

Abstract
Context:
Compliance for non-pharmaceutical interventions for containment of Influenza A H1N1 is determined by community understanding and accurate information by appropriate risk commu-nication strategy.
Aims:
To assess the baseline awareness of public regarding Influenza A H1N1 and its existing risk communication strategy; and to assess public expressed willingness to comply with containment measures.
Materials and Methods:
Sample of 300 subjects (>18 years) coming to primary health centre (PHC) in Delhi was interviewed using a semi-structured questionnaire. The data was collected from 1st July to 1st Sept 2009 by systematic random sampling.
Statistical Analysis Used:
Chi-square test and binary logistic regression.
Results:
Only 66 (22%) individuals had complete knowledge about the spread, symptoms, risk groups, and method of prevention for Influenza A H1N1 infection. Knowledge was significantly higher among males and literates. Only 45 (15%) individuals thought that information given by government on H1N1 is complete and understandable.
Conclusions:
Majority of the respondents were willing to comply with containment measures, if implied by government. It was significantly high among literates.
KEY WORDS: Compliance, influenza A H1N1, non-pharmaceutical intervention, risk communication
INTRODUCTION
According to WHO's estimation, seasonal influenza epidemics result in about 3 to 5 million cases of severe illness worldwide.[1] In order to limit the spread of the disease, WHO recommends the use of non-pharmaceutical interventions (NPIs) like hand washing, cough etiquettes, social distancing, public education, and travel restrictions.[2] A number of studies[3–7] have found the effectiveness of non-pharmaceutical intervention in delaying the temporal effect of a pandemic, reducing the overall and peak attack rate, and reducing the number of deaths. But it has been found that the level of compliance to NPIs may be influenced by the provision of accurate information delivered within a structured commu-nication program.[8] Risk communication strategies must have the capability to provide accurate, credible, actionable, and timely information to the public in culturally and linguistically appropriate ways to inform decision making and reduce uncertainty before, during, and after a public health emergency.[9] The pandemic level of influenza A H1N1 infection has already been reached[10] and the government is implying preventive and curative measures. The present study was conducted with the objective to assess the baseline awareness of the public regarding Influenza A H1N1, existing risk communication strategies for Influenza A H1N1, and willingness to comply with public health containment measures as well as factors influencing compliance.
MATERIALS AND METHODS
A cross-sectional study was conducted in the patients attending the general outdoor patient department (OPD) (catering patients above 18 years) of a Rural Health Training Centre affiliated with a medical college of Delhi from 1st July to 1st Sept 2009.
Clearance was taken from the ethical committee of the institution. A pilot study was conducted in another Primary Health Centre (PHC) affiliated with a medical college taking a sample of 50 individuals for a period of three days, to assess the magnitude of knowledge among the study subjects regarding awareness about influenza A H1N1 infection. On the basis of the results of pilot study, taking the proportion having correct awareness of 30% with power of 80%, level of significance as 0.05 and the worst acceptable proportion as 20%, the required minimum sample size was calculated to be 293. Data was collected in almost 50 working days. Based on earlier OPD records it was found that on an average day general outpatient department attendance was 60-70 patients. Proportion of the new and old patients varied from 40:60 to 50:50. So on an average day 24-30 new attendees were visiting the OPD. To complete our sample, we interviewed every 4th new attendee for a total of 6-7 patients each day.
Only new study subjects were enrolled for the interview. Informed consent was taken from all the respondents. The response rate was good (>90%) as people were curious to talk about the influenza A H1N1 in the current situation of disease.
A pre-tested interview schedule was used. The proforma was designed focusing on the awareness regarding Influenza A H1N1, existing risk communication strategies, risk perception and willingness to comply with public health containment measures.
The interview was semi-structured, with some questions open ended and some closed ended. The questionnaire started with the basic demographic characteristics of the respondent and also enquired about having any child of age <14 years. Then, respondents’ knowledge on the meaning of pandemic, transmission, signs and symptoms, and prevention of Influenza A H1N1 was assessed by asking open-ended questions. The knowledge about the high risk groups for infection and for severe disease was assessed by asking close-ended questions. The respondents who knew accurately about the meaning of pandemic, transmission, signs and symptoms, and prevention of Influenza A H1N1 were said to have ‘Complete Knowledge on H1N1’.
