptions of the development of nicotine dependence have suggested the need for both heavy and long-term smoking, an emerging body of research based on separate cohorts of novice adolescent smokers has demonstrated that symptoms of nicotine dependence can occur soon after smoking initiation (DiFranza, Savageau, Rigotti, et al., 2002; Gervais, O’Loughlin, Meshefedjian, Bancej, & Tremblay, 2006; Kandel, Hu, Griesler, & Schaffran, 2007), at relatively low levels of smoking exposure (Caraballo, Novak, & Asman, 2009; Gervais et al., 2006; Scragg, Wellman, Laugesen, & DiFranza, 2008) and before the establishment of daily smoking habits (DiFranza et al., 2007; Gervais et al., 2006). For example, in a cohort of seventh graders sampled from Montreal secondary schools, 30% and 20% developed mental and physical symptoms of dependence, respectively, within 3 months of reporting their first puff (Gervais et al., 2006). Similarly, based on a cohort of 6th to 10th graders drawn from Chicago public schools, 25% of new adolescent smokers were found to experience symptoms of dependence within 5 months of smoking onset (Kandel et al., 2007). Furthermore, in the Montreal study, it took much less time to develop symptoms of nicotine dependence (e.g., mental addiction, physical addition, cravings, withdrawal symptoms, and tolerance) compared with reaching lifetime consumption of 100 cigarettes and daily smoking (Gervais et al., 2006), indicating that symptoms of nicotine dependence in adolescents can occur before the emergence of established smoking patterns.
Importantly, nicotine dependence symptoms that emerge soon after smoking initiation and/or at low levels of smoking exposure have been shown to represent substantial risk for the development of established and chronic smoking behaviors (Dierker & Mermelstein, 2010; DiFranza, Savageau, Fletcher, et al., 2002). In a cohort of seventh graders drawn from seven public schools in two small cities in Massachusetts, for example, the odds of developing daily smoking was substantially elevated among adolescents reporting one or more dependence symptoms 30 months earlier compared with adolescents who had initiated smoking but reported no nicotine dependence symptoms (DiFranza, Savageau, Fletcher, et al., 2002). More recently, based on a sample of adolescent smokers drawn from Chicago-area schools, LCD and RJM demonstrated that nicotine dependence symptoms reported by 9th- and 10th-grade adolescents who had smoked fewer than 100 cigarettes in their lifetime predicted the development of daily smoking 2 years later, even after controlling for number of cigarettes smoked and use of other tobacco products (Dierker & Mermelstein, 2010).
Although a large number of studies on nicotine dependence have been conducted in adolescents, only a few have examined the development of dependence symptoms from the earliest experiences with smoking (DiFranza, Savageau, Rigotti, et al., 2002; Doubeni, Reed, & Difranza, 2010; Gervais et al., 2006; Kandel et al., 2007). Moreover, the natural course of nicotine dependence that simultaneously includes a consideration of amount of smoking as well as time between smoking initiation and the onset of symptoms has not yet been investigated. The primary objectives of this study are to (a) describe the timing of onset of nicotine dependence symptoms for those who reached 100 cigarettes smoked and those smoking fewer than 100 cigarettes, (b) prospectively examine rates of adolescent smokers who develop nicotine dependence symptoms before reaching established smoking patterns, and (c) determine whether early emerging nicotine dependence symptoms predict smoking behaviors at the 48-month follow-up.
Methods
Participants
As described elsewhere (Dierker & Mermelstein, 2010), the Social and Emotional Contexts of Adolescent Smoking Patterns Study (SECASPS) follows a cohort recruited from 16 Chicago-area high schools. All 9th- and 10th-grade students in these schools completed a brief screening survey of smoking behavior (N = 12,970). In line with the SECASPS’ aim to prospectively study the development of regular smoking behavior, adolescents at the earliest stages of smoking behavior were primarily selected, as well as adolescents who were light regular smokers and samples of nonsmokers who might initiate smoking in the future, according to the following criteria. Students who reported smoking fewer than 100 cigarettes in their lifetime, a common criteria for lifetime nonsmoking status (CDC, 2002) and smoking in the past 90 days, were invited to participate as were all those who smoked in the past 30 days and had smoked more than 100 cigarettes in their lifetime. Additionally, random samples of youth reporting having never smoked or smoking fewer than 100 cigarettes lifetime, but prior to the past 90 days, were also invited to participate. Of the 3,654 students invited, 1,344 agreed to participate (37%). The sample of those who agreed to participate remained ethnically and racially diverse and approximately representative of the greater Chicago metropolitan area in accordance with the goal of sampling. Of these, 1,263 (94%) completed the baseline assessment. Follow-up assessment was conducted at 6, 15, 24, 33, and 48 months with 95% (n = 1,199) of the sample participating in two or more surveys and 86% (n = 1,092) participating in the 48-month follow-up.
