

Abstract
Leiomyoma of the lung is extremely rare. The entity is not described in WHO blue book. Less than 100 cases of leiomyoma of the lung have been reported in the literature. However, vascular leiomyoma has not been reported in the literature, to the author’s best knowledge. Herein reported is the first case of vascular leiomyoma of the lung arising from smooth muscles of the pulmonary artery. A 62-year-old woman (non-smoker) was found to have a small tumor in the upper lobe in the right lung in routine check. Imaging modalities including CT demonstrated no metastatic lesions. Although clinical cytology and biopsy revealed no malignant cell, right upper lobectomy was performed under the clinical diagnosis of lung carcinoma. Grossly, a white tumor of 1 x 0.8 cm was recognized in the lung. Microscopically, the tumor was connected to the pulmonary arteries. The tumor was composed of mature smooth muscles. Small pulmonary arteries are embedded in the tumor. No lymphatics were seen. Immunohistochemically, the tumor cells were poisitive for alpha-smooth muscle actin, vimentin and Ki-67 (labeling 2%). However, they were negative for cytokeratin (CK) AE1/3, CK CAM5.2, desmin, S100 protein, p53, CD34, KIT, HMB45, estrogen receptor, progesterone receptor, and myoglobin. A pathological diagnosis of primary vascular leiomyoma arising from the smooth muscle of pulmonary artery was made. The patient is now free from tumor, and is now alive 10 year after the operation.
Keywords: Lung, leiomyoma, pulmonary artery, immunohistochemistry
Introduction
Leiomyoma of the lung is extremely rare. The entity is not described in WHO blue book. Less than 100 cases of leiomyoma of the lung have been reported in the literature [1-5]. However, vascular leiomyoma has not been reported in the literature, to the author’s best knowledge. Herein reported is the first case of vascular leiomyoma of the lung arising from smooth muscles of the pulmonary artery.
Case report
A 62-year-old woman (non-smoker) was found to have a small tumor in the upper lobe in the right lung in routine check. Imaging modalities including CT demonstrated no metastatic lesions. Although clinical cytology and biopsy revealed no malignant cell, right upper lobectomy was performed under the clinical diagnosis of lung carcinoma. Grossly, a white tumor of 1 x 0.8 cm was recognized in the lung (Figure 1). Microscopically, the tumor was connected to the pulmonary arteries (Figure 1 and 2). The tumor was composed of mature smooth muscles (Figure 3). Small pulmonary arteries are embedded in the tumor (Figure 4). No lymphatics were seen. An immunohistochemical study was performed with the use of Dako EnVision method as previously described [6-10]. Immunohistochemically, the tumor cells were positive for alpha-smooth muscle actin (Figure 5), vimentin and Ki-67 (labeling 2%). However, they were negative for cytokeratin (CK) AE1/3, CK CAM5.2, desmin, S100 protein, p53, CD34, KIT, HMB45, estrogen receptor (ER), progesterone receptor (PgR), and myoglobin. A pathological diagnosis of primary vascular leiomyoma arising from the smooth muscle of pulmonary artery was made. The patient is now free from tumor, and is now alive 10 year after the operation.
Figure 1.
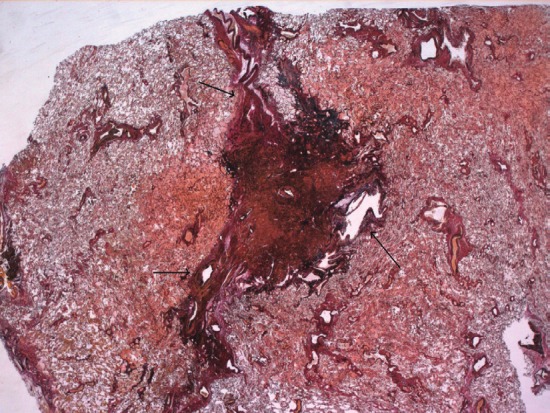
Very low power view. A tumor measuring 1 x 0.8 cm was seen in the right upper lobe. The tumor is continuous to pulmonary arteries (arrows). Small vessels are also seen within the tumor. Elastica Von Gieson, x2.
Figure 2.
