

Abstract
Bronchogenic cysts are generally asymptomatic and are detected incidentally by radiographic imaging as a smooth homogeneous mediastinal/pulmonary lesion. We present a case of a large bronchogenic cyst in the posterior mediastinum mimicking ischemic heart disease in a 70-year-old man with unknown heart disease. In patients with chest pain the rare case of a bronchogenic cyst has to be considered for management of atypical angina pectoris.
KEY WORDS: Bronchogenic cyst, ischemic heart disease, posterior mediastinum
INTRODUCTION
Cysts of the mediastinum constitute a small but important diagnostic group, representing 12%–30% of all primary mediastinal masses.[1] Bronchogenic cysts are the most common cystic masses in the mediastinum. They are congenital lesions arising from abnormal budding of the primitive tracheobronchial tube, which subsequently differentiates into a fluid-filled, blind-ending pouch. More than a half of the patients are asymptomatic and are detected incidentally by radiographic imaging.[2] Most of the bronchogenic cysts are located in the mediastinum, particularly subcarinal and right paratracheal.[3] Bronchogenic cysts in these locations were predisposed to provoke compression symptoms. Especially large cysts may cause left atrial compression, esophageal compression, compression of the main bronchus, or vena cava syndrome.[4,5] We present a case of such large bronchogenic cyst in the posterior mediastinum mimicking ischemic cardiac pain.
CASE REPORT
A 70-year-old man presented in our hospital with intermittent chest pain, dyspnea, dysphagia, and cough since 18 months. Clinical examination was unremarkable. The laboratory tests were without pathologic findings. The echocardiogram (ECG) demonstrated a well-known atrial fibrillation. In the past medical history the patient was treated for hypercholesterolemia, diabetes mellitus, arterial hypertension, and atrial fibrillation. In view of these cardiac risk factors and the possibility of an ischemic heart disease the patient underwent a cardiac catheter examination, but a coronary heart disease could be excluded. To proof other differential diagnoses, such as a thoracic aortic aneurysm or pulmonary diseases a chest computed tomography (CT) was requested, which revealed a 10.5 × 8 × 7 cm homogenous subcarinal mass with fluid density of the posterior mediastinum [Figure 1a]. There was no evidence of invasion of adjacent structures. The mass was seen to compress mainly the right main bronchus [Figure 1b], the left atrium [Figure 1b and c] and the esophagus [Figure 1c], accounting for the symptoms, such as dyspnea, palpitations, chest pain, and dysphagia, respectively. The typical features of the CT pattern (rounded/oval shape, fluid density (<20 HU)) allowing the diagnosis of bronchogenic cyst. Based on these findings and the general consensus that surgery has been advocated as the treatment of choice for symptomatic bronchogenic cysts, the patient was admitted for elective removal of the mediastinal mass. Histopathologic examination of the lesion showed a lining of respiratory epithelium associated with a wall containing smooth muscle, a finding that is characteristic of bronchogenic cyst [Figure 2]. After the cyst excision the patient was completely asymptomatic.
Figure 1.

(a) Contrast-enhanced computed tomography demonstrates a homogeneous 10,5 × 8 × 7 cm mass at the right side of the posterior mediastinum. Axial image at the level of the main pulmonary arteries. (b) Coronal reconstruction showing the lesion sitting at the subcarinal space, elevating the carina and compressing the right main bronchus (arrow). (c) Parasagittal reconstruction of the cyst, which compresses the esophagus (arrow) against the vertebral column posteriorly and impinges on the left atrium inferiorly
Figure 2.