The present analyses were based on 114 participants of this sample who initiated smoking within the year prior to the baseline survey and an additional 55 participants who initiated smoking between baseline and 48 months (total n = 169). The mean age of this sample at baseline was 15.5 years (SD = 0.7), and the average age of smoking onset for the 169 participants was 15.4 years (SD = 1.2, ranging from 13.0 to 18.6). Approximately half (54%) of this sample were female, and the majority (81%) were Caucasian.
Measures
Smoking
For participants who had initiated smoking prior to the baseline assessment, age of smoking initiation was measured with the question, “How old were you the very first time you smoked even a puff of a cigarette?” For those who initiated during the follow-up period, initiation age was recorded as the current age when any smoking was first reported. At each assessment, lifetime smoking was measured with the question “About how many cigarettes have you smoked in your entire life.” Daily smoking was measured at each assessment with the questions “Have you ever smoked cigarettes on a daily basis? (At least 30 days when you smoked every day or nearly every day)” and the question, “How many days did you smoke or try cigarettes in the past 30 days.”
Nicotine Dependence
Individual dependence symptoms were assessed among adolescents who reported ever smoking at least one puff and were measured at each assessment with a shortened version of Nicotine Dependence Syndrome Scale (NDSS; Shiffman, Waters, & Hickcox, 2004), modified for use with adolescents (Clark et al., 2005; Sledjeski et al., 2007; Sterling et al., 2009). Items were answered on a four-point Likert-type scale, ranging from 0 (not at all true) to 3 (very true). A nicotine dependence total score was obtained by averaging responses to all items. The presence or absence of each symptom was established by collapsing response options of “not very true” to “very true” into a single category to generate a dichotomous variable for symptom endorsement (No—not at all true vs. Yes—any of the three positive responses).
Statistical Analysis
At each assessment, reports of dependence symptoms were coded in terms of time (i.e., number of months) since smoking initiation. We first described the development of nicotine dependence in terms of the cumulative probability of the occurrence of each individual symptom according to time in months following smoking initiation using Kaplan–Meier survival analysis, an optimal method for modeling time-to-event data in the presence of censored cases. We then repeated these analyses, using the Log-rank test and stratifying by those who had or had not smoked 100 cigarettes by the end of the follow-up assessment.
Finally, logistic regression models were used to examine whether nicotine dependence (both the NDSS total score and endorsement of individual symptoms) predicted daily smoking at the 48-month follow-up, controlling for previous highest level of smoking frequency (days smoked in past 30 days drawn from each assessment), highest smoking quantity (number of cigarettes smoked in past week at each assessment), gender, ethnicity (White vs. non-White), and age of smoking initiation. Participants with missing data were excluded from the logistic regression analysis. The missing data were primarily caused by the attrition of participants during the 4-year follow-up period. In the present study, smoking behavior at the 4-year follow-up could not be determined for 17 of 169 participants.
Results
Figure 1 illustrates the cumulative probability of each nicotine dependence symptom according to time since smoking initiation. Escalation of the cumulative probability was particularly rapid for reports of “increase in the amount smoked,” “smoking to relieve restlessness and irritability,” and “smoking a lot more now to be satisfied compared to when first smoked,” with substantially slower increases in the cumulative probability of “better functioning in the morning after having a cigarette,” “buying cigarettes instead of lunch,” and “willingness to go outside in a rainstorm to get cigarettes.” Overall, the cumulative increases of individual nicotine dependence symptoms were fairly stable across time.
Figure 1.

Cumulative probability of developing dependence symptoms following smoking initiation. Satisfaction = smoking a lot more now to be satisfied compared with when first smoked; Increase = increase in the amount smoked; Relieve = smoking to relieve restlessness and irritability; Discomfort = smoking to keep from experiencing discomfort; Functioning = better functioning in the morning after having a cigarette; Craving = craving without smoking for a few hours; Uncontrollable = feeling like in the grip of uncontrollable unknown force; Rainstorm = willingness to go outside in a rainstorm to get cigarettes; Smoke outside = willingness to go outside to smoke even in severe weather; and Lunch = buying cigarettes instead of lunch when low on money.
Figure 2 illustrates the number of months after smoking initiation when the cumulative probability of developing each symptom was 25%. The 95% CIs are based on Kaplan–Meier survival analyses. The symptom “increase in the amount smoked” was reported by 25% of smokers within 1 year of initiation, whereas “smoking a lot more now to be satisfied compared to when first smoked” and “smoking to relieve restlessness and irritability” were reported by 25% of smokers within 2 years of initiation. Compared with other individual symptoms, the symptom of “better functioning in the morning after having a cigarette” developed more slowly, taking 4 years to reach a cumulative probability of 25%.
Figure 2.

