

Abstract
Despite the well established influence of peer experiences on adolescent attitudes, thoughts, and behaviors, surprisingly little research has examined the importance of peer context and the increased prevalence of depressive symptoms accompanying the transition into adolescence. Examination of social networks may provide some insight into the role of peers in the vulnerability of some adolescents to depression. To address this issue, we leveraged an existing sample of 5,563 Chinese 10th graders to incorporate social network data into a multilevel regression model of depressive symptoms. We found that, in this sample, being nominated as a friend was more important than being nominated as most liked. Social network centrality was significantly associated with depression; those adolescents who were less connected were more likely to suffer from depression. The risk of depression for those who were marginal members of classroom social networks was substantial. These findings suggest that a social network perspective could help to increase the effectiveness of programs aimed at preventing adolescent depression.
Keywords: Social Network, Adolescent, Depressive Symptoms, Peer relations, China
Adolescence is a developmental period marked by significant growth and change, particularly as it relates to the social environment. It is a time of self-concept and identity development, when peers and peer groups often become a context within which to explore these new roles and identities. When these trends are combined with research demonstrating that individuals who are less socially integrated have more internalizing problems (Almquist, 2009; Berkman, Glass, Brissette, & Seeman, 2000; Ostberg, 2003), it is clear that social environmental and social competence factors become increasingly significant for adolescent development (Ueno, 2005). Social integration is often measured with social network instruments which allow for examination of the structural elements of peer groups (for example, network density, centralization, and transitivity) and also permit a more comprehensive view of the patterns and influence of social relationships.
The link between social isolation and decreased psychological well-being has been well established (for reviews see, Berkman, 1995; House, Landis, & Umberton, 1988), historically dating back to Durkheim’s work in sociological theory (see Gibbs, & Martin, 1958; Inkeles, 1959). Small social networks, low social support, and few or poor quality close relationships have all been linked to depressive symptoms (see Seeman, 1996). For children and adolescents in particular, depression and depressive symptoms – the primary distinction between these two lines of research has typically been clinical diagnosis versus self-report of symptomology (for further detail see Brooks-Gunn, 1991; Petersen, et al., 1993) – have been associated with lower peer acceptance (Rose & Rudolph, 2006) and being less liked by classmates (Caldwell, Rudolph, Troop-Gordon, & Kim, 2004).
Many developmental theories include peer relations as important concepts in both positive and negative adaptation during adolescence, which is not surprising given the prominent place they occupy in an adolescent’s life (For examples, see Bandura, 1989; Baumeister & Leary, 1995; Berndt, 2002; Coie, 1990; Cole, Martin, Peeke, Seroczynski, & Hoffman, 1998; Hartup, 1996; Hartup & Stevens, 1997). The developmentally important tasks related to peer functioning and social competence become criteria for judging successful adjustment and aptitude by an individual, parents, teachers, and the larger society in general. Despite the importance of peer experiences during adolescence, there has been relatively little research examining how peer context and social environment might be important in understanding the increase in the prevalence of depression that accompanies the transition into adolescence.
Social Network Status and Depression among Adolescents
Theorists have long proposed that the environment, the social environment in particular, plays a critical role in the development of psychological distress and illness (for example, see Bowlby, 1951; 1980; 1988; Bronfenbrenner, 1979; 1999), including depression and depressive symptoms. Bowlby (1951) posited a universal human need to form close affective bonds. Over the past several decades of research, these ecological models have been increasingly emphasized in efforts to understand health behaviors.
Luke and Harris (2007) described social network analysis as “uniquely suited to describing, exploring, and understanding these types of structural and relational aspects of health.” As mentioned previously, social integration has received the bulk of the attention, but more recent efforts have begun to examine other structural elements of social networks and their influence on health and well-being (Falci & McNeely, 2009; Ostberg, 2003; Ueno, 2005). For example, measures of centrality in networks assess the extent to which one node connects to other nodes, and the tendency of that node to be positioned near the center of its network. Centrality is often considered an indicator of importance or influence, with the simplest centrality measure being a count of the number of network nominations received from others (the term for this is in-degree centrality). Those with more connections or ties tend to be more central to the network (Valente, 2010). Network centrality has been associated with various health behavior outcomes, such as sexual activity (Ellen et al., 2001), aggression (Xie, Cairns, & Cairns, 2002), and smoking (Alexander, et al., 2001; Valente, Unger, & Johnson, 2005). Other research has suggested positive outcomes (absence of depression) are associated with being athletic, popular, and performing well academically (Farmer & Rodkin, 1996). Fowler and Christakis (2008) found network centrality to be associated with greater happiness, with centrality leading to happiness rather than the opposite in an adult sample.
Social network status is an interpersonal versus intrapersonal measure; it is a more objective measure than how an individual perceives their social influence or competence. For this reason, social network measures are a valuable addition to work attempting to quantify the social world of adolescents (Valente, 2010). Much of the research examining social competence and depression outcomes has solely relied on self-report measures (typically Likert-type scales) of perceptions of peer status and social competence (Caldwell, Rudolph, Troop-Gordon, & Kim, 2004; House, Landis, & Umberton, 1988). This cognitive approach has demonstrated that an individual’s perceptions about the social environment and how he or she believes he or she fits into that environment are critically important to depression outcomes. Less work has been done examining how interpersonal measures of the social environment, such as social network nominations, are related to depression in youth. Social network status, much like similar measures of social isolation and integration, has been linked to psychological health and well-being (Berkman, Glass, Brissette, & Seeman, 2000; Ostberg, 2003; Valente, 2010). As adolescents seek out connections to others in the course of developmental processes, peer status becomes an important indicator of growth and adjustment. If efforts to connect are unsuccessful, and result in failure or dysfunctional relationships and social networks, youth can feel socially isolated and excluded; such feelings can develop further into depressive symptoms and other maladaptive health outcomes.
Hypotheses
Structural aspects of peer networks during adolescence—a period when friendships play an increasingly powerful role in development—merits examination for its potential role in depressive symptomology. Therefore, the primary aim of this study was to examine whether social network status in the classroom is associated with adolescent depression outcomes. Accordingly, the study tested whether adolescents with more limited social networks had higher self-reported depressive symptoms. Four hypotheses were developed and tested for this study:
H1: Social network centrality, based on friend nominations, is negatively associated with adolescent depressive symptoms.
H2: Low social network status based on friend nominations is positively associated with depressive symptoms.
H3: Low social network status, based on most liked nominations, is positively associated with depressive symptoms.
These models were tested using a continuous measure of depressive symptoms, as well as using cut-points identified in past work with the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) as a measure of depression. The hypothesis tested for these analyses was:
H4: The associations between social network status and depression are stronger than the associations between social network status and depressive symptoms.
Methods
Sampling
China has two primary high school types, academic (regular) and professional (vocational). Students are tested in middle school and scores from those tests determine which type of school they will attend. Generally, those attending academic schools have a rigorous schedule of courses for three years of high school (10th through 12th grades), designed to increase the chances students will pass college entrance exams. Those attending professional schools are enrolled in a career track, such as computers/IT or public relations, and will complete an internship during their final year(s) in high school with the goal of entering the workforce once they have completed high school. Both school types were included in the study, with an equal number of schools and students from each school type. There are more professional school classes in the study, however, due to a trend for these classes to be smaller.
