

Abstract
Background:
To formulate all intervention strategies for hypertension in the community, it is essential to quantify the magnitude of the disease and its risk factors. The patterns of physical activity have not been studied in terms of their being a risk factor or a predictor of hypertension in Saudi Arabia.
Materials and Methods:
This was a community-based cross-sectional study using the STEP-wise approach of adults and a multistage, stratified, cluster random sample. Data were collected using a questionnaire which included sociodemographics, blood pressure, patterns, levels and duration of physical activity.
Results:
Of a total of 4758, 1213 (25.5%) were hypertensives. Hypertension was significantly negatively associated with total levels and duration of physical activity in leisure, transport, and work. Significant predictors of hypertension included lower levels of work involving a moderate physical activity for 10 min, walking/cycling for 10 min continuously, and vigorous activity during leisure time.
Conclusions:
Hypertension is prevalent among adults; physical inactivity is a significant risk factor and predictor. Targeting this modifiable risk factor can help in prevention, early diagnosis, and control.
Keywords: Adults, hypertension, physical activity, Saudi Arabia
INTRODUCTION
Epidemiological studies have indicated that physical inactivity is associated with a variety of noncommunicable diseases (NCDs), and overall 1.9 million deaths are attributable to physical inactivity.[1,2] Hypertension is one of the most common NCDs affecting a quarter to about half of the adult population in many countries including Kingdom of Saudi Arabia (KSA).[3–6] It is a complex disorder with many genetic and environmental causes. Poor lifestyle such as physical inactivity is one of the risk factors predisposing to its occurrence and complications. It is claimed that virtually all individuals (hypertensives and normotensives) can benefit from regular physical activity, whether it is vigorous exercise or some moderate health-enhancing physical activity.[7] Prospective cohort studies have generally demonstrated that physical activity or physical fitness is associated with a reduced risk of hypertension.[8–10] All blood pressure measurements were greater in the least physically active persons including prepubertal children.[11–13] In KSA, as in other Gulf countries, a dramatic rise in the standard of living, increased mechanization, and the use of computer and telecommunication technology have resulted in low levels of physical activity and sedentary living.[14–18] The current levels of physical inactivity are also partly due to little participation in physical activity during leisure time and an increase in sedentary behavior in work-related and domestic activities. Likewise, an increase in the use of “passive” modes of transport has also been associated with the declining level of physical activity.[15,16] Increased urbanization resulting in several environmental factors such as violence, heavy traffic, pollution, and absence of parks, sidewalks, and sports and recreational facilities discourage participation in physical activity. These changes may have contributed to the high prevalence of many chronic NCDs such as hypertension. Previous studies in KSA[3,4] have reported the association of hypertension with physical inactivity in general, but the studies did not discuss the association of hypertension with the levels, patterns, or duration of physical activity. This study aims to compare patterns of physical activity of normotensive and hypertensive adults and identify significant risk factors of physical activity and predictors of hypertension. To the best of our knowledge, this is the first study of its kind and scope in KSA. It is hoped that the results will be beneficial in designing programs for the prevention and control of hypertension.
MATERIALS AND METHODS
This is a cross-sectional community-based study done in 2005 covering the entire Kingdom of Saudi Arabia. The WHO STEPwise approach to Surveillance (STEPS) of NCD risk factors was the basis for the conduct of the survey and for the collection of data.[19]
Study population and sampling
A multistage stratified cluster random sampling technique was used to recruit a representative sample of the total population, aged 15–64 years, in Saudi Arabia. Stratification was based on age (five 10-year-old groups) and gender (male/female, two groups). All health regions of the country (20 regions) were covered. Based upon the proposed methodology of the WHO STEPwise approach, a sample size of 196 was calculated for each of these 10 strata. A list of all primary health care centers (PHCCs) in each region was prepared and 10% of these PHCCs were randomly chosen, and allocated a regional sample that was proportionate to the size of their catchment population in the sampled PHCCs. To identify the households, a map of the health center coverage area was used. Each house was assigned a number and a simple random draw was made.
Data collection
Data were collected using the WHO STEP wise approach which includes a questionnaire, physical measurements plus biochemical measurements including hypertension, other chronic diseases, and risk factors in addition to the pattern, intensity, and duration of physical activity. The questionnaire was translated into Arabic by a team of physicians and translated back to ensure accuracy of translation. The Arabic instrument was pretested and corrected before being tried on 51 eligible respondents to check the accuracy of the wording and comprehension of the questions. All required adjustments were then made in the instrument in the light of the pretest.
