

Abstract
Aim:
To assess the prevalence and correlates of current smoking, awareness of hazards, and quitting behavior among smokers 30 years and above.
Materials and Methods:
Study design: Cross-sectional; Setting: Gokulpuri, a resettlement colony in East Delhi, India; Sample size: 911, persons aged 30 years and above using systematic random sampling; Study tools: Semi-structured questionnaire.
Results:
Prevalence of current smoking was found to be 24.6% (95% CI 21.90 - 27.49). Majority 198 (88.4%) of current smokers smoked bidi exclusively, and on an average 13.5 bidi/cigarette were smoked per day. Multivariate analysis showed the factors associated with current smoking as male sex, advancing age, illiteracy, skilled occupation, low socio-economic status, and low BMI (P < 0.001). 64.2% were aware of the hazards of smoking. 63 (21.9%) had quit smoking in the past, majority due to the health problems. Low educational status was associated with poor hazard awareness and quitting behavior.
Conclusion:
Smoking is a significant problem among poor and illiterate males, shows an increasing trend with an advancing age and is directly associated with skilled occupation and low BMI. There are significant gaps in knowledge regarding hazards of smoking.
KEY WORDS: Awareness, prevalence, quit, resettlement, smoking
INTRODUCTION
Tobacco use is a leading public health problem all over the world with 82% of the world's 1.1 billion smokers residing in low and middle income countries and where, in contrast to the declining consumption in high-income countries, tobacco consumption is on the rise.[1] Indian studies have recognized tobacco use as a major health hazard.[2,3] Tobacco consumption has overall been a major contributor to deaths due to circulatory diseases, pulmonary and malignant diseases in India.[2] Smoking also increases the incidence of clinical tuberculosis, is a cause of half the male tuberculosis deaths in India, and of a quarter of all male deaths in middle age.[3] Information on prevalence of tobacco use in India is available from surveys carried out in general community. According to the national cross-sectional household survey, India has more than 200 million tobacco consumers; however, prevalence of smoking and tobacco chewing varies widely between different states, and has a strong association with individual's socio-cultural characteristics.[4] A recent nationwide study on smoking and mortality in India estimated that smoking in persons between the ages of 30 and 69 years is responsible for about 1 in 20 deaths of women and 1 in 5 deaths of men, totaling to 1 million deaths per year.[5] Study of smoking pattern among middle age and elderly has received poor attention despite its proven implications on health. The present study was thus carried out to determine:
Prevalence and correlates of tobacco smoking among persons aged 30 years and above in a resettlement colony of Delhi.
Level of awareness regarding hazards of tobacco smoking.
Quitting behavior among smokers and factors influencing such behavior.
MATERIALS AND METHODS
From previous study, the prevalence of current smoking in Delhi was 23.2%,[6] which would require a sample size of at least 595 subjects to estimate the prevalence of current smoking with 15% relative precision and with 95% confidence.
This cross-sectional study was conducted in Gokulpuri, a resettlement colony in New Delhi, India during May 2007 - April 2008. The study included persons aged 30 years and above residing in the study area at the time of survey. The area has 4 blocks A, B, C, D with a total population of 22100 (5402, 5222, 5792, 5684 respectively in the 4 blocks). There are 4041 households and 2404 houses (568, 576, 643, and 617 houses, respectively, in blocks A, B, C, D). Every 4th house was selected by the systematic random sampling method in each of the 4 blocks of the area. From each of the selected houses, one household having person(s) 30 years and above age was selected. If the house had more than one household with persons above 30, lottery was drawn to select the household. If there was no person above 30 in house visited, the immediate next house was chosen. In the selected household, all the persons above 30 years who were willing to participate and giving written informed consent were included in the study. A total of 600 households (142, 144, 160, and 154, respectively, in the 4 blocks) were selected, and 955 individuals were approached. Out of these, 911 persons were interviewed (211, 227, 238, and 235 persons in 4 blocks, respectively).
