

Abstract
Adenopathy and extensive skin patch overlying a plasmacytoma is a very rare syndrome featuring a red-to-brown, violaceous skin patch along with a plasmacytoma. Only 11 case reports exist in the literature. Skin biopsies from the cutaneous patch overlying the plasmacytoma exhibit a dermal vascular hyperplasia with increased surrounding dermal mucin. Radiation therapy is used to treat and cure the plasmacytoma.
Adenopathy and extensive skin patch overlying a plasmacytoma (AESOP) syndrome is a very rare constellation of findings seen in patients with a yet-to-be diagnosed solitary plasmacytoma.1,2 There are only 11 cases reported in the literature; the first report dates back to Sheinker in 1938 (Tables 1).3
TABLE 1.
Summary of patients with AESOP syndrome ranked by ascending age
| PATIENT/REFERENCE | AGE/SEX | LYMPH-ADENOPATHY | NEUROPATHY | PLASMA-CYTOMA SITE | OTHER DISEASES | MONOCLONAL IMMUNO-GLOBULIN (IG) | TREATMENT | OUTCOME AFTER TREATMENT |
|---|---|---|---|---|---|---|---|---|
| 11,2 | 18/Male | + | - | 1st, 2nd, 3rd ribs | None | IgG | Radiation | Cured |
| 21 | 34/Male | + | + | 5th rib | None | None | Radiation | Favorable |
| 31,2 | 39/Male | + | + | Sternum | None | Unknown | None | Died 15 months later |
| 41,2 | 42/Male | + | + | Sternum | POEMS, Castleman’s disease | IgA λ | Chemo | Unkown |
| 51,2 | 43/Male | + | + | Skull | Castleman’s disease | IgG λ | Surgery and radiation | Cured |
| 61,2,4 | 54/Male | + | + | Scapula | Osteolysis | None | Radiation | No follow up |
| 71,2,5 | 58/Male | + | + | Clavicle | None | None | Radiation | Favorable |
| 82 | 64/Female | - | - | 6th rib | None | IgG λ | Not known | No follow up |
| 91 | 66/Male | + | + | 6th rib | POEMS | IgG λ | Surgery | Died 4.5 years later |
| 101 | 68/Female | + | + | Sternum | POEMS | IgG λ | Surgery and radiation | Favorable |
| 111 | 73/Male | + | - | Sternum | None | None | Radiation | Favorable |
CLINICAL FEATURES
The 11 patients with AESOP syndrome described in the literature comprise nine men and two women (age range=18–73 years). All presented with a slow-growing red, brown, or violaceous skin patch with irregular, possibly elevated, borders and featuring clearly visible blood vessels on the thoracic cavity (Figure 1). In two instances, the lesion appeared atrophic and had a fine desquamation at the edges. The temperature of the skin patch was either normal or warm. The duration of the rash at diagnosis spanned from three months to more than one year, with a size at presentation ranging from 8 to 18cm. Additionally, some patients had smaller satellite lesions near the main one. The patch has been reported to expand at a rate of 5 to 10cm per year.2 Most of the patients presented with polyneuropathies, which caused facial and lingual parasthesias, dysesthesia, and hypotonia of the limbs, areflexia, ascending paralysis of upper and lower limbs, hypertrophy, and dyspnea. The majority of patients had unilateral or bilateral lymphadenopathy in the axillary, supraclavicular, cervical, and/or mediastinal areas that became evident after the appearance of the cutaneous patch.1,4,5 The palpable lymph nodes were mobile and firm, ranging in size from 1 to 3cm. Three patients also had concurrent polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes (POEMS) syndrome, another cluster of findings known to be associated with a plasmacytoma.1,6Notably, POEMS syndrome developed as late as 18 years after the resection of the plasmacytoma.7 One of these patients died and another developed hepatosplenomegaly, diabetes mellitus, and elevated antithyroglobulin antibodies.7
Figure 1.
