

Abstract
Introduction:
Successful root canal treatment depends primarily on the removal of micro-organisms through chemo-mechanical instrumentation of the root canal system. This encompasses shaping by mechanical removal of the dentine and cleaning by chemical disinfection of microorganisms and dissolution of organic tissues from the root canal. While root canal shaping can be predictably and efficiently attained with advanced instrumentation technology, effective cleaning of the entire root canal system remains a challenge. Rotary nickel titanium instruments are known for their efficient preparation of root canal. This is mainly because of the super elasticity of the nickel titanium alloy which gives an increased flexibility and allows the instrument to efficiently follow the original path of root canal. The purpose of this study is to compare the cleaning efficiency and shaping ability of M two, K3, Race ni-ti rotary instruments during the preparation of curved canals in extracted molars.
Materials and Methods:
Thirty teeth with 18 mm as their working length were selected and divided into three groups of 10 teeth each Angle of curvature, Radius of curvature, was determined using computerized tomography. A Pre and Post-operative measurement of canal width and volume was recorded and compared using CT. The teeth was then sectioned into two halves and subjected to scanning electron microscope. Images were taken at the level of apical third, middle third and coronal third for debris and smear layer. Scoring was done separately for both debris and smear layer.
Results:
Results were tabulated and statistically analyzed to evaluate the shaping ability and cleaning efficiency. Instruments were examined for any deformation or fracture during canal preparation.
Conclusion:
M two showed greater enlargements in all the three levels, when compared its width and volume, with other two instruments. K3 was better than Race when compared among them. In the scanning electron microscope study for debris and smear layer M Two performed better followed by K3 and Race.
Keywords: Cleaning and shaping, Computerized tomography, and M Two, rotary Ni Ti
Introduction
Successful root canal treatment depends primarily on the removal of micro-organisms through chemo-mechanical instrumentation of the root canal system. While root canal shaping can be predictably and efficiently attained with advanced instrumentation technology, effective cleaning of the entire root canal system remains a challenge.[1]
Shaping implies the development of a unique shape for every root canal, which is directly related not only to the length but also to the position and curvature of each individual root and root canal. Curvature is a frequent occurrence in the human dentition and when a curvature is present, endodontic preparations become difficult. These problems have resulted in a wide search of innovative materials, instruments and techniques to obtain a clean disinfected, debris free canal for obturation.[2]
The NiTi alloy Nitinol was developed in the early 1960's by W.F. Buchler.[3] Rotary nickel titanium instruments are more efficient in preparation of root canal, as the super elasticity of the nickel titanium alloy gives an increased flexibility and allows the instrument to efficiently follow the original path of root canal.[4]
The purpose of this ex vivo study is to compare the shaping ability and cleaning efficiency of M two with K3 and RaCe nickel titanium rotary instruments in the mesio buccal root of maxillary upper first molars with 25 to 35 degree curvature and radius of 4 mm to 9 mm which is determined by computerized tomography. K3 and RaCe were chosen because both systems have been reported to respect original root canal curvature well and also safe to use, these two instruments were as controls under identical experimental conditions.
Materials and Methods
Sixty extracted human upper first molar free from caries which were extracted due to periodontal reasons were taken and stored in saline. All these teeth were scanned with Computerized Tomography (CT) (G E COMPANY). Using Schneider technique, the angle and radius of curvature was determined. Forty five teeth were selected and included in the study with their curvature ranging from 25 to 35 degree and radii 4 to 9 mm.
In the pool of forty five teeth 10 roots had separate (MB2) canals. For standardization, the root with (MB2) canals was excluded from the study.
The access opening was done using Endo access bur (Dentsply) and the canal patency was checked with 10 size file (k file). The working length was obtained by measuring the length of the initial instrument at the apical foramen minus 1mm as the safety allowance. All selected teeth had a mesio buccal root length of 18 mm from coronal end till the radiographic apex. Occlusal reduction was done wherever necessary to maintain the working length of 18 mm.