Data collectors
Data were collected by 54 males and 54 females working in teams of four persons each: a male data collector, a female data collector, a driver, and a female assistant. Data collection teams were supervised by a hierarchy of a local supervisor, regional coordinators, and a national coordinator.
Training of data collectors
All persons involved in data collection attended a comprehensive training workshop which explained the interview techniques, data collection tools, practical applications, and field guidelines.
Blood pressure measurement
The measurements were taken using a digital sphygmomanometer. Before taking the measurements, the respondent was advised to sit quietly and rest for 5 min with the legs uncrossed and the right arm free of any clothing. Then, the right arm was placed on the table with the palm facing upward. The appropriate cuff size was selected. The artery position mark (ART) was aligned with the brachial artery. The cuff was wrapped snugly around the arm and fastened securely. The cuff was kept at the level of the heart during measurement. Taking of measurements involved the following: pushing the START button automatically inflated the cuff and displayed and recorded systolic blood pressure (SBP) and diastolic blood pressure (DBP) readings. A second reading was taken 5 min after the first and a third 5 min later.
Definition of hypertension
The subject was labeled hypertensive if the average of the three blood pressure measurements was 140 mmHg or above for systolic and/or 90 mmHg or above for diastolic blood pressure, or the subject was a known hypertensive previously diagnosed by a health professional.
Physical activity measure
The physical activity measure used was the Global Physical Activity Questionnaire (GPAQ)[20] which comprised 19 questions about physical activity performed in a typical or normal week. The GPAQ measure asked about the frequency (days) and the time (minutes/hours) spent doing moderate to vigorously intense physical activity in three domains: (i) work-related physical activity (paid and unpaid, including household chores); (ii) active commuting (walking and cycling); and (iii) discretionary leisure time (recreation) physical activity. GPAQ is an instrument derived from the long and short forms of the International Physical Activity Questionnaire (IPAQ) which has been validated and widely used to assess physical activity patterns.[21] The test retest reliability of GPAQ (short-term assessment in a 3- to 7-day interval) produced good-to-excellent results (r = 0.67–0.81) and the concurrent validity against IPAQ for total physical activity yielded a moderate-to-good correlation (r = 0.54); questions on sedentary activity generated a good correlation (r = 0.65).[22]
Data management
Questionnaires collected from the field were reviewed by team leaders of each team before submission to the headquarters for data entry. Double entry of the questionnaires was performed using EPI-INFO 2000 software and EpiData software.[23] After data entry, data cleaning was conducted. New variables were defined by adopting the standard STEPS variables (STEPS Data Management Manual, draft version v1.5, October 2003).
Statistical analysis
Descriptive statistics, t-test, Mann–Whitney test were used as appropriate after checking for normality. The level of significance was set at < 0.05 throughout the study. The data were processed in SPSS, version 17.
Ethical clearance and confidentiality
The protocol and the instrument of the surveillance were approved by the Ministry of Health, Center of Biomedical Ethics, and the concerned authorities in KSA. Informed consent was obtained from all subjects. Confidentiality of data was assured indicating that data would only be used for the stated purpose of the survey.
RESULTS
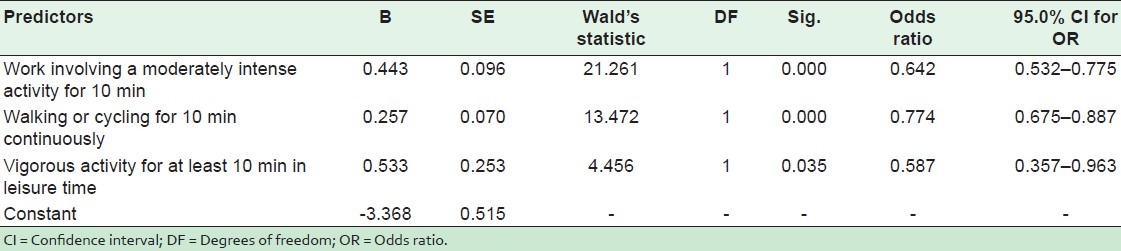
Of the total 4758 subjects who participated in the study, about 51% were females. A total of 1213 were hypertensives giving a prevalence of 25.5% (27.1% males and 23.9% females). Of the subjects, only 12.1%, 20.2%, and 46.1% were physically active in recreational, work- and transport-related activities, respectively. Physical inactivity in general was significantly associated with females, the elderly, retired, and persons living in the central region. Pearson's correlation coefficient was calculated for systolic and diastolic blood pressures separately and the total duration of physical activity in minutes per day for all subjects (hypertensives and normotensives). There was a significant negative correlation indicating that as the total duration of physical activity increased , both systolic and diastolic pressures decreased (r = -0.048, P = 0.001, for systolic pressure; r = -0.037, P = 0.013, for diastolic blood pressure). Hypertension was significantly negatively associated with the total level of physical activity as shown in Table 1. In Table 2, the comparison between physical activity patterns in hypertensive and normotensive subjects using odds ratios and 95% confidence intervals. All lower levels of physical activity in leisure, transport, and work were significantly associated with an increased risk of hypertension. Table 3 compares the mean duration of the different patterns of the physical activity of the hypertensives and normotensives. The table shows that for hypertensives durations of all patterns of physical activity were significantly shorter. Table 4 shows multiple logistic regression analysis for significant predictors of hypertension. All significant risk factors in Tables 2 and 3 were included in the logistic regression model. Three lower physical activity patterns were significant predictors of hypertension. These were: work involving moderate physical activity for 10 min, walking/cycling for 10 min continuously, and vigorous activity in leisure time.