The study included a total sample of 5,563 10th grade students from a convenience sample of 24 schools, 12 of each school type, from 124 classes in the city of Chengdu in the Sichuan province in southwestern China. We chose this sample because the data contained the desired information on social relations between sample members as well as data on depression and depressive symptoms and because it was readily available to us.
Data collection
The data for this study was collected as pre-intervention, baseline measurements of a larger parent study examining the efficacy of a school-based tobacco prevention program focusing on social influences. All assessments were paper-based surveys and all participants had active parental consent and student assent. Pre-intervention assessments were collected prior to any intervention delivery, with the pre-test occurring approximately one week prior to intervention implementation for those assigned to the Program condition. The baseline survey was collected approximately one month prior to the pre-test. There were two reasons for the two waves of pre-intervention data collection: 1) the major holiday, Chinese New Year, occurred during that time and would have disrupted data collection efforts and 2) the assessments were each fairly substantial and splitting the measures between two surveys prevented students from becoming fatigued and improved the quality of the data. However, for the purposes of this study, and due to the short time between pre-intervention assessments and relative stability of the measures of interest over such a short time period, the data is considered cross-sectional in nature.
Measures
Depressive symptoms (CES-D; Radloff, 1977)
The CES-D is a self-administered scale containing 20 items. The answers to each item, which indicate the frequency of the symptoms, are structured on a 4-point Likert scale ranging from 1 (Less than 1 day) to 4 (5-7 days). The answers are summed across all 20 items. The total scores can range from 0 to 60. The Cronbach’s alpha for the scale for the entire sample was good at α = 0.89.
Depression
Radloff’s (1977) original work using clinical diagnostic comparisons suggested, and it was commonly accepted, that persons who score 16 or above were likely to be clinically depressed; however, more recent studies suggest that the cut-point needs to be raised to 24 or higher if the tool is to achieve appropriate diagnostic characteristics (Gotlib, Lewinsohn, & Seeley, 1995; Roberts, Lewinsohn, & Seeley, 1991). The Mandarin-Chinese version of the CES-D (MC-CES-D) has been validated and used in Hong Kong (Cheung & Bagley, 1998) and among community samples of adolescents in Taiwan (Lin et al., 2008). Yang and colleagues (2004) used the MC-CES-D in a two-phase survey for depressive disorders among non-referred adolescents in Taiwan. They found that the adolescents with total MC-CES-D scores greater than 28 were more likely to have major depressive disorder with or without functional impairment. Based on these previous studies, with similar populations, the present study defined those adolescents whose MC-CES-D score was 28 or higher as having significant depression (dichotomized depression outcome measure: 0 = CES-D <28; 1= CES-D ≥28).
Social network measures
Sociometric procedures were used to obtain measures of adolescents’ social network status. Peer nominations were used to collect information from each student regarding peer status. Adolescents were asked to list up to five people in their class who they considered their best friends. Students wrote the first and last names of their friends. Similarly, students nominated the five people they considered to be the most liked by people in their class. Peer nominations were later matched to study ids and names were dropped from the data to protect confidentiality. These nominations were then used to calculate network metrics for the study.
The simplest measure of network centrality is a count of the number of nominations a person gives (out-degree) or receives (in-degree). People with more friends will tend to be more central. The measure of network centrality used in this study (hypothesis 1) is in-degree, because it is the more commonly used measure of peer status in the literature (for example, see Bonacich, 1987; Borgatti, Carley, & Krackhardt, 2006; Krackhardt, 1992; Strauss & Pollack, 2003) and also due to the methodological constraint on out-degree of allowing only five, rather than unlimited, nominations. A standardized measure (to account for the different classroom network sizes) of in-degree was calculated and used in the models for this study.
In order to further explore social network status in a school classroom, researchers often divide individuals into different status categories based on their social network nominations. Network status categories are created to form a measure with a normal distribution, since the underlying network measures are usually skewed left. Categorization of network data also allows for more detailed examination of those on the fringes of the social network, as well as those who are highly central to the network. Those who receive an “average” number of nominations are of less interest in this type of analysis and often serve as the reference group. Five social network status categories were created from the friend nomination data for this study, similar to those created in past research (Almquist, 2009; Ostberg, 2003; Ostberg & Modin, 2008). The first category included those who did not receive any nominations. This group, the “marginalized” category, is usually considered at highest risk for many negative health behavior outcomes and consists of those students whom no one else has connected to the larger classroom social network. The second group consists of the “peripheral” members of the network, who received one or two friend nominations. Figure 1 is an example of one classroom friend network. Those with marginal and peripheral status end up around the edges of the network, with few and weak connections (typically one-way, non-reciprocated nominations if any) to peer groups within the class. The “accepted” category is the largest and includes those receiving three to five nominations. The “popular” category are those with six or seven nominations and the “favorites” those who received eight or more.
Figure 1.
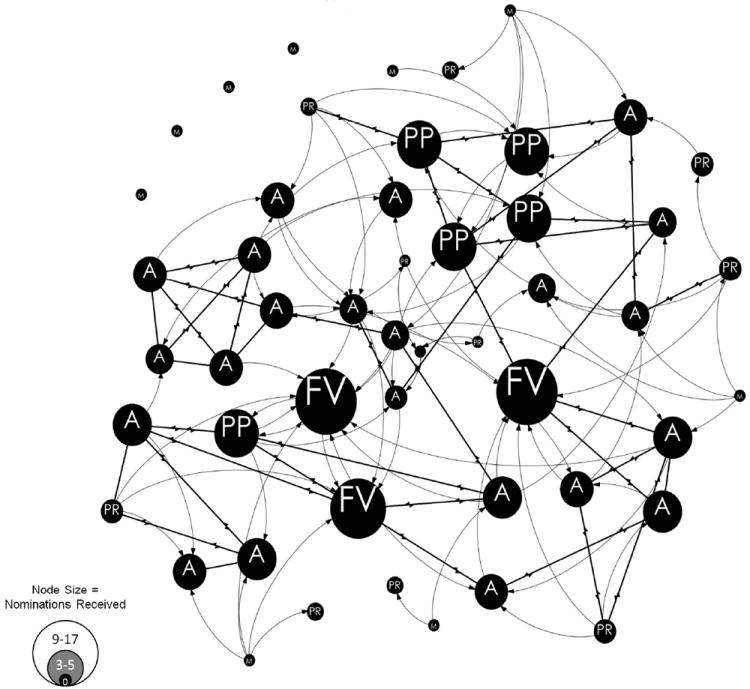
Classroom Friend Network Example
*Note that FV = Favorite; PP = Popular; A = Accepted; PR = Peripheral; M = Marginal
**Curved lines represent one-way friend nominations, straight lines represent mutual friend nominations
The same five status categories were created for the most liked nominations; however, because the distribution for this type of nomination differs from the friend data, the construction of the categories was different. Most liked nominations, often called “sociometric popularity,” usually have a larger range than friend nomination data with more network members receiving zero or only one nomination. A few network members usually receive the bulk of the most liked nominations in a classroom (see Figure 2). Therefore, the marginal category remains the same (no most liked nominations), but the other categories have slightly different cut-points (peripheral = 1 nomination; accepted = 2-4; popular = 5-8; and favorite = 9 or more nominations).
Figure 2.