Number of months after initiation of cigarette smoking at which the cumulative probability of developing dependence symptoms is 25%. Error bars represent 95% CI based on Kaplan–Meier survival analyses. Satisfaction = smoking a lot more now to be satisfied compared with when first smoked; Increase = increase in the amount smoked; Relieve = smoking to relieve restlessness and irritability; Discomfort = smoking to keep from experiencing discomfort; Functioning = better functioning in the morning after having a cigarette; Craving = craving without smoking for a few hours; Uncontrollable = feeling like in the grip of uncontrollable unknown force; Rainstorm = willingness to go outside in a rainstorm to get cigarettes; Smoke outside = willingness to go outside to smoke even in severe weather; and Lunch = buying cigarettes instead of lunch when low on money.
The potential contributions of smoking to the natural course of nicotine dependence symptoms were examined next using the log-rank test to evaluate differences in the Kaplan–Meier survival curve estimates between those smoking more or less than 100 cigarettes. These analyses showed that each symptom was significantly more prevalent among adolescents who had smoked more than 100 cigarettes by the end of the follow-up assessment, compared with those smoking fewer than 100 cigarettes. Among adolescents who had smoked more than 100 cigarettes, the vast majority of individual symptoms had a cumulative probability more than 75% by the end of the follow-up period. Symptoms such as “smoking a lot more now to be satisfied compared to when first smoked,” “increase in the amount smoked,” and “smoking to relieve restlessness and irritability” reached a cumulative probability of 75% within 3 years of smoking initiation, whereas it took symptoms of “smoking to keep from experiencing discomfort,” “willingness to go outside to smoke even in severe weather,” “craving without smoking for a few hours,” and “willingness to go outside in a rainstorm to get cigarettes” 48–54 months to reach a cumulative probability of 75%.
Figures 3–5 illustrate the cumulative probability of the three most commonly reported nicotine dependence symptoms. Although these symptoms are reported by nearly all of the 100+ smokers, notably, more than 40% of adolescents smoking less than 100 cigarettes reported having “increase in the amount smoked,” and approximately 20% of those who smoked less than 100 cigarettes reported “smoking to relieve restlessness and irritability” and “smoking a lot more now to be satisfied compared to when first smoked.”
Figure 3.
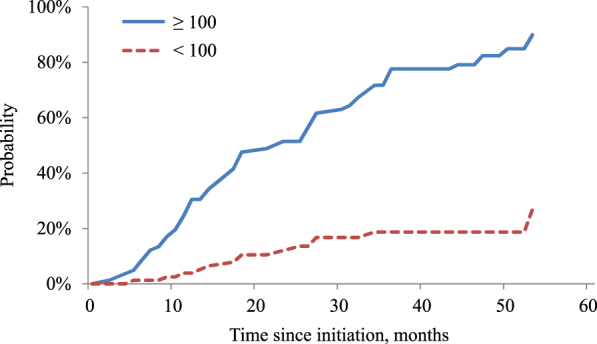
Cumulative probability of developing dependence symptom “smoking a lot more now to be satisfied compared to when first smoked” stratified by lifetime cigarette consumption. ≥100, total = 82, failed = 66, censored = 16. <100, total = 80, failed = 14, censored = 66. p < .0001.
Figure 4.
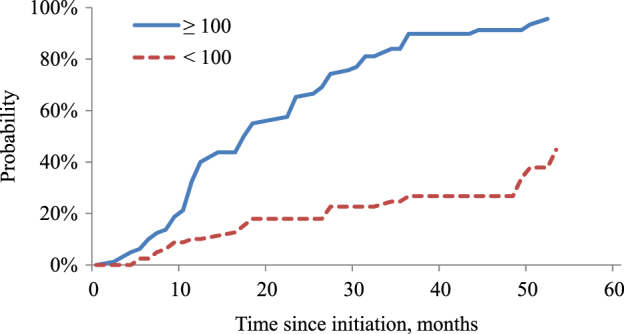
Cumulative probability of developing dependence symptom of “increase in the amount smoked” stratified by lifetime cigarette consumption. ≥100, total = 80, failed = 73, censored = 7; <100, total = 81, failed = 23, censored = 58. p < .0001.
Figure 5.
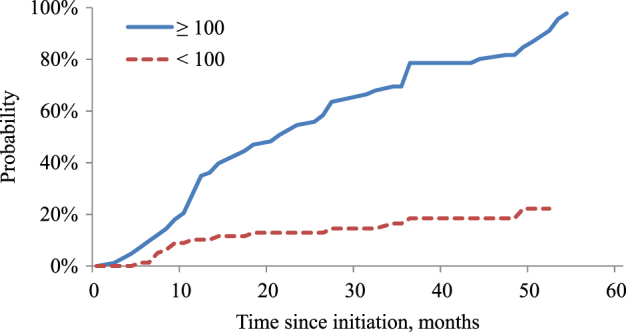
Cumulative probability of developing dependence symptom of “smoking to relieve restlessness and irritability” stratified by lifetime cigarette consumption. ≥100, total = 83, failed = 72, censored = 11; <100, total = 80, failed = 15, censored = 65. p < .0001.