Table 1.
Overall level of physical activity among hypertensives and nonhypertensives

Table 2.
Association of physical activity patterns and hypertension status
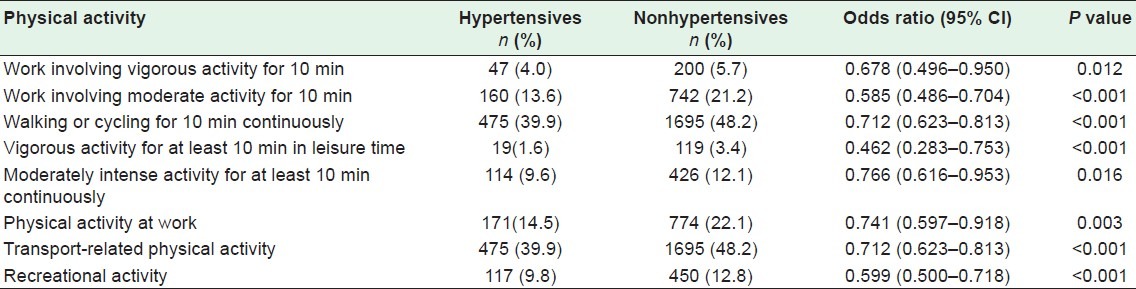
Table 3.
Duration of physical activity patterns and blood pressure status

Table 4.
Logistic regression model to predict hypertension from some physical activity patterns and levels after adjusting for age
DISCUSSION
The level of physical inactivity in KSA is a worrying condition. This study as well as previous studies has shown that physical inactivity in KSA was high indicating the sedentary nature of the Saudi population.[3,4,14–17] The overwhelming majority of men and women did not reach the recommended physical activity levels required for the promotion of health and the prevention of disease.[15] The knowledge of students in KSA of the role of physical activity in the prevention of hypertension is rather weak.[24] Consequently, it is not surprising that the study revealed that hypertension affected more than a quarter of the population, physical inactivity being a significant contributor. Significant risk factors for hypertension included low levels of physical activity for all patterns of activities (leisure-, work-, and transport-related and recreational activities). Three patterns of physical activity were significant predictors of hypertension. These were work related involving a moderate physical activity for 10 min, walking/cycling for 10 min continuously, and vigorous activity in leisure time. Physical inactivity was significantly negatively correlated with both systolic and diastolic blood pressures in this study, and in previous studies in KSA .Total physical inactivity was significantly associated with hypertension.[3,4] These findings are in agreement with findings of many studies worldwide. Studies have reported that both fitness and activity were inversely associated with the development of hypertension[9,10] and that physical activity of a moderate intensity lowered systolic and diastolic pressures in both normotensive and hypertensive subjects by 2–7 mmHg.[8] Walking during leisure or working in many communities was associated with the decreased prevalence of hypertension.[25,26] Physical inactivity was definitely and strongly associated with hypertension in this and other studies, but the pattern of the levels and intensity of physical activity were not consistent. Meta-analyses of randomized control trials assessing the effectiveness of exercise training in lowering blood pressure revealed significant heterogeneity, reflecting the varied subject demography and exercise schedules used in different studies.[27,28] The available data suggest that aerobic exercise of a moderate intensity is associated with a significant reduction in blood pressure in hypertensive and normotensive participants and in overweight as well as normal weight participants.[28] Increasing the exercise intensity above recommended levels did not have any additional impact on the reduction of blood pressure.[29] Even though it is well established that moderate exercise lowers blood pressure in most hypertensives, in some studies about a quarter did not respond to exercise training.[30]
This study detailed the association of physical activity and hypertension in terms of intensity, duration, and patterns. The most important point is that all persons should be physically active. Although the mechanism of how physical activity reduces the risk of hypertension remains unclear, the finding that an increase in activities in daily life is associated with a lower risk of hypertension as reported in this study, and others should encourage all of us to advocate physical activity in all age groups. Aerobic activity is the preferred type of activity as a means of lowering blood pressure,[31] but all other patterns are useful. As found in a recent study in KSA,[32] the enhanced quality and a broadened scope of health education if given to patients who go to easily accessible PHCCs all over the country would improve the awareness and practice of healthy behaviors such as the inclination to become more physically active.