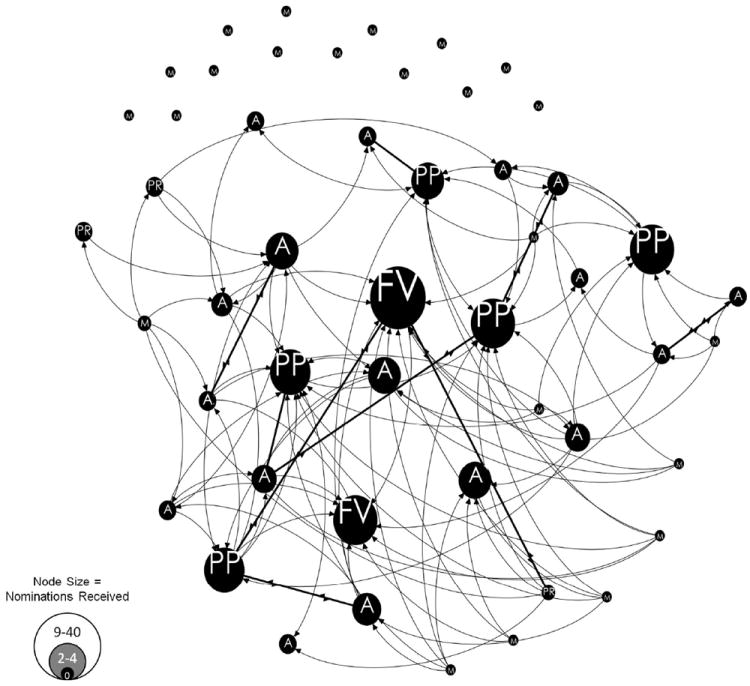
Classrooom Most Liked Network Example
*Note that FV = Favorite; PP = Popular; A = Accepted; PR = Peripheral; M = Marginal
**Curved lines represent one-way friend nominations, straight lines represent mutual friend nominations
The category cut-points for both the friend and most liked peer status measures were determined by past research (Almquist, 2009; Ostberg, 2003; Ostberg & Modin, 2008), theory and conceptual logic (e.g. students who receive no nominations are conceptually different than those who receive even one nomination from a peer, which is why the marginal category should always be the same – those with no nominations), and the distribution of the data (hence, slightly different cut-points for the two different peer nomination types was necessary in order to create peer status variables that each had a normal distribution).
Demographic covariates and control variables
Variables controlled for in the models include: socioeconomic status, age, female (female=1; male=0), and school type (academic or professional). Socioeconomic status was calculated using both mother’s and father’s education level and a measure of an adolescent’s disposable income.
Due to the large amount of research examining social cognitions, we know that an individual’s perceptions of their social environment, acceptance, and competence can contribute in a large way to depression-related outcomes (for review, see Jacobs, Reinecke, Gollan, & Kane, 2008). Therefore, it was necessary to control for these perceptions in order to determine if social network status contributes to depression independently of these social cognitions. Perceived social self-efficacy was controlled for in the models and was measured with the Perceived Social Self-Efficacy Scale (PSSE, Smith & Betz, 2000). This is a twenty-five item scale that asks about confidence in your ability to perform social tasks, with items structured on a 5-point Likert scale ranging from 1 (No confidence at all) to 5 (Complete confidence). Answers were summed with total scores ranging from 1 to 125. Cronbach’s alpha for the scale was good (α = 0.90). Smith and Betz (2000) suggested that the validity and reliability data on the PSSE support the scale as a strong measure of social self-efficacy across gender and ethnic groups. Further, Fan and colleagues (2010) recently validated the scale in Chinese samples and found excellent psychometric properties, including a single-factor structure, high internal consistency, high test-retest reliability, and acceptable convergent and discriminant validities. These findings essentially replicated the original findings from Smith and Betz (2000) on the scale. As would be expected, social network status and Perceived Social Self-Efficacy were significantly correlated (r= 0.15 for friend in-degree and r=0.18 for most liked in-degree, p<0.05 for both). However the correlations were small to moderate, suggesting the measures are quantifying different aspects of an adolescent’s social world (intra- versus interpersonal).
Data Analysis
Both multilevel linear and logistic regression analysis procedures were used to analyze the data. Multilevel analysis was needed to explain individual-level outcomes with school and class level characteristics. All analyses were done using STATA version 11 (StataCorp, 2009), with social network metrics calculated using UCINet (Borgatti, Everett, & Freeman, 1999).
To examine the first hypothesis, that in-degree centrality is negatively associated with depressive symptoms, multilevel linear regression analyses were conducted, simultaneously entering in-degree and the demographic and control variables in the level-one (fixed effects) model and school type in the level-three (school-level random effects) model for depressive symptoms. There were no level two (class level) variables, though level of analysis was included in the random effects model.
Two other models were tested in the same fashion to examine hypotheses two and three, that low social network status is positively associated with depressive symptoms. Dummy variables for each status category were included in these models; Model 2 for status based on friend nominations and Model 3 for status based on most liked nominations. The accepted category served as the reference group. The two categories below “accepted,” the “peripheral” and “marginal” categorizations serve as the low status measures mentioned in the second and third hypotheses.
The final hypothesis was analyzed by multilevel logistic regression and examined the same independent variables as the first three models. These final three models used an outcome that was a dichotomized version of the CES-D score, with scores of ≥28 equal to one and all other scores equal to zero (see Measures for further details of cut-scores).
Results
Distribution of Demographic Characteristics and Main Study Variables
The participation rate for the study was high, with a 93.3% participation rate. Table 1 presents descriptive data for the sample. The average age of participants was 15.8 and the mean SES, ranging from 1-10 on a composite measure including mother and father education and allowance per week, was 4.4. The mean depressive symptoms score (CES-D; range: 1-60) for the sample is 17.9. Using a cut-point score of 28 or greater on the CES-D resulted in 16.8% of the sample reporting being depressed. The mean score on the perceived social self-efficacy scale was 80.4 with a range of 1-125. The average number of friends a student nominated was 3.7, and 3.5 was the average for most liked nominations. The most friend nominations received by a single student was 17 and the most liked nominations received by a single student was 40. About half of the sample (49.3%) had a friend network status of “accepted,” whereas 33% had an “accepted” most liked network status.
Table 1.