A more detailed examination of order of onset of smoking milestones (i.e., 100 cigarettes and daily smoking) and nicotine dependence symptoms revealed that “increase in the amount smoked,” “smoking to relieve restlessness and irritability,” “smoking a lot more now to be satisfied compared to when first smoked,” and “willingness to go outside to smoke even in severe weather” occurred before daily smoking for more than one third of adolescents who had reached daily smoking levels (Table 1). The onset of several symptoms was similarly common before reaching 100 cigarettes smoked (i.e., “increase in the amount smoked,” “smoking to relieve restlessness and irritability,” “smoking a lot more now to be satisfied compared to when first smoked,” “willingness to go outside to smoke even in severe weather,” and “smoking to keep from experiencing discomfort”).
Table 1.
Proportion of Participants Who Reported Experiencing Individual Dependence Symptoms Before, During the Same Wave, and After Reaching the Smoking Milestones of 100 Cigarettes and Daily Smoking
| Symptoms | Smoked 100 or more (n = 85) | Daily smoking (n = 78) | ||||
| Before (%) | Same wave (%) | After (%) | Before (%) | Same wave (%) | After (%) | |
| Smoking a lot more now to be satisfied compared with when first smoked | 45.9 | 30.6 | 4.7 | 37.6 | 30.6 | 7.1 |
| Increase in the amount smoked | 58.8 | 31.8 | 1.2 | 55.3 | 21.2 | 4.7 |
| Smoking to relieve restlessness and irritability | 47.1 | 35.3 | 4.7 | 44.7 | 25.9 | 7.1 |
| Smoking to keep from experiencing discomfort | 35.3 | 32.9 | 4.7 | 30.6 | 27.1 | 8.2 |
| Better functioning in the morning after having a cigarette | 9.4 | 29.4 | 15.3 | 5.9 | 27.1 | 16.5 |
| Craving without smoking for a few hours | 31.8 | 25.9 | 11.8 | 24.7 | 31.8 | 9.4 |
| Feeling like in the grip of uncontrollable unknown force | 23.5 | 27.1 | 9.4 | 22.4 | 24.7 | 10.6 |
| Willingness to go outside in a rainstorm to get cigarettes | 18.8 | 32.9 | 10.6 | 17.6 | 25.9 | 15.3 |
| Willingness to go outside to smoke even in severe weather | 38.8 | 34.1 | 4.7 | 35.3 | 28.2 | 7.1 |
| Buying cigarettes instead of lunch when low on money | 17.6 | 30.6 | 11.8 | 10.6 | 31.8 | 11.8 |
Finally, to establish the predictive validity of these symptoms, we examined whether the development of individual nicotine dependence symptoms was associated with smoking behavior at the 48-month assessment. The majority of nicotine dependence symptoms as well as the overall NDSS score were found to be strongly predictive of both daily and past week smoking, after controlling for previous smoking, gender, ethnicity, and age of smoking initiation (Table 2). For example, adolescent smokers who reported “increase in the amount smoked” were five times more likely to smoke daily (odds ratios [OR] = 5.61, 95% CI 1.44–21.91) at the 48-month assessment than those not reporting this symptom. Similarly, adolescent smokers who reported “feeling like in the grip of uncontrollable unknown force” were three times more likely to smoke in the past week (OR = 3.24, 95% CI 1.17–8.95) at the 48-month assessment that those not reporting this symptom.
Table 2.
Odds Ratio (95% CI) for the Occurrence of Nicotine Dependence Symptoms and Smoking Behaviors at the 48-Month Follow-up (n = 169)a
| Symptoms | Smoked in the past week | Smoked daily in the past month |
| Smoking a lot more now to be satisfied compared with when first smoked | 2.35 (0.89–6.19) | 2.38 (0.80–7.06) |
| Increase in the amount smoked | 4.53 (1.45–14.17) | 5.61 (1.44–21.91) |
| Smoking to relieve restlessness and irritability | 2.49 (0.93–6.65) | 4.63 (1.49–14.40) |
| Smoking to keep from experiencing discomfort | 3.18 (1.18–8.54) | 4.90 (1.65–14.52) |
| Better functioning in the morning after having a cigarette | 7.26 (1.52–34.67) | 4.78 (1.35–16.95) |
| Craving without smoking for a few hours | 2.55 (0.94–6.88) | 7.78 (2.39–25.32) |
| Feeling like in the grip of uncontrollable unknown force | 3.24 (1.17–8.95) | 4.72 (1.56–14.33) |
| Willingness to go outside in a rainstorm to get cigarettes | 3.86 (1.34–11.13) | 3.52 (1.13–10.98) |
| Willingness to go outside to smoke even in severe weather | 3.72 (1.39–9.94) | 10.68 (3.14–36.32) |
| Buying cigarettes instead of lunch when low on money | 3.59 (1.27–10.13) | 4.95 (1.53–15.94) |
| Maximum NDSS scale from baseline to 24 monthsb | 14.62 (5.31–40.27) | 7.25 (1.86–28.26) |
Notes. NDSS = Nicotine Dependence Syndrome Scale.