The respondents were also enquired about the perceived fatality and perceived vulnerability for the disease (Yes/No). The next questions included the availability of medicine for influenza A H1N1 and the place to avail themselves of these medicines. Then, multiple questions were asked to assess the awareness about facilities and services (special wards, mask, health education, free testing, and treatment) provided by the government. To know any change in the behaviour of respondents since the onset of outbreak of Influenza A H1N1, questions were asked about change in the cough etiquettes, hand hygiene, avoiding public place and getting more information. Participants were also asked if they would comply with the containment measures (restriction to go to school, office, travel and public places) if imposed by the government in future. Questions were also asked about the source of information and opinion on how reliable (complete, scientific, and understandable) the source of information is.
After completion of the interview the various queries of the people about the Influenza A H1N1 were sorted out, and correct and complete information about the disease was provided by the health educator. The mastercharts were prepared in the excel sheet. Statistical analysis was done using Chi square and binary logistic regression tests.
RESULTS
A total of 300 respondents were interviewed, which included 155 (51.7%) females and 145 (48.3%) males. Mean age of the study population was 31.51 years and 247 (82.3%) study subjects were in the 20-49 year age group. Almost half (170; 56.7%) of the study subjects at the time of interview were not doing any economically gainful work, i.e., being either a home maker, student, unemployed, or retired. Among the remaining, 130 (43.3%) earning study subjects, 83 (27.6%) were salaried, while 47 (16.3%) were daily wage earner. It was also found that 17 (20.5%) of the salaried and 5 (10.6%) of the daily wage earner were unable to work at home.
At the time of interview, majority (249; 83.0%) of respondents were not suffering from any disease. Among the remaining (51; 17.0%) diseased respondents, 33 (11.0%) were suffering from disease conditions, which are known risk factor for occurrence of complication in Influenza A H1N1, e.g., asthma, diabetes mellitus, renal disease, and other chronic diseases.
About two-third (198; 66.0%) of individuals knew the exact meaning of the word pandemic. It was found that two-third (201; 67.0%) respondents were aware of the method of spread of disease; three-fourth (228; 76.0%) knew at least one symptom of Influenza A H1N1 correctly; and 210 (70.0%) individuals knew at least one method of prevention of this disease correctly. Almost half (143; 47.8%) of the respondents had a wrong notion that there is no specific risk group for Influenza A H1N1. About a quarter (83; 27.7%) of respondents were aware that Influenza A H1N1 is more dangerous in children, elderly people and individuals with diseases, which make them more prone for Influenza A H1N1, e.g., Diabetes Mellitus, Asthma, Renal diseases, etc. The knowledge about the different aspects of pandemic was significantly more among males than females and among literates than illiterates [Table 1]. Although males (122; 84.1%) were found to be significantly (P<0.001) more literate as compared to females (101; 74.3%), only 66 (22.0%) of the individuals had complete knowledge on Influenza A H1N1, i.e., methods of spread, symptoms, methods of prevention, and high risk group of Influenza H1N1, which did not differ significantly among males and females. Other factors that were assessed but found to be insignificant were marital status, occupation, earning status, children in family, and disease status.
Table 1.
Association of knowledge for pandemic Influenza A H1N1 with gender and education status of study subjects

About half of the study subjects (164; 54.0%) knew that free testing and medicine facilities were being provided by the government for Influenza A HIN1. Only 129 (43%) individuals were aware about the separate wards created in hospitals by the government for Influenza A H1N1 patients. When knowledge was assessed for the various facilities provided by the government for control of Influenza A H1N1; it was found that literate people knew significantly more than illiterate and females were found to have equal knowledge as their male counterpart except for knowledge of diagnosis and treatment facilities, which was less in females [Table 2]. Other factors assessed and found to be insignificant were marital status, occupation, earning status, disease status, sources of information like TV, radio, newspaper, Internet. Also, no significant difference has been found among male and female regarding the different sources of information.