Sample Characteristic
| Total | Academic | Professional | Girls | Boys | Range | |
|---|---|---|---|---|---|---|
| Schools | 24 | 12 | 12 | |||
| Classes | 124 | 56 | 68 | |||
| Mean class size (SD) | 51.8 (12.2) | 55.6 (13.8) | 48.3 (9.3) | |||
| Gender | ||||||
| Male (%) | 50.3% | 49.4% | 50.9% | |||
| Female (%) | 49.7% | 50.6% | 49.1% | |||
| Mean Age (SD) | 15.8 (0.72) | 15.7 (0.64) | 16.0 (0.77) | 15.7 (0.70) | 15.9 (0.73) | 13-19 |
| Mean SESa (SD) | 4.4 (1.5) | 5.0 (1.5) | 3.8 (1.2) | 4.4 (1.5) | 4.4 (1.5) | 1-10 |
| Mean CES-D Score (SD) | 17.9 (11.0) | 18.7 (11.4) | 17.1 (10.5) | 18.6 (11.4) | 17.1 (10.5) | 0-60 |
| CES-D Score ≥ 28b (%) | 16.8% | 21.7% | 16.2% | 21.5% | 16.2% | |
| Mean PSSE (SD) | 80.4 (19.9) | 80.8 (20.4) | 80.0 (19.5) | 80.3 (18.6) | 80.6 (21.3) | 1-125 |
| Social network measures | ||||||
| Mean friend nominations (SD) | 3.7 (2.4) | 4.0 (2.3) | 3.8 (2.3) | 4.1 (2.2) | 3.7 (2.3) | 0-17 |
| Mean friends nominated (SD) | 3.7 (2.0) | 3.9 (1.9) | 3.6 (2.1) | 4.0 (1.8) | 3.5 (2.1) | 0-5 |
| Mean most liked nominations (SD) | 3.2 (4.3) | 3.5 (4.5) | 3.5 (4.3) | 3.2 (4.2) | 3.8 (4.6) | 0-40 |
| Mean most liked nominated (SD) | 3.5 (1.9) | 3.6 (1.8) | 3.5 (1.9) | 3.8 (1.8) | 3.3 (1.9) | 0-5 |
| Friend social network status (%) | ||||||
| Marginalized (0 friend noms.) | 3.0% | 2.4% | 3.2% | 2.0% | 3.7% | |
| Peripheral (1-2 noms.) | 11.7% | 25.7% | 28.3% | 23.4% | 30.8% | |
| Accepted (3-5 noms.) | 49.3% | 47.1% | 46.8% | 49.3% | 44.3% | |
| Popular (6-7 noms.) | 28.8% | 17.2% | 15.0% | 17.5% | 14.7% | |
| Favorite (8+ noms.) | 7.2% | 7.6% | 6.7% | 7.8% | 6.5% | |
| Most liked network status (%) | ||||||
| Marginalized (0 most liked noms) | 21.0% | 22.3% | 19.7% | 24.6% | 17.3% | |
| Peripheral (1 nom.) | 20.1% | 20.1% | 20.0% | 20.3% | 19.8% | |
| Accepted (2-4 noms.) | 33.0% | 31.5% | 34.5% | 31.2% | 34.9% | |
| Popular (5-8 noms.) | 15.7% | 14.7% | 16.7% | 14.9% | 16.7% | |
| Favorite (9+ noms.) | 10.2% | 11.4% | 9.1% | 9.0% | 11.3% |
SES was measured by calculating the mean of the answers on three questions for each student. Two questions asked about father’s and mother’s highest level of education (1-7) and the third question asked about allowance per week (1-10).
Differences in Study Variables by School and Gender
A series of t-tests were conducted to determine equivalence on the main study variables for adolescents in the different school types and for males and females. Academic and professional school students were significantly different on depressive symptoms, t(5369) = 5.29, p < 0.01, with those attending academic schools having significantly higher CES-D scores (a mean score of 18.7 versus 17.1 for those in professional schools). There were also significant differences on the social network measures for the different school types, with academic school students nominating more friends, t(6068) = 5.41, p < 0.01, and most liked, t(4578) = 3.38, p < 0.01, as well as being nominated more as friends, t(5688) = 3.51, p < 0.01. The only network measure with no significant differences by school type was most liked nominations received. Due to these significant baseline differences by school type, in particular the differences on the outcome measures, all models were run separately for each school type.
Differences also existed between males and females on certain study variables. As would be expected, depressive symptoms were significantly different, t(5369) = 5.13, p < 0.01, with females reporting higher mean CES-D scores (18.6 versus 17.1 for males). Females nominated more friends, t(6068) = 8.87, p < 0.01, and more people as most liked, t(4578) = 9.14, p < 0.01. Girls also received more friend nominations, t(5688) = 6.77, p < 0.01, than boys, but boys received more nominations for most liked, t(5688) = 5.33, p < 0.01, than girls. Again, due to these significant differences in the main variables, the models were run separately for girls and boys in order to more fully examine the study hypotheses.
Main Results
Multilevel linear regression analysis of social network status and depressive symptoms
The first model tested hypothesis one, that in-degree is negatively associated with depressive symptoms (see Model 1 in Table 2) indicating that those who receive more nominations are less likely to report depressive symptoms. Perceptions of social self-efficacy was the strongest predictor of adolescents’ depressive symptoms across all subgroups. In-degree centrality was significantly associated with CES-D scores for the total sample, β= -0.04, p < 0.01, and for the professional school sample, β= -0.05, p < 0.05. The association, however, is driven primarily by the significant association found for professional school girls, β= -0.08, p < 0.01. Hypothesis one was not confirmed for academic school students.
Table 2.
Standardized coefficients (β) for Three Models of Social Network Status and Depressive Symptoms by School Type & Gender
|
Depressive Symptoms
| |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Academic | Professional | |||||||||||||||||||
|
| |||||||||||||||||||||
| All | Girls | Boys | All | Girls | Boys | ||||||||||||||||
|
| |||||||||||||||||||||
| Modela | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 |
|
Fixed Effects Estimatesb
| |||||||||||||||||||||
| In-Degree (Friend) | -0.04** | -0.03 | -0.03 | -0.03 | -0.05* | -0.08** | -0.01 | ||||||||||||||
| Perceived Social Self Efficacy | -0.19** | -0.23** | -0.25** | -0.20** | -0.16** | -0.23** | -0.10** | ||||||||||||||
| Age | 0.02 | 0.02 | 0.03 | 0.02 | 0.03 | 0.05+ | 0.02 | ||||||||||||||
| SES | 0.08** | 0.05* | 0.06+ | 0.05+ | 0.12** | 0.17** | 0.07* | ||||||||||||||
| Female | 0.07** | 0.17** | 0.12** | ||||||||||||||||||
|
| |||||||||||||||||||||
|
Network Status (Friend)
| |||||||||||||||||||||
| Marginal | 0.04** | 0.01 | 0.01 | <0.01 | 0.07** | 0.11** | 0.05+ | ||||||||||||||
| Peripheral | 0.04* | 0.04+ | 0.07* | 0.02 | 0.04+ | 0.05 | 0.02 | ||||||||||||||
| Accepted | ref. | ref. | ref. | ref. | ref. | ref. | ref. | ||||||||||||||
| Popular | -0.01 | -0.01 | 0.02 | -0.05 | -0.01 | -0.02 | 0.01 | ||||||||||||||
| Favorite | 0.01 | -0.01 | 0.02 | -0.05+ | 0.02 | 0.02 | 0.03 | ||||||||||||||
|
| |||||||||||||||||||||
|
Network Status (Liked)
| |||||||||||||||||||||
| Marginal | 0.02 | 0.04 | 0.07* | -0.01 | 0.01 | <0.01 | 0.02 | ||||||||||||||
| Peripheral | 0.03 | 0.03 | 0.05 | 0.02 | 0.02 | 0.01 | 0.03 | ||||||||||||||
| Accepted | ref. | ref. | ref. | ref. | ref. | ref. | ref. | ||||||||||||||
| Popular | 0.02 | 0.01 | 0.03 | -0.02 | 0.02 | 0.05 | -0.01 | ||||||||||||||
| Favorite | 0.01 | <0.01 | 0.05 | -0.04 | 0.01 | <0.01 | 0.03 | ||||||||||||||
|
| |||||||||||||||||||||
|
Random Effects Estimates
| |||||||||||||||||||||
| Level 3 (School) | <0.01 | <0.01 | <0.01 | ||||||||||||||||||
| School Type | 0.06** | 0.06** | 0.05** | ||||||||||||||||||
| Level 2 (Class) | 0.07** | 0.08** | 0.10** | 0.09** | 0.10** | 0.13** | 0.11* | 0.12* | 0.17** | 0.14** | 0.16** | 0.19** | 0.10** | 0.08* | 0.09* | 0.10* | 0.09* | 0.12* | 0.20** | 0.17** | 0.12* |
|
| |||||||||||||||||||||
| Observations | 4626 | 4442 | 3935 | 2267 | 2162 | 1929 | 1202 | 1164 | 1048 | 1065 | 998 | 881 | 2359 | 2280 | 2006 | 1262 | 1229 | 1095 | 1097 | 1051 | 911 |
Three models were run using multilevel linear regression: Model 1 examined in-degree (from friend nominations) as the independent variable (IV) of interest; Model 2 examined the five different network status categories from friend nominations as the IV of interest; and Model 3 examined the five network status categories from most liked nominations as the IV of interest.