CONCLUSIONS
Regular physical activity, fitness, and exercise are critically important for the health and well being of people of all ages. This study and others have demonstrated that virtually all individuals (hypertensives and normotensives) can benefit from regular health-enhancing physical activity. Specifically tailored and culturally sensitive interventions including physical activity that address multiple health behaviors are necessary for the prevention, and control of hypertension and other chronic morbidities. Special attention should be given to females, the elderly, and retired persons.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Waxman A. WHO's global strategy on diet, physical activity and health. Scand J Nutrition. 2004;48:58–60. doi: 10.1177/156482650402500310. [DOI] [PubMed] [Google Scholar]
- 2.Geneva: World Health Organization; 2002. World Health Organization. The world health report 2002 Reducing risks, promoting healthy life. [Google Scholar]
- 3.Al-Hamdan N, Saeed A, Kutbi A, Choudhry AJ, Nooh R. Characteristics, Risk Factors, and Treatment Practices of Known Adult Hypertensive Patients in Saudi Arabia. Int J Hypertens. 2011;2010:168739. doi: 10.4061/2010/168739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou YY, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28:77–84. [PubMed] [Google Scholar]
- 5.Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: Analysis of worldwide data. Lancet. 2005;365:217–23. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- 6.Perkovic V, Huxley R, Wu Y, Prabhakaran D, MacMahon S. The burden of blood pressure-related disease: A neglected priority for global health. Hypertension. 2007;50:991–7. doi: 10.1161/HYPERTENSIONAHA.107.095497. [DOI] [PubMed] [Google Scholar]
- 7.Carnethon MR, Evans NS, Church TS, Lewis CE, Schreiner PJ, Jacobs DR, Jr, et al. Joint associations of physical activity and aerobic fitness on the development of incident hypertension: Coronary artery risk development in young adults. Hypertension. 2010;56:49–55. doi: 10.1161/HYPERTENSIONAHA.109.147603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fagard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Med Sci Sports Exerc. 2001;33(6 Suppl):S484–92. doi: 10.1097/00005768-200106001-00018. discussion S93-4. [DOI] [PubMed] [Google Scholar]
- 9.Hu G, Barengo NC, Tuomilehto J, Lakka TA, Nissinen A, Jousilahti P. Relationship of physical activity and body mass index to the risk of hypertension: A prospective study in Finland. Hypertension. 2004;43:25–30. doi: 10.1161/01.HYP.0000107400.72456.19. [DOI] [PubMed] [Google Scholar]
- 10.Nakanishi N, Suzuki K. Daily life activity and the risk of developing hypertension in middle-aged Japanese men. Arch Intern Med. 2005;165:214–20. doi: 10.1001/archinte.165.2.214. [DOI] [PubMed] [Google Scholar]
- 11.Alomari MA, Keewan EF, Qhatan R, Amer A, Khabour OF, Maayah MF, et al. Blood pressure and circulatory relationships with physical activity level in young normotensive individuals: IPAQ validity and reliability considerations. Clin Exp Hypertens. 2011;33:345–53. doi: 10.3109/10641963.2010.531848. [DOI] [PubMed] [Google Scholar]
- 12.Parker ED, Schmitz KH, Jacobs DR, Jr, Dengel DR, Schreiner PJ. Physical activity in young adults and incident hypertension over 15 years of follow-up: The CARDIA study. Am J Public Health. 2007;97:703–9. doi: 10.2105/AJPH.2004.055889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gopinath B, Hardy LL, Teber E, Mitchell P. Association between physical activity and blood pressure in prepubertal children. Hypertens Res. 2011;34:851–5. doi: 10.1038/hr.2011.46. [DOI] [PubMed] [Google Scholar]
- 14.Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: A brief review. East Mediterr Health J. 2004;10:663–70. [PubMed] [Google Scholar]