Table 2.
Association of knowledge for facilities provided by government with gender and education status of the study subjects

A higher number of individuals think Influenza A H1N1 is a fatal disease (84.0%) and they are at risk of getting the infection (78.9%). Furthermore, the respondents who were literate, and consider themselves at risk of getting infection found to have significantly higher perception that influenza A H1N1 is a fatal disease but the this perception did not differ significantly by education level of respondents whether it is low or high.
Most common source of information among interviewees about Influenza A H1N1 was TV (232; 77.3%) followed by radio (111; 37.0%), newspaper (102; 34.0%), friends (82; 27.3%), relatives (47; 15.7%), and doctors (30; 10.0%). On analysis it was found that media (TV, radio, and newspaper) was the significantly more important source of information among individuals with higher education (P<0.001) and have complete knowledge about Influenza A H1N1 (P=0.017). A majority of the respondents (254; 84.7%) believed that government is much more reliable than the private source as a source of information. When asked about the choice of individuals about the media source by which they could approach the government during the pandemic period, television (148; 49.3%) was the most preferred, followed by radio (92; 30.7%), newspaper (81; 27%) and Internet (14; 4.7%). Only 45 (15%) individuals thought that the current information given by the government is based on scientific knowledge, complete, and understandable.
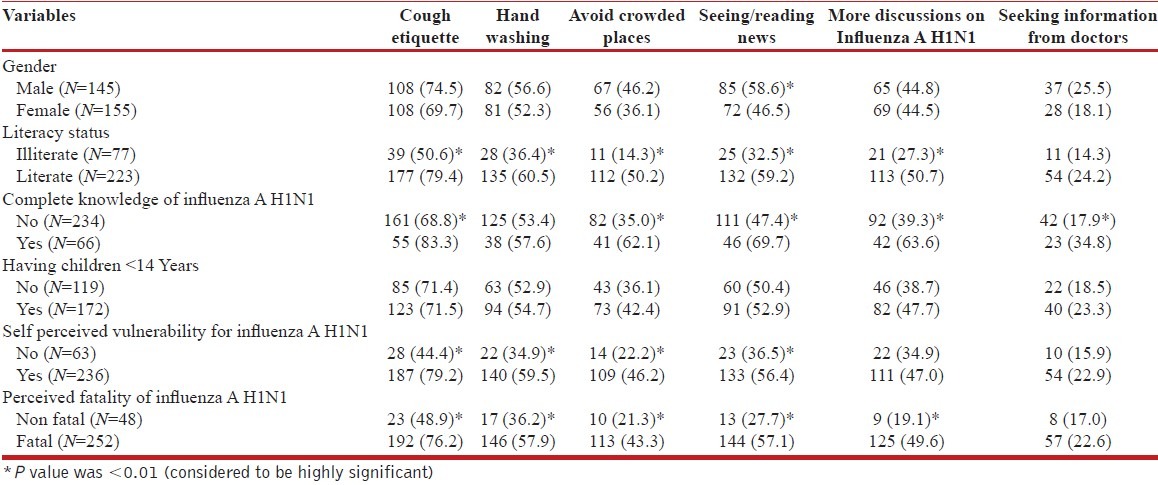
After the onset of outbreak, the respondents reported changes in their own behaviour regarding non-pharmaceutical interventions (NPI's). It was found that 216 (72.0%) individuals have improved their cough etiquettes, 163 (54.3%) improved their hand washing habits; and 123 (41.0%) avoided the crowded places. It was found that 60-150 (20.0-50.0%) subjects have changed their habits for seeking more information about Influenza A H1N1, e.g., reading of newspaper, consulting doctor, discuss among themselves. Table 3 depicts how the behaviour of the individuals for different NPIs varies with different variables. According to results, people who are literate; have complete knowledge on Influenza A H1N1; consider themselves at risk for getting Influenza A H1N1 infection (self-perceived vulnerability for H1N1); and consider Influenza A H1N1 as a fatal disease (disease which always lead to death once you get it), showed significantly more behaviour change than their counterparts. Other variable assessed and found to be insignificant were sex of the individuals and having children in the family.