A pretested semi-structured questionnaire was used for data collection. The socio-demographic variables collected were age, sex, educational attainment, and occupation of the participant and income of the family. Socio-economic status was determined using the Modified Kuppuswamy scale.[7] Subjects were interviewed about their smoking status. They were classified as current smokers: Smoked regularly for within 1 month prior to examination; non smokers: Never smoked or occasionally smoking; Ex-smokers: Stopped more than 1 month prior to examination; and ever smokers comprising of current and ex-smokers.[6] Details on the different forms of smoking used, including cigarette and bidi and hukkah as well as on the numbers smoked per day, were obtained from the smokers. Pack years were calculated from the average number of cigarettes and/or bidis smoked per day; 1 pack year taken as smoking 20 cigarettes or 80 bidis for 1 year.[6] Weight was measured in kilograms using a Portable Adult weighing Scale. Participants were asked to stand still on scale with face forward, and place arms on the sides of the body. Height was measured in centimeters without the participant wearing foot or head gear. Before the reading was taken, the participant was requested to have feet together, heels against the wall, knees straight, and look straight ahead and a point corresponding to height was marked on the wall using a hard cardboard. The distance between floor and the point was noted using a non-stretchable metallic measuring tape.
Data was coded, analyzed, and statistically evaluated using SPSS (Statistical Package for Social Sciences, version 16.0). Categorical variables were described using Chi-square test and fisher's exact test. Trend Chi-square test was used to find increasing trend of percentages. Odds ratios (OR), 95% confidence interval (95% CI), and P-values were calculated for each predictor variable. Significance was determined for a P-value ≤ 0.05. A Univariate analysis was performed to determine variables related to current smoking. Multivariate logistic regression was performed to determine the independent predictors of current smoking by including variables significant at a level P ≤ 0.2 in univariate analysis.
The study is approved by the institutional ethics committee. An informed consent was sought from the eligible persons. Further information was given to persons who consented to take part in the study, and the participants were free to leave the study any time if they desired to do so.
RESULTS
Out of the 955 people approached, 911 consented to participate in the study giving a response rate of 95.3%.
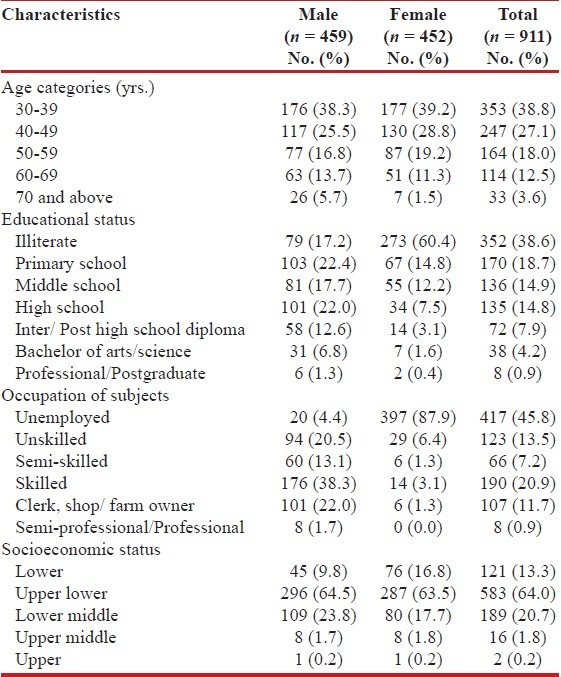
A total of 911 individuals participated in the study with equal representation of both males and females. The age of the participants varied from 30 to 90 years (range - 60 years). Mean age of the subjects was 44.88 ± 11.7 years. Participants aged 30-59 years constituted 83.8% of the study population. There was no difference in the age-wise distribution of males and females up to age of 69 years (χ2 = 2.40, P = 0.49). Majority of the study subjects belonged to the lower socio-economic status. About 40% population consisted of unskilled, semi-skilled, and skilled workers. More than half the population was either illiterate or only primary school pass [Table 1].
Table 1.
Socio-demographic characteristics of the study population
In all, 224 participants were found to be currently smoking, giving an overall prevalence of current smoking to be 24.6% (95% CI 21.90 - 27.49) in the study population. History of ever smoking was reported by 287 (31.5%) participants (95% CI 28.57 - 34.59) [Table 2].
Table 2.
Distribution of study participants according to smoking status
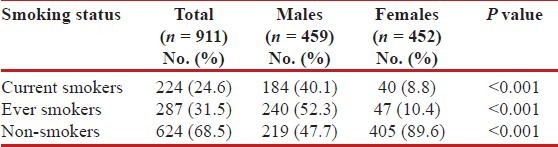
Among current smokers, majority 198 (88.4%) smoked bidi exclusively, 18 (8%) smoked cigarette exclusively, and 8 (3.6%) smoked a combination of bidi and hookah/cigarette. With respect to the amount of tobacco smoke exposure in ever smokers, most 116 (40.4%) had less than 2.5 pack year exposure, 78 (27.2%) had an exposure between 2.51 - 6.25 pack years, 66 (23%) between 6.26 - 13.50 pack years, whereas 27 (9.4%) had more than 13.5 pack year exposure. On an average, 13.5 bidi/cigarette were smoked by smokers per day.