Thirty teeth with 18 mm as their working length were selected and divided into three groups of 10 teeth each. Three NiTi rotary instruments K3, M two, and RaCe were used and they were divided into three groups. All the teeth were numbered 1 to 10 and were kept separately in sterile individual boxes for easy identification.
Group A - K3 Ni Ti rotary instrument (1-10)
Group B - RaCe Ni Ti rotary instrument (11-20)
Group C - M two Ni Ti rotary instrument (21-30)
Instrumentation
Initial filing was done from 15 to 25 size k file
All the three groups were instrumented with Anthogyr Mini head reduction gear hand piece 1 : 124 (Denstply) After each instrumentation the canal was irrigated with 5 ml of 5.25% sodium hypochlorite and finally flushed with saline. Crown down technique was used in a gentle in and out motion according to the manufacturers’ instruction.
Evaluation of shaping ability
After the canal preparation, the teeth were scanned again. The width and volume were calculated in the prepared tooth.
The pre and post operative images were compared and evaluated by subtracting the values of the images to determine the shaping ability of the instrument. The difference prior to and after instrumentation was analyzed statistically using ANOVA and the post hoc Student-Newman Keuls test.
Evaluation of cleaning efficiency
All root canals were prepared for SEM investigation and examined under the SEM (Philips PSEM 500 ×, Eindhoven, The Netherlands). After instrumentation the canals of each group were dried with paper points. The mesio buccal root was separated from the tooth using a diamond disc. Two shallow grooves were cut on each root in a bucco lingual direction. The roots were then split longitudinally with a chisel and mallet and the sections were prepared for SEM.
Separate evaluations were recorded for debris and smear layer. The cleanliness of each specimen was evaluated in three areas (apical, middle, and coronal third of the root) by means of a numerical evaluation scale (Hulsmann et al. 1997). The data established for scoring the debris and the smear layer were separately recorded and analyzed statistically. Owing to the ordinal nature of the scores, the data were subjected to the nonparametric Kruskal—Wallis test.
Instrument deformation
Length of the used ni-ti instruments was checked visually to assess instrument breakage or deformation.
Results
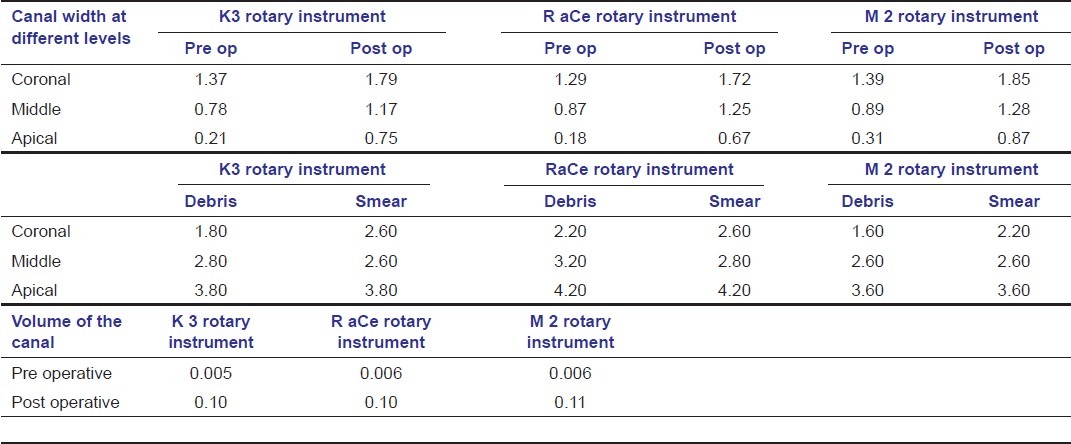
Comparison of Width of the instruments in coronal, middle and apical region shown in Table 1.
Table 1.