Table 3.
Change in behaviour related to different non pharmaceutical interventions and its relationship with different variables
The willingness of the respondents to comply with containment measures, if implemented by the government in the future for the containing the spread of infection was also analysed. Three-fourth 226 (75.0%) study subjects responded that would comply if government put restriction on going school of children. The willingness for compliance with the other containment measure was 147 (49%) for not going to workplace; 123 (41%) for not going outdoor; 124 (41.3%) for not going to religious places; 137 (45.7%) for not going on cremation of any relative; and 197 (65.7%) for not travelling inside or outside the country.
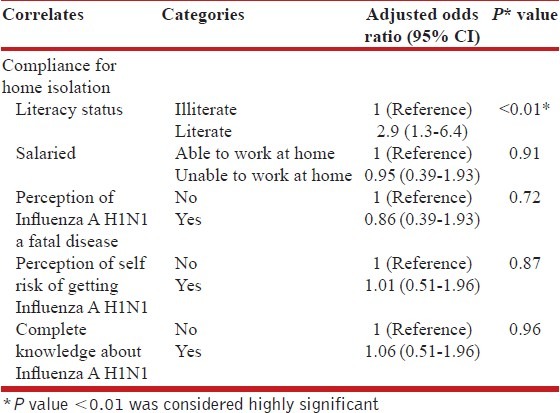
Individuals who responded yes to all containment measures were considered complaint with home isolation. Table 4 shows the result of logistic regression that was applied to know the significant factors associated with compliance for home isolation if suggested by the government. After adjusting for (1) literacy status, (2) salaried individuals whether able to work at home or not, (3) perception of individuals for Influenza A H1N1 as fatal disease, (4) perception of self-risk, and (5) complete knowledge about influenza A H1N1, it was found that literacy status (OR=2.96, CI=1.36-6.45) was significantly associated with compliance for home isolation during pandemic among the study subjects.
Table 4.
Logistic regression analysis showing the significant factors for compliance for home isolation if indicated during pandemic among the study subjects
DISCUSSION
Although 66% of the study population knew the exact meaning of the pandemic, only 22% of the study population had complete knowledge about the Influenza A H1N1 in our study. Eastwood et al.,[11] reported a low level of knowledge, only 44% of national sample of adult Australians knew the term “pandemic influenza” and the proportion of Australians with a reasonable understanding of pandemic influenza was as low as 23%. Wong et al.,[12] calculated the mean total knowledge score of 7.30 (SD±1.961) out of a possible score of 13 about H1N1, with Chinese having the highest scores, followed by Indians, then Malays. These findings are difficult to be compared with our study because the scoring used by them was not a part of our study.
Knowledge about different preventive and curative services provided by the government was low in our study. It was not significantly associated with the sources of information like TV, radio, newspaper, Internet. This finding supports that the information on various services provided by health agencies should be a part of the Information, education and communication (IEC) through common media, so that the people can utilize these services in a timely and appropriate manner.
Wong et al.,[12] also reported that majority of the participants (73.8%) perceived the Influenza A H1N1 infection as often deadly, similar to our findings. However they reported perceived susceptibility to influenza A H1N1 infection as low, dissimilar to our findings of high (78.9%) perceived susceptibility. Infact in our study, high perceived susceptibility to infection was found to be significantly associated with more behavior change regarding NPIs since the last outbreak. This shows that high perceived susceptibility would help in further containment of Influenza A H1N1.
As we found that in our study commonest source of information among study population was media (TV, followed by newspaper and radio), as in other study,[13] particularly among literates and those who had complete knowledge. Though the literacy should not be an issue in this scenario when media is an important source of information like in our study, the completeness of knowledge depends on the understanding of the facts by a person, which depends on the education status as one factor. These findings support need of research into other important methods of providing the complete information in general population, e.g., health camps to improve the knowledge of Influenza A H1N1 and preventive and curative services provided by the government.
