

Abstract
Background:
The availability of oral health services are very scarce in rural India; therefore the unmet treatment needs of rural population are very high. Hence, a retrospective study was conducted to evaluate the types of patients, disease pattern, and services rendered in outreach programs in rural areas of Haryana.
Materials and Methods:
A The data were obtained from records of outreach programs conducted, in last 3 months, by Swami Devi Dyal Hospital and Dental College. The data from were analyzed using descriptive statistics.
Results:
A total of 1371 individuals in the age group of 4--70 years (56.8% males and 43.2% females) attended the outreach program seeking the treatment. Dental caries (43.7%), gingivitis (27.2%), and periodontitis (22.9%) were commonly observed dental diseases. The services provided were oral prophylaxis (51.2%), restoration (22.9%), referral (20%), and extractions (8.8%).
Conclusion:
The attendance and utilization of dental services in the out reach programs seem to be influenced by sociodemographic characteristics of the population.
Keywords: Disease pattern, out reach program, utilization
Introduction
Over the years significant improvement in health has been witnessed. However, this improvement has been experienced unequally across the population, being higher among better off. India is a developing country with second highest population in the world. A mismatch exists between oral health professionals and the population they serve. About 80% of dentists work in major cities in India, compared to the population where more than 70% of the Indians reside in the rural areas. The dentist to population ratio is 1:10,000 in urban areas whereas 1:150,000 in rural areas. Even with a workforce of 118,000 qualified dentists in the country, the most basic oral health education and simple interventions are also not available to vast majority of population.[1]
Oral health is not only important for appearance and sense of well-being but also for overall health. Dental caries and periodontal diseases may contribute to many serious conditions, such as diabetes and respiratory diseases. Poor oral health can affect the quality of life, appearance, and self-esteem, and has been linked to sleeping problems, as well as behavioral and developmental.[2] It has been proven that early diagnosis and appropriate treatment can prevent worsening of the oral diseases.[3] Thus, maintaining good oral health includes both prevention of oral disease occurrence as well as treatment of any existing condition.
According to WHO, the provision of oral health care services is very little in rural parts of India, further complexity is lent by the great variation that occurs across this population on social parameters such as income and education.[4] Few of the studies conducted on the rural population of India have concluded that the unmet treatment need of the population is very high and the services present are inadequate in most parts of the country.[5–7]
Equity in access to health care is one of the objectives of health care system. Mooney[8] argues that access is merely a question of supply, while utilization depends on both supply and demand. Individual utilization of health care is possibly affected by many factors that are not connected to health care per se but shape individuals’ demand for health care. Hence the present study was conducted to evaluate the types of patients, disease pattern, and services provided in outreach programs.
Materials and Methods
The retrospective study was conducted using the data collected from the various outreach programs conducted by Swami Devi Dyal Hospital and Dental College in last 3 months (October, November and December, 2011). These outreach programs were carried out in the rural area of the Panchkula district, Haryana. The data from all the patients attending the program were included in the study. The data included the information about the diagnosis as well as the treatment of the patients. The data were analyzed using SPSS version 18. The descriptive statistics as used to describe the type of patients, pattern of oral diseases, and services provided in the outreach programs.
Results
A total of 1371 subjects in the age group of 4-70 years were included in the study. Table 1 shows the frequency distribution of study subjects attending the outreach programs according to their socio-demographic characteristics. The maximum number of patients (35.7%) belonged to the age group of 36- -55 years and least number of patients (15.4%) attending out reach program were in the age group of >55 years. The female attendance (56.8%) was more than male attendance (43.2%). A total of 42.1% were illiterate and only 8.3% were graduate and above. A total of 61.2% of the total subjects were unskilled laborers, that is most of them being farmers, students, and housewives and only 2.1% belonged to managerial class.
Table 1.