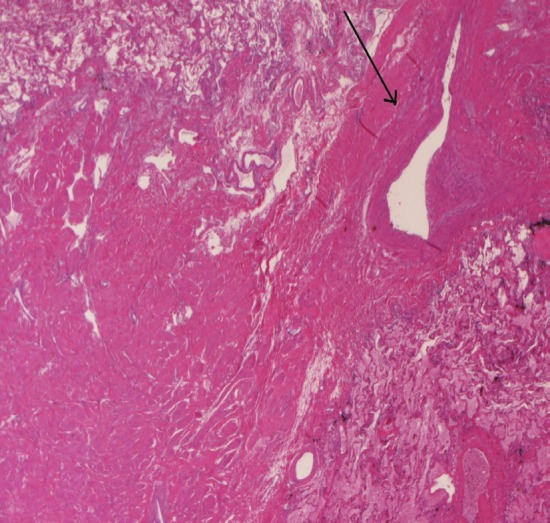
The tumor (center) with continuous to a pulmonary artery (arrow). HE, x20.
Figure 3.
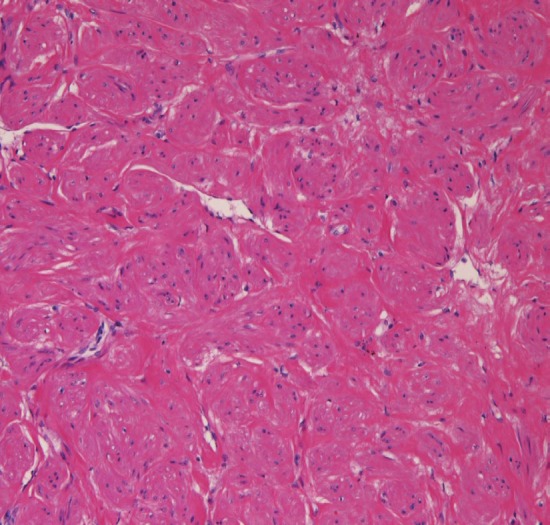
The tumor consists of mature smooth muscle with acidophilic cytoplasm. HE, x200.
Figure 4.
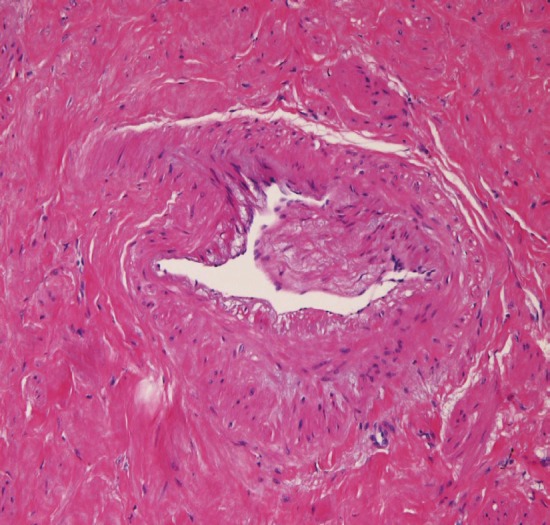
Small pulmonary arteries (center) are scattered within the tumor. HE, x200.
Figure 5.
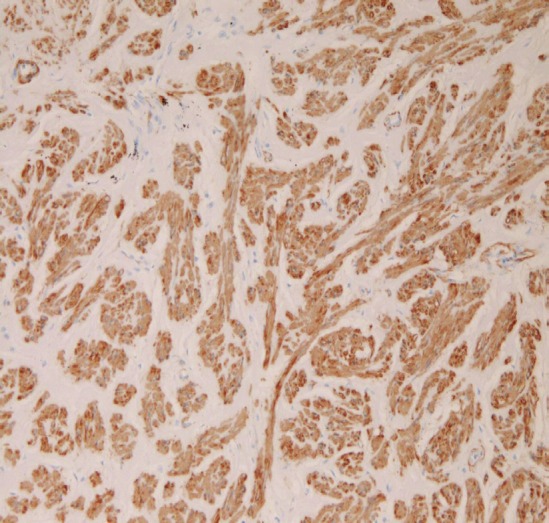
The tumor is positive for alpha-smooth muscle actin. Immunostaining, x200.