The covariates were included in all three models, however, they did not differ between models and are therefore only reported under the first model for table readability.
p<0.10,
p<0.05,
p<0.01
Model 2 examined hypothesis two, which stated that low social network status based on friend nominations is associated with depressive symptoms, and resulted in mixed findings (see Table 2). Both low status categories, marginal and peripheral, were positively associated with CES-D scores, β=0.04, p < 0.05 for both, in the total sample. When subgroups were analyzed separately, however, the results were different. Marginal status was significant for professional students, β= 0.07, p < 0.01), though was stronger for girls, β= 0.11, p < 0.01, with boys only showing a trend towards significance, β= 0.05, p < 0.10. For academic school students, the marginal categorization was not significantly associated with depressive symptoms. Peripheral status was only significant for academic school girls, β= 0.07, p < 0.05. The categories indicating higher peer status, popular and favorite, were not significantly associated with depressive symptoms. The one exception was a trend towards a protective effect for academic school boys, β= -0.05, p < 0.10.
Model 3 in Table 2 examined hypotheses three, which stated that low social network status based on most liked nominations is associated with depressive symptoms, and was not well supported. Only marginal status was significantly associated with depressive symptoms for academic girls, β= 0.07, p < 0.05. This indicates, that for this sample, not being nominated as a friend is more important than having peers consider one as most liked in relation to depressive symptoms.
Multilevel logistic regression analysis of social network status and depression
Table 3 present the results for logistic regression analyses testing hypothesis four, that the associations will be stronger between social network status and depression than depressive symptoms. While direct comparisons between coefficients cannot be made, the magnitude of the associations can be considered. The associations between in-degree and depression show a similar pattern in this analysis as with the linear regression. Higher in-degree is protective against depression, AOR=0.88, p < 0.01, with the association being primarily driven by professional school girls, AOR=0.83, p < 0.05. The main differences between the logistic and linear regression results appear for Model 2. While the pattern of significant associations remain mostly the same, with professional school students showing significant associations between lower social status and depression, AOR=3.30, p < 0.01 for marginal and AOR=1.38, p < 0.05 for peripheral) and academic school students not showing this, the additional information comes in the form of the magnitude of the associations. The risk of depression for those who are marginal members of professional school social networks is substantial, with marginal girls at greatest risk, AOR=4.71, p < 0.01, and with marginal boys reporting fairly high risk as well, AOR=2.51, p < 0.01. Peripheral status showed a trend towards significance for professional girls, AOR=1.39, p<0.10, but not for boys.
Table 3.
Adjusted Odds Ratios for Three Models of Social Network Status and Depression (CES-D ≥28) by School Type & Gender
|
Depression (CES-D ≥28)
| |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Modela | Total Sample | Academic | Professional | ||||||||||||||||||
|
| |||||||||||||||||||||
| All | Girls | Boys | All | Girls | Boys | ||||||||||||||||
|
| |||||||||||||||||||||
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |
|
Fixed Effects Estimatesb
| |||||||||||||||||||||
| In-Degree (Friend) | 0.88** | 0.91+ | 0.91 | 0.89 | 0.84* | 0.83* | 0.85 | ||||||||||||||
| PSSE | 0.69** | 0.58** | 0.53** | 0.64** | 0.84* | 0.66** | 1.07 | ||||||||||||||
| Age | 1.06 | 1.04 | 1.07 | 0.93 | 1.07 | 1.10 | 1.04 | ||||||||||||||
| SES | 1.17** | 1.06 | 1.08 | 1.05 | 1.36** | 1.56** | 1.14 | ||||||||||||||
| Female | 1.48** | 1.52** | 1.52** | ||||||||||||||||||
|
| |||||||||||||||||||||
|
Network Status (Friend)
| |||||||||||||||||||||
| Marginal | 1.92** | 0.95 | 0.69 | 1.22 | 3.30** | 4.71** | 2.51* | ||||||||||||||
| Peripheral | 1.29** | 1.26+ | 1.25 | 1.28 | 1.38* | 1.39+ | 1.35 | ||||||||||||||
| Accepted | ref. | ref. | ref. | ref. | ref. | ref. | ref. | ||||||||||||||
| Popular | 0.85 | 0.76+ | 0.86 | 0.61+ | 0.96 | 0.98 | 0.97 | ||||||||||||||
| Favorite | 0.92 | 0.72 | 0.79 | 0.63 | 1.2 | 1.36 | 0.97 | ||||||||||||||
|
| |||||||||||||||||||||
|
Network Status (Liked)
| |||||||||||||||||||||
| Marginal | 1.14 | 1.24 | 1.33 | 1.17 | 1.04 | 0.81 | 1.44 | ||||||||||||||
| Peripheral | 1.16 | 1.15 | 1.12 | 1.19 | 1.19 | 1.26 | 1.1 | ||||||||||||||
| Accepted | ref. | ref. | ref. | ref. | ref. | ref. | ref. | ||||||||||||||
| Popular | 1.17 | 1.05 | 1.18 | 0.88 | 1.3 | 1.68* | 0.82 | ||||||||||||||
| Favorite | 1.06 | 0.98 | 1.3 | 0.7 | 1.12 | 1.1 | 1.27 | ||||||||||||||
|
| |||||||||||||||||||||
|
Random Effects Estimates
| |||||||||||||||||||||
| Level 3 (School) | <0.01 | <0.01 | <0.01 | ||||||||||||||||||
| School Type | 0.14** | 0.13** | 0.12** | ||||||||||||||||||
| Level 2 (Class) | 0.11 | 0.11 | 0.16* | 0.15 | 0.10 | 0.15 | 0.20+ | 0.19 | 0.22 | 0.40** | 0.32* | 0.36* | 0.23* | 0.16 | 0.20+ | 0.05 | 0.02 | <0.01 | 0.60** | 0.48** | 0.49** |
|
| |||||||||||||||||||||
| Observations | 4629 | 4444 | 3937 | 2268 | 2162 | 1929 | 1202 | 1164 | 1048 | 1066 | 998 | 881 | 2361 | 2282 | 2008 | 1262 | 1229 | 1095 | 1099 | 1053 | 913 |
Three models were run using multilevel logistic regression: Model 1 examined in-degree (from friend nominations) as the independent variable (IV) of interest; Model 2 examined the five different network status categories from friend nominations as the IV of interest; and Model 3 examined the five network status categories from most liked nominations as the IV of interest.
The covariates were included in all three models, however, they did not differ between models and are therefore only reported under the first model for table readability.
p<0.10,
p<0.05,
p<0.01
Model 3 in Table 3 does not support an association between network status based on most liked nominations, similar to the linear regression results, with one notable exception. Contrary to expectations, for professional school girls, those with popular status are at greater risk for depression, AOR=1.68, p<0.05.