Distribution of study subjects according to sociodemographic characteristics
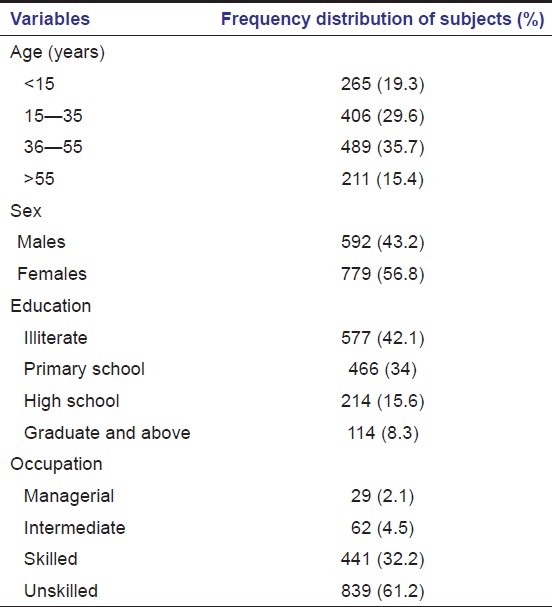
Table 2 shows the disease pattern of the study subjects attending the out reach programs. The prevalence of dental caries was found to be 43.7% and for gingivitis and periodontitis it was 27.2% and 22.9% respectively. The other conditions included partial or complete edentulousness, fractured teeth, malocclusion, dental fluorosis, and soft tissue lesions which were found to be 6.2%.
Table 2.
Distribution of study subjects according to the disease pattern
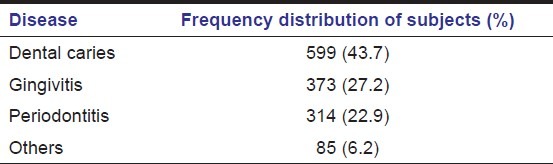
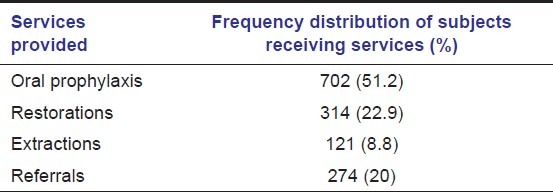
Table 3 shows the various services provided to the study subjects according to the diagnosis. These included oral prophylaxis (51.2%), restorations (22.9%), and extractions (8.8%). Out of total, 20% were referred to the college for complex treatment and rehabilitation.
Table 3.
Distribution of study subjects according to services provided at the outreach programs
Discussion
The enjoyment of highest attainable level of health is a fundamental right of every human being without discrimination based on race, religion, socioeconomic condition. There are several challenges faced in the delivery of oral health care services to the rural population such as deficiency of manpower, poor accessibility, affordability, and availability. The utilization of health care services depends upon health attitudes, social structure, and social demographic factors along with affordability and accessibility and the need for use of services. In many developing countries like India, it is often difficult for the rural population to get access to oral health services. So the present study was conducted to study the type of patient, disease pattern, and services that can be provided at free dental outreach programs.
It was found that most of the patients attending the dental out reach programs were in the age group 15-55 years (65.3%), hence less utilization by the children and older individuals, >55 years of age, which was in agreement with other studies.[9,10] It may reflect the attitude of the older individuals toward their oral health and of the parents toward the oral health of their children. Meng et al,[11] found that dental fear and fear of dental pain have independent negative effects on dental utilization which could be the factor associated with utilization in the present study.
The utilization of dental services was found to be higher in females compared to males which is in accordance with findings of other studies.[10–13] It may be due to the fact that females have a greater tendency to expect good outcome from dental attendance and also because most of the females were housewives they could attend the outreach programs, while men were bread earners hence were not available at their homes.
A total of 56.1% patients attending the outreach program were either illiterate or had low level of education which might be because of the location of the outreach program being rural areas.