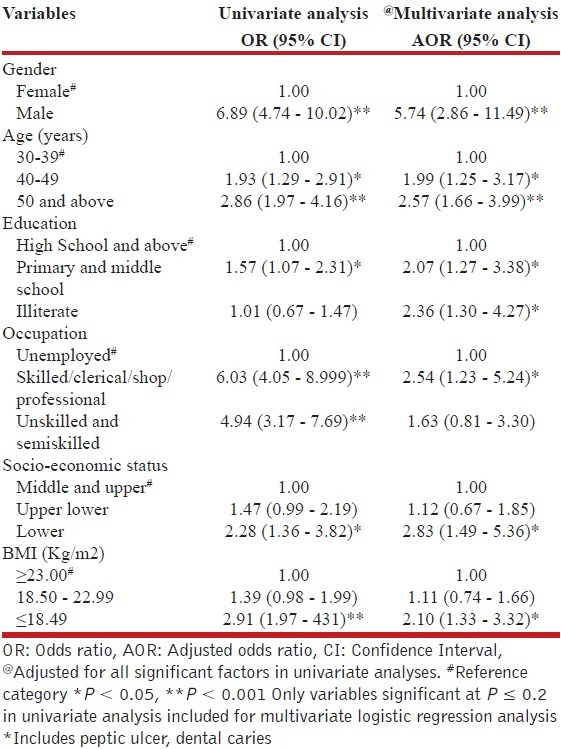
More male participants were found to be currently smoking 184 (40.1%) in comparison to females (8.8%), and the association between tobacco smoking and gender was statistically significant (P < 0.001) [Table 2]. Smoking showed an increasing trend with an advancing age in both males and females [Table 3]. On univariate analysis, smoking was found to be significantly associated with advancing age, primary and middle education, lower socio-economic status, unskilled semi-skilled and skilled occupation, and lower BMI. On multivariate analysis, the factors, which were found to be significantly associated with current smoking, were: Male sex (OR = 5.74 (95% CI 2.86 - 11.49)), advancing age (OR = 1.99 (95% CI 1.25 - 3.17) for age 40 49 years, (OR = 2.57 (95% CI 1.66 - 3.99) for 50 years and above), lower education (OR = 2.07 (95% CI 1.27 - 3.38)) for up to middle school, (OR = 2.36 (95% CI 1.30 - 4.27) for illiterate), skilled occupation (OR = 2.54 (95% CI 1.23 - 5.24)), lower socio-economic status (OR = 2.83 (95% CI 1.49 - 5.36)), and low BMI (OR = 2.10 (95% CI 1.33 - 3.32)) [Table 4]. There was an increasing trend of smoking with increasing age (χ2tr = 22.9, P < 0.001), decreasing BMI (χ2tr = 23.68, P < 0.001), and low socio-economic status (χ2tr = 9.82, P = 0.0017).
Table 3.
Prevalence of current smoking among males and females according to socio-demographic factors and BMI

Table 4.
Multiple logistic regression analysis to evaluate factors associated with smoking
Of all participants in the study, 585 (64.2%) were aware of the hazards of tobacco smoking. Current smokers 69.6% (156 out of 224) had better knowledge than non-smokers (62.4%). Most of the respondents believed that smoking increased the chances of tuberculosis, respiratory problems, and cancer [Table 5].
Table 5.
Participants’ awareness regarding hazards of tobacco smoking

Of the 287 ever smokers, 63 (21.9%) had quit smoking in the past due to some reason. 17 (5.9%) participants stopped smoking for less than a year, whereas majority 46 (16%) had quit for more than a year. Among the 63 successful quitters, 17 (27%) did not have a specific reason to quit and did so by self offered vow to quit. Majority 35 (55.5%), however, quit smoking due to the initiation of health problems, which included respiratory problems (36.5%) like diagnosed cases of chronic obstructive pulmonary disease, exacerbation of asthma, chronic cough, and breathlessness; heart disease (3.17%) and other illnesses (15.8%). Apart from these, other factors contributing to quitting were social or familial pressure, either by spouse/other family member(s) in 8 (12.6%) cases and awareness regarding hazards of smoking in 3 (4.7%) cases. Literate smokers were more likely to quit than illiterate smokers (60.3% vs 39.7%).