Discussion
This study examined the association between social network status and depressive symptoms among Chinese adolescents. Consistent with previous research on social integration and depressive symptoms, the findings support a negative association between the more general measure of social network status, in-degree centrality for friend nominations, and depressive symptoms. These findings indicate that the higher the in-degree, the lower the depressive symptoms. Therefore, the more friend nominations an adolescent received from their classroom peers, the fewer depressive symptoms they reported. The specific hypothesis regarding low friend social network status and depressive symptoms was also supported. Individuals with fewer friends, who are on the fringe of the classroom social network, reported higher depressive symptoms. This is consistent with previous research that has shown that a lack of integration is associated with depression outcomes (Brendgen, Vitaro, & Bukowski, 2000; Falci & McNeely, 2009; Ueno, 2005). This finding was primarily driven by professional school students, with significant associations for both boys and girls, yet a stronger association for girls. For the most part, high social status was not significantly associated with depressive symptoms or depression, even in a negative direction. This indicates that while low social network status appears to be a risk factor for depression outcomes, it does not necessarily follow that high status is protective.
However, there was one contrary finding regarding high status network members. Professional school girls with popular status based on “most liked” nominations actually had an increased risk for depression. There is some research supporting this finding; Falci & McNeely (2009) reported adolescents with social networks that were either too small or too large reported higher levels of depressive symptoms. They put forth the idea that for those with high social status, higher depressive symptoms stem from a sense of duty or obligation. They stated that more friends require more time and energy to maintain and “could result in role strain.” Findings from this study indicate that this is the case for girls but not boys and professional school students and not academic school students. Also, this was not the case for peer status based on friend nominations.
Differences in study findings between social status based on friend nominations and status based on most liked nominations indicates that these are distinct constructs that measure unique aspects of an adolescent’s social status. Status based on friend nominations was more significantly associated with depressive symptoms, indicating that close friendships are perhaps a more important indicator for depression-related outcomes for Chinese adolescents. However, there was one instance where “most liked” status was important, for professional school girls, as mentioned previously. This finding suggests that while lower friend status is a risk factor as would be expected, it may be higher most liked status that is a risk factor for depression. Further explorations of the distinctions between these two social network measures and their differential effect on depression outcomes are needed.
There are clear differences between the two school types in the relationship between social network status and depressive symptoms. The associations are stronger for professional school students. The Chinese school system is set up differently than Western school systems, with academic school students required to spend many more hours per week studying for college entrance exams. They also have more pressure put on them to do well academically by their parents and teachers, and more competition from their classmates. They have little free time to socialize, which may be one reason for the differences noted in the study. Professional school students have more free time and fewer pressures – though for some, they may already consider themselves “failures” for not getting into an academic school, which could present a unique risk factor for depressive symptoms on its own. While academic school students, particularly the girls, report the highest levels of depressive symptoms, they do not appear to be that closely associated with what occurs in their social network. Dealing with school and family stress as well as gender role expectations could be a larger factor in their depression outcomes; however, further study would be required to examine this.
Study Limitations
The study presented several limitations that should be considered when interpreting the findings. First, this study did not include measures of the quality or strength of a reported relationship. It may be that the quality of social network ties can weight the relationship between these measures and depressive symptoms. For example, it may not matter if an individual has few friends if the quality of those friendships is very high, where friends provide maximum support, feelings of closeness, and understanding. It may also be the case that discrepancies between nominations given and received (for example, when a student nominates a peer as a friend but is not nominated by that person in return) are more important than the overall number of nominations to depressive symptoms.
Second, while the associations reported were significant, the effects were small. This could potentially limit the meaningfulness of the findings; however some have suggested that small effect size can still have practical applicability (Rosenthal, Rosnow, & Rubin, 2000). Due to the cross-sectional nature of the data, causal direction cannot be determined. The results can suggest avenues for future research, but cannot explain causal mechanisms leading from social network status to depressive outcomes. Further study with longitudinal data would enable a study of the evolution of the network over time and the relationship of these temporal dynamics to depressive symptomatology.
The CES-D is a self report assessment of depressive symptoms, rather than a clinical assessment of syndrome or disorder, therefore the findings of this study do not generalize to populations who have diagnosable disorders and it is not possible to determine whether the suggested relationships between social network status and depression-related outcomes are important mechanisms operating in more clinical populations. Also, though the design and measurement of the study enables examination of data from more than one source, which is a considerable strength of the study, the social network nomination format was limited to school-based peers which may not be the most influential peers for all youth.
Despite these limitations, the results confirm that social network status is significantly associated with depressive symptoms for Chinese adolescents.
Implications and Future Directions
It has become clear that depression has an impact on adolescent adjustment and psychological functioning (Petersen et al., 1993). Depressed mood and depressive symptoms have been found to explain over two-thirds of the variance in adolescent well-being (Mahon & Yarcheski, 2001). These and other findings (e.g. Harrington, 1998) indicate that even relatively mild depressive symptoms can result in impaired functioning. Therefore, those with sub-clinical depressive symptoms during adolescence need to be considered at increased risk for negative outcomes.
The developmental importance of peer relations places a premium on understanding their influence on the etiology and psychopathology of health behavior. The study of physical and mental well-being must include consideration of the importance of context, and during adolescence the context is inherently social. Peer relationships among adolescents are commonly organized hierarchically. The daily social world of youth often carries a specific social order with rewards and penalties depending on the skill with which an adolescent navigates this environment. The peer status of youth has been linked to mental health and negative health behaviors into young adulthood (Michell & Amos, 1997; Ostberg, 2002; Roff & Wirth, 1984). Both friendship ties and the overall structure of the social network, in addition to individual social status, have been found to influence adolescent health (Ueno, 2005; Kiesner, 2002). This suggests that the organization, structure, and distribution of social status among peer groups can influence adolescent development.
The results show that social network centrality and social network status are significantly associated with both depressive symptoms and depression for the total sample of Chinese adolescents, but it was clear when examining the models by the different subgroups that there are noticeable differences in magnitude and meaningfulness for these groups. Chinese youth experience unique social environments that, in some regards, are quite different from Western youth. As much of the previous work on the effects of social status on depression outcomes has been conducted with Western cultures, this study adds to the work by examining these hypotheses in a collectivist, Eastern culture. The meaning and influence social interactions have for Chinese adolescents may affect their association with depressive symptoms. This is a promising avenue for future work, as the impact of rapid social and cultural changes in China is still unclear and rates of psychological distress and outcomes, such as depression and suicidal behavior is on the rise (Daly, 2009).
Prevention work with youth often takes a “social influences” approach. The findings from this study suggest that a social network perspective could help to increase the effectiveness of programs aimed at preventing adolescent depression-related outcomes. Lower social network status is associated with increased risk, so increasing social integration within a classroom, particularly for those on the fringes of the network may help to decrease depression. Creating a social environment that values acceptance and inclusion could go a long way in decreasing the depressive symptoms of an adolescent at risk. The findings can also help to identify those at the highest risk, who could benefit from more intensive or targeted intervention.
Many factors have been found to increase vulnerability to depression for adolescents and many of the problem behaviors that prevention research has targeted have been linked to depression as well. While depression is generally conceptualized as an individual disorder with a strong focus on problematic thoughts and perceptions, maladaptive interpersonal functioning also contributes to its development and progression. Preventing distress and dysfunction in the social networks of youth at risk for depression, as well as improving interpersonal competencies, should be a key aim of future prevention work focusing on this developmental period.