Adjusting for the occurrence of corresponding outcome before 48-month follow-up, sex, ethnicity, and age of smoking initiation.
Dichotomized at 0.2 because of severe skewness.
Discussion
The SECASPS recruited novice adolescent smokers and those who had never smoked and followed the cohort for 4 years, providing a opportunity to examine the development of nicotine dependence from the earliest experiences with smoking. The present findings replicate previous work documenting the early emerging symptoms (Rose, Dierker, & Donny, 2010) and confirm that the development of these symptoms in many cases occurs before the onset of more established smoking patterns (Gervais et al., 2006; O’Loughlin, Gervais, Dugas, & Meshefedjian, 2009). The present study also extends previous research by describing the natural course of nicotine dependence symptoms in terms of the timing of their development both before and after the establishment of two smoking milestones (i.e., 100 cigarettes and daily smoking).
Notably, the symptoms found to emerge following earliest exposures in the present study are highly consistent with those found within a large, nationally representative sample of novice adolescent and young adult smokers (Rose et al., 2010). Rose et al. found that several symptoms were endorsed by those smoking as little as 1–3 days per month, and typically only 1 cigarette/day, with the most prevalent symptoms being “irritability after not smoking for a while,” “increase in the amount smoked,” and “needing to smoke more to feel satisfied” (Rose et al., 2010). These are also among the symptoms that have been found to have a high probability of endorsement at even low levels of nicotine dependence severity (Rose & Dierker, 2010). Further, the emergence of symptoms meant to measure behavioral manifestations of tolerance (i.e., “increase in the amount smoked” and “smoking a lot more now to be satisfied compared to when first smoked”) suggests that tolerance may be among the earliest indicators of nicotine dependence and thus important for preventative recognition of the dependence process.
The early development of tolerance symptoms in novice adolescent smokers may at least partially relate to the shortening of latencies between smoking one’s most recent cigarette and the onset of withdrawal symptoms, a process that has been well-characterized in dependent smokers (DiFranza et al., 2011). Specifically, the shortening of the latency-to-withdrawal that accompanies each additional cigarette may explain the need for increased amounts of smoking, in that youth find themselves having to smoke more in order to relieve or prevent withdrawal symptoms (DiFranza et al., 2011). Confirming this literature on latency-to-withdrawal, the current findings also demonstrate that nicotine dependence symptoms, and tolerance in particular, can occur in novice smokers and at less-than-daily patterns of smoking.
Although previous studies have demonstrated that the development of symptoms of nicotine dependence in many cases occurs before the onset of more established smoking patterns (Gervais et al., 2006; O’Loughlin et al., 2009), none have previously described the natural course of nicotine dependence specifically among adolescent smokers who had not yet consumed 100 cigarettes. We found, for example, that 20% of adolescents smoking fewer than 100 cigarettes reported “smoking to relieve restlessness and irritability” and “smoking a lot more now to be satisfied.” Although this study closely resembles a previous report by Gervais et al. (2006) with respect to both study design and the objective to describe the natural course of nicotine dependence in novice adolescent smokers, there are also notable differences. Gervais used different criteria for assessing nicotine dependence (six symptoms based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, and International Classification of Diseases, 10th Revision, rather than the adolescent version of the NDSS). Additionally, the analysis performed by Gervais et al. pooled more established adolescent smokers (smoked 100 cigarettes) with more novice smokers who had not yet smoked 100 cigarettes and did not stratify by this criterion. Thus, the current findings may be more generalizable to novice adolescent smokers. These differences in measurement and smoking populations may explain the difference between the results of the current study and those of Gervais’ study regarding the relative order of tolerance development compared with other dependence symptoms. Most notably, the current study extends beyond examining the natural course of nicotine dependence symptoms in evaluating the predictive validity of each of these symptoms for future smoking behavior.
The plausibility of the presence of symptoms at these very low levels of smoking exposure has been previously discussed by DiFranza et al. (DiFranza et al., 2000; DiFranza, Savageau, Rigotti, et al., 2002). Briefly, although changes in the brain have not yet been directly linked to behavioral experiences of addiction following the earliest experimentation with smoking, the fact that the number of nicotinic receptors in the brain increases as early as the second dose of nicotine (Changeux, 2010) suggests that experience of nicotine symptoms for many may indeed be fast.