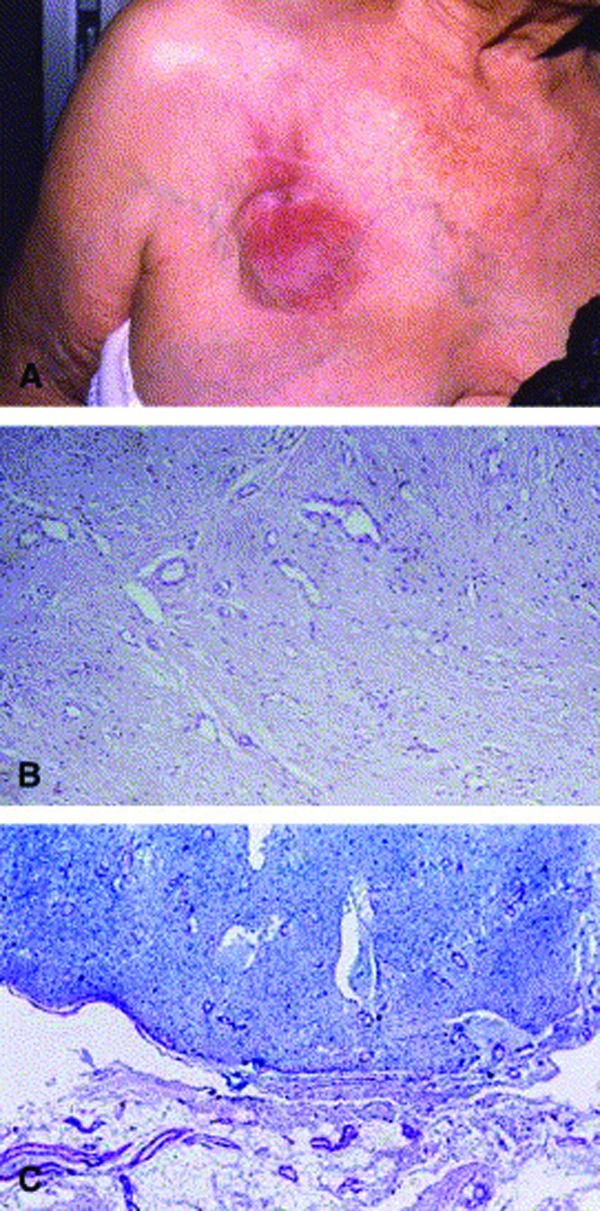
(A) Erythema-tous, slowly enlarging, ill-defined plaque on chest. Note prominent vessels on chest wall. (B) Histo-pathology showing diffuse reactive vascular hyperplasia (angiomatosis) in edematous, mucinous stroma. Note some prominent endothelial cells lining vessel walls. (Hematoxilin-eosin stain; original magnification x200.) (C) Abundant mucin deposition in dermal stroma associated with vascular hyperplasia and sparing subcutis. (Alcian blue, pH 2.5; original magnification x100.)
Reproduced with permission from the Journal of the American Academy of Dermatology.2
IMAGING AND LABORATORY CHARACTERISTICS
In all cases, imaging studies revealed a solitary osteolytic or osteodense mass in the bone underneath the cutaneous lesion except for one case, in which the mass was present, but distant from the skin lesion. In a few patients, the bone mass was palpable underneath the cutaneous lesion. In most instances, it was located on a rib or the sternum; in other cases, it was located on the skull, scapula, or clavicle. The histological analysis of these excised bone masses was consistent with a plasmacytoma by immunohistochemical demonstration of either the monotypic kappa (κ) or lambda (λ) immunoglobulin light chains.1,2
Skin biopsies taken from the cutaneous patch overlying the plasmacytoma revealed a benign-appearing dermal vascular hyperplasia with increased surrounding dermal mucin.1,6 Some cases also featured a perivascular inflammatory dermal infiltrate mainly consisting of lymphocytes, neutrophils, and macrophages (Figure 1).1 Immunohistochemical staining, carried out in some instances, did demonstrate λ chain deposition, mainly around the dermal blood vessels.2 One case showed increased fibrosis in the deep dermis and hypodermis. The epidermis was mostly spared; only one case featured mild epidermal spongiosis and exocytosis.1
Histopathological examination of the excised lymph nodes revealed either nonspecific findings (such as hyperplasia of native lymphocytes and sinusoidal lymphoplasmacytosis) or, in two of the patients, histological findings consistent with Castleman’s disease, a condition known to be associated with POEMS syndrome.6 The classic histological findings of Castleman’s disease consist of follicular lymphoid hyperplasia, possibly exhibiting germinal centers, along with significant proliferation of the capillaries and hyperplasia of the endothelial cells.8,9
Other laboratory findings worth mentioning include a monoclonal spike in serum electrophoresis, Bence Jones proteinuria, and hypercellularity and hyperproteinemia of the cerebrospinal fluid. However, none of the patients met the criteria for a diagnosis of multiple myeloma. When performed, laboratory testing for Borrelia burgdorferi proved unrevealing.1,2 Electromyographic studies confirmed the presence of axono-myelinic motor and sensory neuropathy.1,4,5,7
MANAGEMENT
It is now well established that radiation therapy can be curative for patients with plasmacytomas.10 Most of the patients who received radiation or a combination of surgery and radiation had favorable outcomes. Two of the patients died from complications secondary to POEMS syndrome. One patient who developed POEMS syndrome was treated with radiation therapy and experienced resolution of all signs and symptoms after four months.1
DISCUSSION
As outlined above, AESOP syndrome is a rare condition that presents with a unique dermatological finding—a relatively large, intensely red or erythrocyanotic patch on the skin, usually on the thoracic region, accompanied by a solitary plasmacytoma and its associated symptoms. The histopathological findings of dermal vascular hyperplasia without endothelial atypia and increased dermal mucin are not specific; the term “mucinous angiomatosis” has been suggested to describe these aggregate findings.2 It is worth noticing, however, that other diseases feature increased dermal mucin in the context of increased immunoglobulin deposition (i.e., scleromyxedema and persistent papular mucinosis).1