Comparison of Width of the instruments in coronal, middle and apical region
Discussion
The study compares the shaping ability and cleaning efficiency of M two instrument with K3 and RaCe using CT.
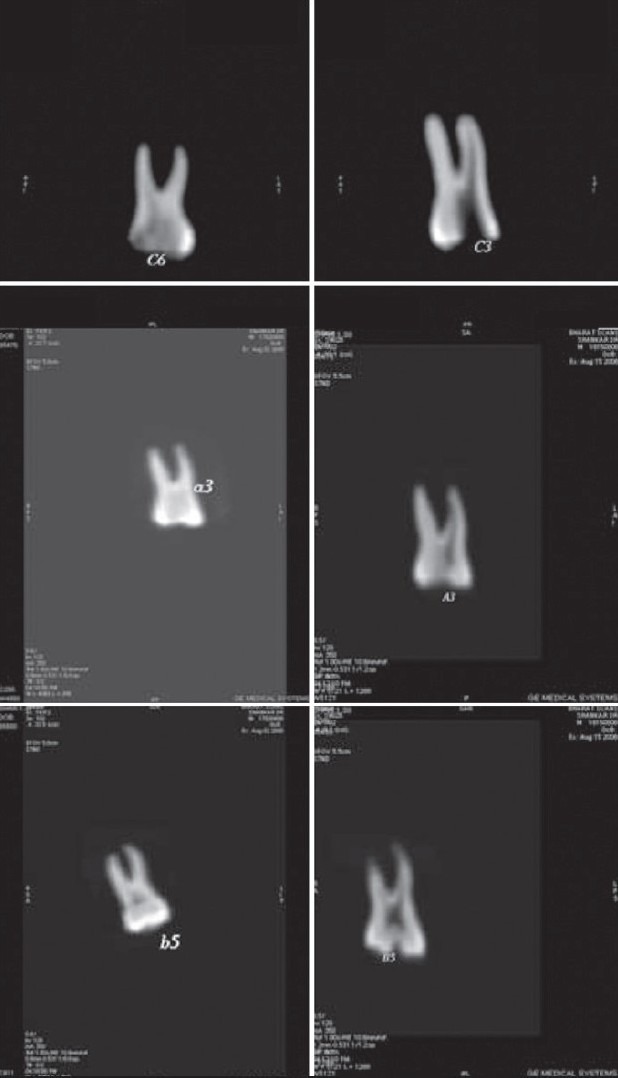
CT uses a fan shaped beam and multiple exposures in 360 degree around an object to reveal the internal architecture of the object. In this way the clinician can view the morphological and pathological features from three different dimensional perspectives.[5]
Two techniques followed for determining the canal shape:
Superimposition of the pre and post-operative images using radiographs or CT scan.[6]
Subtracting the values from pre and post operative images from the computer[7]
Shaping ability
In the present study, the second method was followed to determine the shaping ability by subtracting the pre and post operative values bucco-lingually for the canal width and volume using computerized tomography. The Dicom Viewer software used in this study demonstrates the sections at different levels of the canal. The software allows easy measurement of canal changes as, each image has an accurate scale to measure, thereby decreasing the potential of a radiographic or photographic error which is similar to the studies done by Gluskin et al.[6]
The pre and post operative images of the surface area (width) of the canal were matched and evaluated. The amount of instrumented surface could be calculated by subtracting the pre operative images with post operative images, which is in accordance with the study done by Peters et al, and Bergmans et al. in 2001.[7,8]
While comparing the coronal 3rd of the three experimental groups, the post operative width of the M two was more than that of K3 and RaCe. In the middle and apical 3rd again the width of M two was marginally higher than K3 and RaCe. M two showed better shaping ability when compared to K3 and RaCe in all the three sections [Figure 1 and 2].
Figure 1.

Width of canals M2 and Race
Figure 2.