The present study further demonstrated that nicotine dependence among novice adolescent smokers is strongly predictive of future smoking in that the vast majority of symptoms predicted both daily and nondaily smoking at the 48-month assessment, even when controlling for amount of previous smoking. Taken with previous work that has confirmed the predictive validity of early emerging symptoms in the development of chronic smoking behaviors (Dierker & Mermelstein, 2010; DiFranza, Savageau, Fletcher, et al., 2002), these results provide strong evidence for the importance of the early recognition of nicotine dependence symptoms as a potential target for intervention among novice smokers. To date, the focus of intervention has largely been to prevent or delay first puff and then to intervene again by supporting cessation but primarily among chronic smokers or special populations such as pregnant women (Ranney et al., 2006).
The major strengths of the present study include a prospective design that follows an adolescent cohort of new smokers over a 4-year period and measurement of nicotine dependence from the earliest experiences with smoking. Despite these important strengths, a few study limitations should also be noted. First, the direct comparison across studies of the number of months required for the emergence of individual nicotine dependence symptoms requires a consideration of differences in measurement. Craving, for example, was reported among 25% of smokers from the Montreal study within 5 months of smoking initiation (Gervais et al., 2006), whereas in the present study 25% of smokers achieved craving within 27 months of initiation. In the Montreal study, craving was defined as ever having cravings to smoke cigarettes, whereas in the present study, the NDSS item restricted craving to those experiences occurring when not smoking for a few hours, a difference that may at least partially account for timing.
Second, the generalization of the results may be limited in some ways. Because examination of the natural course of dependence symptoms was conducted among those who initiated smoking between age 13 and 18 (mean age = 15.4), any generalization of the results is limited to smokers who initiate during this period of adolescence. Earlier or later onset may also show somewhat different timing in terms of the emergence of dependence symptoms. Particularly, because the sample initiated smoking at a later age than when most initiation occurs, the results should not be generalized to adolescents who initiated smoking at a younger age. Additionally, the relatively low proportion of adolescents who agreed to participate in the study among all adolescents who were invited is another factor that may limit the generalization of these results. However, the racial and ethnic diversity in the final sample is similar to another comparable study (DiFranza et al., 2000), and these findings may nevertheless be robust across different populations.
Third, considering that a relatively large proportion of novice adolescent smokers developed symptoms of nicotine dependence during the same assessment period as the occurrence of the two milestones (i.e., 100 cigarettes and daily smoking), future studies with a shorter observation interval are needed to better characterize timing between smoking milestones and development of nicotine dependence symptoms. Conversely, studies spanning a longer time frame, as well as forthcoming assessment waves of the current SECASPS, are likely to capture a greater proportion of adolescents who progress to these milestones.
Finally, the measurement of number of months for the development of nicotine dependence symptoms is less precise for participants who initiated smoking within the year prior to the baseline assessment than for those initiating during the follow-up. Notably, however, when comparing these two groups, the differences in the cumulative probability of developing each symptom within 3 years after smoking initiation were not significant suggesting that combining these two groups does not bias the results. The only exception was for reports of “smoking to keep from experiencing discomfort” in which the cumulative probability was significantly greater for those initiating smoking within the year prior to baseline (43.6%) compared with those initiating during the follow-up period (22.9%), p = .01.
In summary, the present study adds to the growing body of literature on the natural course of nicotine dependence by replicating previous research that has suggested that nicotine dependence symptoms can develop soon after smoking initiation at low level of exposure and before the occurrence of established smoking patterns. Moreover, our findings confirm previous studies that have evaluated the relationship between emerging symptoms and later smoking behavior (Dierker & Mermelstein, 2010; DiFranza, Savageau, Fletcher, et al., 2002; DiFranza et al., 2007), showing a strong and independent relationship between these early reported symptoms and risk for future smoking, over and above the level of tobacco use. Taken together, these findings suggest that novice adolescent smokers should not be neglected in smoking cessation intervention, and screening and effective intervention for early emerging symptoms among adolescent smokers may prevent the development of chronic smoking.
Funding
This research was supported by Project Grant P01 CA098262 (R.J.M.) from the National Cancer Institute, grants DA022313, DA022313 -S (L.C.D.), and DA029834 (J.S.R.) from the National Institute on Drug Abuse, and a Center Grant (DA010075) awarded to the Methodology Center, Penn State University.
Declaration of Interests
The authors report no conflict of interest.