In our study, self-reported behavior change for non-pharmaceutical intervention was high among those who consider Influenza A H1N1 as a fatal disease, similar findings were reported in other studies.[14,15] We found complete knowledge and self-perceived vulnerability for Influenza A H1N1 was a significant predictor for self-reported behavior change for NPI. Similar findings were reported by Wong and colleagues,[16] who reported knowledge and level of fear was a significant predictor for practice of health protective behavior across the three ethnic groups. Similar findings were also observed by Lau and colleagues,[17–19] during an outbreak (SARS) in Hong Kong in which they found beliefs and knowledge was directly correlated with immediate behaviour change. These findings emphasize the importance of improving the existing methods and research into new methods to improve the complete knowledge of the population to bring out the behavior change for the further containment of the pandemic.
We found that reported willingness comply with public health containment measures was low, (<50%, except for not going to schools and on cremation). As given in results, the literate people had significantly more knowledge about Influenza A H1N1 and were significantly more willing to comply with government regulation. This could be because of proper knowledge and understanding of the situation. In our study, the willingness of the respondents to comply with containment measures was not significantly related to perceived fatality of the disease, but Kristiansen et al.,[15] in their study found majority of those who considered influenza A H1N1 pandemic as a serious health threat were ready to stay at home too. The reason for different finding from our may be due to, our have defining home isolation by taking different variables like not going to school, office, religious places, etc while they have asked it directly.
We reported low (15%) perceived credibility (measured by completeness, understandability, and scientifically based information) about the information. In contrast Eastwood et al.,[11] reported in their study that about two-third of (69.3%) respondents thought that health authorities had provided sufficient information on swine flu. This could be because of different risk communication strategies in the two countries. Low perceived credibility in our study could be because of the diverse nature of information providers. As majority (84.6%) of the study population trust government health authorities to communicate disaster health information rather than private health authorities, greater emphasis must be put on risk communication by government health agencies rather than diverse nature of information provider, so that the faith of the people on the credibility of the information provided increases.
This study had some limitations. As being a cross-sectional study, we could not assess the how the behaviour has changed over the period of influenza A H1N1 pandemic. Moreover, the study conducted near the beginning of the pandemic when media attention and public curiosity about the disease was high, which could affect the results. We assessed the self-reported behaviour and future self-reported compliance with the containment measure if implemented by the government agency. But there could be a difference in actual practice and self-reported behaviour and compliance. As the study was conducted at one of the PHC affiliated with medical college catering to a specified population, finding of the study cannot be generalized. In statistical analysis we have used OR more frequently as with frequent outcomes, OR will overestimate the effect.
On the basis of the study, it can be concluded that as the uneducated had incomplete knowledge about disease and were less willing to comply for home isolation, hence there is a need of more communication about the disease by using more available, accessible and reliable sources of information, particularly to uneducated section also, so that majority of the population can comply with legislative measures enforced by the govt. in future, if needed. This is the time to prepare the population for acceptance of non-pharmaceutical intervention. Further research studies are needed to evaluate the effectiveness of various communication strategies focussing NPI's in the community. The above listed results can serve as an indicator to assess planning of the government for risk communication for emergencies like Influenza A H1N1.