- 15.Al-Nozha MM, Al-Hazzaa HM, Arafah MR, Al-Khadra A, Al-Mazrou YY, Al-Maatouq MA, et al. Prevalence of physical activity and inactivity among Saudis aged 30-70 years. A population-based cross-sectional study. Saudi Med J. 2007;28:559–68. [PubMed] [Google Scholar]
- 16.Al-Refaee SA, Al-Hazzaa HM. Physical activity profile of adult males in Riyadh City. Saudi Med J. 2001;22:784–9. [PubMed] [Google Scholar]
- 17.Midhet F, Al Mohaimeed AR, Sharaf F. Dietary practices, physical activity and health education in qassim region of saudi arabia. Int J Health Sci (Qassim) 2010;4:3–10. [PMC free article] [PubMed] [Google Scholar]
- 18.Ramadan J, Vuori I, Lankenau B, Schmid T, Pratt M. Developing a national physical activity plan: The Kuwait example. Glob Health Promot. 2010;17:52–7. doi: 10.1177/1757975910365230. [DOI] [PubMed] [Google Scholar]
- 19.World Health Organization. STEPwise approach to chronic disease risk factor surveillance (STEPS) 2011. [Last accessed on 2011 Sep 15]. [Last cited on 2011 Nov 30]; Available from: http://www.who.int/chp/steps/riskfactor/en/index.html .
- 20.World Health Organization. GPAQ Global Physical Activity Questionnaire. 2011. [Last accessed on 2011 Sep 15]. [Last cited on 2011 May 15]; Available from: http://www.who.int/chp/steps/resources/GPAQ_Analysis_Guide.pdf .
- 21.The IPAQ group. IPAQ International Physical Activity Questionnaire. [Last accessed on 2011 Sep 15]. [Last cited on 2011 May 15]; Available from: http://www.ipaq.ki.se/
- 22.Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ) J Public Health. 2006;14:66–70. [Google Scholar]
- 23.Lauritsen J, Bruus M. Odense Denmark: The EpiData Association; 2000-2008. EpiData Entry. A comprehensive tool for validated entry and documentation of data. [Google Scholar]
- 24.Taha AZ. Self-reported knowledge and pattern of physical activity among school students in Al Khobar, Saudi Arabia. East Mediterr Health J. 2008;14:344–55. [PubMed] [Google Scholar]
- 25.Hayashi T, Tsumura K, Suematsu C, Okada K, Fujii S, Endo G. Walking to work and the risk for hypertension in men: The Osaka Health Survey. Ann Intern Med. 1999;131:21–6. doi: 10.7326/0003-4819-131-1-199907060-00005. [DOI] [PubMed] [Google Scholar]
- 26.Hu G, Jousilahti P, Antikainen R, Tuomilehto J. Occupational, commuting, and leisure-time physical activity in relation to cardiovascular mortality among finnish subjects with hypertension. Am J Hypertens. 2007;20:1242–50. doi: 10.1016/j.amjhyper.2007.07.015. [DOI] [PubMed] [Google Scholar]
- 27.Halbert JA, Silagy CA, Finucane P, Withers RT, Hamdorf PA, Andrews GR. The effectiveness of exercise training in lowering blood pressure: A meta-analysis of randomised controlled trials of 4 weeks or longer. J Hum Hypertens. 1997;11:641–9. doi: 10.1038/sj.jhh.1000509. [DOI] [PubMed] [Google Scholar]
- 28.Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: A meta-analysis of randomized, controlled trials. Ann Intern Med. 2002;136:493–503. doi: 10.7326/0003-4819-136-7-200204020-00006. [DOI] [PubMed] [Google Scholar]
- 29.Choudhury A, Lip GY. Exercise and hypertension. J Hum Hypertens. 2005;19:585–7. doi: 10.1038/sj.jhh.1001851. [DOI] [PubMed] [Google Scholar]
- 30.Hagberg JM, Park JJ, Brown MD. The role of exercise training in the treatment of hypertension: An update. Sports Med. 2000;30:193–206. doi: 10.2165/00007256-200030030-00004. [DOI] [PubMed] [Google Scholar]
- 31.Goodwin KA, Headley SA, Pescatello LS. Exercise Prescription for the Prevention and Management of Hypertension. Am J Lifestyle Med. 2009;3:446–9. [Google Scholar]
- 32.Midhet FM, Sharaf FK. Impact of health education on lifestyles in central Saudi Arabia. Saudi Med J. 2011;32:71–6. [PubMed] [Google Scholar]