DISCUSSION
The purposes of this population-based study were to estimate the prevalence and correlates of current smoking among middle-aged and elderly people and to assess their knowledge and quitting behavior. Only few surveys have been conducted in Delhi with the objective of estimating the prevalence of tobacco smoking, especially among these age groups. National survey on smoking[4] has shown wide variations between urban and rural areas, age, gender, education, and other socio-demographic variables across the country. In the present study, the prevalence of current smoking among people aged 30 years and above in an urban resettlement colony of Delhi was estimated to be 24.6%, and this was much higher among males (40.1%) than females (8.8%). Similar findings had been reported from Delhi by Chhabra et al.[6] in a clustered community-based study in 2001 with about 50% of adult males between 30-60 years found to be current smokers, and very few female subjects admitting to smoking. The overall prevalence of smoking among 4141 persons, aged 18 years and above, belonging to different socio-economic strata, was estimated to be 23.2% (males 39.1% and females 2.6%).[6] Other studies in Delhi among persons aged 15 years and above have also shown a higher level of smoking habit among males (23.9%[4] to 29.5%[8]) in comparison to females (1.8%[4] to 4.2%[8]). Recently, a survey in urban area of Chennai[3] also reported a 38% prevalence of smoking among males aged 35-69 years in the city. One of the important factors for low prevalence of smoking among females was social unacceptability. There was an increasing trend of smoking with an increasing age being higher among older age groups compared with the younger ones. The prevalence of smoking in both the sexes increased with age leveling off after 70 years of age. Similar gender differences in smoking and increasing trends with age have been reported earlier in Delhi,[6] on a national level,[8] and in Zambia.[9]
Majority of the smokers in the present study preferred bidi (89%) and few smoked cigarettes (8%). The use of hukka in the study population was negligible. Bidi is preferred by the study population due to economic reasons as it is much cheaper than cigarette. On an average, 13.5 bidi/cigarettes were smoked by smokers per day. Similar findings have been reported by Chhabra[6] in Delhi with 60% smokers above 18 years age smoking bidi. A multi-centric study in Delhi, Kanpur, Chandigarh, and Bangalore also found that most (51.7%) of the urban smokers smoked bidis with an average consumption being 12.4 bidi/cigarette per day.[8]
In the present study, tobacco use was highest amongst the illiterates wherein 54% and 12% of illiterate males and females respectively smoked tobacco. Illiterates were 2.3 times more likely to smoke than high school passed. Other studies by Rani[4] and Chhabra[6] have also shown lower literacy level to be a strong predictor of smoking. We also found 3-fold increased risk of smoking among people with low socio-economic status. Studies in the past have already suggested that the poor are 8-10 times more likely to smoke bidis.[1] Similar trends have been observed in Delhi by Chhabra[6] and on a country wide basis by Jindal,[8] and the national cross-sectional survey.[4] Interestingly, we found that overweight or obese people were less likely to be current smokers than lean people. An inverse relation of BMI and smoking has been demonstrated by various studies.[9,10]
Overall, the study highlights that smoking is a significant problem among males who are lesser educated and belong to low socio-economic class.
With regard to awareness regarding hazards of tobacco smoking, two third of the people in this study had some knowledge on this aspect. Interestingly, smokers had better knowledge as compared to non-smokers. However, there were huge gaps in knowledge, and majority participants knew very little of the wide implications of tobacco use on health. Added to it, a sizable population did not have any knowledge of impact of tobacco on health. This might be attributed to low level of education in the study population. Poor literacy status has been found to be associated with poor awareness of the health hazards of tobacco consumption, increased likelihood of exposure to conditions favoring initiation of smoking and chewing of tobacco, and higher overall risk taking behavior.[11]
In the present study, around 21.9% of ever smokers had quit smoking. Among those who quit, majority did so due to their health problems. Among 11000 ever smokers of 15 years and above age, Jindal[8] had reported a quit rate of 10% with health problems being an important reason for abstinence.
