

Summary
Trabeculectomy for treatment of glaucoma associated with Sturge-Weber syndrome has a poor success rate. We report the presence of anomalous vessels over the trabeculectomy bleb in a patient with Sturge-Weber syndrome after trabeculectomy combined with mitomycin.
Case Report
A 54-year-old male with Sturge-Weber syndrome presented with decreased vision and an intraocular pressure (IOP) of 35 mm Hg in his right eye. He was on topical levobunolol, dorzolamide and bimatoprost in his Right eye. His IOP in the left eye was 16 mm Hg without any anti glaucoma therapy. Apart from corkscrew subconjunctival vessels at the limbus, there were no conjunctival angiomatous malformations ( Figure 1). Fundus examination showed evidence of glaucomatous cupping of 0.9 in the right eye and 0.3 in the left eye. A visual field test showed advanced field defects in the right eye and a normal field in left eye.
Figure 1.
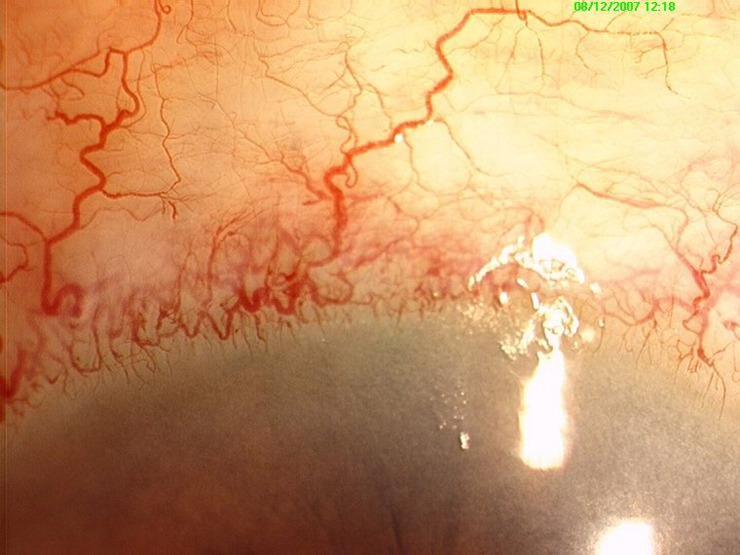
Preoperative photograph of the right eye of the patient with Sturge Weber syndrome showing conjunctival and episcleral vessels.
A standard limbus-based trabeculectomy with subconjunctival application of mitomycin C (0.2 mg/ml for 3 minutes) was performed to control his IOP. At 1 month follow-up, he presented with a well-functioning, diffuse bleb in his right eye. Three months postoperatively IOP in the right eye was 16 mm Hg. Slit-lamp examination revealed a diffuse avascular bleb. At 6 months, the bleb showed abnormal conjunctival vascularization in the form of palisades at the base of the bleb with a leash of anomalous vessels extending from the adjoining area over the anterior superior surface of the bleb. IOP in his right eye was 27 mm Hg. The trabeculectomy ostium was patent on gonioscopic examination. The patient was started on topical levobunolol 0.5% solution twice daily in the right eye for IOP control. At 1 year, the avascular area had decreased, while the conjunctival vascularization showed an increasing palisade of anomalous vessels ( Figure 2); IOP in his right eye was 16 mm Hg with topical levobunolol 0.5%.
Figure 2.