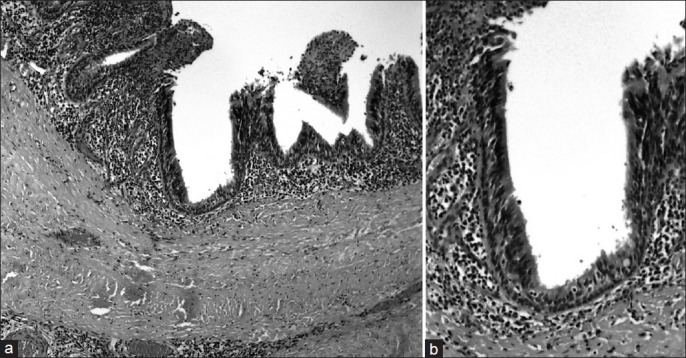
(a) Histopathologic findings of resected cyst revealed ciliated pseudostratified columnar epithelium with a reactive component of lymphocytic infiltrate; (b) Reactive component of lymphocytic infiltrate. Smooth muscle is seen beneath the epithelial lining (arrow). (Hematoxylin- eosin stain; original magnification, ×150)
DISCUSSION
Bronchogenic cysts are congenital lesions derived from abnormal budding of the primitive tracheobronchial tube that occurs during the first 16 weeks of gestation.[4] The majority of bronchogenic cysts are found in the mediastinum, with a reported incidence of 70–85%, although they may also be located in the lung, pericardium, retroperitoneum, thymus, diaphragm, or neck.[4] Mediastinal cysts are usually located in the middle and posterior mediastinum.[3] The most common presenting symptoms are cough, chest pain, and dyspnea. Maier's classification subdivides cysts anatomically into 4 groups: subcarinal cysts, paratracheal cysts, hilar cysts, and paraesophageal cysts.[6,7] Subcarinal and right paratracheal locations are the most typical sites,[3] which may cause compression symptoms.[5] The intermittent chest pain of our patient may result from compression of the esophagus (gastroesophageal reflux) and left atrial compression (atrial fibrillation). Based on the fact that a large bronchogenic cyst can also mimic an acute coronary syndrome a detailed history, laboratory tests, and investigations, including radiographic imaging are absolute necessary prior to the treatment of an assumed acute coronary syndrome.[8]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Wychulis AR, Payne WS, Clagett OT, Woolner LB. Surgical treatment of mediastinal tumors: A 40 year experience. J Thorac Cardiovasc Surg. 1971;62:379–92. [PubMed] [Google Scholar]
- 2.Patel SR, Meeker DP, Biscotti CV, Kirby TJ, Rice TW. Presentation and management of bronchogenic cysts in the adult. Chest. 1994;106:79–85. doi: 10.1378/chest.106.1.79. [DOI] [PubMed] [Google Scholar]
- 3.Takeda S, Miyoshi S, Minami M, Ohta M, Masaoka A, Matsuda H. Clinical spectrum of mediastinal cysts. Chest. 2003;124:125–32. doi: 10.1378/chest.124.1.125. [DOI] [PubMed] [Google Scholar]
- 4.St-Georges R, Deslauriers J, Duranceau A, Vaillancourt R, Deschamps C, Beauchamp G, et al. Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg. 1991;52:6–13. doi: 10.1016/0003-4975(91)91409-o. [DOI] [PubMed] [Google Scholar]
- 5.Tiwari MK, Yadav R, Mathur RM, Shrivastava CP. Mediastinal bronchogenic cyst presenting with dysphagia and back pain. Lung India. 2010;27:86–8. doi: 10.4103/0970-2113.63612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Maier HC. Bronchiogenic cysts of the mediastinum. Ann Surg. 1948;127:476–502. doi: 10.1097/00000658-194803000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tireli GA, Ozbey H, Temiz A, Salman T, Celik A. Bronchogenic cysts: A rare congenital cystic malformation of the lung. Surg Today. 2004;34:573–6. doi: 10.1007/s00595-004-2777-6. [DOI] [PubMed] [Google Scholar]
- 8.McGlynn TJ, Jr, Burnside JW, Gatenby RA. Symptomatic abdominal bronchogenic cyst mimicking acute ischemic heart disease. Heart Lung. 1981;10:109–11. [PubMed] [Google Scholar]