Width of canal K3
Volume was determined using the dicom viewer software.[6] The volume determination is based on visual mapping and subtracting the pre and post operative images. By subtracting the pre canal volume from the post canal volume, the volume of canal was determined. Furthermore, visual inspection of the general shape could be made in all the three experimental groups. Even though there were only minimal difference, M two was marginally better than K3, followed by RaCe [Figure 3 and 4][9,7].
Figure 3.
Volume of canal after using M2, K3, Race
Figure 4.
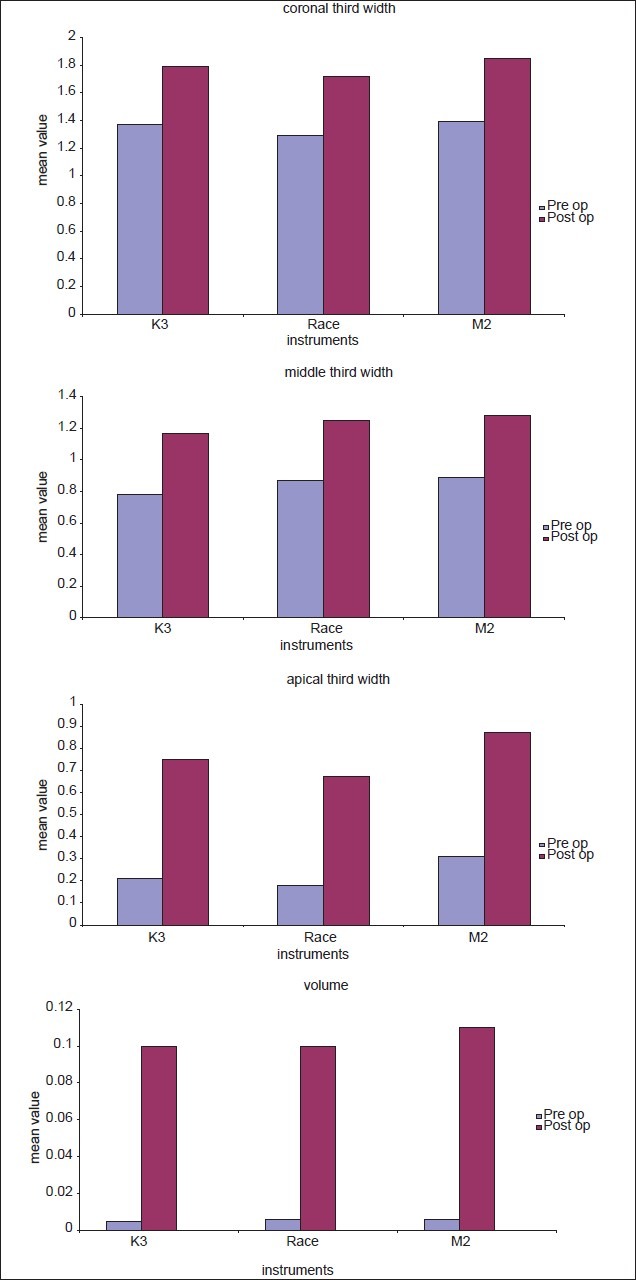
Graphical representation of canal width and volume
Cleaning efficiency
Sodium hypochlorite (NaOCl) is the most favored endodontic Root canal irrigant in modern practice because of its tissue-dissolving, antiseptic, antibacterial and lubricant properties. In this study, the canal was irrigated between each successive instrument with 5 ml of 5.25% sodium hypochlorite. The final flush was performed with 5 ml of saline solution using a disposable syringe similar to the studies done by Schafer et al.[10,11]
In all three instrumentation, the partially un-instrumented areas with remaining debris were found in all groups and all canal sections, and are similar with studies done by Hulsmann et al. and Peters et al.[12,8,13]
The present study indicates that the middle and coronal third were cleaner when compared to the apical third of the canals regardless of the instruments and technique used [Figure 5].
Figure 5.