References
- Berrettini WH, Lerman CE. Pharmacotherapy and pharmacogenetics of nicotine dependence. American Journal of Psychiatry. 2005;162:1441–1451. doi: 10.1176/appi.ajp.162.8.1441. doi:10.1176/appi.ajp.162.8.1441. [DOI] [PubMed] [Google Scholar]
- Biener L, Siegel M. Behavior intentions of the public after bans on smoking in restaurants and bars. American Journal of Public Health. 1997;87:2042–2044. doi: 10.2105/ajph.87.12.2042. doi:10.2105/AJPH.87.12.2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caraballo RS, Novak SP, Asman K. Linking quantity and frequency profiles of cigarette smoking to the presence of nicotine dependence symptoms among adolescent smokers: Findings from the 2004 National Youth Tobacco Survey. Nicotine & Tobacco Research. 2009;11:49–57. doi: 10.1093/ntr/ntn008. doi:10.1093/ntr/ntn008. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Cigarette smoking among adults—United States, 2000. Morbidity & Mortality Weekly Report. 2002;51:642–645. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5129a3.htm. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Smoking restrictions in large-hub airports—United States, 2002 and 2010. Morbidity & Mortality Weekly Report. 2010a;59:1484–1487. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a3.htm. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Vital signs: Current cigarette smoking among adults aged ≥18 years—United States, 2009. Morbidity & Mortality Weekly Report. 2010b;59:1135–1140. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5935a3.htm. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Ten great public health achievements—United States, 2001–2010. Morbidity & Mortality Weekly Report. 2011;60:619–623. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6019a5.htm. [PubMed] [Google Scholar]
- Chaloupka FJ. Macro-social influences: The effects of prices and tobacco-control policies on the demand for tobacco products. Nicotine & Tobacco Research. 1999;1(Suppl. 2):S77–S81. doi: 10.1080/14622299050011681. doi:10.1080/14622299050011861. [DOI] [PubMed] [Google Scholar]
- Changeux JP. Nicotine addiction and nicotinic receptors: Lessons from genetically modified mice. Nature reviews. Neuroscience. 2010;11:389–401. doi: 10.1038/nrn2849. doi:10.1038/nrn2849. [DOI] [PubMed] [Google Scholar]
- Clark DB, Wood DS, Martin CS, Cornelius JR, Lynch KG, Shiffman S. Multidimensional assessment of nicotine dependence in adolescents. Drug and Alcohol Dependence. 2005;77:235–242. doi: 10.1016/j.drugalcdep.2004.08.019. doi:10.1016/j.drugalcdep.2004.08.019. [DOI] [PubMed] [Google Scholar]
- Dierker L, Mermelstein R. Early emerging nicotine-dependence symptoms: A signal of propensity for chronic smoking behavior in adolescents. Journal of Pediatrics. 2010;156:818–822. doi: 10.1016/j.jpeds.2009.11.044. doi:10.1016/j.jpeds.2009.11.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Dussault GF. The federal initiative to halt the sale of tobacco to children—The Synar Amendment, 1992–2000: Lessons learned. Tobacco Control. 2005;14:93–98. doi: 10.1136/tc.2004.009373. doi:10.1136/tc.2004.009373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Rigotti NA, McNeill AD, Ockene JK, Savageau JA, St Cyr D, et al. Initial symptoms of nicotine dependence in adolescents. Tobacco control. 2000;9:313–319. doi: 10.1136/tc.9.3.313. doi:10.1136/tc.9.3.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Fletcher K, Ockene JK, Rigotti NA, McNeill AD, et al. Measuring the loss of autonomy over nicotine use in adolescents: The DANDY (Development and Assessment of Nicotine Dependence in Youths) study. Archives of Pediatrics and Adolescent Medicine. 2002;156:397–403. doi: 10.1001/archpedi.156.4.397. doi:10.1136/tc.11.3.228. [DOI] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Fletcher K, O’Loughlin J, Pbert L, Ockene JK, et al. Symptoms of tobacco dependence after brief intermittent use: The Development and Assessment of Nicotine Dependence in Youth-2 study. Archives of Pediatrics and Adolescent Medicine. 2007;161:704–710. doi: 10.1001/archpedi.161.7.704. doi:10.1001/archpedi.161.7.704. [DOI] [PubMed] [Google Scholar]
- DiFranza JR, Savageau JA, Rigotti NA, Fletcher K, Ockene JK, McNeill AD, et al. Development of symptoms of tobacco dependence in youths: 30 Month follow up data from the DANDY study. Tobacco Control. 2002;11:228–235. doi: 10.1136/tc.11.3.228. doi:10.1136/tc.11.3.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFranza JR, Wellman RJ, Mermelstein R, Pbert L, Klein JD, Sargent JD, et al. The natural history and diagnosis of nicotine addiction. Current Reviews in Pediatrics. 2011;7:88–96. doi:10.2174/157339611795735648. [Google Scholar]
