

Abstract
A neonate with unilateral complete duplex system with congenital giant megaureter of the upper moiety presenting as abdominal lump is reported. A left upper moiety nephroureterectomy was performed. Such an anomaly with this presentation has not been reported in neonates.
KEY WORDS: Duplex kidney, hydronephrosis, megaureter
INTRODUCTION
Congenital giant megaureter (CGM) comprises an extremely rare subgroup of megaureter. The CGM can be associated with other genitourinary anomalies such as duplex renal systems, megacalicosis, contralateral hydronephrosis, or cryptorchidism.[1] Duplication is one of the common causes of renal asymmetry with an overall incidence of 0.3-0.6%.[1] We report a unique case of unilateral complete duplex system with congenital giant megaureter of the upper moiety in a neonate presenting as abdominal lump.
CASE REPORT
A 20-day-old, full term boy weighing 2.8 kg presented with progressive distension of the abdomen for one week. The antenatal period was unsupervised. The first passage of meconium had been normal. No abnormality was detected on general physical examination. The abdominal examination revealed an ill-defined soft abdominal mass with a smooth surface measuring 15×10 cm. The mass was occupying the left flank and left hypochondrium extending into the left iliac fossa and umbilical regions. The urinalysis, blood urea and serum creatinine were normal. An ultrasound of the abdomen showed a large convoluted anechoic cystic mass filling almost the whole abdomen without clarifying its origin; the cystic mass seemed to fold on itself crossing the midline and extending into the pelvis. The left kidney was not visualized clearly. The right kidney was normal. A contrast-enhanced computed tomography (CECT) scan of abdomen and pelvis [Figure 1] showed a large, non-enhancing, irregular shaped, cystic lesion involving the entire abdomen and pelvis insinuating into and causing compression over adjacent structures. Inferiorly, the lesion was tapering and ending into the lower portion of left side of pelvis. The lesion was seen to be arising from upper portion of the left kidney. There was no renal parenchyma seen in the upper portion of left kidney. A small portion of normal left kidney was seen at the lower pole. Voiding cystourethrogram showed normal bladder and urethra. Nuclear scan facility was not available in our institute.
Figure 1.
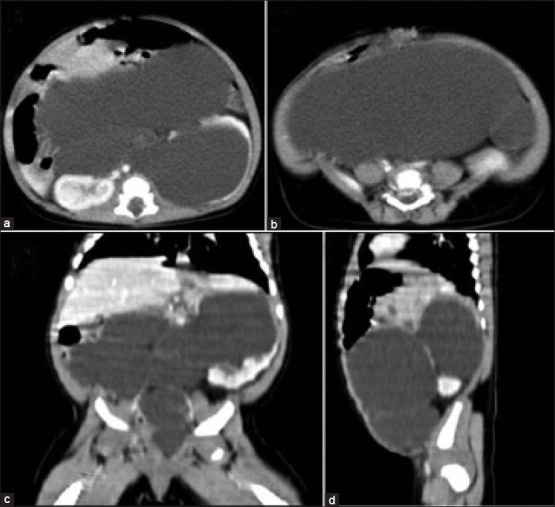
Post-contrast axial images of computed tomography abdomen and pelvis. (a) and (b) show a large cystic mass filling the entire abdomen and pelvis and arising from the left kidney. (c) Reformatted coronal image and (d) sagittal image further confirms the origin of the mass from upper portion of the left kidney. Inferiorly, the mass is tapering and ending into the lower portion of left side of pelvis
On exploration, there was complete duplex system on the left side. The lower moiety had good amount of cortex with normal ureter. The upper moiety had atrophic parenchyma with a huge, dilated and tortuous megaureter (diameter=6 cm; total length=35 cm) till the lower end [Figure 2]. The lower end terminated blindly behind the lower posterior wall of the bladder as a cul-de-sac. A left upper moiety nephroureterectomy was performed. The postoperative period was uneventful. The child was asymptomatic and doing well at nine months follow-up.
Figure 2.