ACKNOWLEDGEMENT
We are thankful to the Department of Community Medicine for the support in this research work.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Leo SY, Lye CD, Chow A. Influenza in the tropics. Lancet Infect Dis. 2009;9:457–8. doi: 10.1016/S1473-3099(09)70182-3. [DOI] [PubMed] [Google Scholar]
- 2.Geneva: World Health Organization; 2005. [accessed on 2010 Jun 15]. WHO checklist for influenza pandemic preparedness planning. Available from: http://www.who.int/csr/resources/publications/influenza/WHO_CDS_CSR_GIP_2005_4/en/ [Google Scholar]
- 3.Markel H, Lipman HB, Navarro JA, Sloan A, Michalsen JR, Stern AM, et al. Non-pharmaceutical interventions implemented by US cities during the 1918-19 influenza pandemic. JAMA. 2007;298:644–54. doi: 10.1001/jama.298.6.644. [DOI] [PubMed] [Google Scholar]
- 4.Hatchett RJ, Mecher CE, Lipsitch M. Public health interventions and epidemic intensity during the 1918 influenza pandemic. Proc Natl Acad Sci. 2007;104:7582–7. doi: 10.1073/pnas.0610941104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bootsma MC, Ferguson NM. The effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Natl Acad Sci. 2007;104:7588–93. doi: 10.1073/pnas.0611071104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bell DM. Non-pharmaceutical interventions for pandemic influenza, international measures. Emerg Infect Dis. 2006;12:81–7. doi: 10.3201/eid1201.051370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bell DM. Non-pharmaceutical interventions for pandemic influenza, national and community measures. Emerg Infect Dis. 2006;12:88–94. doi: 10.3201/eid1201.051371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jefferson T, Foxlee R, Del Mar C, Dooley L, Ferroni E, Hewak B, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: Systematic review. BMJ. 2008;336:77–80. doi: 10.1136/bmj.39393.510347.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ringel SJ, Trentacost E, Lurie N. How well did health departments communicate about risk at the start of the swine flu epidemic in 2009? Health Aff (Millwood) 2009;28:w743–50. doi: 10.1377/hlthaff.28.4.w743. [DOI] [PubMed] [Google Scholar]
- 10.New influenza A (H1N1) virus: Global epidemiological situation. Geneva: WHO; 2009. Jun, World Health Organization. WER 19 June 2009. Report No.: ISSN 0049-8114. [Google Scholar]
- 11.Eastwood K, Durrheim D, Francis JL, d’Espaignet ET, Duncan S, Islam F, et al. Knowledge about pandemic influenza and compliance with containment measures among Australians. Bull World Health Organ. 2009;87:588–94. doi: 10.2471/BLT.08.060772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wong LP, Sam IC. Knowledge and attitudes in regard to pandemic influenza A (H1N1) in a multiethnic community of Malaysia. Int J Behave Med. 2011;18:112–21. doi: 10.1007/s12529-010-9114-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wong LP, Sam IC. Public sources of information and information needs for pandemic influenza A(H1N1) J Community Health. 2010;35:676–82. doi: 10.1007/s10900-010-9271-4. [DOI] [PubMed] [Google Scholar]
- 14.Lau JTF, Griffiths S, Choi K, Lin C. Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am J Infect Control. 2010;38:374–80. doi: 10.1016/j.ajic.2010.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kristiansen IS, Halvorsen PA, Gyrd-Hansen D. Influenza A H1N1 pandemic: Perception of risk and individual precautions in a general population. Cross sectional study. BMC Public Health. 2007;7:48. doi: 10.1186/1471-2458-7-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wong LP, Sam IC. Behavioral responses to the influenza A H1N1 A(H1N1) outbreak in Malaysia. J Behav Med. 2011;34:23–31. doi: 10.1007/s10865-010-9283-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lau JT, Kim JH, Tsui HY, Griffiths S. Anticipated and current preventive behaviors in response to an anticipated human-to-human H5N1epidemic in the Hong Kong Chinese general population. BMC Infect Dis. 2007;7:18. doi: 10.1186/1471-2334-7-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lau JT, Tsui H, Kim JH, Griffiths S. Perceptions about status and modes of H5N1 transmission and associations with immediate behavioral responses in the Hong Kong general population. Prev Med. 2006;43:406–10. doi: 10.1016/j.ypmed.2006.06.007. [DOI] [PubMed] [Google Scholar]
- 19.Lau JT, Kim JH, Tsui H, Griffiths S. Perceptions related to human avian influenza A H1N1 and their associations with anticipated psychological and behavioral responses at the onset of outbreak in the Hong Kong Chinese general population. Am J Infect Control. 2007;35:38–49. doi: 10.1016/j.ajic.2006.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]