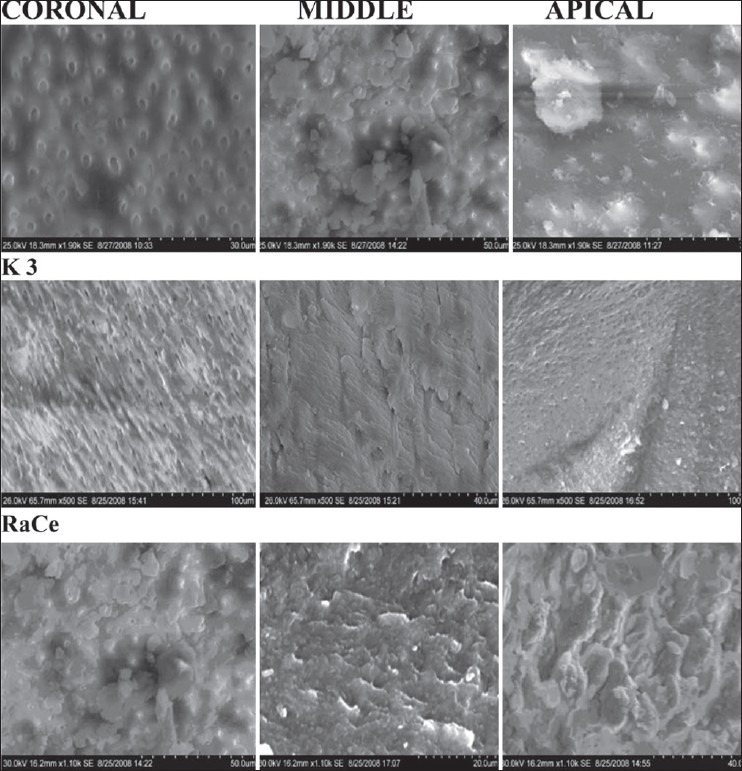
Smear layer sem pictures
M two had lesser remaining debris when compared with K3 and RaCe. In the present study it was also found that the increasing amounts of debris and smear layer were towards the apical region after preparation with all the three instruments and more in RaCe Ni Ti instrument which was identical with studies done by (Hulsmann et al. and Plotino et al.)[14,15]
To summarize, M Two had better results in cleaning and shaping of root canal when compared with K3 and RaCe rotary instruments, which may be due to its instrument design with[16] two sharp cutting edges and relatively small diameter with S shaped cross section, Non cutting safety tip, and above all increasing pitch length (blade chamber) from the tip to the shaft. This design is alleged to have two functions: i) to eliminate threading and binding in continuous rotation (ii) to reduce the transportation of debris towards the apex.
Instrument failure
All the three Ni Ti rotary instrument sequence used in this study respected the canal anatomy and there was no instrument fracture. In the present study no instrument separated and no instrument was permanently deformed. This may be due to the fact that each set of instruments were used only in ten teeth and only in mesio buccal canals, which is well within the safe number of uses recommended by manufacturer.
Conclusion
Within the limitations of this ex vivo study:
All the three groups of instruments had an increase in canal width and volume and were safe to use with limited applications. M two showed greater canal enlargement in all three levels, when compared to its width and volume, followed by K3 and RaCe.
In the scanning electron microscope study for debris and smear layer, M two had less debris and smear layer score in all the three levels followed by K3 and RaCe. Instruments were unable to produce a dentine surface free from smear layer and debris in the apical third. No incidence of instrument fracture or deformation was observed.