Surgical findings upon laparotomy (a) The dilated left upper moiety ureter occupies almost the whole abdomen, and its dimensions are evidenced by the caliber discrepancy between the ureter and the small bowel. (b) Gross specimen of the giant megaureter and atrophic kidney
DISCUSSION
CGM is an extremely rare condition.[2] This condition is characterized by giant ureteral dilatation producing an elongated and distorted ureter. Distally, there may be a congenital ureteral stenosis or atresia, or a ureter of approximately normal caliber. The associated kidney or moiety may be hypoplastic, dysplastic, or hydronephrotic with associated atrophic renal parenchyma. Usually, the function and volume of the bladder are normal.[3] Congenital segmental giant megaureter (CSGM) is an extremely rare condition, with less than 10 cases reported in the literature. In CSGM, there is primary involvement of a segment of ureter with sparing of the proximal and the distal parts.
A complete duplex system results from an anomalous origin of two ureteric buds or branching of a single ureteral bud developing from a very short common excretory duct. The latter would be absorbed into the bladder early enough to allow separation of the duplicated ureters during their cephalolateral migration in the bladder, resulting in a complete duplication. The pathogenesis of the CGM is unclear. A complete ureteral obstruction may result in renal dysplasia if it develops early in the second trimester, or hydronephrosis with/without atrophic parenchyma if it develops after the kidney has started producing urine.[4] The treatment of choice for a totally dilated ureter corresponding to a poor or non-functioning dysplastic kidney is nephroureterectomy. If there is a segmental cystic dilatation with preserved renal function, excision followed by uretero-ureterostomy can be performed.[5] We performed nephroureterectomy in our patient because of the non-functional upper moiety.
Uson et al.[6] and Lelli-Chiesa et al.[7] reported a case of a giant ureter presenting as an abdominal mass in a newborn. There are only a few cases of duplex renal system reported in the literature in which the ureter has assumed massive proportions, completely overshadowing the renal pelvis and parenchyma. Mahajan et al.[8] reported a case of an adult woman who had unilateral upper-pole giant hydroureter in a duplex kidney which was incidentally detected during caesarean section. The authors performed heminephrectomy. Whitmore et al.[9] reported a case of giant hydronephrosis of a duplex system associated with ureteral ectopia.
This case highlights the extent to which a ureter can dilate in neonate. To our knowledge, this is the first case with CGM with duplex system presenting as abdominal lump in a neonate.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kelalis PP. Renal pelvis and ureter. In: Kelalis PP, King LR, Belman AB, editors. Clinical Pediatric Urology. 2nd ed. Philadelphia: Saunders; 1985. pp. 672–725. [Google Scholar]
- 2.Peters CA. Perinatal urology. In: Wein AJ, Kavoussi LR, Novick AC, editors. Campbell-Walsh Urology. 9th ed. Philadelphia: Saunders; 2007. pp. 3176–97. [Google Scholar]
- 3.Huang CJ. Congenital giant megaureter. J Pediatr Surg. 1987;22:235–9. doi: 10.1016/s0022-3468(87)80336-6. [DOI] [PubMed] [Google Scholar]
- 4.Privett JT, Jeans WD, Roylance J. The incidence and importance of renal duplication. Clin Radiol. 1976;27:521–30. doi: 10.1016/s0009-9260(76)80121-3. [DOI] [PubMed] [Google Scholar]
- 5.Ramaswamy S, Bhatnagar V, Mitra DK, Gupta AK. Congenital segmental giant megaureter. J Pediatr Surg. 1995;30:123–4. doi: 10.1016/0022-3468(95)90629-0. [DOI] [PubMed] [Google Scholar]
- 6.Uson AC, Womack CE, Berdon WE. Giant ectopic ureter presenting as an abdominal mass in a newborn infant. J Pediatr. 1972;80:473–6. doi: 10.1016/s0022-3476(72)80510-9. [DOI] [PubMed] [Google Scholar]
- 7.Lelli-Chiesa P, Cupaioli M, Rossi C, Dòmini M, Angelone A. Congenital giant megaureter: first neonatal case. J Pediatr Surg. 2001;36:944–5. doi: 10.1053/jpsu.2001.23996. [DOI] [PubMed] [Google Scholar]
- 8.Mahajan NN, Sahay S, Kale A, Nasre M. Unilateral upper-pole giant hydroureter in a duplex renal system: an incidental finding in cesarean section. Arch Gynecol Obstet. 2008;278:149–51. doi: 10.1007/s00404-007-0543-x. [DOI] [PubMed] [Google Scholar]
- 9.Whitmore RB, 3rd, Schellhammer PF. Giant hydronephrosis of a duplex system associated with ureteral ectopia. J Urol. 1989;141:1186–8. doi: 10.1016/s0022-5347(17)41209-2. [DOI] [PubMed] [Google Scholar]