- Doubeni CA, Reed G, Difranza JR. Early course of nicotine dependence in adolescent smokers. Pediatrics. 2010;125:1127–1133. doi: 10.1542/peds.2009-0238. doi:10.1542/peds.2009-0238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fichtenberg CM, Glantz SA. Effect of smoke-free workplaces on smoking behaviour: Systematic review. British Medical Journal. 2002;325:188. doi: 10.1136/bmj.325.7357.188. doi:10.1136/bmj.325.7357.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garrett BE, Dube SR, Trosclair A, Caraballo RS, Pechacek TF. Cigarette smoking—United States, 1965–2008. Surveillance Summaries: Morbidity & Mortality Weekly Report. 2011;60(Suppl):109–113. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/su6001a24.htm. [PubMed] [Google Scholar]
- Gervais A, O’Loughlin J, Meshefedjian G, Bancej C, Tremblay M. Milestones in the natural course of onset of cigarette use among adolescents. Canadian Medical Association Journal. 2006;175:255–261. doi: 10.1503/cmaj.051235. doi:10.1503/cmaj.051235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu MC, Davies M, Kandel DB. Epidemiology and correlates of daily smoking and nicotine dependence among young adults in the United States. American Journal of Public Health. 2006;96:299–308. doi: 10.2105/AJPH.2004.057232. doi:10.2105/AJPH.2004.057232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kandel DB, Hu MC, Griesler PC, Schaffran C. On the development of nicotine dependence in adolescence. Drug and Alcohol Dependence. 2007;91:26–39. doi: 10.1016/j.drugalcdep.2007.04.011. doi:10.1016/j.drugalcdep.2007.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levy DT, Nikolayev L, Mumford E. Recent trends in smoking and the role of public policies: Results from the SimSmoke tobacco control policy simulation model. Addiction. 2005;100:1526–1536. doi: 10.1111/j.1360-0443.2005.01205.x. doi:10.1111/j.1360-0443.2005.01205.x. [DOI] [PubMed] [Google Scholar]
- Nelson DE, Mowery P, Asman K, Pederson LL, O’Malley PM, Malarcher A, et al. Long-term trends in adolescent and young adult smoking in the United States: Metapatterns and implications. American Journal of Public Health. 2008;98:905–915. doi: 10.2105/AJPH.2007.115931. doi:10.2105/AJPH.2007.115931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Loughlin J, Gervais A, Dugas E, Meshefedjian G. Milestones in the process of cessation among novice adolescent smokers. American Journal of Public Health. 2009;99:499–504. doi: 10.2105/AJPH.2007.128629. doi:10.2105/AJPH.2007.128629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ranney L, Melvin C, Lux L, McClain E, Morgan L, Lohr KN. Tobacco use: Prevention, cessation, and control. Evidence Report/Technology Assessment. 2006;140:1–120. Retrieved from http://www.ahrq.gov/downloads/pub/evidence/pdf/tobaccouse/tobuse.pdf. [PMC free article] [PubMed] [Google Scholar]
- Rose JS, Dierker LC. An item response theory analysis of nicotine dependence symptoms in recent onset adolescent smokers. Drug and Alcohol Dependence. 2010;110:70–79. doi: 10.1016/j.drugalcdep.2010.02.006. doi:10.1016/j.drugalcdep.2010.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rose JS, Dierker LC, Donny E. Nicotine dependence symptoms among recent onset adolescent smokers. Drug and Alcohol Dependence. 2010;106:126–132. doi: 10.1016/j.drugalcdep.2009.08.012. doi:10.1016/j.drugalcdep.2009.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scragg R, Wellman RJ, Laugesen M, DiFranza JR. Diminished autonomy over tobacco can appear with the first cigarettes. Addictive Behaviors. 2008;33:689–698. doi: 10.1016/j.addbeh.2007.12.002. doi:10.1016/j.addbeh.2007.12.002. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Waters A, Hickcox M. The Nicotine Dependence Syndrome Scale: A multidimensional measure of nicotine dependence. Nicotine & Tobacco Research. 2004;6:327–348. doi: 10.1080/1462220042000202481. doi:10.1080/1462220042000202481. [DOI] [PubMed] [Google Scholar]
- Sledjeski E, Dierker L, Costello D, Shiffman S, Donny E, Flay B. Predictive validity of four nicotine dependence measures in a college sample. Drug and Alcohol Dependence. 2007;87:10–19. doi: 10.1016/j.drugalcdep.2006.07.005. doi:10.1016/j.drugalcdep.2006.07.005. [DOI] [PubMed] [Google Scholar]
- Sterling KL, Mermelstein R, Turner L, Diviak K, Flay B, Shiffman S. Examining the psychometric properties and predictive validity of a youth-specific version of the Nicotine Dependence Syndrome Scale (NDSS) among teens with varying levels of smoking. Addictive Behaviors. 2009;34:616–619. doi: 10.1016/j.addbeh.2009.03.016. doi:10.1016/j.addbeh.2009.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wakefield MA, Chaloupka FJ, Kaufman NJ, Orleans CT, Barker DC, Ruel EE. Effect of restrictions on smoking at home, at school, and in public places on teenage smoking: Cross sectional study. British Medical Journal. 2000;321:333–337. doi: 10.1136/bmj.321.7257.333. doi:10.1136/bmj.321.7257.333. [DOI] [PMC free article] [PubMed] [Google Scholar]