The skin lesions of AESOP syndrome are thought to arise from a process known as contiguous inflammation of the skin (CIS). In CIS, a localized and irregularly shaped erythema develops over another process, such as an infection or neoplasm, localized in a deeper anatomic structure.1,2,11 In the case of AESOP syndrome, the plasmacytoma may secrete angiogenic growth-promoting factors, such as vascular endothelial growth factor (VEGF), which would in turn induce vascular proliferation in the overlying dermis.1,2 Accordingly, an anti-VEGF monoclonal antibody (bevacizumab) has been recently proposed as a therapeutic option.12
Plasma cell dyscrasias, such as multiple myeloma, are commonly known to cause neuropathic symptoms. These symptoms generally precede the diagnosis of the tumor by a median of 1.5 years.7 The neuropathy associated with plasma cell dyscrasias is usually secondary to compression of a nerve or its vascular supply by the tumor mass. Despite these findings, neuropathy is still a rare symptom in solitary plasmacytoma.5 Kuwabara12 recently suggested that VEGF might play a role in altering the blood brain barrier, thereby allowing neurotoxic substances to adversely affect the nervous tissues, and ultimately resulting in demyelination. In addition to the previously mentioned mechanisms, microvascular proliferation may also contribute to the neuropathy in some yet undiscovered way.12
Footnotes
DISCLOSURE:The authors report no relevant conflicts of interest.
REFERENCES
- 1.Lipsker D, Rondeau M, Massard G, Grosshans E. The AESOP (adenopathy and extensive skin patch overlying a plasmacytoma) syndrome: report of 4 cases of a new syndrome revealing POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes) syndrome at a curable stage. Medicine (Baltimore) 2003;82:51–59. doi: 10.1097/00005792-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Rongioletti F, Romanelli P, Rebora A. Cutaneous mucinous angiomatosis as a presenting sign of bone plasmacytoma: a new case of (A)ESOP syndrome. J Am Acad Dermatol. 2006;55:909–910. doi: 10.1016/j.jaad.2006.04.072. [DOI] [PubMed] [Google Scholar]
- 3.Sheinker I. Myelom und nervensystem. Dtsch Z Nervenheik. 1938;147:247–273. [Google Scholar]
- 4.Crow RS. Peripheral neuritis in myelomatosis. Br Med J. 1956;2:802–804. doi: 10.1136/bmj.2.4996.802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Read D, Warlow C. Peripheral neuropathy and solitary plasmacytoma. J Neurol Neurosurg Psychiatry. 1978;41:177–184. doi: 10.1136/jnnp.41.2.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Leite AC, Nascimento OJ, Lima MA, Andrada-Serpa MJ. POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein, skin lesions) syndrome: a South America’s report. Arq Neuropsiquiatr. 2007;65:516–520. doi: 10.1590/s0004-282x2007000300030. [DOI] [PubMed] [Google Scholar]
- 7.Sakemi H, Okada H. An autopsy case of Crow-Fukase syndrome which developed 18 years after the first manifestation of plasmacytoma. Intern Med. 1992;31:50–54. doi: 10.2169/internalmedicine.31.50. [DOI] [PubMed] [Google Scholar]
- 8.Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956;9:822–830. doi: 10.1002/1097-0142(195607/08)9:4<822::aid-cncr2820090430>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 9.Barrie JR, English JC, Muller N. Castleman’s disease of the lung: radiographic, high-resolution CT and pathologic findings. AJR Am J Roentgenol. 1996;166:1055–1056. doi: 10.2214/ajr.166.5.8615241. [DOI] [PubMed] [Google Scholar]
- 10.Bataille R, Sany J. Solitary myeloma: clinical and prognostic features of a review of 114 cases. Cancer. 1981;48:845–851. doi: 10.1002/1097-0142(19810801)48:3<845::aid-cncr2820480330>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 11.Helmbold P, Kaufhold A, Hegemann B, Marsch WC. Contiguous inflammation of the skin. Eur J Dermatol. 1999;9:48–50. [PubMed] [Google Scholar]
- 12.Kuwabara S. [Crow-Fukase (POEMS) syndrome] Brain Nerve. 2010;62:395–400. [PubMed] [Google Scholar]