This paper illustrates the contribution that social network analysis can provide to studies examining human development. Some of the earliest antecedents of social network analysis were studies conducted by researchers interested in developmental issues (see Bott, 1928; Hagman, 1933; Wellman, 1926), so a rich history links these two fields. The evolution of social network analysis again provides developmental studies with a useful methodology that allows for a more detailed study of social processes that goes beyond the “self” perspective. The social environment remains important throughout the life course, yet differs and changes across developmental periods; social network analysis is a practical and informative methodology that is uniquely equipped to examine the impact of this environment on human development.
Acknowledgments
We would also like to acknowledge the hard work of the Chengdu Municipal CDC. This study was approved by both the institutional review boards of the University of Southern California and the Chengdu Municipal Center for Disease Control and Prevention. Finally, we would like to express thanks to the municipal government, Health Bureau, and Education Committee in Chengdu, China for their support.
This work was supported by Transdisciplinary Tobacco Use Research Center funding (grant number 1 P50 CA84735-01) from the National Cancer Institute (NCI), National Institute on Drug Abuse (NIDA), and National Institute on Alcohol Abuse and Alcoholism (NIAAA).
Contributor Information
Janet Okamoto, National Cancer Institute.
C. Anderson Johnson, Claremont Graduate University.
Adam Leventhal, University of Southern California.
Joel Milam, University of Southern California.
Mary Ann Pentz, University of Southern California.
David Schwartz, University of Southern California.
Thomas W. Valente, University of Southern California
References
- Alexander C, Piazza M, Mekos D, Valente TW. Peer networks and adolescent cigarette smoking: An analysis of the national longitudinal study of adolescent health. Journal of Adolescent Health. 2001;29:22–30. doi: 10.1016/s1054-139x(01)00210-5. [DOI] [PubMed] [Google Scholar]
- Almquist Y. Peer status in school and adult disease risk: a 30-year follow-up study of disease-specific morbidity in a Stockholm cohort. Journal of Epidemiology and Community Health. 2009;63:1028–1034. doi: 10.1136/jech.2009.088377. [DOI] [PubMed] [Google Scholar]
- Bandura A. Social cognitive theory. In: Vasta R, editor. Annals of child development: Six theories of child development-Revised formulations and current issues. Vol. 6. Greenwich, CT: JAI Press; 1989. pp. 1–60. [Google Scholar]
- Baumeister RF, Leary MR. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin. 1995;117:497–529. [PubMed] [Google Scholar]
- Berkman LF. The role of social relations in health promotion. Psychosomatic Medicine. 1995;57:245–254. doi: 10.1097/00006842-199505000-00006. [DOI] [PubMed] [Google Scholar]
- Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Social Science & Medicine. 2000;51:843–857. doi: 10.1016/s0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- Berndt TJ. Friendship quality and social development. Current Directions in Psychological Science. 2002;11:7–10. [Google Scholar]
- Bonacich P. Power and centrality: A family of measures. American Journal of Sociology. 1987;92(5):1170–1182. [Google Scholar]
- Borgatti SP, Carley KM, Krackhardt D. On the robustness of centrality measures under conditions of imperfect data. Social Networks. 2006;28(2):124–136. [Google Scholar]
- Borgatti SP, Everett MG, Freeman LC. UCINET 6.0 Version 6.232. Natick: Analytic Technologies; 2006. [Google Scholar]
- Bott H. Observation of play activities in a nursery school. Genetic Psychology Monographs. 1928;4:44–88. [Google Scholar]
- Bowlby J. Maternal Care and Mental Health. New York: Schocken; 1951. [PMC free article] [PubMed] [Google Scholar]
- Bowlby J. International psychoanalytical library, no 109. Vol. 3. London: Hogarth Press; 1980. Loss: Sadness & Depression. Attachment and Loss. [Google Scholar]
- Bowlby J. Tavistock professional book. London: Routledge; 1988. A Secure Base: Parent-Child Attachment and Healthy Human Development. [Google Scholar]
- Brendgen M, Vitaro F, Bukowski WM. Deviant friends and early adolescents’ emotional and behavioral adjustment. Journal of Research on Adolescence. 2000;10(2):173–189. [Google Scholar]
- Bronfenbrenner U. The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Bronfenbrenner U. Environments in developmental perspective: Theoretical and operational models. In: Friedman SL, Wachs TD, editors. Measuring environment across the life span: Emerging methods and concepts. Washington, DC: American Psychological Association; 1999. pp. 3–29. [Google Scholar]
- Brooks-Gunn J, Petersen AC. Studying the emergence of depression and depressive symptoms during adolescence. Journal of Youth and Adolescence. 1991;20(2):115–119. doi: 10.1007/BF01537603. [DOI] [PubMed] [Google Scholar]
- Caldwell MS, Rudolph KD, Troop-Gordon W, Kim D. Reciprocal influences among relational self views, social disengagement, and peer stress during adolescence. Child Development. 2004;75(4):1140–1154. doi: 10.1111/j.1467-8624.2004.00730.x. [DOI] [PubMed] [Google Scholar]
- Cheung CK, Bagley C. Validating an American scale in Hong Kong: The Center for Epidemiological Studies Depression Scale (CES-D) Journal of Psychology. 1998;132(2):169–186. doi: 10.1080/00223989809599157. [DOI] [PubMed] [Google Scholar]
- Coie JD. Towards a theory of peer rejection. In: Asher SR, Coie JD, editors. Peer rejection in childhood. Cambridge, MA: Cambridge University Press; 1990. pp. 365–401. [Google Scholar]
- Cole DA, Martin JM, Peeke LG, Seroczynski AD, Hoffman K. Are cognitive errors of underestimation predictive or reflective of depressive symptoms in children: A longitudinal study. Journal of Abnormal Psychology. 1998;107:481–496. doi: 10.1037//0021-843x.107.3.481. [DOI] [PubMed] [Google Scholar]
- Daly R. Depression biggest contributor to global disease burden. Psychiatric News. 2009;44(1):7. [Google Scholar]
- Ellen J, Dolcini M, Bir ND, Harper G, Watson S, Valente TW. Social network centrality and sexual activity among a household sample of urban African American adolescents. Connections. 2001;24(2):76–81. [Google Scholar]
- Falci C, McNeely C. Too many friends: Social integration, network cohesion and adolescent depressive symptoms. Social Forces. 2009;87(4):2031–2062. [Google Scholar]
- Fan J, Meng H, Gao X, Lopez FJ, Liu C. Validation of a U.S. adult social self-efficacy inventory in Chinese population. The Counseling Psychologist. 2010;38(4):473–496. [Google Scholar]
- Farmer TW, Rodkin PC. Antisocial and prosocial correlates of classroom social positions: The social network centrality perspective. Social Development. 1996;5:174–188. [Google Scholar]
- Fowler NA, Christakis JH. Dynamic spread of happiness in a large social network: Longitudinal analysis over 20 years in the Framingham Health Study. British Medical Journal. 2008;337:2338–2347. doi: 10.1136/bmj.a2338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbs JP, Martin WT. A theory of status integration and its relationship to suicide. American Sociological Review. 1958;23:14–147. [Google Scholar]