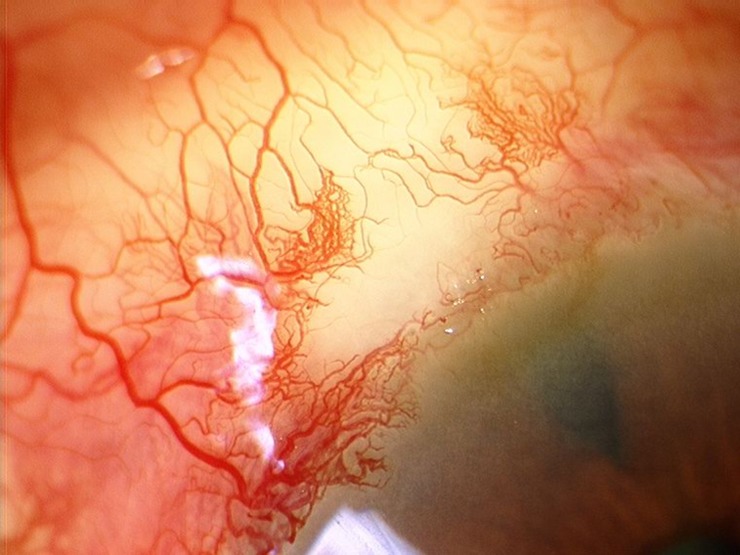
Postoperative photograph at 1 year follow-up showing new palisades of anomalous vessels over the bleb site.
Discussion
Due to the high risk of bleb failure in patients with Sturge-Weber syndrome, modulated trabeculectomy using antimitotic agents has been advocated.1–3 Mitomycin C is known to have a direct toxic effect on the overlying conjunctiva, inhibiting the angiogenic activity of blood vessels and fostering conjunctival avascularity. It also prevents subconjunctival and subscleral fibrosis.
In our patient, intraoperative mitomycin C failed to deter anomalous angiogenesis over the bleb. At 1 year, he presented with progressive growth of the anomalous vessels over an avascular bleb; the characteristic pattern of palisades may resemble a malformation rather than the normal conjunctival vasculature seen on a failing bleb. These palisade of vessels do not represent the typical corkscrew or stretched vessels decribed in failing blebs of non-Sturge-Weber syndrome eyes.4,5 As the trabeculectomy ostium was patent and there was no encapsulation, the presence of these anomalous vessels may have contributed to the bleb failure.
The long-term course of the angiomatosis process in the eye or elsewhere in the body in these cases is not known. In our case, the growth of anomalous vessels over the bleb was noted to progress in the area of involvement, with a gradual decrease in the avascular area of the bleb over a period of 12 months. We are not sure whether the mechanism of anomalous angiogenesis can be attributed to raised episcleral venous pressure or whether the anomalous angiogenesis constitutes a process unrelated to the surgery.
This case highlights the possibility of anomalous vascularization of trabeculectomy blebs in cases of Sturge-Weber syndrome, which may be a cause of trabeculectomy failure even after the use of mitomycin C.
References
- 1.Aggarwal HC, Sandramouli S, Sihota R, Sood NN. Sturge Weber syndrome: Management of glaucoma with combined trabeculotomy-trabeculectomy. Ophthalmic Surg. 1993;24:399–402. [PubMed] [Google Scholar]
- 2.Hamush NG, Coleman AL, Wilson MR. Ahmed Glaucoma valve for management of glaucoma in Sturge Weber syndrome. Am J Ophthalmol. 1999;128:758–60. doi: 10.1016/s0002-9394(99)00259-7. [DOI] [PubMed] [Google Scholar]
- 3.Mandal AK. Primary combined trabeculotomy-trabeculectomy for early onset glaucoma in Sturge Weber syndrome. Ophthalmology. 1999;106:1621–27. doi: 10.1016/S0161-6420(99)90462-1. [DOI] [PubMed] [Google Scholar]
- 4.Picht G, Grehn F. Classification of filtering blebs in trabeculectomy: biomicroscopy and functionality. Curr Opin Ophthalmol. 1998;9(2):2–8. doi: 10.1097/00055735-199804000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Sacu S, Rainer G, Findl O, Georgopoulos M, Vass C. Correlation between the early morphological appearance of filtering blebs and outcome of trabeculectomy with mitomycin C. J Glaucoma. 2003;12:430–5. doi: 10.1097/00061198-200310000-00006. [DOI] [PubMed] [Google Scholar]