Computer tomography can be used as a non invasive and non destructive technique to evaluate various aspects of root canal preparation, both in vitro and in vivo. It is a valuable tool to study root canal geometry and changes after preparation in three dimensions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Lim TS, Wee TY, Choi MY, Koh WC, Sae-Lim V. Light and scanning electron microscopic evaluation of Glyde file prep in smear layer removal. Int Endod J. 2003;36:336–43. doi: 10.1046/j.1365-2591.2003.00648.x. [DOI] [PubMed] [Google Scholar]
- 2.Schilder H. Cleaning and shaping the root canal. Vol. 18. Bonaire: DCNA; 1974. pp. 269–99. [PubMed] [Google Scholar]
- 3.Thompson SA. An overview of nickel titanium alloys used in dentistry. Int Endod J. 2000;33:297–310. doi: 10.1046/j.1365-2591.2000.00339.x. [DOI] [PubMed] [Google Scholar]
- 4.Ayar LR, Love RM. Shaping ability of ProFile and K3 rotary Ni-Ti instruments when used in a variable tip sequence in simulated curved root canals. Int Endod J. 2004;37:593–601. doi: 10.1111/j.1365-2591.2004.00851.x. [DOI] [PubMed] [Google Scholar]
- 5.Brooks S. Advances in dental imaging. Computed Tomography. DCNA. 1993;187:513–20. [Google Scholar]
- 6.Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84. doi: 10.1046/j.1365-2591.2001.00422.x. [DOI] [PubMed] [Google Scholar]
- 7.Bergmans L, Van Cleynenbreugel J, Wevers M, Lambrechts P. A methodology for quantitative evaluation of root canal instrumentation using microcomputed tomography. Int Endod J. 2001;34:390–8. doi: 10.1046/j.1365-2591.2001.00413.x. [DOI] [PubMed] [Google Scholar]
- 8.Peters OA, Schonenberger K, Laib A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. IEJ. 2001;34:221–30. doi: 10.1046/j.1365-2591.2001.00373.x. [DOI] [PubMed] [Google Scholar]
- 9.Bergmans L, Van Cleynenbreugel J, Beullens M, Wevers M, Van Meerbeek B, Lambrechts P. Progressive versus constant tapered shaft design using NiTi rotary instruments. Int Endod J. 2003;36:288–95. doi: 10.1046/j.1365-2591.2003.00650.x. [DOI] [PubMed] [Google Scholar]
- 10.Schafer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary M two instruments. Part1: shaping ability in simulated curved canals. Int Endod J. 2006;39:196–202. doi: 10.1111/j.1365-2591.2006.01074.x. [DOI] [PubMed] [Google Scholar]
- 11.Schafer E, Vlassis M. Comparative investigation of two rotary nickel- titanium instruments: ProTaper versus RaCe. Part 1: Shaping ability in simulated curved canals. Int Endod J. 2004;37:229–38. doi: 10.1111/j.0143-2885.2004.00786.x. [DOI] [PubMed] [Google Scholar]
- 12.Hülsmann M, Rümmelin C, Schäfers F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments: a comparative SEM investigation. J Endod. 1997;23:301–6. doi: 10.1016/S0099-2399(97)80410-4. [DOI] [PubMed] [Google Scholar]
- 13.Peters OA, Peters CI, Schönenberger K, Barbakow F. ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. Int Endod J. 2003;36:86–92. doi: 10.1046/j.1365-2591.2003.00626.x. [DOI] [PubMed] [Google Scholar]
- 14.Hulsmann M, Gressmann G, Schafers F. A comparative study of root canal preparation using FlexMaster and HERO 642 rotary Ni-Ti instruments. Int Endod J. 2003;36:358–66. doi: 10.1046/j.1365-2591.2003.00664.x. [DOI] [PubMed] [Google Scholar]
- 15.Plotino G, Grande NM, Sorci E, Malagnino VA, Somma F. A comparison of cyclic fatigue between used and new Mtwo Ni-Ti rotary instruments. Int Endod J. 2006;39:716–23. doi: 10.1111/j.1365-2591.2006.01142.x. [DOI] [PubMed] [Google Scholar]
- 16.Sonntag D, Ott M, Kook K, Stachniss V. Root canal preparation with the NiTi systems K3, Mtwo and ProTaper. Aust Endod J. 2007;33:73–81. doi: 10.1111/j.1747-4477.2007.00062.x. [DOI] [PubMed] [Google Scholar]