- Goodman E. The role of socioeconomic status gradients in explaining differences in US adolescents’ health. American Journal of Public Health. 1999;89(10):1522–1528. doi: 10.2105/ajph.89.10.1522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gotlib IH, Lewinsohn PM, Seeley JR. Symptoms versus a diagnosis of depression: Differences in psychosocial functioning. Journal of consulting and clinical psychology. 1995;63(1):90–100. doi: 10.1037//0022-006x.63.1.90. [DOI] [PubMed] [Google Scholar]
- Hagman EP. The companionships of preschool children. University of Iowa Studies in Child Welfare. 1933;7:10–69. [Google Scholar]
- Harrington NR. Bipolar versus unipolar mood disorders: The role of cognitive processes and life stress in differential diagnosis, symptom changes, family history, and comorbidity. Dissertation Abstracts International: Section B: The Sciences and Engineering. 1998;59(3-B):1367. [Google Scholar]
- Hartup WW. The company they keep: Friendships and their developmental significance. Child Development. 1996;67:1–13. [PubMed] [Google Scholar]
- Hartup WW, Stevens N. Friendship and adaptation in the life course. Psychological Bulletin. 1997;121:355–370. [Google Scholar]
- House JS, Landis KR, Umberton D. Social relationships and health. Science. 1988;24(4865):540–545. doi: 10.1126/science.3399889. [DOI] [PubMed] [Google Scholar]
- Inkeles A. Personality and Social Structure. In: Merton RK, Broom L, Cottrell LS, editors. Sociological Today. New York: Basic Books; 1959. pp. 249–76. [Google Scholar]
- Jacobs RH, Reinecke MA, Gollan JK, Kane P. Empirical evidence of cognitive vulnerability for depression among children and adolescents: A cognitive science and developmental perspective. Clinical Psychology Review. 2008;28(5):759–782. doi: 10.1016/j.cpr.2007.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiesner J. Depressive symptoms in early adolescence: Their relations with classroom problem behavior and peer status. Journal of Research on Adolescence. 2002;12:463–478. [Google Scholar]
- Krackhardt D. The strength of strong ties. In: Nohria N, Eccles RG, editors. Networks and organizations: Structure, form and action. Boston: Harvard Business School Press; 1992. pp. 216–239. [Google Scholar]
- Lam CK, Lim PPJ, Low BL, Ng LL, Chiam PC, Sahadevan S. Depression in dementia: A comparative and validation study of four brief scales in the elderly Chinese. International Journal of Geriatric Psychiatry. 2004;19(5):422–428. doi: 10.1002/gps.1098. [DOI] [PubMed] [Google Scholar]
- Lin HC, Tang TC, Yen JY, Ko CH, Huang CF, Liu SC, Yen CF. Depression and its association with self-esteem, family, peer, and school factors in a population of 9586 adolescents in southern Taiwan. Psychiatry and Clinical Neuroscience. 2008;62:412–420. doi: 10.1111/j.1440-1819.2008.01820.x. [DOI] [PubMed] [Google Scholar]
- Luke DA, Harris JK. Network analysis in public health: history, methods, and applications. Annual Review of Public Health. 2007;28:69–93. doi: 10.1146/annurev.publhealth.28.021406.144132. [DOI] [PubMed] [Google Scholar]
- Mahon NE, Yarcheski A. Outcomes of depression in early adolescents. Western Journal of Nursing Research. 2001;23(4):360–375. doi: 10.1177/01939450122045212. [DOI] [PubMed] [Google Scholar]
- Michell L, Amos A. Girls, pecking order and smoking. Social Science and Medicine. 1997;44:1861–1869. doi: 10.1016/s0277-9536(96)00295-x. [DOI] [PubMed] [Google Scholar]
- Ostberg V. Children in classrooms: Peer status, status distribution, and mental well-being. Social Science & Medicine. 2003;56:17–29. doi: 10.1016/s0277-9536(02)00006-0. [DOI] [PubMed] [Google Scholar]
- Ostberg V, Modin B. Status relations in school and their relevance for health in a life course perspective: Findings from the Aberdeen children of the 1950s cohort study. Social Science & Medicine. 2008;66:835–848. doi: 10.1016/j.socscimed.2007.10.018. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Compas BE, Brooks-Gunn J, Stemmler M, Ey S, Grant KE. Depression in adolescence. American Psychologist. 1993;48(2):155–168. doi: 10.1037//0003-066x.48.2.155. [DOI] [PubMed] [Google Scholar]
- Radloff L. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Reinherz HZ, Giaconia RM, Pakiz B, Silverman AB, Frost AK, Lefkowitz ES. Psychosocial risk for major depression in late adolescence: A longitudinal community study. Journal of the American Academy of Child & Adolescent Psychiatry. 1993;32(6):1155–1163. doi: 10.1097/00004583-199311000-00007. [DOI] [PubMed] [Google Scholar]
- Roberts RE, Lewinsohn PM, Seeley JR. Screening for adolescent depression: A comparison of depression scales. Journal of the American Academy of Child & Adolescent Psychiatry. 1991;30(1):58–66. doi: 10.1097/00004583-199101000-00009. [DOI] [PubMed] [Google Scholar]
- Roberts RE, Roberts CR, Chen YR. Ethnocultural differences in prevalence of adolescent depression. American Journal of Community Psychology. 1997;25(1):95–110. doi: 10.1023/a:1024649925737. [DOI] [PubMed] [Google Scholar]
- Roff D, Wirth RD. Childhood social adjustment, adolescent status, and young adult mental health. American Journal of Orthopsychiatry. 1984;54:595–602. doi: 10.1111/j.1939-0025.1984.tb01529.x. [DOI] [PubMed] [Google Scholar]
- Rose A, Rudolph KD. A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin. 2006;132:98–131. doi: 10.1037/0033-2909.132.1.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal R, Rosnow RL, Rubin DB. Contrasts and effect sizes in behavioral research: A correlational approach. Cambridge University Press; 2000. [Google Scholar]
- Seeman TE. Social ties and health: The benefits of social integration. Annals of Epidemiology. 1996;6:442–451. doi: 10.1016/s1047-2797(96)00095-6. [DOI] [PubMed] [Google Scholar]
- Smith HM, Betz NE. Development and validation of a scale of perceived social self-efficacy. Journal of Career Assessment. 2000;8:283–301. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 11. College Station, TX: StataCorp LP; 2009. [Google Scholar]
- Strauss RS, Pollack HA. Social marginalization of overweight children. Archives of Pediatrics and Adolescent Medicine. 2003;157:746–752. doi: 10.1001/archpedi.157.8.746. [DOI] [PubMed] [Google Scholar]
- Ueno K. The effects of friendship networks on adolescent depressive symptoms. Social Science Research. 2005;34:484–510. [Google Scholar]
- Valente TW, Unger JB, Johnson CA. Do popular students smoke? The association between popularity and smoking among middle school students. Journal of Adolescent Health. 2005;37(4):323–329. doi: 10.1016/j.jadohealth.2004.10.016. [DOI] [PubMed] [Google Scholar]
- Valente TW. Social networks and health: Models, methods, and applications. New York: Oxford University Press; 2010. [Google Scholar]
- Wellman B. The school child’s choice of companions. Journal of Educational Research. 1926;14:126–132. [Google Scholar]
- Xie H, Cairns RB, Cairns BD. The development of social aggression and physical aggression: A narrative analysis of interpersonal conflicts. Aggressive Behavior. 2002;28:341–355. [Google Scholar]
- Yang HJ, Soong WT, Kuo PH, Chang HL, Chen WJ. Using the CES-D in a two-phase survey for depressive disorders among non referred adolescents in Taipei: A stratum-specific likelihood ratio analysis. Journal of Affective Disorders. 2004;82:419–430. doi: 10.1016/j.jad.2004.04.008. [DOI] [PubMed] [Google Scholar]