The disease pattern showed dental caries to have highest prevalence followed by gingivitis. These findings were in accordance to National oral health survey conducted in 2002–2003.[6] The most common services provided in the outreach programs were oral prophylaxis, restoration, and extractions.
Hence in order to improve the dental attendance, the barriers have to be identified and controlled by appropriate education and intervention. The results indicate that there is a need to motivate people giving them information but paying attention to the individual reasons which restrict their behavior.
The limitation of the present study was localization of the study; therefore, to determine the relative effects of the barriers, further investigation should be conducted. In order to gain a better understanding of how people use dental services and why, other structural and oral health variables need to be studied.
Conclusion
The utilization of dental services in the outreach programs has been found to be influenced by sociodemographic characteristics of the population. The services provided in the outreach programs should be based on the felt needs of the population so that both attendance and the utilization of dental services can be increased thereby improving the oral health status of the population.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Tandon S. Challenges to the oral health workforce in India. J Dent Educ. 2004;68:28–33. [PubMed] [Google Scholar]
- 2.Diwan S, Saxena V, Bansal S, Kandpal SD, Gupta N. Oral Health: Knowledge and Practices in Rural Community. Indian J Comm. Health. 2011;22:29–33. [Google Scholar]
- 3.Lo EC, Lin HC, Wang ZJ, Wong MC, Schwarz E. Utilisation of dental services in Southern China. J Dent Res. 2001;80:1471–4. doi: 10.1177/00220345010800051701. [DOI] [PubMed] [Google Scholar]
- 4.Reisine S. A path analysis of the utilization of dental services. Community Dent Oral Epidemiol. 1987;15:119–24. doi: 10.1111/j.1600-0528.1987.tb00497.x. [DOI] [PubMed] [Google Scholar]
- 5.Agarwal V, Khatri M, Singh G, Gupta G, Marya CM, Kumar V. Prevalence of periodontal diseases in India. J Oral Health Comm Dent. 2010;4:7–16. [Google Scholar]
- 6.New Delhi, India: Dental Council of India; 2004. National oral health Survey and Fluoride mapping 2002-2003. [Google Scholar]
- 7.Bhat M. Oral health status and treatment needs of a rural Indian fishing community. West Indian Med J. 2008;57:414–7. [PubMed] [Google Scholar]
- 8.Mooney GH. Equity in health care: Confronting the confusion. Eff Health Care. 1983;1:179–85. [PubMed] [Google Scholar]
- 9.Syrjala AM, Knuuttila ML, Syrjala LK. Reasons preventing regular dental care. Community Dent Oral Epidemiol. 1992;20:10–4. doi: 10.1111/j.1600-0528.1992.tb00665.x. [DOI] [PubMed] [Google Scholar]
- 10.Manski RJ, Magder LS. Demographic and Socioeconomic predictors of dental care utilization. J Am Dent Assoc. 1998;129:195–200. doi: 10.14219/jada.archive.1998.0177. [DOI] [PubMed] [Google Scholar]
- 11.Meng X, Heft MW, Bradley MM, Lang PJ. Effect of fear on dental utilization behaviors and oral health outcome. Community Dent Oral Epidemiol. 2007;35:292–301. doi: 10.1111/j.1600-0528.2007.00315.x. [DOI] [PubMed] [Google Scholar]
- 12.Slack-Smith LM, Mills CR, Bulsara MK, O’Grady MJ. Demographic health and lifestyle factors associated with dental service attendance by young adults. Aust Dent J. 2007;52:205–9. doi: 10.1111/j.1834-7819.2007.tb00490.x. [DOI] [PubMed] [Google Scholar]
- 13.Pizarro V, Ferrer M, Domingo-Salvany A, Benach J, Borrell C, Pont A, et al. The utilization of dental care services according to health insurance coverage in Catalonia (Spain) Community Dent Oral Epidemiol. 2009;37:78–84. doi: 10.1111/j.1600-0528.2008.00439.x. [DOI] [PubMed] [Google Scholar]