Discussion
Smooth muscle tumors of the lung are very rare. Our tumor is apparently vascular leiomyoma arising from the smooth muscles of the pulmonary artery. The current tumor is not epithelial tumor because of negative CK. The present tumor is benign histologically. The negative p53 and very low Ki-67 labeling (2%) exclude malignancy in the current tumor. The current tumor is obviously different from sarcomas of the pulmonary arteries or veins. The present tumor is not benign metastasizing leiomyoma from the uterus because of negative ER and PgR. The current tumor is not lymphangioleiomyomatosis because of the absence of lymphatics and also because of negative S100 and HMB45. The present tumor is not neurogenic tumor because of negative S100 protein. The present tumor is not extra-gastrointestinal stromal tumor (eGIST) because of negative KIT and CD34. The current tumor is not rhabdomyoma because of negative myoglobin. The present tumor is not perivascular epithelioid or myoid cell tumors histologically and because of negative HMB45. The current tumor is apparently different from inflammatory myofibroblastic tumor, because no inflammatory features are present in the present tumor.
Primary leiomyoma of the lung is extremely rare. It affects mainly female and mean age is around 35 years [2]. Symptoms include chest pain, cough, fever, hemoptysis, or asymptomatic. It may be incidentally found at autopsy [1]. The surgical intervention may be necessary in cases of clinically suspected lung cancer. The prognosis and survival is excellent [1-5]. In the present case, the tumor is not an ordinary leiomyoma but a vascular leiomyoma. A PubMed search of vascular leiomyoma or angioleiomyoma of the lung did not revealed vascular leiomyoma of the lung. Thus, this may be the first case of vascular leiomyoma of the lung. In the lung, smooth muscles are present in the pulmonary arteries, pulmonary veins, bronchial arteries, and the bronchial tree. In the present case, the vascular leiomyoma was continuous to smooth muscles of the pulmonary arteries, suggesting that the vascular leiomyoma arose from the smooth muscles of the pulmonary arteries.
In conclusion, the author reported the probable first case of vascular leiomyoma arising from the smooth muscles of the pulmonary arteries.
Conflict of interest statement
The author has no conflict of interest.
References
- 1.Agnos JW, Starkey GW. Primary leiomyosarcoma and leiomyoma of the lung. N Engl J Med. 1958;258:12–17. doi: 10.1056/NEJM195801022580103. [DOI] [PubMed] [Google Scholar]
- 2.Orlowski TM, Stasiak K, Kolodziej J. Leiomyoma of the lung. J Tjrac Cadiovas Surg. 1978;76:257–261. [PubMed] [Google Scholar]
- 3.White SH, Ibrahim NB, Forrester-Wood CP, Jeyasingham K. Leiomyoma of the lower respiratory tract. Thorax. 1985;40:306–311. doi: 10.1136/thx.40.4.306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gal AA, Brooks JS, Pietra GG. Leiomyomatous neoplasms of the lung: a clinical, histologic and immunohistochemical study. Mod Pathol. 1990;2:209–216. [PubMed] [Google Scholar]
- 5.White SH, Ibrahim NB, Forrester-Wood CP, Jeyasingham K. Leiomyoma of the lower respiratory tract. Thorax. 1985;40:306–311. doi: 10.1136/thx.40.4.306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Terada T, Kawaguchi M, Furukawa K, Sekido Y, Osamura Y. Minute mixed ductal-endocrine carcinoma of the pancreas with predominant intraductal growth. Pathol Int. 2002;52:740–746. doi: 10.1046/j.1440-1827.2002.01416.x. [DOI] [PubMed] [Google Scholar]
- 7.Terada T, Kawaguchi M. Primary clear cell adenocarcinoma of the peritoneum. Tohoku J Exp Med. 2005;206:271–275. doi: 10.1620/tjem.206.271. [DOI] [PubMed] [Google Scholar]
- 8.Terada T. Intraductal tubular carcinoma, intestinal type, of the pancreas. Pathol Int. 2009;59:53–58. doi: 10.1111/j.1440-1827.2008.02325.x. [DOI] [PubMed] [Google Scholar]
- 9.Terada T. Ductal adenoma of the breast: Immunohistochemistry of two cases. Pathol Int. 2008;58:801–805. doi: 10.1111/j.1440-1827.2008.02315.x. [DOI] [PubMed] [Google Scholar]
- 10.Terada T, Tanigichi M. Intraductal oncocytic papillary neoplasm of the liver. Pathol Int. 2004;54:116–123. doi: 10.1111/j.1440-1827.2004.01594.x. [DOI] [PubMed] [Google Scholar]