CONCLUSION
It is a matter of concern to find high levels of smoking, especially among the illiterate and poor people. This is bound to increase the disease burden from chronic illnesses apart from communicable and nutrition-related diseases in these vulnerable groups. Smoking has also shown a rising trend with age emphasizing that initiation into the habit may occur at any age and not just among young people. This implies that tobacco control policies will have to focus on almost all age groups up to the 50 plus age. In this regard, health education can play a pivotal role and can have a lasting impact on reduction of tobacco smoking by improving awareness levels of the population. This can be done through mass media and through school and community-based education programs. In view of the limited knowledge among people regarding health implications of tobacco use, there is need to design appropriate health education material for illiterates and poorer sections of the population and also to elaborate the scope of warning labels on tobacco packs with focus on other potential hazards of smoking like heart disease, hypertension, chronic lung disease, and infertility as well rather than just focusing on cancer. The association between smoking and body mass index should be explored further, so that an appropriate intervention can be designed that addresses both smoking and nutrition.
Limitations
Though the study provides useful information, it may have some limitations. The survey was done in urban resettlement colony of Delhi, and hence the results can only be generalized to the sampled population. Our survey was cross-sectional, and smoking status was by self-reporting. Therefore, some participants may have under-reported their smoking habit. Moreover, due to the existing social taboo about tobacco use, some female participants, in particular, might not have reported their smoking habit. In spite of these limitations, we believe that our findings have not been significantly affected.
ACKNOWLEDGEMENTS
The authors are grateful to all the participants for their kind cooperation in carrying out this survey.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Gajalakshmi CK, Jha P, Ranson K, Nguyen S. Global patterns of smoking and smoking attributable mortality. In: Jha P, Chaloupka FJ, editors. Tobacco control in developing countries. 1st ed. New York: Oxford University Press; 2000. pp. 11–39. [Google Scholar]
- 2.Singh RB, Singh S, Chattopadhya P, Singh K, Singh V, Kulshrestha SK, et al. Tobacco consumption in relation to causes of death in an urban population of north India. Int J Chron Obstruct Pulmon Dis. 2007;2:177–85. [PMC free article] [PubMed] [Google Scholar]
- 3.Gajalakshmi V, Peto R, Kanaka TS, Jha P. Smoking and mortality from tuberculosis and other diseases in India: Retrospective study of 43000 adult male deaths and 35000 controls. Lancet. 2003;362:507–15. doi: 10.1016/S0140-6736(03)14109-8. [DOI] [PubMed] [Google Scholar]
- 4.Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control. 2003;12:e4. doi: 10.1136/tc.12.4.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jha P, Jacob B, Gajalakshmi V, Gupta PC, Dhingra N, Kumar R, et al. A nationally representative case-control study of smoking and death in India. N Engl J Med. 2008;358:1137–47. doi: 10.1056/NEJMsa0707719. [DOI] [PubMed] [Google Scholar]
- 6.Chhabra SK, Rajpal S, Gupta R. Patterns of smoking in Delhi and comparison of chronic respiratory morbidity among beedi and cigarette smokers. Indian J Chest Dis Allied Sci. 2001;43:19–26. [PubMed] [Google Scholar]
- 7.Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy's socioeconomic status scale-updating for 2007. Indian J Pediatr. 2007;74:1131–2. [PubMed] [Google Scholar]
- 8.Jindal SK, Aggarwal AN, Chaudhry K, Chhabra SK, D’Souza GA, Gupta D, et al. Tobacco smoking in India: Prevalence, quit-rates and respiratory morbidity. Indian J Chest Dis Allied Sci. 2006;48:37–42. [PubMed] [Google Scholar]
- 9.Siziya S, Babaniyi O, Songolo P, Nsakashalo-Senkwe M. Prevalence and correlates for tobacco smoking among persons aged 25 years or older in Lusaka urban district, Zambia. J Public Health Epidemiol. 2011;3:43–8. [Google Scholar]
- 10.Shukla HC, Gupta PC, Mehta HC, Hebert JR. Descriptive epidemiology of body mass index of an urban adult population in western India. J Epidemiol Community Health. 2002;56:876–80. doi: 10.1136/jech.56.11.876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bobak M, Jha P, Nguyen S. Poverty and smoking. In: Jha P, Chaloupka FJ, editors. Tobacco control in developing countries. 1st ed. New York: Oxford University Press; 2000. pp. 41–62. [Google Scholar]